

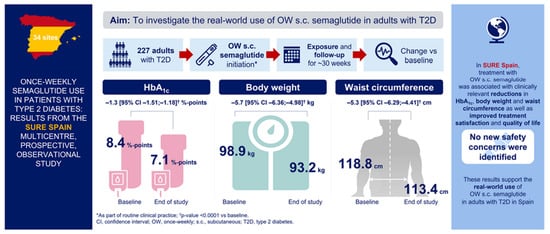
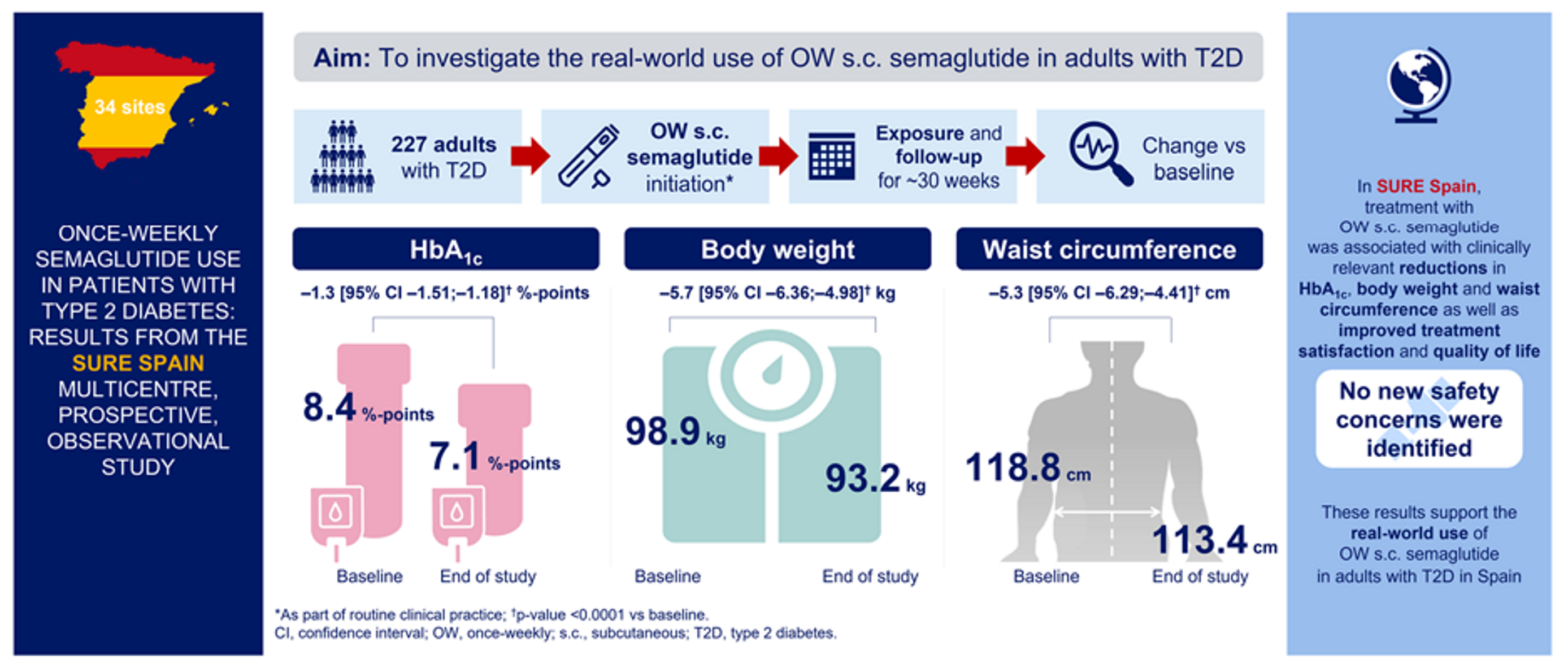
Once-Weekly Semaglutide Use in Patients with Type 2 Diabetes: Results from the SURE Spain Multicentre, Prospective, Observational Study
 , ,
, , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Endpoints
2.4. Safety
