
Position of the Hyoid Bone and Dimension of Nasopharynx and Oropharynx after Occlusal Splint Therapy and Physiotherapy in Patients Diagnosed with Temporomandibular Disorders


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Investigation
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
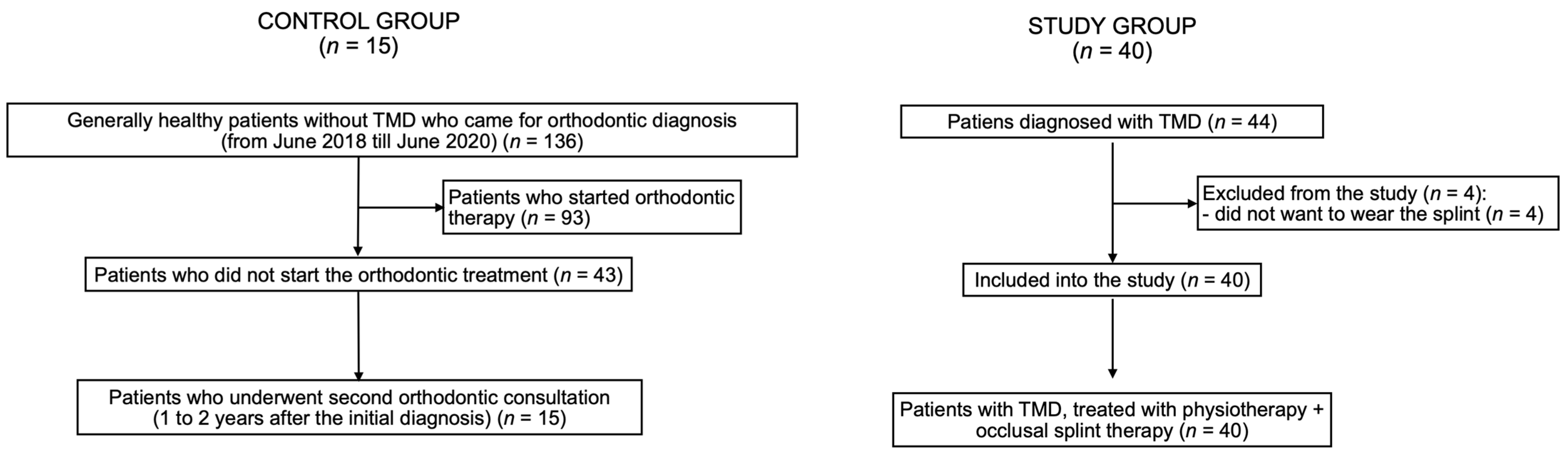
3.1. Flow of Participants
3.2. Research Question
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Auvenshine, R.C.; Pettit, N.J. The hyoid bone: An overview. Cranio 2020, 38, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Jose, N.P.; Shetty, S.; Mogra, S.; Shetty, V.S.; Rangarajan, S.; Mary, L. Evaluation of hyoid bone position and its correlation with pharyngeal airway space in different types of skeletal malocclusion. Contemp. Clin. Dent. 2014, 5, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Kraaijenga, S.A.; van der Molen, L.; Heemsbergen, W.D.; Remmerswaal, G.B.; Hilgers, F.J.; van den Brekel, M.W. Hyoid bone displacement as parameter for swallowing impairment in patients treated for advanced head and neck cancer. Eur. Arch. Otorhinolaryngol. 2017, 274, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Na, Y.J.; Jang, J.S.; Lee, K.H.; Yoon, Y.J.; Chung, M.S.; Han, S.H. Thyroid cartilage loci and hyoid bone analysis using a video fluoroscopic swallowing study (VFSS). Medicine 2019, 98, e16349. [Google Scholar] [CrossRef]
- Mohamed, A.S.; Habumugisha, J.; Cheng, B.; Zhao, M.; Guo, Y.; Zou, R.; Wang, F. Three-dimensional evaluation of hyoid bone position in nasal and mouth breathing subjects with skeletal Class I, and Class II. BMC Oral Health 2022, 22, 228. [Google Scholar] [CrossRef]
- Kapos, F.P.; Exposto, F.G.; Oyarzo, J.F.; Durham, J. Temporomandibular disorders: A review of current concepts in aetiology, diagnosis and management. Oral Surg. 2020, 13, 321–334. [Google Scholar] [CrossRef]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Interdisciplinary Approach to the Temporomandibular Joint Osteoarthritis-Review of the Literature. Medicina 2020, 56, 225. [Google Scholar] [CrossRef]
- Derwich, M.; Gottesman, L.; Urbanska, K.; Pawlowska, E. Craniovertebral and Craniomandibular Changes in Patients with Temporomandibular Joint Disorders after Physiotherapy Combined with Occlusal Splint Therapy: A Prospective Case Control Study. Medicina 2022, 58, 684. [Google Scholar] [CrossRef]
