
Does Smoking Affect OSA? What about Smoking Cessation?

 ,
,  , ,
, ,
Abstract
1. Introduction
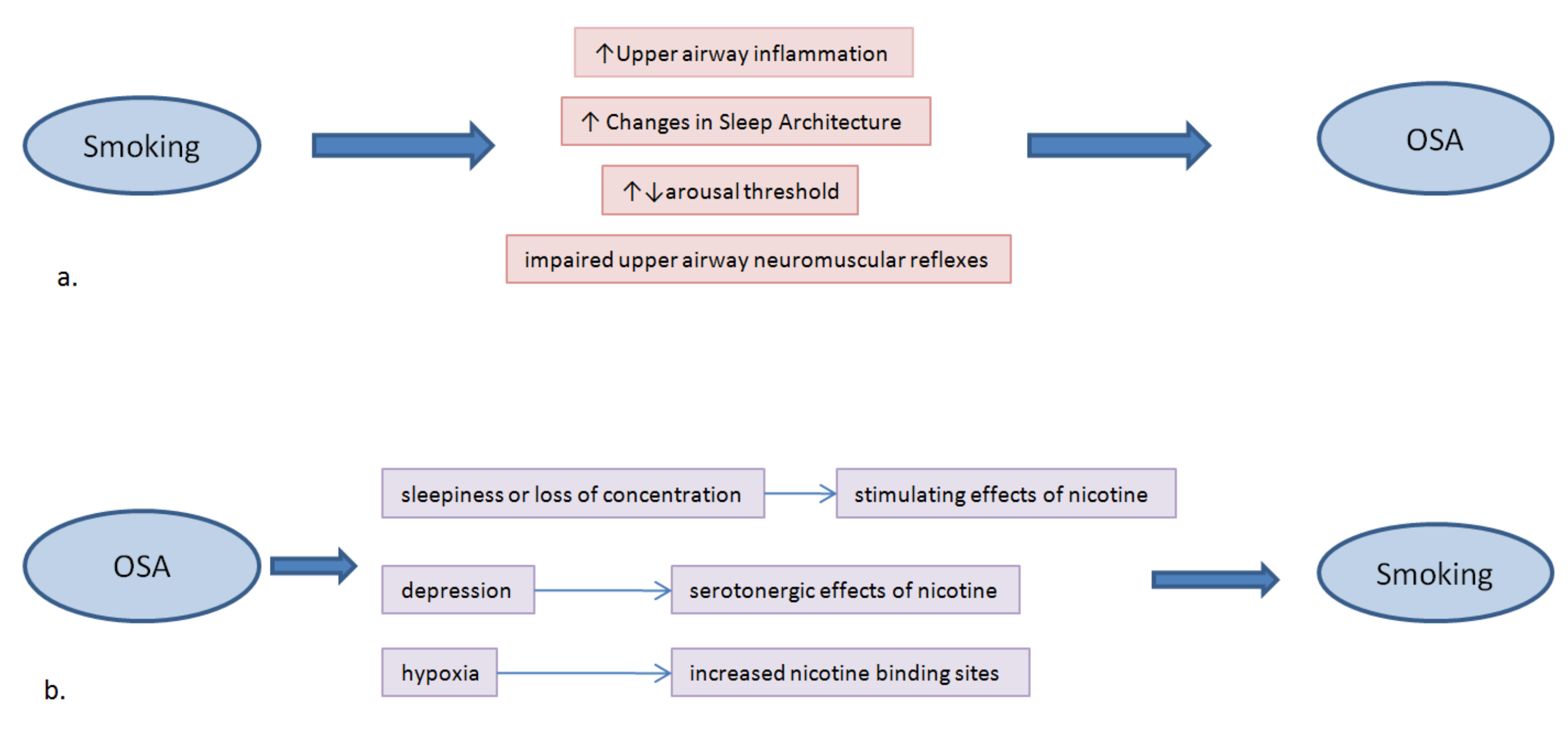
2. Mechanisms by Which Smoking Can Result in OSA
2.1. Upper Airway Inflammation due to Inhalation of Cigarette Smoke
2.2. Changes in Sleep Architecture and Smoking
2.3. Smoking May Affect Arousal Threshold
2.4. Smoking May Impair Upper Airway Neuromuscular Reflexes
3. Association between Smoking and OSA
4. Does OSA Predispose to Smoking?
5. Nicotine and Sleep
6. Smoking Cessation and Sleep
7. Smoking Cessation Treatments and OSA
7.1. Nicotine Replacement Therapy
7.1.1. The Effects of NRT on Sleep of Smokers during Smoking Cessation
7.1.2. Effects of NRT for OSA Treatment
7.2. Bupropion
7.3. Varenicline
7.4. Nortriptyline
7.5. Clonidine
7.6. Cytisine
8. Incidental Effects of Smoking Abstinence on OSA
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dempsey, J.A.; Veasey, S.C.; Morgan, B.J.; O’Donnell, C.P. Pathophysiology of Sleep Apnea. Physiol. Rev. 2010, 90, 47–112. [Google Scholar] [CrossRef] [PubMed]
- Marshall, N.S.; Wong, K.K.H.; Liu, P.Y.; Cullen, S.R.J.; Knuiman, M.W.; Grunstein, R.R. Sleep Apnea as an Independent Risk Factor for All-Cause Mortality: The Busselton Health Study. Sleep 2008, 31, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- George, C.; Nickerson, P.; Hanly, P.; Millar, T.; Kryger, M. Sleep apnoea patients have more automobile accidents. Lancet 1987, 330, 447. [Google Scholar] [CrossRef]
- Jordan, A.S.; McSharry, D.G.; Malhotra, A. Adult obstructive sleep apnoea. Lancet 2013, 383, 736–747. [Google Scholar] [CrossRef]
- Weaver, T.E.; Grunstein, R.R. Adherence to Continuous Positive Airway Pressure Therapy: The Challenge to Effective Treatment. Proc. Am. Thorac. Soc. 2008, 5, 173–178. [Google Scholar] [CrossRef]
- Randerath, W.; Verbraecken, J.; de Raaff, C.; Hedner, J.; Herkenrath, S.; Hohenhorst, W.; Jakob, T.; Marrone, O.; Marklund, M.; McNicholas, W.T.; et al. European Respiratory Society guideline on non-CPAP therapies for obstructive sleep apnoea. Eur. Respir. Rev. 2021, 30, 210200. [Google Scholar] [CrossRef]
- Eckert, D.J.; White, D.P.; Jordan, A.S.; Malhotra, A.; Wellman, A. Defining Phenotypic Causes of Obstructive Sleep Apnea. Identification of Novel Therapeutic Targets. Am. J. Respir. Crit. Care Med. 2013, 188, 996–1004. [Google Scholar] [CrossRef]
- Edwards, B.A.; Eckert, D.J.; McSharry, D.G.; Sands, S.A.; Desai, A.; Kehlmann, G.; Bakker, J.P.; Genta, P.R.; Owens, R.L.; White, D.P.; et al. Clinical Predictors of the Respiratory Arousal Threshold in Patients with Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2014, 190, 1293–1300. [Google Scholar] [CrossRef]
- Younes, M.; Ostrowski, M.; Thompson, W.; Leslie, C.; Shewchuk, W. Chemical Control Stability in Patients with Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2001, 163, 1181–1190. [Google Scholar] [CrossRef]
- Deleanu, O.C.; Pocora, D.; Mihalcu¸ta, S.; Ulmeanu, R.; Zaharie, A.M.; Mihal¸tan, F.D. Influence of smoking on sleep and obstructive sleep apnea syndrome. Pneumologia 2016, 65, 28–35. [Google Scholar]
