
Compromised Teeth Preserve or Extract: A Review of the Literature

 and
and 
Abstract
:1. Introduction
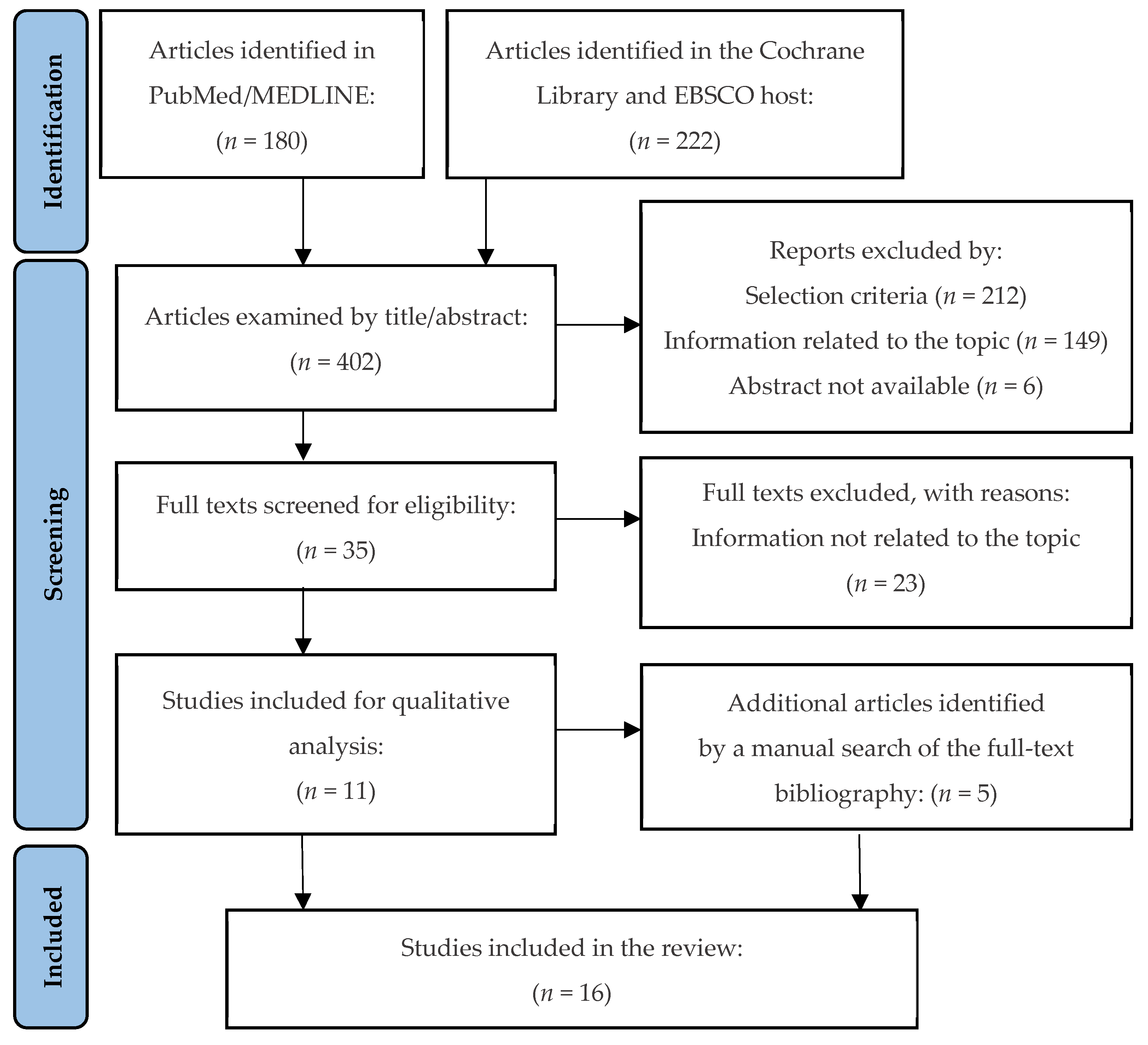
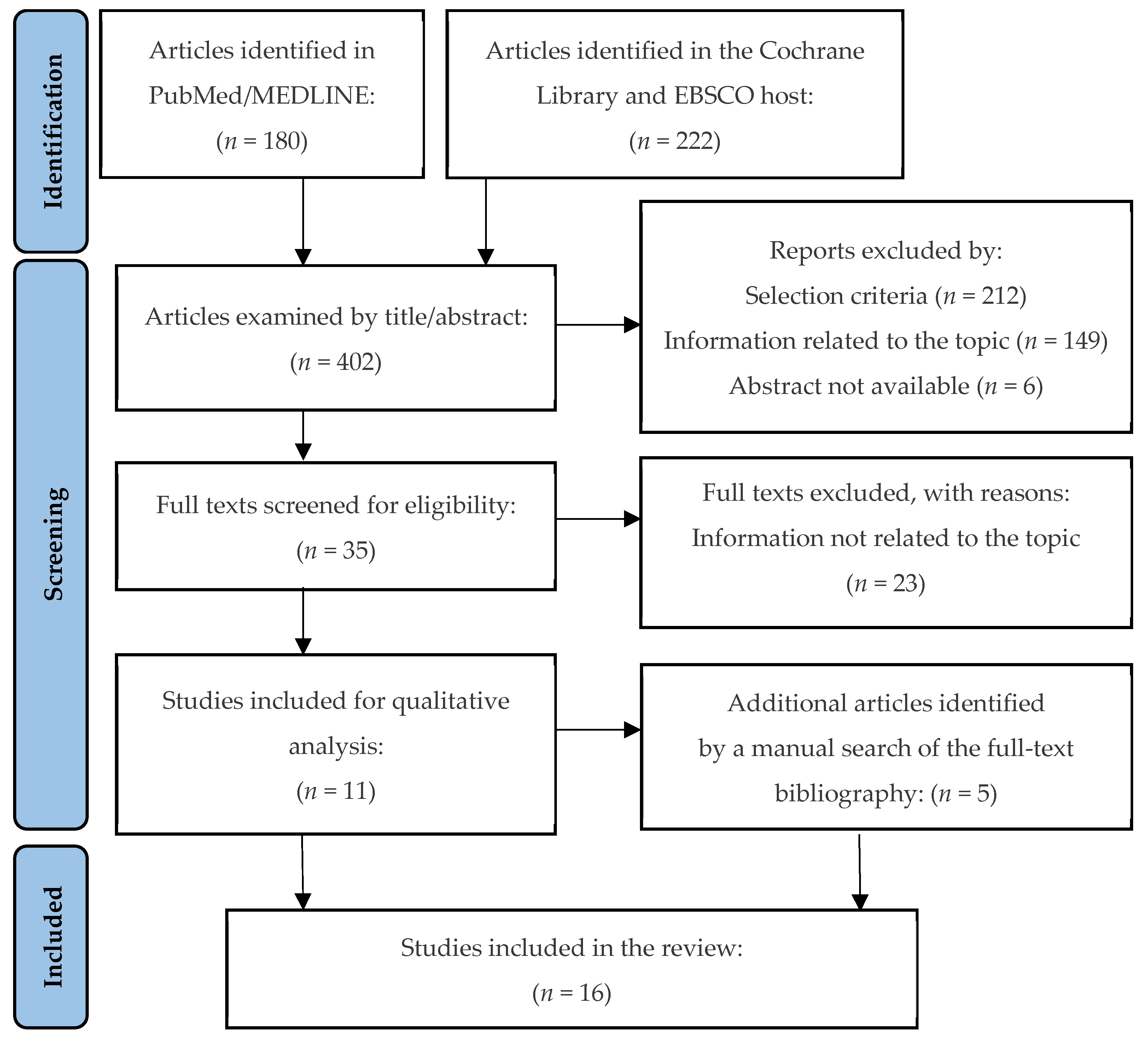
2. Materials and Methods
3. Results
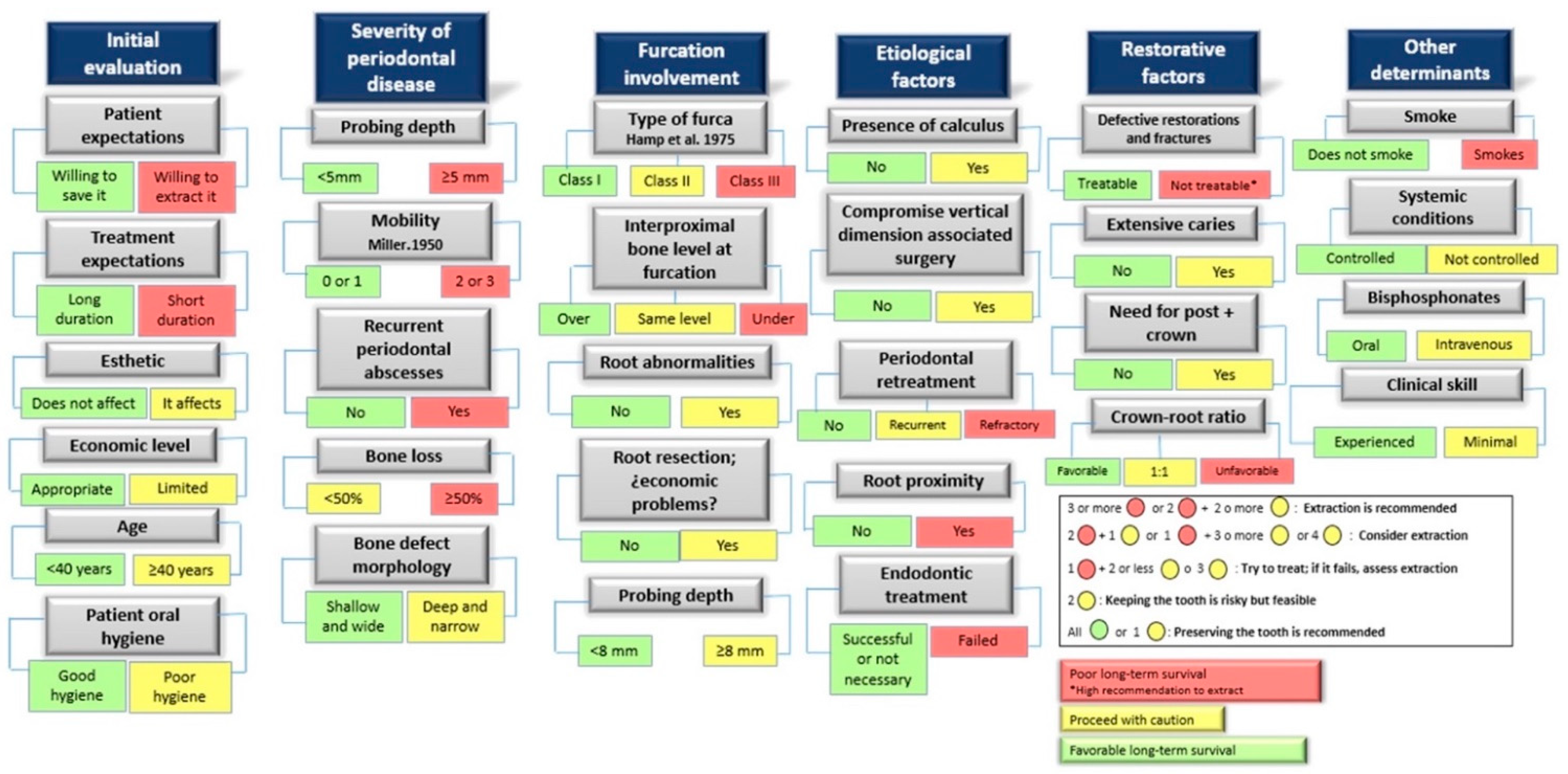
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polzer, I.; Schimmel, M.; Müller, F.; Biffar, R. Edentulism as part of the general health problems of elderly adults. Int. Dent. J. 2010, 60, 143–155. [Google Scholar] [PubMed]
- De Melo, M.A.; Lino, P.A.; Dos Santos, T.R.; Vasconcelos, M.; Lucas, S.D.; de Abreu, M.H. A 15-year time-series study of tooth extraction in brazil. Medicine 2015, 94, e1924. [Google Scholar]
- Samet, N.; Jotkowitz, A. Classification and prognosis evaluation of individual teeth—A comprehensive approach. Quintessence Int. 2009, 40, 377–387. [Google Scholar] [PubMed]
- Beck, J.D. Risk revisited. Community Dent. Oral Epidemiol. 1998, 26, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Kwok, V.; Caton, J.G. Commentary: Prognosis revisited: A system for assigning periodontal prognosis. J. Periodontol. 2007, 78, 2063–2071. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Liao, H.; Fiorellini, J.P.; Kim, S. Factors affecting treatment planning decisions for compromised anterior teeth. Int. J. Periodontics Restor. Dent. 2014, 34, 389–398. [Google Scholar]
- Greenstein, G.; Greenstein, B.; Cavallaro, J. Prerequisite for treatment planning implant dentistry: Periodontal prognostication of compromised teeth. Compend. Contin. Educ. Dent. 2007, 28, 436–446. [Google Scholar]
- Pjetursson, B.E.; Tan, W.C.; Tan, K.; Brägger, U.; Zwahlen, M.; Lang, N.P. A systematic review of the survival and complication rates of resin-bonded bridges after an observation period of at least 5 years. Clin. Oral Implants Res. 2008, 19, 131–141. [Google Scholar] [CrossRef]
- Carlsson, G.E. Critical review of some dogmas in prosthodontics. J. Prosthodont. Res. 2009, 53, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Lekholm, U.; Gunne, J.; Henry, P.; Higuchi, K.; Lindén, U.; Bergström, C. Survival of the brånemark implant in partially edentulous jaws: A 10-year prospective multicenter study. Int. J. Oral Maxillofac. Implants. 1999, 14, 639–645. [Google Scholar]
