
Increased Carcinoembryonic Antigen (CEA) Level Is Highly Associated with Low Skeletal Muscle Mass in Asymptomatic Adults: A Population-Based Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
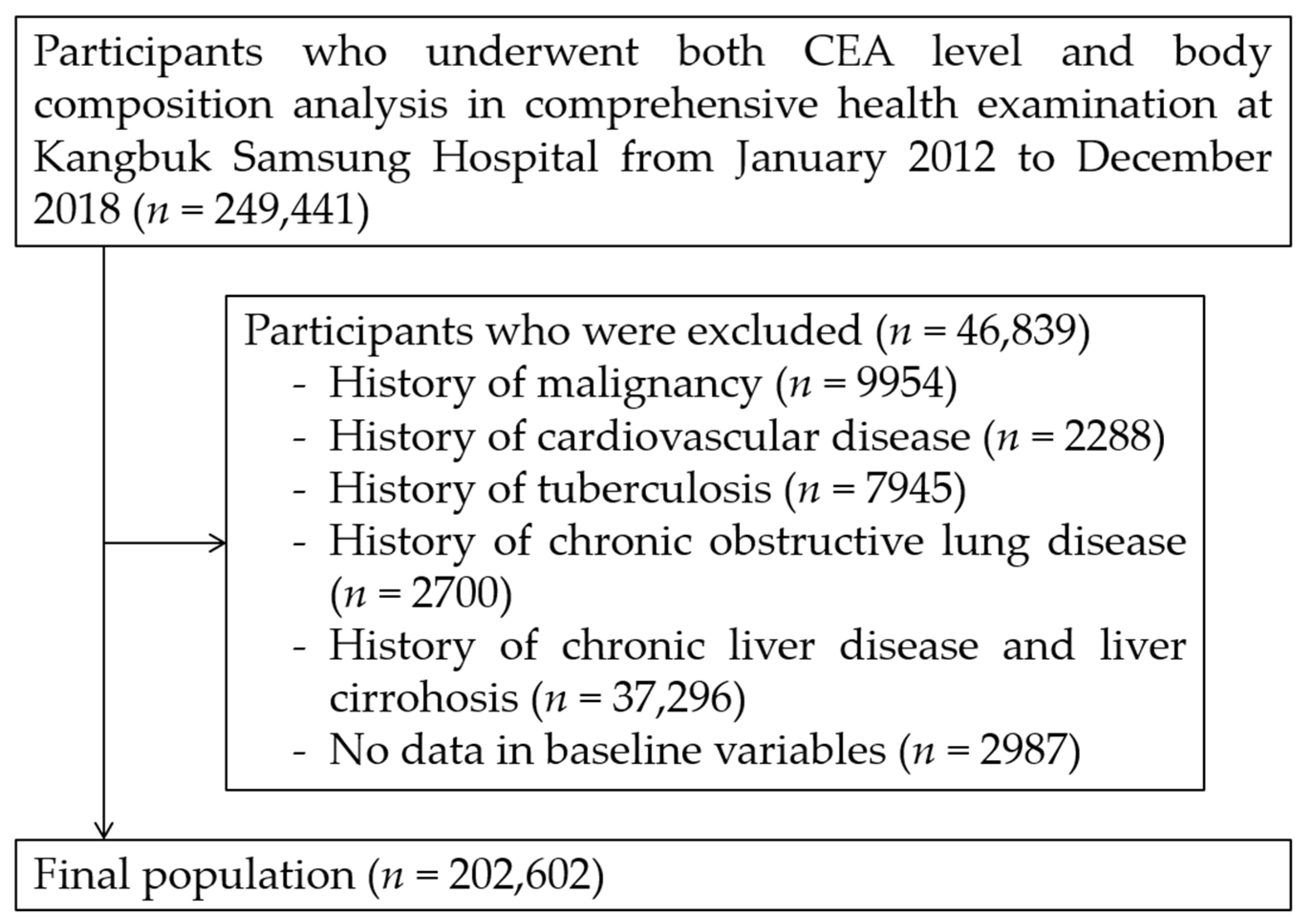
2.1. Study Population
2.2. Data Collection and Classification of Participants
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Comparison of CEA Levels between Subjects Classified by Skeletal Muscle Mass
3.3. Association between High CEA Levels and LMM
3.4. Subgroup Analysis by Age and Sex
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hall, C.; Clarke, L.; Pal, A.; Buchwald, P.; Eglinton, T.; Wakeman, C.; Frizelle, F. A review of the role of carcinoembryonic antigen in clinical practice. Ann. Coloproctol. 2019, 35, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Ishizaka, N.; Ishizaka, Y.; Toda, E.; Koike, K.; Yamakado, M.; Nagai, R. Are serum carcinoembryonic antigen levels associated with carotid atherosclerosis in Japanese men? Arterioscler. Thromb Vasc. Biol. 2008, 28, 160–165. [Google Scholar] [CrossRef] [PubMed][Green Version]
- No, J.I.; Yang, J.Y.; Hyun, H.J.; Yeon, C.S.; Choi, H.J. Factors associated with serum levels of carcinoembryonic antigen in healthy non-smokers. Korean J. Fam. Med. 2013, 34, 413–419. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yang, Y.; Xu, M.; Huang, H.; Jiang, X.; Gong, K.; Liu, Y.; Kuang, X.; Yang, X. Serum carcinoembryonic antigen elevation in benign lung diseases. Sci. Rep. 2021, 11, 19044. [Google Scholar] [CrossRef]
- Clarke, C.; Hine, K.R.; Dykes, P.W.; Whitehead, T.P.; Whitfield, A.G. Carcinoembryonic antigen and smoking. J. R. Coll. Physicians Lond. 1980, 14, 227–228. [Google Scholar]
- Park, J.S.; Choi, G.-S.; Jang, Y.S.; Jun, S.H.; Kang, H. Influence of Obesity on the Serum Carcinoembryonic Antigen Value in Patients with Colorectal CancerAssociation between BMI and CEA Value. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2461–2468. [Google Scholar] [CrossRef]
- Prado, C.M.; Purcell, S.A.; Alish, C.; Pereira, S.L.; Deutz, N.E.; Heyland, D.K.; Goodpaster, B.H.; Tappenden, K.A.; Heymsfield, S.B. Implications of low muscle mass across the continuum of care: A narrative review. Ann. Med. 2018, 50, 675–693. [Google Scholar] [CrossRef]
- Tuttle, C.S.L.; Thang, L.A.N.; Maier, A.B. Markers of inflammation and their association with muscle strength and mass: A systematic review and meta-analysis. Ageing Res. Rev. 2020, 64, 101185. [Google Scholar] [CrossRef]