2.5. Statistical Analyses
3. Results
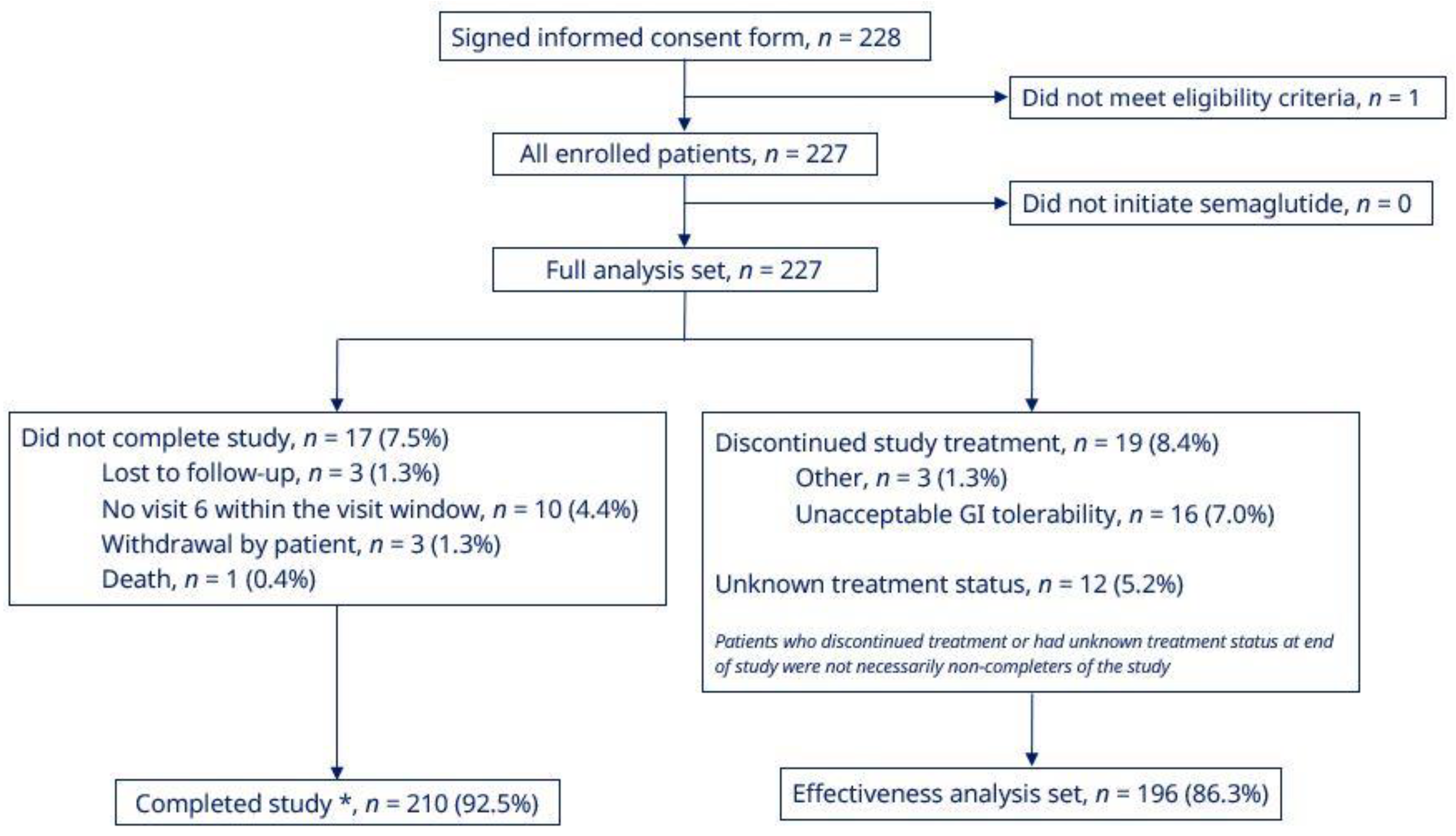
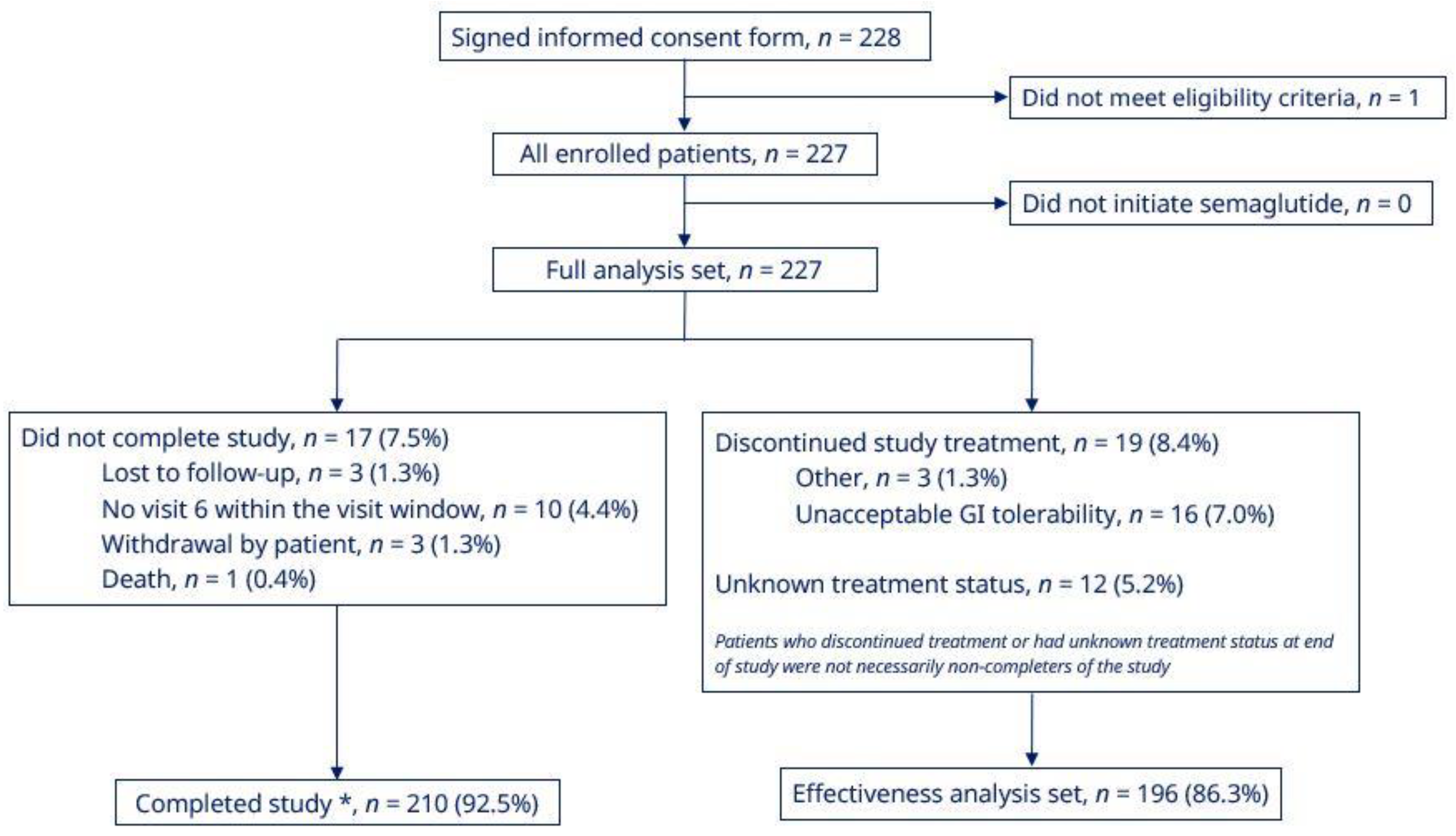
3.1. Patient Population and Baseline Characteristics
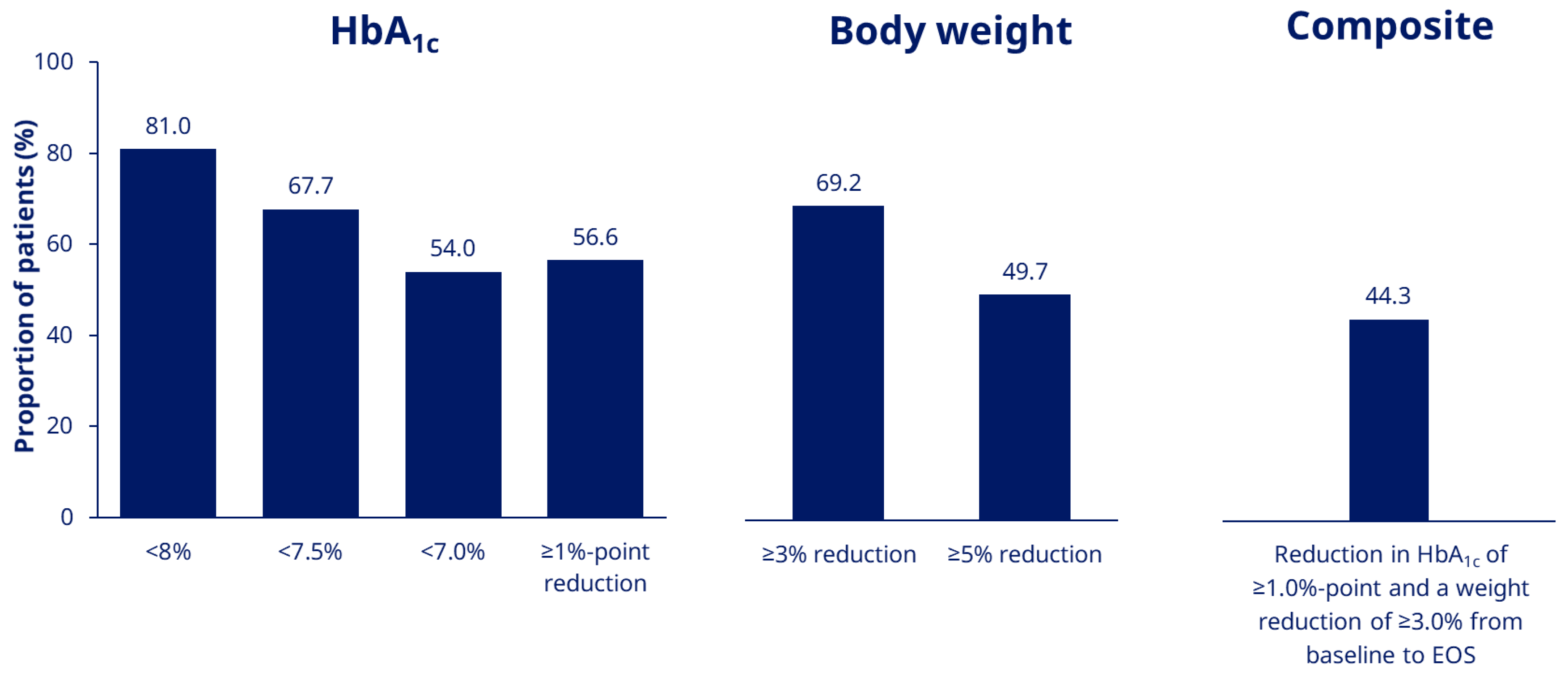
3.2. HbA1c, BW, BMI, and Waist Circumference Outcomes
3.3. Sensitivity Analyses
3.4. Semaglutide Dose