- Kao, R.T. Strategic extraction: A paradigm shift that is changing our profession. J. Periodontol. 2008, 79, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Donos, N.; Laurell, L.; Mardas, N. Hierarchical decisions on teeth vs. implants in the periodontitis-susceptible patient: The modern dilemma. Periodontol. 2000 2012, 59, 89–110. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; Sukekava, F.; Wennström, J.L.; Lindhe, J. Tissue modeling following implant placement in fresh extraction sockets. Clin. Oral Implant. Res. 2006, 17, 615–624. [Google Scholar] [CrossRef]
- Botticelli, D.; Berglundh, T.; Lindhe, J. Hard-tissue alterations following immediate implant placement in extraction sites. J. Clin. Periodontol. 2004, 31, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, L.; Wasserman, B. A long-term survey of tooth loss in 600 treated periodontal patients. J. Periodontol. 1978, 49, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Song, H.Y.; Han, K.; Cho, K.; Kim, Y. Number of remaining teeth and health–related quality of life: The korean national health and nutrition examination survey 2010–2012. Health Qual. Life Outcomes 2019, 17, 1–10. [Google Scholar] [CrossRef]
- Meyers, I.A. Herodontics–is there a place for maintaining the apparently hopeless tooth? Aust. Dent. J. 2019, 64, S71–S79. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 29, 372. [Google Scholar] [CrossRef]
- Bäumer, A.; El Sayed, N.; Kim, T.; Reitmeir, P.; Eickholz, P.; Pretzl, B. Patient-related risk factors for tooth loss in aggressive periodontitis after active periodontal therapy. J. Clin. Periodontol. 2011, 38, 347–354. [Google Scholar] [CrossRef]
- D’Aiuto, F.; Ready, D.; Parkar, M.; Tonetti, M.S. Relative contribution of patient-, tooth-, and site-associated variability on the clinical outcomes of subgingival debridement. I. probing depths. J. Periodontol. 2005, 76, 398–405. [Google Scholar] [CrossRef]
- De Beule, F.; Alsaadi, G.; Perić, M.; Brecx, M. Periodontal treatment and maintenance of molars affected with severe periodontitis (DPSI = 4): An up to 27-year retrospective study in a private practice. Quintessence Intl. 2017, 48, 391–405. [Google Scholar]
- Goh, V.; Hackmack, P.P.; Corbet, E.F.; Leung, W.K. Moderate-to long-term periodontal outcomes of subjects failing to complete a course of periodontal therapy. Aust. Dent. J. 2017, 62, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Graetz, C.; Dörfer, C.E.; Kahl, M.; Kocher, T.; Fawzy El-Sayed, K.; Wiebe, J.F.; Gomer, K.; Rühling, A. Retention of questionable and hopeless teeth in compliant patients treated for aggressive periodontitis. J. Clin. Periodontol. 2011, 38, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Graetz, C.; Sälzer, S.; Plaumann, A.; Schlattmann, P.; Kahl, M.; Springer, C.; Dörfer, C.; Schwendicke, F. Tooth loss in generalized aggressive periodontitis: Prognostic factors after 17 years of supportive periodontal treatment. J. Clin. Periodontol. 2017, 44, 612–619. [Google Scholar] [CrossRef]