- Favier, F.B.; Benoit, H.; Freyssenet, D. Cellular and molecular events controlling skeletal muscle mass in response to altered use. Pflug. Arch. 2008, 456, 587–600. [Google Scholar] [CrossRef]
- Li, Z.; Tong, X.; Ma, Y.; Bao, T.; Yue, J. Relationship between Low skeletal muscle mass and arteriosclerosis in western China: A cross-sectional study. Front. Cardiovasc. Med. 2021, 8, 735262. [Google Scholar] [CrossRef]
- Aleman-Mateo, H.; Ruiz Valenzuela, R.E. Skeletal muscle mass indices in healthy young Mexican adults aged 20–40 years: Implications for diagnoses of sarcopenia in the elderly population. Sci. World J. 2014, 2014, 672158. [Google Scholar]
- Aarons, C.B.; Bajenova, O.; Andrews, C.; Heydrick, S.; Bushell, K.N.; Reed, K.L.; Thomas, P.; Becker, J.M.; Stucchi, A.F. Carcinoembryonic antigen-stimulated THP-1 macrophages activate endothelial cells and increase cell-cell adhesion of colorectal cancer cells. Clin. Exp. Metastasis 2007, 24, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Akil, E.; Bulut, A.; Kaplan, I.; Ozdemir, H.H.; Arslan, D.; Aluclu, M.U. The increase of carcinoembryonic antigen (CEA), high-sensitivity C-reactive protein, and neutrophil/lymphocyte ratio in Parkinson’s disease. Neurol. Sci. 2015, 36, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghurabi, B.H.; Al-Hassan, A.A.; Ghazi, H.F. Serum CEA and IL-6 levels in patients with ulcerative colitis. Al-Mustansiriyah J. Sci. 2009, 20, 1–7. [Google Scholar]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef]
- Feliciano, E.M.C.; Kroenke, C.H.; Meyerhardt, J.A.; Prado, C.M.; Bradshaw, P.T.; Kwan, M.L.; Xiao, J.; Alexeeff, S.; Corley, D.; Weltzien, E.; et al. Association of systemic inflammation and sarcopenia with survival in nonmetastatic colorectal cancer: Results from the C SCANS study. JAMA Oncol. 2017, 3, e172319. [Google Scholar] [CrossRef]
- Chang, Y.; Ryu, S.; Sung, K.-C.; Cho, Y.K.; Sung, E.; Kim, H.-N.; Jung, H.-S.; Yun, K.E.; Ahn, J.; Shin, H. Alcoholic and non-alcoholic fatty liver disease and associations with coronary artery calcification: Evidence from the Kangbuk Samsung Health Study. Gut 2019, 68, 1667–1675. [Google Scholar] [CrossRef]
- Kwon, H.; Cho, J.H.; Lee, D.Y.; Park, S.E.; Park, C.Y.; Lee, W.Y.; Oh, K.W.; Park, S.W.; Rhee, E.J. Association between thyroid hormone levels, body composition and insulin resistance in euthyroid subjects with normal thyroid ultrasound: The Kangbuk Samsung Health Study. Clin. Endocrinol. 2018, 89, 649–655. [Google Scholar] [CrossRef]
- Lee, W.; Chang, Y.; Shin, H.; Ryu, S. Self-reported and cotinine-verified smoking and increased risk of incident hearing loss. Sci. Rep. 2021, 11, 8103. [Google Scholar] [CrossRef]