- Bearpark, H.; Elliott, L.; Grunstein, R.; Cullen, S.; Schneider, H.; Althaus, W.; Sullivan, C. Snoring and sleep apnea. A population study in Australian men. Am. J. Respir. Crit. Care Med. 1995, 151, 1459–1465. [Google Scholar] [CrossRef] [PubMed]
- Franklin, K.A.; Gíslason, T.; Omenaas, E.; Jõgi, R.; Jensen, E.J.; Lindberg, E.; Gunnbjörnsdóttir, M.; Nyström, L.; Laerum, B.N.; Björnsson, E.; et al. The Influence of Active and Passive Smoking on Habitual Snoring. Am. J. Respir. Crit. Care Med. 2004, 170, 799–803. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, E.; Taube, A.; Janson, C.; Gislason, T.; Svärdsudd, K.; Boman, G. A 10-Year Follow-up of Snoring in Men. Chest 1998, 114, 1048–1055. [Google Scholar] [CrossRef] [PubMed]
- Wetter, D.W.; Young, T.B.; Bidwell, T.R.; Badr, M.S.; Palta, M. Smoking as a risk factor for sleep-disordered breathing. Arch. Intern. Med. 1994, 154, 2219–2224. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, V.; Dixon-Williams, S.; Thornton, J.D. Where there is smoke there is sleep apnea: Exploring the relationship between smoking and sleep apnea. Chest 2014, 146, 1673–1680. [Google Scholar] [CrossRef]
- Lui, M.M.S.; Mak, J.C.W.; Lai, A.Y.K.; Hui, C.K.M.; Lam, J.C.M.; Lam, D.C.L.; Ip, M.S.M. The Impact of Obstructive Sleep Apnea and Tobacco Smoking on Endothelial Function. Respiration 2016, 91, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-W.; Chang, C.-H.; Chuang, H.-Y.; Cheng, H.-Y.; Lin, C.-I.; Chen, H.-T.; Yang, C.-C. What is the association between secondhand smoke (SHS) and possible obstructive sleep apnea: A meta-analysis. Environ. Health 2022, 21, 58. [Google Scholar] [CrossRef]
- Kim, K.S.; Kim, J.H.; Park, S.Y.; Won, H.-R.; Lee, H.-J.; Yang, H.S.; Kim, H.J. Smoking Induces Oropharyngeal Narrowing and Increases the Severity of Obstructive Sleep Apnea Syndrome. J. Clin. Sleep Med. 2012, 8, 367–374. [Google Scholar] [CrossRef]
- Schrand, J.R. Is sleep apnea a predisposing factor for tobacco use? Med. Hypotheses 1996, 47, 443–448. [Google Scholar] [CrossRef]
- Lin, Y.-N.; Li, Q.-Y.; Zhang, X.-J. Interaction between smoking and obstructive sleep apnea: Not just participants. Chin. Med. J. 2012, 125, 3150–3156. [Google Scholar]
- Daijo, H.; Hoshino, Y.; Kai, S.; Suzuki, K.; Nishi, K.; Matsuo, Y.; Harada, H.; Hirota, K. Cigarette smoke reversibly activates hypoxia-inducible factor 1 in a reactive oxygen species-dependent manner. Sci. Rep. 2016, 6, srep34424. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Karuga, F.F.; Szmyd, B.; Białasiewicz, P. HIF-1α as a Mediator of Insulin Resistance, T2DM, and Its Complications: Potential Links With Obstructive Sleep Apnea. Front. Physiol. 2020, 11, 1035. [Google Scholar] [CrossRef] [PubMed]
- Series, F.; Roy, N.; Marc, I. Effects of sleep deprivation and sleep fragmentation on upper airway collapsibility in normal subjects. Am. J. Respir. Crit. Care Med. 1994, 150, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Wetter, D.; Young, T. The Relation Between Cigarette Smoking and Sleep Disturbance. Prev. Med. 1994, 23, 328–334. [Google Scholar] [CrossRef]