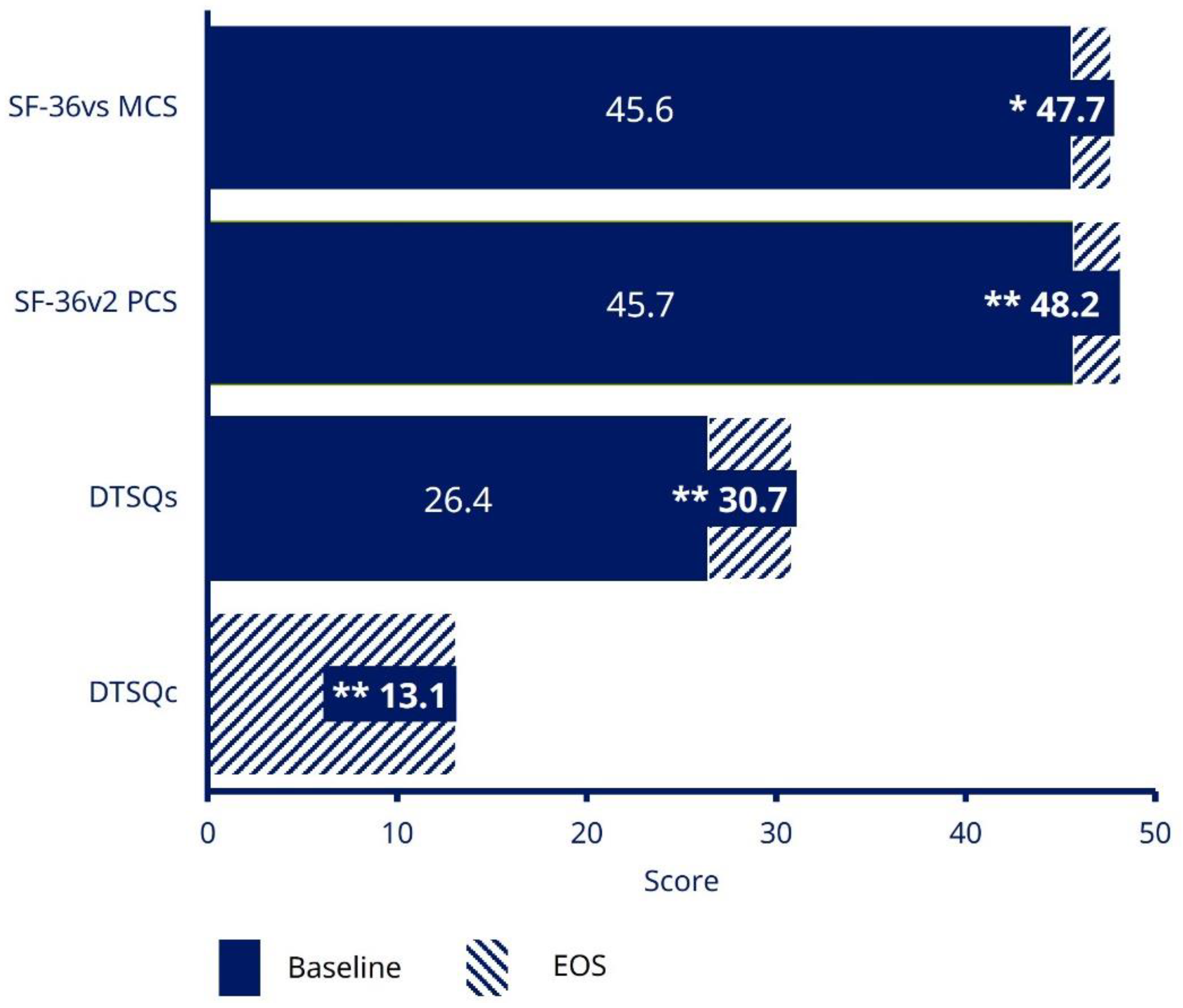
3.5. Patient-Reported Outcomes
3.6. Adverse Events and Hypoglycaemia
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soriguer, F.; Goday, A.; Bosch-Comas, A.; Bordiú, E.; Calle-Pascual, A.; Carmena, R.; Casamitjana, R.; Castaño, L.; Castell, C.; Catalá, M.; et al. Prevalence of diabetes mellitus and impaired glucose regulation in Spain: The Di@bet.es Study. Diabetologia 2012, 55, 88–93. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation Diabetes Atlas 2021, Tenth Edition. Available online: https://diabetesatlas.org/atlas/tenth-edition/ (accessed on 3 March 2022).