- Traversy, G.; Chaput, J.P. Alcohol consumption and obesity: An update. Curr. Obes. Rep. 2015, 4, 122–130. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Baumgartner, R.N.; Ross, R. Estimation of skeletal muscle mass by bioelectrical impedance analysis. J. Appl. Physiol. 2000, 89, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Newman, A.B.; Kupelian, V.; Visser, M.; Simonsick, E.; Goodpaster, B.; Nevitt, M.; Kritchevsky, S.B.; Tylavsky, F.A.; Rubin, S.M.; Harris, T.B.; et al. Sarcopenia: Alternative definitions and associations with lower extremity function. J. Am. Geriatr. Soc. 2003, 51, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef]
- Budd, J.R.; Durham, A.P.; Gwise, T.E.; Iriarte, B.; Kallner, A.; Linnet, K.; Magari, R.; Vaks, J.E. Measurement Procedure Comparison and Bias Estimation Using Patient Samples; Approved Guideline (EP09-A3), 3rd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2013. [Google Scholar]
- McEnroe, R.J.; Durham, A.P.G.; Goldford, M.D.; Kondratovich, M.V.; Lababidi, S.; Magari, R.; Middle, J.G.; Pierson-Perry, J.F.; Vaks, J.E. Evaluation of Precision of Quantitative Measurement Procedures; Approved Guideline (EP05-A3), 3rd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2014. [Google Scholar]
- Tholen, D.W.; Kroll, M.; Astles, J.R.; Caffo, A.L.; Happe, T.M.; Krouwer, J.; Lasky, F. Evaluation of the Linearity of Quantitative Measurement Procedures: A Statistical Approach; Approved Guideline (EP06-A), 2nd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2003. [Google Scholar]
- Saito, G.; Sadahiro, S.; Kamata, H.; Miyakita, H.; Okada, K.; Tanaka, A.; Suzuki, T. Monitoring of serum carcinoembryonic antigen levels after curative resection of colon cancer: Cutoff values determined according to preoperative levels enhance the diagnostic accuracy for recurrence. Oncology 2017, 92, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.J.; Kwon, M.J.; Woo, H.Y.; Park, H. Analysis of 25-hydroxyvitamin D status according to age, gender, and seasonal variation. J. Clin. Lab. Anal. 2016, 30, 905–911. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Shan, L.; Li, T.; Gu, W.; Gao, Y.; Zuo, E.; Qiu, H.; Li, R.; Cheng, X. Application of prognostic models based on psoas muscle index, stage, pathological grade, and preoperative carcinoembryonic antigen level in stage II–III colorectal cancer patients undergoing adjuvant chemotherapy. J. Oncol. 2022, 2022, 6851900. [Google Scholar] [CrossRef]
- Toth, C.A.; Thomas, P.; Broitman, S.A.; Zamcheck, N. Receptor-mediated endocytosis of carcinoembryonic antigen by rat liver Kupffer cells. Cancer Res. 1985, 45, 392–397. [Google Scholar]