- Phillips, B.A.; Danner, F.J. Cigarette smoking and sleep disturbance. Arch. Intern. Med. 1995, 155, 734–737. [Google Scholar] [CrossRef]
- McNamara, J.P.; Wang, J.; Holiday, D.B.; Warren, J.Y.; Paradoa, M.; Balkhi, A.M.; Fernandez-Baca, J.; McCrae, C. Sleep disturbances associated with cigarette smoking. Psychol. Health Med. 2013, 19, 410–419. [Google Scholar] [CrossRef]
- Zhang, L.; Samet, J.; Caffo, B.; Punjabi, N.M. Cigarette Smoking and Nocturnal Sleep Architecture. Am. J. Epidemiol. 2006, 164, 529–537. [Google Scholar] [CrossRef]
- Zhang, L.; Samet, J.; Caffo, B.; Bankman, I.; Punjabi, N.M. Power Spectral Analysis of EEG Activity During Sleep in Cigarette Smokers. Chest 2008, 133, 427–432. [Google Scholar] [CrossRef]
- Jaehne, A.; Unbehaun, T.; Feige, B.; Lutz, U.C.; Batra, A.; Riemann, D. How smoking affects sleep: A polysomnographical analysis. Sleep Med. 2012, 13, 1286–1292. [Google Scholar] [CrossRef]
- Conway, S.; Roizenblatt, S.; Palombini, L.; Castro, L.; Bittencourt, L.; Silva, R.; Tufik, S. Effect of smoking habits on sleep. Braz. J. Med Biol. Res. 2008, 41, 722–727. [Google Scholar] [CrossRef]
- Eckert, D.J.; Younes, M.K. Arousal from sleep: Implications for obstructive sleep apnea pathogenesis and treatment. J. Appl. Physiol. 2014, 116, 302–313. [Google Scholar] [CrossRef] [PubMed]
- DiFranza, J.R.; Aligne, C.A.; Weitzman, M. Prenatal and Postnatal Environmental Tobacco Smoke Exposure and Children’s Health. Pediatrics 2004, 113, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.S.; Parslow, P.M.; Ferens, D.; Bandopadhayay, P.; Osborne, A.; Watts, A.-M.; Cranage, S.M.; Adamson, T. Arousal responses and risk factors for sudden infant death syndrome. Sleep Med. 2002, 3, S61–S65. [Google Scholar] [CrossRef]
- St-Hilaire, M.; Duvareille, C.; Avoine, O.; Carreau, A.M.; Samson, N.; Micheau, P.; Doueik, A.; Praud, J.P. Effects of postnatal smoke exposure on laryngeal chemorefl exes in newborn lambs. J. Appl. Physiol. 2010, 109, 1820–1826. [Google Scholar] [CrossRef] [PubMed]
- Kashyap, R.; Hock, L.M.; Bowman, T.J. Higher prevalence of smoking in patients diagnosed as having obstructive sleep apnea. Sleep Breath. 2001, 5, 167–172. [Google Scholar] [CrossRef]
- Boussoffara, L.; Boudawara, N.; Sakka, M.; Knani, J. Smoking habits and severity of obstructive sleep apnea hypopnea syndrome. Rev. Mal. Respir. 2013, 30, 38–43. [Google Scholar] [CrossRef]
- Varol, Y.; Anar, C.; Tuzel, O.E.; Guclu, S.Z.; Ucar, Z.Z. The impact of active and former smoking on the severity of obstructive sleep apnea. Sleep Breath. 2015, 19, 1279–1284. [Google Scholar] [CrossRef]
- Bielicki, P.; Trojnar, A.; Sobieraj, P.; Wąsik, M. Smoking Status in Relation to Obstructive Sleep Apnea Severity (OSA) And Cardiovascular Comorbidity in Patients with Newly Diagnosed OSA. Adv. Respir. Med. 2019, 87, 103–109. [Google Scholar] [CrossRef]
- Yosunkaya, S.; Kutlu, R.; Vatansev, H. Effects of smokıng on patıents wıth obstructıve sleep apnea syndrome. Clin. Respir. J. 2021, 15, 147–153. [Google Scholar] [CrossRef]