- Bilici, S.; Yigit, O.; Celebi, O.O.; Yasak, A.G.; Yardimci, A.H. Relations between Hyoid-Related Cephalometric Measurements and Severity of Obstructive Sleep Apnea. J. Craniofac. Surg. 2018, 29, 1276–1281. [Google Scholar] [CrossRef]
- Neelapu, B.C.; Kharbanda, O.P.; Sardana, H.K.; Balachandran, R.; Sardana, V.; Kapoor, P.; Gupta, A.; Vasamsetti, S. Craniofacial and upper airway morphology in adult obstructive sleep apnea patients: A systematic review and meta-analysis of cephalometric studies. Sleep Med. Rev. 2017, 31, 79–90. [Google Scholar] [CrossRef]
- Derwich, M.; Pawlowska, E. Do the Mandibular Condyles Change Their Positions within Glenoid Fossae after Occlusal Splint Therapy Combined with Physiotherapy in Patients Diagnosed with Temporomandibular Joint Disorders? A Prospective Case Control Study. J. Pers. Med. 2022, 12, 254. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Rocabado, M.; Iglarsh, Z.A. Physical modalities and manual techniques used in the treatment of maxillofacial pain. In Musculoskeletal Approach to Maxillofacial Pain, 1st ed.; JB Lippincott: Philadelphia, PA, USA, 1991; pp. 187–192. [Google Scholar]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Is the Temporomandibular Joints’ Reciprocal Clicking Related to the Morphology and Position of the Mandible, as Well as to the Sagittal Position of Lower Incisors?—A Case-Control Study. Int. J. Environ. Res. Public Health 2021, 18, 4994. [Google Scholar] [CrossRef] [PubMed]
- Rocabado, M. Biomechanical relationship of the cranial, cervical, and hyoid regions. J. Craniomandib. Pract. 1983, 1, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Xiong, X.; Yan, Z.; Xiao, C.; Zheng, Y.; Wang, J. Hyoid Bone Position in Patients with and without Temporomandibular Joint Osteoarthrosis: A Cone-Beam Computed Tomography and Cephalometric Analysis. Pain Res. Manag. 2021, 2021, 4852683. [Google Scholar] [CrossRef] [PubMed]
- Ekici, Ö.; Camcı, H. Relationship of temporomandibular joint disorders with cervical posture and hyoid bone position. Cranio 2021, 18, 1–10. [Google Scholar] [CrossRef]