- Grigorie, M.M.; Suciu, I.; Zaharia, D.; Ionescu, E.; Chirila, M.; Voiculeanu, M. Hopeless tooth? prognosis and comprehensive treatment. A case report. J. Med. Life 2021, 14, 287–294. [Google Scholar] [CrossRef]
- Kamma, J.J.; Baehni, P.C. Five-year maintenance follow-up of early-onset periodontitis patients. J. Clin. Periodontol. 2003, 30, 562–572. [Google Scholar] [CrossRef]
- Kavarthapu, A.; Malaiappan, S. Management of periodontic–endodontic lesion in aggressive periodontitis-9 months follow-up: Report of a case. Indian J. Dent. Res. 2019, 30, 149–153. [Google Scholar]
- Machtei, E.E.; Hirsch, I. Retention of hopeless teeth: The effect on the adjacent proximal bone following periodontal surgery. J. Periodontol. 2007, 78, 2246–2252. [Google Scholar] [CrossRef]
- Martinez-Canut, P. Predictors of tooth loss due to periodontal disease in patients following long-term periodontal maintenance. J. Clin. Periodontol. 2015, 42, 1115–1125. [Google Scholar] [CrossRef]
- Saminsky, M.; Halperin-Sternfeld, M.; Machtei, E.E.; Horwitz, J. Variables affecting tooth survival and changes in probing depth: A long-term follow-up of periodontitis patients. J. Clin. Periodontol. 2015, 42, 513–519. [Google Scholar] [CrossRef]
- Seshima, F.; Nishina, M.; Namba, T.; Saito, A. Periodontal regenerative therapy in patient with chronic periodontitis and type 2 diabetes mellitus: A case report. Bull. Tokyo Dent. Coll. 2016, 57, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Tözüm, T.F.; Keçeli, H.G.; Serper, A.; Tuncel, B. Intentional replantation for a periodontally involved hopeless incisor by using autologous platelet-rich plasma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e119–e124. [Google Scholar] [CrossRef] [PubMed]
- Zafiropoulos, G.K.; di Prisco, M.O.; Deli, G.; Hoffmann, O. Maintenance of class III trifurcated molars versus implant placement in regenerated extraction sockets: Long-term results of 2 cases. J. Oral Implantol. 2011, 37, 141–155. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G. Long-term maintenance of an apparently hopeless tooth: A case report. Eur. J. Esthet. Dent. 2007, 2, 390–404. [Google Scholar]
- Nunn, M.E.; Fan, J.; Su, X.; Levine, R.A.; Lee, H.; McGuire, M.K. Development of prognostic indicators using classification and regression trees for survival. Periodontol. 2000 2012, 58, 134–142. [Google Scholar] [CrossRef]