- Ioannidou, D.; Kalamaras, G.; Kotoulas, S.-C.; Pataka, A. Smoking and Obstructive Sleep Apnea: Is There An Association between These Cardiometabolic Risk Factors?—Gender Analysis. Medicina 2021, 57, 1137. [Google Scholar] [CrossRef]
- Casasola, G.G.; Alvarez-Sala, J.L.; Marques, J.A.; Sánchez-Alarcos, J.M.F.; Tashkin, D.P.; Espinós, D. Cigarette smoking behavior and respiratory alterations during sleep in a healthy population. Sleep Breath. 2002, 6, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Nieto, F.J.; Young, T.B.; Lind, B.K.; Shahar, E.; Samet, J.M.; Redline, S.; D’Agostino, R.B.; Newman, A.B.; Lebowitz, M.D.; Pickering, T.G.; et al. Association of Sleep-Disordered Breathing, Sleep Apnea, and Hypertension in a Large Community-Based Study. JAMA 2000, 283, 1829–1836. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Lin, B.M.; Markt, S.; Stampfer, M.J.; Laden, F.; Hu, F.B.; Tworoger, S.S.; Redline, S. Sex differences in the associations of obstructive sleep apnoea with epidemiological factors. Eur. Respir. J. 2018, 51, 1702421. [Google Scholar] [CrossRef] [PubMed]
- Hoflstein, V. Relationship between smoking and sleep apnea in clinic population. Sleep 2002, 25, 519–524. [Google Scholar] [PubMed]
- Hsu, W.-Y.; Chiu, N.-Y.; Chang, C.-C.; Chang, T.-G.; Lane, H.-Y. The association between cigarette smoking and obstructive sleep apnea. Tob. Induc. Dis. 2019, 17, 27. [Google Scholar] [CrossRef] [PubMed]
- Shao, C.; Qi, H.; Fang, Q.; Tu, J.; Li, Q.; Wang, L. Smoking history and its relationship with comorbidities in patients with obstructive sleep apnea. Tob. Induc. Dis. 2020, 18, 56. [Google Scholar] [CrossRef]
- Taveira, K.V.M.; Kuntze, M.M.; Berretta, F.; De Souza, B.D.M.; Godolfim, L.R.; Demathe, T.; Canto, G.D.L.; Porporatti, A.L. Association between obstructive sleep apnea and alcohol, caffeine and tobacco: A meta-analysis. J. Oral Rehabil. 2018, 45, 890–902. [Google Scholar] [CrossRef]
- Balfour, D.J. Neuroplasticity within the Mesoaccumbens Dopamine System and its Role in Tobacco Dependence. Curr. Drug Target-CNS Neurol. Disord. 2002, 1, 413–421. [Google Scholar] [CrossRef]
- Guzmαn-Marνn, R.; Alam, M.N.; Mihailescu, S.; Szymusiak, R.; McGinty, D.; Drucker-Colνn, R. Subcutaneous administration of nicotine changesdorsal raphe serotonergic neurons discharge rate during REM sleep. Brain Res. 2001, 888, 321–325. [Google Scholar] [CrossRef]
- Fidone, S.; Gonzalez, C.; Yoshizaki, K. Effects of low oxygen on the release of dopamine from the rabbit carotid body in vitro. J. Physiol. 1982, 333, 93–110. [Google Scholar] [CrossRef]
- Collins, A.C. Genetic influences on tobacco use: A review of human and animal studies. Int. J. Addict. 1990, 25, 35–55. [Google Scholar] [CrossRef] [PubMed]