- Andrade, A.V.; Gomes, P.F.; Teixeira-Salmela, L.F. Cervical spine alignment and hyoid bone positioning with temporomandibular disorders. J. Oral Rehabil. 2007, 34, 767–772. [Google Scholar] [CrossRef]
- Câmara-Souza, M.B.; Figueredo, O.M.C.; Maia, P.R.L.; Dantas, I.S.; Barbosa, G.A.S. Cervical posture analysis in dental students and its correlation with temporomandibular disorder. Cranio 2018, 36, 85–90. [Google Scholar] [CrossRef]
- Young, J.W.; McDonald, J.P. An investigation into the relationship between the severity of obstructive sleep apnoea/hypopnoea syndrome and the vertical position of the hyoid bone. Surgeon 2004, 2, 145–151. [Google Scholar] [CrossRef]
- Gungor, A.Y.; Turkkahraman, H.; Yilmaz, H.H.; Yariktas, M. Cephalometric comparison of obstructive sleep apnea patients and healthy controls. Eur. J. Dent. 2013, 7, 48–54. [Google Scholar] [CrossRef] [Green Version]
- Tsumori, N.; Abe, S.; Agematsu, H.; Hashimoto, M.; Ide, Y. Morphologic characteristics of the superior pharyngeal constrictor muscle in relation to the function during swallowing. Dysphagia 2007, 22, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, Y. Gross anatomical observations of attachments of the middle pharyngeal constrictor. Clin. Anat. 2014, 27, 603–609. [Google Scholar] [CrossRef]
- Veasey, S.C.; Rosen, I.M. Obstructive Sleep Apnea in Adults. N. Engl. J. Med. 2019, 380, 1442–1449. [Google Scholar] [CrossRef] [PubMed]
- Gulotta, G.; Iannella, G.; Vicini, C.; Polimeni, A.; Greco, A.; de Vincentiis, M.; Visconti, I.C.; Meccariello, G.; Cammaroto, G.; De Vito, A.; et al. Risk Factors for Obstructive Sleep Apnea Syndrome in Children: State of the Art. Int. J. Environ. Res. Public Health 2019, 16, 3235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, J.L.; Rosen, I. Utility of the modified Mallampati grade and Friedman tongue position in the assessment of obstructive sleep apnea. J. Clin. Sleep Med. 2020, 16, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Nuckton, T.J.; Glidden, D.V.; Browner, W.S.; Claman, D.M. Physical examination: Mallampati score as an independent predictor of obstructive sleep apnea. Sleep 2006, 29, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Rundo, J.V. Obstructive