- Li, W.; Moylan, J.S.; Chambers, M.A.; Smith, J.; Reid, M.B. Interleukin-1 stimulates catabolism in C2C12 myotubes. Am. J. Physiol. Cell Physiol. 2009, 297, C706–C714. [Google Scholar] [CrossRef]
- Reid, M.B.; Li, Y.P. Tumor necrosis factor-alpha and muscle wasting: A cellular perspective. Respir. Res. 2001, 2, 269–272. [Google Scholar] [CrossRef]
- Haddad, F.; Zaldivar, F.; Cooper, D.M.; Adams, G.R. IL-6-induced skeletal muscle atrophy. J. Appl. Physiol. 2005, 98, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, A.A.; Sheffield-Moore, M.; Yeckel, C.W.; Gilkison, C.; Jiang, J.; Achacosa, A.; Lieberman, S.A.; Tipton, K.; Wolfe, R.R.; Urban, R.J. Testosterone administration to older men improves muscle function: Molecular and physiological mechanisms. Am. J. Physiol. Endocrinol. Metab. 2002, 282, E601–E607. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.J.; Liu, H.; Garcia, J.M. Sex differences in muscle wasting. Adv. Exp. Med. Biol. 2017, 1043, 153–197. [Google Scholar] [PubMed]
- Blaak, E. Gender differences in fat metabolism. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Do, J.G.; Lee, Y.T.; Yoon, K.J. Sarcopenic obesity associated with high-sensitivity C-reactive protein in age and sex comparison: A two-center study in South Korea. BMJ Open 2018, 8, e021232. [Google Scholar] [CrossRef]
- Abellan van Kan, G. Epidemiology and consequences of sarcopenia. J. Nutr. Health Aging 2009, 13, 708–712. [Google Scholar] [CrossRef]
- Nogami, E.; Miyai, N.; Zhang, Y.; Sakaguchi, M.; Hayakawa, H.; Hattori, S.; Utsumi, M.; Uematsu, Y.; Arita, M. Association of cigarette smoking with muscle mass reduction and Low muscle strength in community-dwelling elderly men. Nihon Eiseigaku Zasshi 2021, 76, 21003. [Google Scholar] [CrossRef]
- Sekiya, K.; Sakai, T.; Homma, S.; Tojima, H. Pulmonary tuberculosis accompanied by a transient increase in serum carcinoembryonic antigen level with tuberculous empyema drainage. Intern. Med. 2007, 46, 1795–1798. [Google Scholar] [CrossRef][Green Version]
- Kashiwabara, K.; Nakamura, H.; Kiguchi, T.; Yagyu, H.; Yokoi, T.; Matsuoka, T. Chronological change of respiratory function in smokers with elevated serum carcinoembryonic antigen levels. Clin. Chim. Acta 1998, 28, 179–186. [Google Scholar] [CrossRef]
- Wu, S.; Gu, W. Association of T stage and serum CEA levels in determining survival of rectal cancer. Front. Med. 2019, 6, 270. [Google Scholar] [CrossRef]