- LaRowe, L.R.; Ditre, J.W. Pain, nicotine, and tobacco smoking: Current state of the science. Pain 2020, 161, 1688–1693. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarski, P.; Karuga, F.F.; Szmyd, B.; Sochal, M.; Białasiewicz, P.; Strzelecki, D.; Gabryelska, A. The Role of Inflammation, Hypoxia, and Opioid Receptor Expression in Pain Modulation in Patients Suffering from Obstructive Sleep Apnea. Int. J. Mol. Sci. 2022, 23, 9080. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, D. The possible contribution of neuronal nicotinic acetylcholine receptors in depression. Dialogues Clin. Neurosci. 2005, 7, 207–216. [Google Scholar] [CrossRef]
- Hughes, J.R. Effects of abstinence from tobacco: Valid symptoms and time course. Nicotine Tob. Res. 2007, 9, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Jaehne, A.; Loessl, B.; Bárkai, Z.; Riemann, D.; Hornyak, M. Effects of nicotine on sleep during consumption, withdrawal and replacement therapy. Sleep Med. Rev. 2009, 13, 363–377. [Google Scholar] [CrossRef]
- Riedel, B.W.; Durrence, H.H.; Lichstein, K.L.; Taylor, D.J.; Bush, A.J. The Relation Between Smoking and Sleep: The Influence of Smoking Level, Health, and Psychological Variables. Behav. Sleep Med. 2004, 2, 63–78. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Kales, J.D.; Scharf, M.B.; Bixler, E.O.; Kales, A. Cigarette Smoking Associated with Sleep Difficulty. Science 1980, 207, 551–553. [Google Scholar] [CrossRef]
- Prosise, G.L.; Bonnet, M.H.; Berry, R.B.; Dickel, M.J. Effects of Abstinence from Smoking on Sleep and Daytime Sleepiness. Chest 1994, 105, 1136–1141. [Google Scholar] [CrossRef]
- Cummings, K.; Giovino, G.; Jaén, C.R.; Emrich, L.J. Reports of smoking withdrawal symptoms over a 21 day period of abstinence. Addict. Behav. 1985, 10, 373–381. [Google Scholar] [CrossRef]
- Patterson, F.; Grandner, M.; Malone, S.K.; Rizzo, A.; Davey, A.; Edwards, D.G. Sleep as a Target for Optimized Response to Smoking Cessation Treatment. Nicotine Tob. Res. 2017, 21, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Colrain, I.M.; Trinder, J.; Swan, G.E. The impact on smoking cessation on objective and subjective markers of sleep: Review, synthesis and recommendations. Nicotine Tob. Res. 2004, 6, 913–925. [Google Scholar] [CrossRef] [PubMed]
- Salin-Pascual, R.J. Effects of nicotine replacement therapies on sleep. Sleep Med. 2006, 7, 105–106. [Google Scholar] [CrossRef] [PubMed]
- Burgess, E.S.; Brown, R.A.; Kahler, C.W.; Niaura, R.; Abrams, D.B.; Goldstein, M.G.; Miller, I.W. Patterns of change in depressive symptoms during smoking cessation: Who’s at risk for relapse? J. Consult. Clin. Psychol. 2002, 70, 356–361. [Google Scholar] [CrossRef]
- Barua, R.S.; Rigotti, N.A.; Benowitz, N.L.; Cummings, K.M.; Jazayeri, M.A.; Morris, P.B.; Ratchford, E.V.; Sarna, L.; Stecker, E.C.; Wiggins, B.S. ACC Expert Consensus Decision Pathway on Tobacco Cessation Treatment: A Report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J. Am. Coll. Cardiol. 2018, 72, 3332–3365. [Google Scholar] [CrossRef]
- Wetter, D.W.; Fiore, M.C.; Baker, T.B.; Young, T.B. Tobacco withdrawal and nicotine replacement influence objective measures of sleep. J. Consult. Clin. Psychol. 1995, 63, 658–667. [Google Scholar] [CrossRef]