- American Diabetes Association. 8. Obesity Management for the Treatment of Type 2 Diabetes: Standards of Medical Care in Diabetes–2020. Diabetes Care 2020, 43 (Suppl. 1), S89–S97. [Google Scholar] [CrossRef]
- Chung, W.K.; Erion, K.; Florez, J.C.; Hattersley, A.T.; Hivert, M.F.; Lee, C.G.; McCarthy, M.I.; Nolan, J.J.; Norris, J.M.; Pearson, E.R.; et al. Precision Medicine in Diabetes: A consensus report from the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020, 43, 1617–1635. [Google Scholar] [CrossRef] [PubMed]
- Meier, J.J. GLP-1 receptor agonists for individualized treatment of type 2 diabetes mellitus. Nat. Rev. Endocrinol. 2012, 8, 728–742. [Google Scholar] [CrossRef] [PubMed]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of hyperglycemia in type 2 diabetes, 2015: A patient-centered approach: Update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2015, 38, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Prasad-Reddy, L.; Isaacs, D. A clinical review of GLP-1 receptor agonists: Efficacy and safety in diabetes and beyond. Drugs Context 2015, 4, 212283. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschweitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Marso, S.P.; Daniels, G.H.; Brown-Fransen, K.; Kristensen, P.; Mann, J.F.E.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshamanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef]
- Reyes-García, R.; Moreno-Pérez, Ó.; Tejera-Pérez, C.; Fernández-García, D.; Bellido-Castañeda, V.; de la Torre Casares, M.L.; Rozas-Moreno, P.; Fernández-García, J.C.; Martínez, A.M.; Escalada-San Martín, J.; et al. Document on a comprehensive approach to type 2 diabetes mellitus. Endocrinol. Diabetes Nutr. (Engl. Ed.) 2019, 66, 443–458. [Google Scholar] [CrossRef]
- Novo Nordisk. Ozempic® (Semaglutide) Summary of Product Characteristics. 2018. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/004174/WC500244163.pdf (accessed on 23 March 2022).
- Lau, J.; Bloch, P.; Schäffer, L.; Pettersson, I.; Spetzler, J.; Kofoed, J.; Madsen, K.; Knudsen, L.B.; McGuire, J.; Steensgaard, D.B.; et al. Discovery of the once-weekly glucagon-like peptide-1 (GLP-1) analogue semaglutide. J. Med. Chem. 2015, 58, 7370–7380. [Google Scholar] [CrossRef] [PubMed]
- Nauck, M.A.; Meier, J.J. Pioneering oral peptide therapy for patients with type 2 diabetes. Lancet Diabetes Endocrinol. 2019, 7, 500–502. [Google Scholar] [CrossRef]
- Ahmann, A.J.; Capehorn, M.; Charpentier, G.; Dotta, F.; Henkel, E.; Lingvay, I.; Holst, A.G.; Annett, M.P.; Aroda, V.R. Efficacy and safety of once-weekly semaglutide versus exenatide ER in subjects with type 2 diabetes (SUSTAIN 3): A 56-week, open-label, randomized clinical trial. Diabetes Care 2018, 41, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Ahrén, B.; Masmiquel, L.; Kumar, H.; Sargin, M.; Karsbøl, J.D.; Jacobsen, S.H.; Chow, F. Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as an add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2): A 56-week, double-blind, phase 3a, randomised trial. Lancet Diabetes Endocrinol. 2017, 5, 341–354. [Google Scholar] [CrossRef]
- Capehorn, M.S.; Catarig, A.-M.; Furberg, J.K.; Janez, A.; Price, H.C.; Tadayon, S.; Vergès, B.; Marre, M. Efficacy and safety of once-weekly semaglutide 1.0 mg vs once-daily liraglutide 1.2 mg as add-on to 1–3 oral antidiabetic drugs in subjects with type 2 diabetes (SUSTAIN 10). Diabetes Metab. 2020, 46, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Aroda, V.R.; Bain, S.C.; Cariou, B.; Piletič, M.; Rose, L.; Axelsen, M.; Rowe, E.; DeVries, J.H. Efficacy and safety of once-weekly semaglutide versus once-daily insulin glargine as add-on to metformin (with or without sulfonylureas) in insulin-naive patients with type 2 diabetes (SUSTAIN 4): A randomised, open-label, parallel-group, multicentre, multinational, phase 3a trial. Lancet Diabetes Endocrinol. 2017, 5, 355–366. [Google Scholar] [PubMed]
- Lingvay, I.; Catarig, A.-M.; Frias, J.P.; Kumar, H.; Lausvig, N.L.; le Roux, C.W.; Thielke, D.; Viljoen, A.; McCrimmon, R.J. Efficacy and safety of once-weekly semaglutide versus daily canagliflozin as add-on to metformin in patients with type 2 diabetes (SUSTAIN 8): A double-blind, phase 3b, randomised controlled trial. Lancet Diabetes Endocrinol. 2019, 7, 834–844. [Google Scholar] [CrossRef]
- Pratley, R.E.; Aroda, V.R.; Lingvay, I.; Lüdemann, J.; Andreassen, C.; Navarria, A.; Viljoen, A. SUSTAIN 7 investigators; Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): A randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol. 2018, 6, 275–286. [Google Scholar] [CrossRef]
- Rodbard, H.W.; Lingvay, I.; Reed, J.; de la Rosa, R.; Rose, L.; Sugimoto, D.; Araki, E.; Chu, P.-L.; Wijayasinghe, N.; Norwood, P. Semaglutide added to basal insulin in type 2 diabetes (SUSTAIN 5): A randomized, controlled trial. J. Clin. Endocrinol. Metab. 2018, 103, 2291–2301. [Google Scholar] [CrossRef]
- Sorli, C.; Harashima, S.; Tsoukas, G.M.; Unger, J.; Karsbøl, J.D.; Hansen, T.; Bain, S.C. Efficacy and safety of once-weekly semaglutide monotherapy versus placebo in subjects with type 2 diabetes (SUSTAIN 1): A double-blind, randomised, placebo-controlled, parallel-group, multinational, multicentre phase 3a trial. Lancet Diabetes Endocrinol. 2017, 5, 251–260. [Google Scholar] [CrossRef]
- Zinman, B.; Bhosekar, V.; Bush, R.; Holst, I.; Ludvik, B.; Thielke, D.; Thrasher, J.; Woo, V.; Philis-Tsimikas, A. Semaglutide once weekly as add-on to SGLT-2 inhibitor therapy in type 2 diabetes (SUSTAIN 9): A randomised, placebo-controlled trial. 2019. Lancet Diabetes Endocrinol. 2019, 7, 356–367. [Google Scholar] [CrossRef]
- Blonde, L.; Khunti, K.; Harris, S.B.; Meizinger, C.; Skolnik, N.S. Interpretation and impact of real-world clinical data for the practicing clinician. Adv. Ther. 2018, 35, 1763–1774. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency, Guideline on Good Pharmacovigilance Practices (GVP)-Module VI. 2017. Available online: https://www.ema.europa.eu/en/documents/regulatory-procedural-guideline/guideline-good-pharmacovigilance-practices-gvp-module-vi-collection-management-submission-reports_en.pdf (accessed on 8 March 2022).