- Lundgren, D.; Rylander, H.; Laurell, L. To save or to extract, that is the question. natural teeth or dental implants in periodontitis-susceptible patients: Clinical decision-making and treatment strategies exemplified with patient case presentations. Periodontol. 2000 2008, 47, 27–50. [Google Scholar] [CrossRef]
- Levin, L.; Halperin-Sternfeld, M. Tooth preservation or implant placement: A systematic review of long-term tooth and implant survival rates. J. Am. Dent. Assoc. 2013, 144, 1119–1133. [Google Scholar] [CrossRef]
- Caplan, D.J.; Li, Y.; Wang, W.; Kang, S.; Marchini, L.; Cowen, H.J.; Yan, J. Dental restoration longevity among geriatric and special needs patients. JDR Clin. Transl. Res. 2019, 4, 41–48. [Google Scholar] [CrossRef]
- Avila, G.; Galindo-Moreno, P.; Soehren, S.; Misch, C.E.; Morelli, T.; Wang, H. A novel decision-making process for tooth retention or extraction. J. Periodontol. 2009, 80, 476–491. [Google Scholar] [CrossRef]
- Halperin–Sternfeld, M.; Levin, L. Do we really know how to evaluate tooth prognosis? A systematic review and suggested approach. Quintessence Int. 2013, 44, 447–456. [Google Scholar]
- Pretzl, B.; Wiedemann, D.; Cosgarea, R.; Kaltschmitt, J.; Kim, T.S.; Staehle, H.J.; Eickholz, P. Effort and costs of tooth preservation in supportive periodontal treatment in a german population. J. Clin. Periodontol. 2009, 36, 669–676. [Google Scholar] [CrossRef] [PubMed]
- D’Cruz, L. Dento-legal considerations about an MI approach. Br. Dent. J. 2017, 223, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Diamantatou, T.; Kotina, E.; Roussou, I.; Kourtis, S. Treatment options for anterior teeth with questionable prognosis: Critical factors in determining whether to maintain or extract. J. Esthet. Restor. Dent. 2016, 28, 157–170. [Google Scholar] [CrossRef]
- Moshaverinia, A.; Kar, K.; Chee, W.W. Treatment planning decisions: Implant placement versus preserving natural teeth. J. Calif. Dent. Assoc. 2014, 42, 859–868. [Google Scholar] [PubMed]
- Saghafi, N.; Heaton, L.J.; Bayirli, B.; Turpin, D.L.; Khosravi, R.; Bollen, A. Influence of clinicians’ experience and gender on extraction decision in orthodontics. Angle. Orthod. 2017, 87, 641–650. [Google Scholar] [CrossRef]
- Baba, N.Z.; Goodacre, C.J.; Kattadiyil, M.T. Tooth retention through root canal treatment or tooth extraction and implant placement: A prosthodontic perspective. Quintessence Int. 2014, 45, 405–416. [Google Scholar]