- Staner, L.; Luthringer, R.; Dupont, C.; Aubin, H.; Lagrue, G. Sleep effects of a 24-h versus a 16-h nicotine patch: A polysomnographic study during smoking cessation. Sleep Med. 2006, 7, 147–154. [Google Scholar] [CrossRef]
- Gillin, J.C.; Lardon, M.; Ruiz, C.; Golshan, S.; Salin-Pascual, R. Dose-dependent effects of transdermal nicotine on early morning awakening and rapid eye movement sleep time in non-smoking normal volunteers. J. Clin. Psychopharmacol. 1994, 14, 264–267. [Google Scholar] [CrossRef]
- Imperial Cancer Research Fund General Practice Research Group. Effectiveness of a nicotine patch in helping people stop smoking: Results of a randomized trial in general practice. BMJ 1993, 306, 1304–1308. [Google Scholar] [CrossRef]
- Gourlay, S.G.; Forbes, A.; Marriner, T.; Pethica, D.; McNeil, J.J. Double blind trial of repeated treatment with nicotine patch for relapsed smokers. BMJ 1995, 311, 363–366. [Google Scholar] [CrossRef]
- Jorenby, D.E.; Hatsukami, D.K.; Smith, S.S.; Fiore, M.C.; Allen, S.; Jensen, J.; Baker, T.B. Characterization of tobacco withdrawal symptoms: Transdermal nicotine reduces hunger and weight gain. Psychopharmacology 1996, 128, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, P.A.; Lee, G.M.; Wingender, L.; Hurt, R.D.; Croghan, I.T.; Lauger, G.; Offord, K.P.; Gomez-Dahl, L. High dose transdermal nicotine therapy for heavy smokers: Safety, tolerability and measurement of nicotine and cotinine levels. Psychopharmacology 1995, 122, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Rieder, A.; Kunze, U.; Groman, E.; Kiefer, I.; Schoberberger, R. Nocturnal sleep-disturbing nicotine craving: A newly described symptom of extreme nicotine dependence. Acta Med. Austriaca 2001, 28, 21–22. [Google Scholar] [CrossRef] [PubMed]
- Page, F.; Coleman, G.; Conduit, R. The effect of transdermal nicotine patches on sleep and dreams. Physiol. Behav. 2006, 88, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Johansson, C.J.; Olsson, P.; Gunnarsson, P.O.; Saewe, U. Pharmacokinetics of a 16 hour transdermal nicotine patch. Clin. Drug Investig. 1996, 12, 198–206. [Google Scholar] [CrossRef]
- Aubin, H.-J.; Luthringer, R.; Demazières, A.; Dupont, C.; Lagrue, G. Comparison of the effects of a 24-hour nicotine patch and a 16-hour nicotine patch on smoking urges and sleep. Nicotine Tob. Res. 2006, 8, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Gothe, B.; Strohl, K.P.; Levin, S.; Cherniack, N.S. Nicotine: A Different Approach to Treatment of Obstructive Sleep Apnea. Chest 1985, 87, 11–17. [Google Scholar] [CrossRef]
- Davila, D.G.; Hurt, R.D.; Offord, K.P.; Harris, C.D.; Shepard, J.W. Acute effects of transdermal nicotine on sleep architecture, snoring, and sleep-disordered breathing in nonsmokers. Am. J. Respir. Crit. Care Med. 1994, 150, 469–474. [Google Scholar] [CrossRef]
- Zevin, S.; Swed, E.; Cahan, C. Clinical Effects of Locally Delivered Nicotine in Obstructive Sleep Apnea Syndrome. Am. J. Ther. 2003, 10, 170–175. [Google Scholar] [CrossRef]
- Huecker, M.R.; Smiley, A.; Saadabadi, A. Bupropion. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470212/ (accessed on 25 June 2022).