- Loewenstein, M.S.; Zamcheck, N. Carcinoembryonic antigen (CEA) levels in benign gastrointestinal disease states. Cancer 1978, 42, 1412–1418. [Google Scholar] [CrossRef]
- Ko, I.G.; Park, E.M.; Choi, H.J.; Yoo, J.; Lee, J.K.; Jee, Y.S. Proper exercise decreases plasma carcinoembryonic antigen levels with the improvement of body condition in elderly women. Tohoku J. Exp. Med. 2014, 233, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Bahat, G.; Tufan, A.; Kilic, C.; Aydın, T.; Akpinar, T.S.; Kose, M.; Erten, N.; Karan, M.A.; Cruz-Jentoft, A.J. Cut-off points for height, weight and body mass index adjusted bioimpedance analysis measurements of muscle mass with use of different threshold definitions. Aging Male 2018, 23, 382–387. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total | Normal | Mild LMM | Severe LMM | * p Value | |
|---|---|---|---|---|---|
| Number of subjects (n) | 202,602 | 177,445 | 22,800 | 2357 | |
| Age (years) | 41.7 ± 9.4 | 41.7 ± 9.2 | 41.9 ± 10.8 | 44.7 ± 13.5 | <0.001 †,‡,# |
| Sex, Men | 49.5 | 48.4 | 55.9 | 67.2 | <0.001 † |
| Screening center, Seoul | 35.9 | 36.0 | 35.8 | 35.8 | 0.662 † |
| Height (cm) | 166.9 ± 8.6 | 167.2 ± 8.6 | 164.7 ± 8.1 | 163.3 ± 7.9 | <0.001 †,‡,# |
| BMI (kg/m2) | 23.5 ± 3.5 | 23.9 ± 3.4 | 20.6 ± 2.2 | 19.1 ± 2.1 | <0.001 †,‡,# |
| Appendicular skeletal muscle mass (kg) | 20.1 ± 4.9 | 20.5 ± 4.9 | 17.4 ± 4.0 | 15.9 ± 3.5 | <0.001 †,‡,# |
| SMI (kg/m2) | 7.1 ± 1.1 | 7.2 ± 1.1 | 6.3 ± 0.9 | 5.9 ± 0.8 | <0.001 †,‡,# |
| Current smoker | 13.8 | 13.6 | 15.0 | 19.4 | <0.001 † |
| Heavy drinking a | 18.0 | 18.1 | 17.2 | 19.2 | <0.001 † |
| Systolic blood pressure (mmHg) | 109.6 ± 12.7 | 110.1 ± 12.7 | 106.5 ± 12.0 | 106.9 ± 12.8 | <0.001 †,‡ |
| Diastolic blood pressure (mmHg) | 70.4 ± 9.7 | 70.6 ± 9.7 | 69.3 ±9.3 | 69.9 ± 9.3 | 0.002 †,‡,# |
| Hypertension | 8.7 | 8.8 | 7.9 | 10.0 | <0.001 † |
| Diabetes mellitus | 2.5 | 2.4 | 2.9 | 4.9 | <0.001 † |
| Insulin (mg/dL) | 7.2 ± 4.7 | 7.4 ± 4.9 | 5.8 ± 3.4 | 5.1 ± 3.0 | <0.001 †,‡,# |
| Glucose (mg/dL) | 96.9 ± 15.2 | 97.1 ± 15.0 | 95.8 ± 16.0 | 96.7 ± 19.9 | <0.001 †,# |
| Triglycerides (mg/dL) | 114.1 ± 79.4 | 115.7 ± 81.2 | 102.8 ± 64.2 | 100.9 ± 60.5 | <0.001 †,‡,# |
| Total cholesterol (mg/dL) | 190.8 ± 34.0 | 190.8 ± 33.9 | 190.8 ± 34.0 | 190.2 ± 35.9 | 0.428 |
| LDL-C (mg/dL) | 125.9 ±32.9 | 126.1±32.9 | 124.5±33.2 | 122.4 ±34.7 | <0.001 †,‡,# |
| HDL-C (mg/dL) | 60.9 ± 16.2 | 60.4 ± 16.1 | 64.1 ± 16.3 | 65.5 ± 17.5 | <0.001 †,‡,# |
| AST (IU/L) | 22.0 ± 14.0 | 22.1 ± 14.2 | 21.3 ± 11.0 | 23.4 ± 23.5 | <0.001 †,‡,# |
| ALT (IU/L) | 23.2 ± 19.5 | 23.5 ± 20.0 | 20.6 ± 14.6 | 21.1 ± 19.1 | <0.001 †,‡ |