- Martu, M.A.; Maftei, G.A.; Luchian, I.; Popa, C.; Filioreanu, A.M.; Tatarciuc, D.; Nichitean, G.; Hurjui, L.-L.; Foia, L.-G. Wound healing of periodontal and oral tissues: Part II-Patho-phisiological conditions and metabolic diseases. Rom. J. Oral Rehabil. 2020, 12, 30–40. [Google Scholar]
- Clark, D.; Levin, L. In the dental implant era, why do we still bother saving teeth? J. Endod. 2019, 45, S57–S65. [Google Scholar] [CrossRef]
- Popa, C.G.; Luchian, I.; Ioanid, N.; Goriuc, A.; Martu, I.; Bosinceanu, D.; Martu, M.A.; Tirca, T.; Martu, S. ELISA Evaluation of RANKL Levels in Gingival Fluid in Patients with Periodontitis and Occlusal Trauma. Rev. Chim. 2018, 69, 1578–1580. [Google Scholar] [CrossRef]
- Lin, J.; Tu, C.; Chen, Y.; Wang, C.Y.; Liu, C.M.; Kuo, M.Y.P.; Chang, P.C. Influence of adjacent teeth absence or extraction on the outcome of non-surgical periodontal therapy. Int. J. Environ. Res. Public Health. 2019, 16, 4344. [Google Scholar]
- Ettinger, R.L. Restoring the ageing dentition: Repair or replacement? Int. Dent. J. 1990, 40, 275–282. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
| Author/Year/Country | Design/Follow-Up (Months) | No. Patients/Gender/Age (Years) | No. Teeth/Type of Tooth/Type of Periodontitis/Prognosis | Factors Associated with Decision-Making | Reason for Extracting/ Preserving |
|---|---|---|---|---|---|
| Saminsky, M. et al. (2015) Israel [30] | Cross-sectional 152 ± 25 | 50 31F/19M 46.6 ± 10.6 | 1301 M-Pm-C-I ChP NS | Probing depth General health status Smoking habit Periodontal diagnosis Bacterial plaque index Bleeding on probing | 151 extracted (96 periodontal causes/55 extensive caries or root fracture) |
| Goh, V. et al. (2017) China [22] | Cross-sectional 100.4 ± 44.4 | 65 34F/31M 43.8 ± 11.9 | 1597 M-Pm-C-I AgP-ChP Good (pdep ≤4 mm)-Fair (pdep ≥5 mm)-Questionable (pdep 6–8 mm), Hopeless (pdep ≥8 mm)-Undetermined | General health status Oral hygiene Use of removable prosthesis Smoking habit Dental visit history Number of teeth Bacterial plaque index Bleeding on probing Probing depth Bone crest level | 229 extracted (191 periodontal reasons/23 caries/15 not identifiable by the patient) |
| De Beule, F. et al. (2017) Belgium [21] | Cross-sectional 197 | 402 201F/201M 34–88 | 2559 M* SevP NS | Medical condition Probing Depth Furca engagement Bone loss Gum health Bleeding on probing Tooth type Tooth location | 511 extracted (377 periodontal reasons/60 endodontic problems or endo-periodontal lesions/17 fracture/25 caries/1 prosthetic strategy/31 unknown reason) |