- Leone, F.T.; Zhang, Y.; Evers-Casey, S.; Evins, A.E.; Eakin, M.N.; Fathi, J.; Fennig, K.; Folan, P.; Galiatsatos, P.; Gogineni, H.; et al. Initiating Pharmacologic Treatment in Tobacco-Dependent Adults. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2020, 202, e5–e31. [Google Scholar] [CrossRef]
- Bayard, M.; Bailey, B.; Acharya, D.; Ambreen, F.; Duggal, S.; Kaur, T.; Roller, K.; Tudiver, F.; Rahman, Z.U. Bupropion and Restless Legs Syndrome: A Randomized Controlled Trial. J. Am. Board Fam. Med. 2011, 24, 422–428. [Google Scholar] [CrossRef] [PubMed]
- McCall, C.A.; Winkelman, J.W. Respiratory-Related Leg Movements of Sleep Are Associated with Serotonergic Antidepressants But Not Bupropion. J. Clin. Sleep Med. 2018, 14, 1569–1576. [Google Scholar] [CrossRef] [PubMed]
- McCarter, S.J.; Howell, M.J. Importance of Rapid Eye Movement Sleep Behavior Disorder to the Primary Care Physician. Mayo Clin. Proc. 2016, 91, 1460–1466. [Google Scholar] [CrossRef] [PubMed]
- Gandotra, K.; Jaskiw, G.E.; Williams, S.G.; Fuller, M.A.; Chen, P.; Wilson, B.; ElGhoul, R.; Konicki, E.; Strohl, K.P. Development of Insomnia Associated with Different Formulations of Bupropion. Prim. Care Companion CNS Disord. 2021, 23, 20br02621. [Google Scholar] [CrossRef]
- Nofzinger, E.A.; Reynolds, C.F.; Thase, M.E.; Frank, E.; Jennings, J.R.; Fasiczka, A.L.; Sullivan, L.R.; Kupfer, D.J. REM sleep enhancement by bupropion in depressed men. Am. J. Psychiatry 1995, 152, 274–276. [Google Scholar]
- Tonstad, S.; Tønnesen, P.; Hajek, P.; Williams, K.E.; Billing, C.B.; Reeves, K.R.; for the Varenicline Phase 3 Study Group. Effect of Maintenance Therapy with Varenicline on Smoking Cessation: A Randomized Controlled Trial. JAMA 2006, 296, 64–71. [Google Scholar] [CrossRef]
- Coe, J.W.; Brooks, P.R.; Vetelino, M.G. An alpha4-beta2 nicotine receptor partial agonist for smoking cessation. J. Med. Chem. 2005, 48, 3474–3477. [Google Scholar] [CrossRef]
- Thomas, K.H.; Martin, R.M.; Knipe, D.W.; Higgins, J.P.T.; Gunnell, D. Risk of neuropsychiatric adverse events associated with varenicline: Systematic review and meta-analysis. BMJ 2015, 350, 1109. [Google Scholar] [CrossRef]
- Foulds, J.; Russ, C.; Yu, C.-R.; Zou, K.H.; Galaznik, A.; Franzon, M.; Berg, A.; Hughes, J.R. Effect of Varenicline on Individual Nicotine Withdrawal Symptoms: A Combined Analysis of Eight Randomized, Placebo-Controlled Trials. Nicotine Tob. Res. 2013, 15, 1849–1857. [Google Scholar] [CrossRef]
- Savage, R.L.; Zekarias, A.; Caduff-Janosa, P. Varenicline and Abnormal Sleep Related Events. Sleep 2015, 38, 833–837. [Google Scholar] [CrossRef]
- Polini, F.; Principe, R.; Scarpelli, S.; Clementi, F.; De Gennaro, L. Use of varenicline in smokeless tobacco cessation influences sleep quality and dream recall frequency but not dream affect. Sleep Med. 2016, 30, 1–6. [Google Scholar] [CrossRef]
- Htoo, A.; Talwar, A.; Feinsilver, S.; Greenberg, H. Smoking and sleep disorders. Med Clin. N. Am. 2004, 88, 1575–1591. [Google Scholar] [CrossRef] [PubMed]
- Romigi, A.; Vitrani, G. Improvement of Restless Legs Syndrome by Varenicline as Antismoking Treatment. J. Clin. Sleep Med. 2013, 9, 1089–1090. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pataka, A.; Frantzidis, C.; Kalamaras, G.; Gkivogkli, P.; Kotoulas, S.; Nday, C.; Chriskos, P.; Karagianni, M.; Styliadis, C.; Paraskevopoulos, E.; et al. Varenicline administration for smoking cessation may reduce apnea hypopnea index in sleep apnea patients. Sleep Med. 2021, 88, 87–89. [Google Scholar] [CrossRef] [PubMed]
- FDA Updates and Press Announcements on Nitrosamine in Varenicline (Chantix). Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-updates-and-press-announcements-nitrosamine-varenicline-chantix (accessed on 10 June 2022).