- International Society of Pharmacoepidemiology. Guidelines for good pharmacoepidemiology practice (GPP). Pharmacoepidemiol. Drug Saf. 2016, 25, 2–10. [Google Scholar] [CrossRef]
- American Diabetes Association. 6. Glycemic Targets: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018, 41 (Suppl. 1), S55–S64. [Google Scholar] [CrossRef]
- National Institute for Clinical Excellence. Type 2 Diabetes in Adults: Management [NG28]. 2015. Available online: http://www.nice.org.uk/guidance/ng28 (accessed on 8 March 2022).
- Morisky, D.E.; Ang, A.; Krousel-Wood, M.; Ward, H.J. Predictive validity of a medication adherence measure in an outpatient setting. J. Clin. Hypertens. 2008, 10, 348–354. [Google Scholar] [CrossRef]
- Krousel-Wood, M.; Islam, T.; Webber, L.S.; Re, R.N.; Morisky, D.E.; Muntner, P. New medication adherence scale versus pharmacy fill rates in seniors with hypertension. Am. J. Manag. Care 2009, 15, 59–66. [Google Scholar]
- Morisky, D.E.; DiMatteo, M.R. Improving the measurement of self-reported medication nonadherence: Response to authors. J. Clin. Epidemiol. 2011, 64, 255–257. [Google Scholar] [CrossRef]
- Mody, R.; Grabner, M.; Yu, M.; Turner, R.; Kwan, A.Y.M.; York, W.; Landó, L.F. Real-world effectiveness, adherence and persistence among patients with type 2 diabetes mellitus initiating dulaglutide treatment. Curr. Med. Res. Opin. 2018, 34, 995–1003. [Google Scholar] [CrossRef]
- Wilke, T.; Mueller, S.; Groth, A.; Berg, B.; Fuchs, A.; Sikirica, M.; Logie, J.; Martin, A.; Maywald, U. Non-persistence and non-adherence of patients with type 2 diabetes mellitus in therapy with GLP-1 receptor agonists: A retrospective analysis. Diabetes Ther. 2016, 7, 105–124. [Google Scholar] [CrossRef]
- Divino, V.; DeKoven, M.; Hallinan, S.; Varo, N.; Wirta, S.B.; Lee, W.C.; Reaney, M. Glucagon-like peptide-1 receptor agonist treatment patterns among type 2 diabetes patients in six European countries. Diabetes Ther. 2014, 5, 499–520. [Google Scholar] [CrossRef] [PubMed]
- Di Loreto, C.; Minarelli, V.; Nasini, G.; Norgiolini, R.; Del Sindaco, P. Effectiveness in real world of once weekly semaglutide in people with type 2 diabetes: Glucagon-like peptide receptor agonist naïve or switchers from other glucagon-like peptide receptor agonists: Results from a retrospective observational study in Umbria. Diabetes Ther. 2022, 13, 551–567. [Google Scholar] [CrossRef] [PubMed]
- Weiss, T.; Yang, L.; Carr, R.D.; Pal, S.; Sawhney, B.; Boggs, R.; Rajpathak, S.; Iglay, K. Real-world weight change, adherence, and discontinuation among patients with type 2 diabetes initiating glucagon-like peptide-1 receptor agonists in the UK. BMJ Open Diabetes Res. Care 2022, 10, e002517. [Google Scholar] [CrossRef] [PubMed]
- Uzoigwe, C.; Liang, Y.; Whitmire, S.; Paprocki, Y. Semaglutide once-weekly persistence and adherence versus other GLP-1RAs in patients with type 2 diabetes in a US real-world setting. Diabetes Ther. 2021, 12, 1475–1489. [Google Scholar] [CrossRef]
- Ferrer-García, J.C.; Galera, R.A.; Arribas Sr., L.; Torrens, M.T.; Lorente, A.S.; Portilla, A.J.; Artero, A.; Sánchez-Juan, C. Receptor agonist in type 2 diabetes: A study to evaluate real-world effectiveness. In Proceedings of the American Diabetes Association 80th Scientific Sessions, Chicago, IL, USA, 12–16 June 2020. Poster number 947-P. [Google Scholar]
- Cárdenas-Salas, J.J.; Sierra, R.; Luca, B.L.; Sánchez, B.; Modroño, N.; Casado, C.; Sánchez, N.M.; Cruces, E.; Vázquez, C. Semaglutide in patients with type 2 diabetes: Real-world data from Spain. In Proceedings of the American Diabetes Association 81st Scientific Sessions, Washington, DC, USA, 25–29 June 2021. Poster number 690-P. [Google Scholar]