| D’Aiuto, F. et al. (2005) England [20] | Cross-sectional 6 | 94 50F/44M 46 ± 9 | 2589 M-Pm-C-I SevP NS | Probing depth Gingival recessions Bacterial plaque index Bleeding on probing Clinical insertion level Furca engagement Tooth mobility Tooth type Smoking habit Periodontal diagnosis | NS |
| Graetz, C. et al. (2017) Germany [24] | Cross-sectional 208.8 ± 57.6 | 57 35F/22M 34.7 ± 8 | 1505 M-Pm-C-I AgP NS | Probing depth Tooth mobility Radiographic bone loss Furca engagement Smoking habit Tooth type Preoperative antibiotic therapy | 232 extracted (prosthetic and periodontal reasons) |
| Machtei, E. & Hirsch, I. (2007) Israel [28] | Cross-sectional 156 | 93 59F/34M 45.54 ± 1.13 | 110 (74 multirooted/36 single root) ChP Hopeless | Probing depth Radiographic bone loss | 53 extracted 57 saved (the decision was made by the patient without influence from the dentist) |
| Bäumer, A. et al. (2011) Germany [19] | Cross-sectional 126 | 84 68F/16M 30.8 ± 4.1 | 2154 M*-Pm-C-I AgP NS | Smoking habit History of periodontal disease Dental status Probing depth ≥5 mm Clinical insertion level Bleeding on probing Suppuration on probing Furca engagement Gingival index Bacterial plaque index Educational level Dental care compliance | 166 extracted (unknown reason) |
| Graetz, C. et al. (2011) Germany [23] | Cross-sectional 193 ± 54 | 68 (34AgP/34ChP) 28F (11AgP/17ChP) 40M (23AgP/17ChP) 33.3 ± 4.1AgP 51.6 ± 7.4ChP | 923AgP/874ChP M-Pm-C-I AgP-ChP Good (bone loss <50%)-Questionable (bone loss ≥50%- < 70%)-Hopeless (bone loss ≥70%) | Smoking habit Radiographic bone loss ≥50% Probing depth Bacterial plaque index Preoperative antibiotic therapy | 142AgP extracted 133ChP extracted (112AgP-48ChP periodontal reasons/the rest due to endodontic involvement, caries, prosthetics, fracture, or unknown reason) |
| Martinez-Canut, P. (2015) Spain [29] | Cross-sectional 242.4 ± 28.8 | 500 344F/156M 22–74 | 12.830 M*-Pm-C-I AgP-ChP NS | Health condition Smoking habit Bacterial plaque index Probing depth >6 mm Gum recession Furca engagement Tooth mobility 2–3 Radiographic bone loss >50% Root crown ratio 1/1 Root anatomy Periodontal diagnosis | 875 extracted (515 periodontal disease/172 non-restorable caries/75 root and/or coronary fracture/26 endodontic complications/85 strategic extraction for prosthetic and orthodontic considerations) |