- Buysse, D.J.; Reynolds, C.F., 3rd; Hoch, C.C.; Houck, P.R.; Kupfer, D.J.; Mazumdar, S.; Frank, E. Longitudinal effects of nortriptyline on EEG sleep and the likelihood of recurrence in elderly depressed patients. Neuropsychopharmacology 1996, 14, 243–252. [Google Scholar] [CrossRef]
- Smith, P.L.; Haponik, E.F.; Allen, R.P.; Bleecker, E.R. The Effects of Protriptyline in Sleep-Disordered Breathing. Am. Rev. Respir. Dis. 1983, 127, 8–13. [Google Scholar] [CrossRef]
- Brownell, L.G.; West, P.; Sweatman, P.; Acres, J.C.; Kryger, M.H. Protriptyline in obstructive sleep apnea: A double-blind trial. N. Engl. J. Med. 1982, 307, 1037–1042. [Google Scholar] [CrossRef]
- Sharma, A.; Gupta, L. Clonidine a Wonder Drug. Indian J. Anesth. Analg. 2019, 6, 2057–2062. [Google Scholar] [CrossRef]
- Issa, F.G. Effect of Clonidine in Obstructive Sleep Apnea. Am. Rev. Respir. Dis. 1992, 145, 435–439. [Google Scholar] [CrossRef]
- Gotti, C.; Clementi, F. Cytisine and cytisine derivatives. More than smoking cessation aids. Pharmacol. Res. 2021, 170, 105700. [Google Scholar] [CrossRef]
- Etter, F. Cytisine for smoking cessation: A literature review and a meta-analysis. Arch. Intern. Med. 2006, 166, 1553–1559. [Google Scholar] [CrossRef] [PubMed]
- Walker, N.; Howe, C.; Glover, M.; McRobbie, H.; Barnes, J.; Nosa, V.; Parag, V.; Bassett, B.; Bullen, C. Cytisine versus Nicotine for Smoking Cessation. N. Engl. J. Med. 2014, 371, 2353–2362. [Google Scholar] [CrossRef] [PubMed]
- Courtney, R.J.; McRobbie, H.; Tutka, P.; Weaver, N.A.; Petrie, D.; Mendelsohn, C.P.; Shakeshaft, A.; Talukder, S.; Macdonald, C.; Thomas, D.; et al. Effect of Cytisine vs Varenicline on Smoking Cessation: A Randomized Clinical Trial. JAMA 2021, 326, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.G.; Mendez-Galvez, C.; Cassels, B.K. Cytisine: A natural product lead for the development of drugs acting at nicotinic acetylcholine receptors. Nat. Prod. Rep. 2012, 29, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Williamson, D.F.; Madans, J.; Anda, R.F.; Kleinman, J.C.; Giovino, G.A.; Byers, T. Smoking Cessation and Severity of Weight Gain in a National Cohort. N. Engl. J. Med. 1991, 324, 739–745. [Google Scholar] [CrossRef]
- Hornyak, M.; Feige, B.; Riemann, D.; Voderholzer, U. Periodic leg movements in sleep and periodic limb movement disorder: Prevalence, clinical significance and treatment. Sleep Med. Rev. 2006, 10, 169–177. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Roth, T. Prevalence of restless legs syndrome and periodic limb movement disorder in the general population. J. Psychosom. Res. 2002, 53, 547–554. [Google Scholar] [CrossRef]


{kind=link}
| NRT—smoking cessation |
|
| NRT—OSA treatment |
|
| Bupropion | |
| Varenicline | |
| Nortriptyline | |
| Clonidine |
|
| Cytisine |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pataka, A.; Kotoulas, S.; Kalamaras, G.; Tzinas, A.; Grigoriou, I.; Kasnaki, N.; Argyropoulou, P. Does Smoking Affect OSA? What about Smoking Cessation? J. Clin. Med. 2022, 11, 5164. https://doi.org/10.3390/jcm11175164
Pataka A, Kotoulas S, Kalamaras G, Tzinas A, Grigoriou I, Kasnaki N, Argyropoulou P. Does Smoking Affect OSA? What about Smoking Cessation? Journal of Clinical Medicine. 2022; 11(17):5164. https://doi.org/10.3390/jcm11175164
Chicago/Turabian StylePataka, Athanasia, Seraphim Kotoulas, George Kalamaras, Asterios Tzinas, Ioanna Grigoriou, Nectaria Kasnaki, and Paraskevi Argyropoulou. 2022. "Does Smoking Affect OSA? What about Smoking Cessation?" Journal of Clinical Medicine 11, no. 17: 5164. https://doi.org/10.3390/jcm11175164
APA StylePataka, A., Kotoulas, S., Kalamaras, G., Tzinas, A., Grigoriou, I., Kasnaki, N., & Argyropoulou, P. (2022). Does Smoking Affect OSA? What about Smoking Cessation? Journal of Clinical Medicine, 11(17), 5164. https://doi.org/10.3390/jcm11175164