| Creatinine (mg/dL) | 0.82 ± 0.22 | 0.82 ± 0.22 | 0.81 ± 0.19 | 0.82 ± 0.27 | <0.001 † |
| CRP (mg/dL) | 0.11 ± 0.30 | 0.12 ± 0.29 | 0.10 ± 0.31 | 0.13 ± 0.45 | 0.041 †,# |
| Normal | Mild LMM | Severe LMM | p for Trend | |
|---|---|---|---|---|
| Classification according to CEA level | <0.0001 | |||
| Normal CEA level (<5 ng/mL) (%) | 98.9 | 98.4 | 95.8 | |
| High CEA level (≥5 ng/mL) (%) | 1.1 | 1.6 | 4.2 |
| Mild LMM, OR (95% CI) | Severe LMM, OR (95% CI) | |
|---|---|---|
| Model 1 | ||
| Normal (<5 ng/mL) | 1 (reference) | 1 (reference) |
| High CEA level (≥5 ng/mL) | 1.357 (1.212–1.519) | 2.669 (2.165–3.290) |
| Model 2 | ||
| Normal (<5 ng/mL) | 1 (reference) | 1 (reference) |
| High CEA level (≥5 ng/mL) | 1.362 (1.207–1.537) | 2.820 (2.259–3.520) |
| Model 3 | ||
| Normal (<5 ng/mL) | 1 (reference) | 1 (reference) |
| High CEA level (≥5 ng/mL) | 1.139 (1.092–1.188) | 2.611 (2.055–3.319) |
| Mild LMM, OR (95% CI) | Severe LMM, OR (95% CI) | |
|---|---|---|
| Age, years | ||
| <40 (n = 95,817) | 1.255 (0.975–1.452) | 1.342 (1.301–1.398) |
| 40~59 (n= 97,466) | 1.047 (0.879–1.247) | 2.283 (1.638–3.182) |
| ≥60 (n = 9319) | 1.609 (1.184–2.185) | 3.149 (2.040–4.860) |
| Sex | ||
| Men (n = 100,278) | 1.261 (1.099–1.447) | 2.273 (1.762–2.933) |
| Women (n = 102,324) | 1.383 (0.933–2.049) | 5.373 (2.705–10.669) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, C.-H.; Lizarraga, A.D.; Lee, Y.-T.; Yoon, K.-J.; Yoo, T.-K. Increased Carcinoembryonic Antigen (CEA) Level Is Highly Associated with Low Skeletal Muscle Mass in Asymptomatic Adults: A Population-Based Study. J. Clin. Med. 2022, 11, 5009. https://doi.org/10.3390/jcm11175009
Park C-H, Lizarraga AD, Lee Y-T, Yoon K-J, Yoo T-K. Increased Carcinoembryonic Antigen (CEA) Level Is Highly Associated with Low Skeletal Muscle Mass in Asymptomatic Adults: A Population-Based Study. Journal of Clinical Medicine. 2022; 11(17):5009. https://doi.org/10.3390/jcm11175009
Chicago/Turabian StylePark, Chul-Hyun, Antonio Diaz Lizarraga, Yong-Taek Lee, Kyung-Jae Yoon, and Tae-Kyung Yoo. 2022. "Increased Carcinoembryonic Antigen (CEA) Level Is Highly Associated with Low Skeletal Muscle Mass in Asymptomatic Adults: A Population-Based Study" Journal of Clinical Medicine 11, no. 17: 5009. https://doi.org/10.3390/jcm11175009
APA StylePark, C.-H., Lizarraga, A. D., Lee, Y.-T., Yoon, K.-J., & Yoo, T.-K. (2022). Increased Carcinoembryonic Antigen (CEA) Level Is Highly Associated with Low Skeletal Muscle Mass in Asymptomatic Adults: A Population-Based Study. Journal of Clinical Medicine, 11(17), 5009. https://doi.org/10.3390/jcm11175009