| Author/Year/Country | Design/Follow-Up (Months) | No. Patients/Gender/Age (Years) | No. Teeth/Type of Tooth/Type of Periodontitis/Prognosis | Factors Associated with Decision-Making | Reason for Extracting/ Preserving |
|---|---|---|---|---|---|
| Grigorie, M.M. et al. (2021) Romania [25] | Case report 48 | 1 1F 62 | 27 M-Pm-C-I ChP Hopeless (pdep >8 mm, with class II or higher furcation involvement and bone loss ≥70%). | Smoking habit Probing depth ≥5 mm Bony vertical defects Furca engagement Tooth mobility Bacterial plaque index Tooth migration Reduced periodontal support Infrabony defect | 1 extracted (caries and endodontic complications) |
| Kavarthapu, A. & Malaiappan, S. (2019) India [27] | Case report 9 | 1 1F 28 | 1 M AgP Bad | Probing depth >8 mm Bleeding on probing Bacterial plaque index Grade II furcation involvement Vertical bone loss Purulent discharge Tooth mobility grade 2 Negative pulp vitality Apical radiolucency | The tooth was saved (patient compliance) |
| Seshima, F. et al. (2016) Japan [31] | Case report 14 | 1 1M 66 | 27 M-Pm-C-I ChP NS | Probing depth ≥7 mm Bone loss Bleeding on probing Bacterial plaque index Blood glucose levels Tooth mobility | 1 extracted (prophylactic reasons: impacted tooth) |
| Zafiropoulos, G.G.K. et al. (2011) Germany [33] | Case report 180/84 | 2 1F/1M 33/39 | 28/26 M-Pm-C-I ChP NS | Probing depth Bleeding on probing Bacterial plaque index Furca engagement Radiographic bone loss ≥50% Tooth mobility Clinical insertion level Periodontal pathogens | Case 1: all were preserved (the patient rejects any extraction); Case 2: 21 extracted (advanced bone loss and/or dental mobility) |
| Zucchelli, G. (2007) Italy [34] | Case report 12–36 | 1 1F 39 | 1 MxLI EndP NS | Probing Depth Bacterial plaque index Bleeding on probing Clinical insertion level Gingival recession ≥3 mm Bone loss Tooth mobility grade 3 Radiographic radiolucency Negative vitality test Absence of fillings | 53 extracted (43 multirooted/10 single root); 57 saved (31 multirooted/26 single root) (unknown reason) |
| Tözüm, T.F. et al. (2006) Turkey [32] | Case report 18 | 1 1M 42 | 1 MdCI ChP NS | Bacterial plaque index Clinical attachment level ≥6 mm Tooth mobility grade 3 Negative vitality test Probing depth ≥4 mm Radiographic bone loss Extrusion Keratinized gingiva ≥2 mm | 1 saved (upon advice from the dentist to consider a new treatment option) |
| Kamma, J.J. & Baehni, P.C. (2003) Greece [26] | Case report 60 | 25 14F/11M 34.3 ± 2.5 | NS NS AgP NS | Smoking habit Bacterial plaque index Gingival index Bleeding on probing Suppuration on probing Probing depth Clinical insertion level Radiographic bone loss | 29 extracted (18 due to furca involvement/the rest unknown reason) |