- Garcia De Lucas, M.D.; Avilés Bueno, B.; Pérez Belmonte, L.M.; Jiménez Millán, A.B.; Rivas Ruiz, F. Semaglutide Achieves Better Metabolic and Weight Control than Other GLP-1 RA in Real Life after 12 Months of Follow-up. In Proceedings of the American Diabetes Association 81st Scientific Sessions, Washington, DC, USA, 25–29 June 2021. Poster number 676-P. [Google Scholar]
- Holmes, P.; Bell, H.E.; Bozkurt, K.; Catarig, A.-M.; Clark, A.; Machell, A.; Sathyapalan, T. Real-world use of once-weekly semaglutide in type 2 diabetes: Results from the SURE UK multicentre, prospective, observational study. Diabetes Ther. 2021, 12, 2891–2905. [Google Scholar] [CrossRef]
- Ekberg, N.R.; Bodholt, U.; Catarig, A.-M.; Catrina, S.-B.; Grau, K.; Holmberg, C.N.; Klanger, B.; Knudsen, S.T. Real-world use of once-weekly semaglutide in patients with type 2 diabetes: Results from the SURE Denmark/Sweden multicentre, prospective, observational study. Prim. Care Diabetes 2021, 15, 871–878. [Google Scholar] [CrossRef]
- Yale, J.F.; Catarig, A.-M.; Grau, K.; Harris, S.; Klimek-Abercrombie, A.; Rabasa-Lhoret, R.; Reardon, L.; Woo, V.; Liutkus, J. Use of once-weekly semaglutide in patients with type 2 diabetes in routine clinical practice: Results from the SURE Canada multicentre, prospective, observational study. Diabetes Obes. Metab. 2021, 23, 2269–2278. [Google Scholar] [CrossRef]
- Rudofsky, G.; Catarig, A.-M.; Favre, L.; Grau, K.; Häfliger, S.; Thomann, R.; Schultes, B. Real-world use of once-weekly semaglutide in patients with type 2 diabetes: Results from the SURE Switzerland multicentre, prospective, observational study. Diabetes Res. Clin. Pract. 2021, 178, 108931. [Google Scholar] [CrossRef]
- Instituto Aragonés de Ciencias de la Salud. Un Nuevo Atlas Muestra la Prescripción Recibida Por la Población Diabética de Aragón en 2020. Available online: https://www.iacs.es/un-nuevo-atlas-muestra-la-prescripcion-recibida-por-la-poblacion-diabetica-de-aragon-en-2020/ (accessed on 8 March 2022).
- Marzullo, P.; Daffara, T.; Mele, C.; Zavattaro, M.; Ferrero, A.; Caputo, M.; Prodam, F.; Aimaretti, G. Real-world evaluation of weekly subcutaneous treatment with semaglutide in a cohort of Italian diabetic patients. J. Endocrinol. Invest. 2022, 45, 1587–1598. [Google Scholar]
- Sánchez, E.; Lecube, A.; Bellido, D.; Monereo, S.; Malagón, M.M.; Tinahones, F.J.; on behalf of the Spanish Society for the Study of Obesity. Leading factors for weight gain during COVID-19 lockdown in a Spanish population: A cross-sectional study. Nutrients 2021, 13, 894. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | 227 |
| Age, years | 59.1 (9.94) |
| Female, n (%) | 111 (48.9) |
| Race, n (%) | |
| White | 221 (97.4) |
| American Indian or Alaska Native | 2 (0.9) |
| Other | 4 (1.8) |
| Body weight, kg | 98.3 (17.89) |
| Waist circumference, cm | 118.8 (12.50) |
| BMI, kg/m2 | 36.4 (5.28) |
| BMI categories, n (%) | |
| Normal (18.5−<25 kg/m2) | 0 |
| Overweight (25−<30 kg/m2) | 12 (5.3) |
| Obese class I (30−<35 kg/m2) | 89 (39.6) |
| Obese class II & III (≥35 kg/m2) | 124 (55.1) |
| Diabetes duration, years | 11.8 (8.10) |
| Baseline HbA1c, % | 8.5 (1.58) |
| HbA1c level, n (%) | |
| <8.0% | 93 (41.0) |
| <7.5% | 62 (27.3) |
| <7.0% | 34 (15.0) |
| Baseline HbA1c, mmol/L | 69.1 (17.3) |
| FPG, mmol/L | 9.9 (3.46) |
| eGFR, mL/min/1.73 m2 | 82.4 (22.58) |
| Lipid composition, mg/dL | |
| HDL cholesterol | 44.8 (13.31) |
| LDL cholesterol | 92.5 (30.76) |
| Total cholesterol | 175.7 (45.41) |
| Triglycerides | 243.9 (298.8) |
| Lipid composition, mmol/L | |
| HDL cholesterol | 1.2 (0.34) |
| LDL cholesterol | 2.4 (0.80) |
| Total cholesterol | 4.6 (1.18) |
| Triglycerides | 2.8 (3.37) |
| Comorbid conditions at baseline, n (%) | |
| Diabetic retinopathy | 29 (12.9) |
| Diabetic neuropathy | 18 (7.9) |
| Diabetic nephropathy | 38 (16.7) |
| Dyslipidaemia | 173 (76.2) |
| Hypertension | 172 (75.8) |
| N | n | Estimate | 95% CI | p-Value | |
|---|---|---|---|---|---|
| HbA1c, % | 196 | 187 | - | - | - |
| Observed mean at baseline | - | - | 8.4 | - | - |
| Estimated mean at EOS | - | - | 7.1 | - | - |
| Change from baseline to EOS | - | - | −1.3 | [−1.51; −1.18] | <0.0001 |
| HbA1c, mmol/mol | 196 | 187 | - | - | - |
| Observed mean at baseline | - | - | 68.5 | - | - |
| Estimated mean at EOS | - | - | 53.8 | - | - |
| Change from baseline to EOS | - | - | −14.7 | [−16.48; −12.86] | <0.0001 |
| Body weight, kg | 196 | 194 | - | - | - |
| Observed mean at baseline | - | - | 98.9 | - | - |
| Estimated mean at EOS | - | - | 93.2 | - | - |
| Change from baseline to EOS | - | - | −5.7 | [−6.36; −4.98] | <0.0001 |
| Percent change from baseline to EOS | - | - | −5.7 | [−6.41; −5.03] | <0.0001 |
| Waist circumference, cm | 196 | 165 | - | - | - |
| Observed mean at baseline | - | - | 118.8 | - | - |
| Estimated mean at EOS | - | - | 113.4 | - | - |
| Change from baseline to EOS | - | - | −5.3 | [−6.29; −4.41] | <0.0001 |
| BMI, kg/m2 | 196 | 194 | - | - | - |
| Observed mean at baseline | - | - | 36.5 | - | - |
| Estimated mean at EOS | - | - | 34.4 | - | - |
| Change from baseline to EOS | - | - | −2.1 | [−2.37; −1.86] | <0.0001 |
| Serious | Non-Serious | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | (%) | E | N | (%) | E | N | (%) | E | |
| AE | 2 | 0.9 | 3 | 13 | 5.7 | 23 | 15 | 6.6 | 26 |
| Severity | |||||||||
| Mild | 0 | 0 | 0 | 6 | 2.6 | 12 | 6 | 2.6 | 12 |
| Moderate | 1 | 0.4 | 2 | 6 | 2.6 | 10 | 7 | 3.1 | 12 |
| Severe | 1 | 0.4 | 1 | 1 | 0.4 | 1 | 2 | 0.9 | 2 |
| GI disorders | 0 | 0 | 0 | 13 | 5.7 | 22 | 13 | 5.7 | 22 |
| Nausea | 0 | 0 | 0 | 7 | 3.1 | 7 | 7 | 3.1 | 7 |
| Vomiting | 0 | 0 | 0 | 5 | 2.2 | 5 | 5 | 2.2 | 5 |
| Diarrhoea | 0 | 0 | 0 | 3 | 1.3 | 3 | 3 | 1.3 | 3 |
| AEs leading to treatment discontinuation | 0 | 0 | 0 | 5 | 2.2 | 6 | 5 | 2.2 | 6 |
| SADRs | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| N | (%) | ||||||||
| Patients with severe or documented hypoglycaemic episodes | 8 | 4.1 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellido, V.; Abreu Padín, C.; Catarig, A.-M.; Clark, A.; Barreto Pittol, S.; Delgado, E. Once-Weekly Semaglutide Use in Patients with Type 2 Diabetes: Results from the SURE Spain Multicentre, Prospective, Observational Study. J. Clin. Med. 2022, 11, 4938. https://doi.org/10.3390/jcm11174938
Bellido V, Abreu Padín C, Catarig A-M, Clark A, Barreto Pittol S, Delgado E. Once-Weekly Semaglutide Use in Patients with Type 2 Diabetes: Results from the SURE Spain Multicentre, Prospective, Observational Study. Journal of Clinical Medicine. 2022; 11(17):4938. https://doi.org/10.3390/jcm11174938
Chicago/Turabian StyleBellido, Virginia, Cristina Abreu Padín, Andrei-Mircea Catarig, Alice Clark, Sofía Barreto Pittol, and Elias Delgado. 2022. "Once-Weekly Semaglutide Use in Patients with Type 2 Diabetes: Results from the SURE Spain Multicentre, Prospective, Observational Study" Journal of Clinical Medicine 11, no. 17: 4938. https://doi.org/10.3390/jcm11174938
APA StyleBellido, V., Abreu Padín, C., Catarig, A.-M., Clark, A., Barreto Pittol, S., & Delgado, E. (2022). Once-Weekly Semaglutide Use in Patients with Type 2 Diabetes: Results from the SURE Spain Multicentre, Prospective, Observational Study. Journal of Clinical Medicine, 11(17), 4938. https://doi.org/10.3390/jcm11174938