| Variable | Total | |
|---|---|---|
| Gender | Women | 868 (60.06%) |
| Men | 577 (39.93%) | |
| Total patients | 1.445 | |
| Age range | 22–88 years | |
| Total teeth examined | 26.553 | |
| Teeth extracted | 2.597 | |
| Periodontal reasons | 1.610 (61.99%) | |
| Prosthetic reasons | 455 (17.52% | |
| Endodontic complications | 86 (3.31%) | |
| Unknown or unidentifiable reason | 446 (17.17%) | |
| Teeth preserved (no initial commitment) | 23.812 | |
| Teeth preserved (with initial commitment) | 144 | |
| The patient made the final decision | 87 (60.41%) | |
| Unknown or unidentifiable reason | 57 (39.58%) | |
| Item | Saminsky, M. et al., 2015 [30] | Goh, V. et al., 2017 [22] | De Beule, F. et al., 2017 [21] | D’Aiuto, F. et al., 2005 [20] | Graetz, C. et al., 2017 [24] | Machtei, E. & Hirsch, I., 2007 [28] | Bäumer, A. et al., 2011 [19] | Graetz, C. et al., 2011 [23] | Martinez-Canut, P., 2015 [29] |
|---|---|---|---|---|---|---|---|---|---|
| Selection | |||||||||
|  | | |  | | | | | |
| | | | | | | | | |
| | | | | | | | | |
| Comparability | |||||||||
| | | | | | | | | |
| | | | | | | | | |
| Results | |||||||||
| | | | | | | | | |
| | | | | | | | | |
| | | | | | | | | |
| Total | 6 | 6 | 7 | 4 | 6 | 7 | 7 | 8 | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cárcamo-España, V.; Cuesta Reyes, N.; Flores Saldivar, P.; Chimenos-Küstner, E.; Estrugo Devesa, A.; López-López, J. Compromised Teeth Preserve or Extract: A Review of the Literature. J. Clin. Med. 2022, 11, 5301. https://doi.org/10.3390/jcm11185301
Cárcamo-España V, Cuesta Reyes N, Flores Saldivar P, Chimenos-Küstner E, Estrugo Devesa A, López-López J. Compromised Teeth Preserve or Extract: A Review of the Literature. Journal of Clinical Medicine. 2022; 11(18):5301. https://doi.org/10.3390/jcm11185301
Chicago/Turabian StyleCárcamo-España, Valentina, Nataly Cuesta Reyes, Paul Flores Saldivar, Eduardo Chimenos-Küstner, Alberto Estrugo Devesa, and José López-López. 2022. "Compromised Teeth Preserve or Extract: A Review of the Literature" Journal of Clinical Medicine 11, no. 18: 5301. https://doi.org/10.3390/jcm11185301
APA StyleCárcamo-España, V., Cuesta Reyes, N., Flores Saldivar, P., Chimenos-Küstner, E., Estrugo Devesa, A., & López-López, J. (2022). Compromised Teeth Preserve or Extract: A Review of the Literature. Journal of Clinical Medicine, 11(18), 5301. https://doi.org/10.3390/jcm11185301