sleep apnea basics. Clevel. Clin. J. Med. 2019, 86, 2–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Mechanisms of Action and Efficacy of Hyaluronic Acid, Corticosteroids and Platelet-Rich Plasma in the Treatment of Temporomandibular Joint Osteoarthritis—A Systematic Review. Int. J. Mol. Sci. 2021, 22, 7405. [Google Scholar] [CrossRef]
- Chęciński, M.; Chęcińska, K.; Nowak, Z.; Sikora, M.; Chlubek, D. Treatment of Mandibular Hypomobility by Injections into the Temporomandibular Joints: A Systematic Review of the Substances Used. J. Clin. Med. 2022, 11, 2305. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
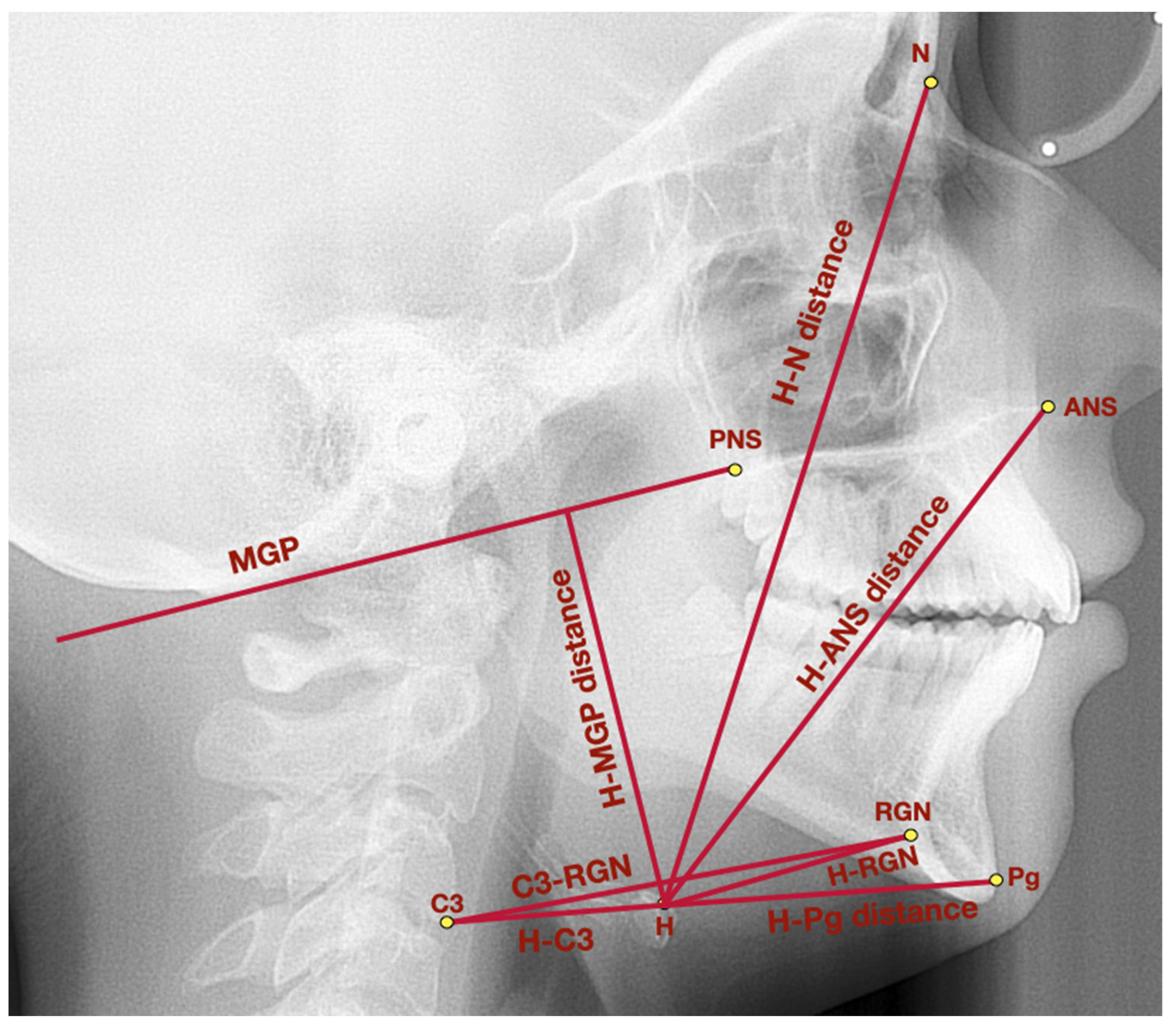
| Measurement | Point/Line/Angle | Description |
|---|---|---|
| General points and lines | Point ANS | Anterior nasal spine–the most prominent point of the anterior nasal spine |
| Point PNS | Posterior nasal spine–the most posterior point of hard palate, crossed by the pterygopalatine fossa | |
| Point Pg | Pogonion–the most prominent point localized in the mental tuberosity | |
| Point N | Nasion–the most anterior point localized in the frontonasal suture | |
| Point H | Hyoidale–the most superior anterior point of the body of the hyoid bone | |
| Point C3 | The most inferior anterior angle of the body of the third cervical vertebra | |
| RGN | Retrognathion–the most posterior inferior aspect of the mandibular symphysis | |
| MGP | McGregor’s Plane–line which links posterior nasal spine with the basiocciput | |
| Hyoid triangle | H-C3 distance | The distance between the points: H and C3 |
| H-RGN distance | The distance between the points: H and RGN | |
| C3-RGN distance | The distance between the points: C3 and RGN | |
| H-H’ distance | The height of the hyoid triangle, measured as a distance between point H and the perpendicular projection of point H onto C3-RGN line | |
| Hyoid bone topography | H-MGP distance | The distance measured between point H and the perpendicular projection of point H onto MGP |
| H-N distance | The distance between the points: hyoidale and nasion | |
| H-ANS distance | The distance between the points: hyoidale and anterior nasal spine | |
| H-Pg distance | The distance between the points: hyoidale and pogonion | |
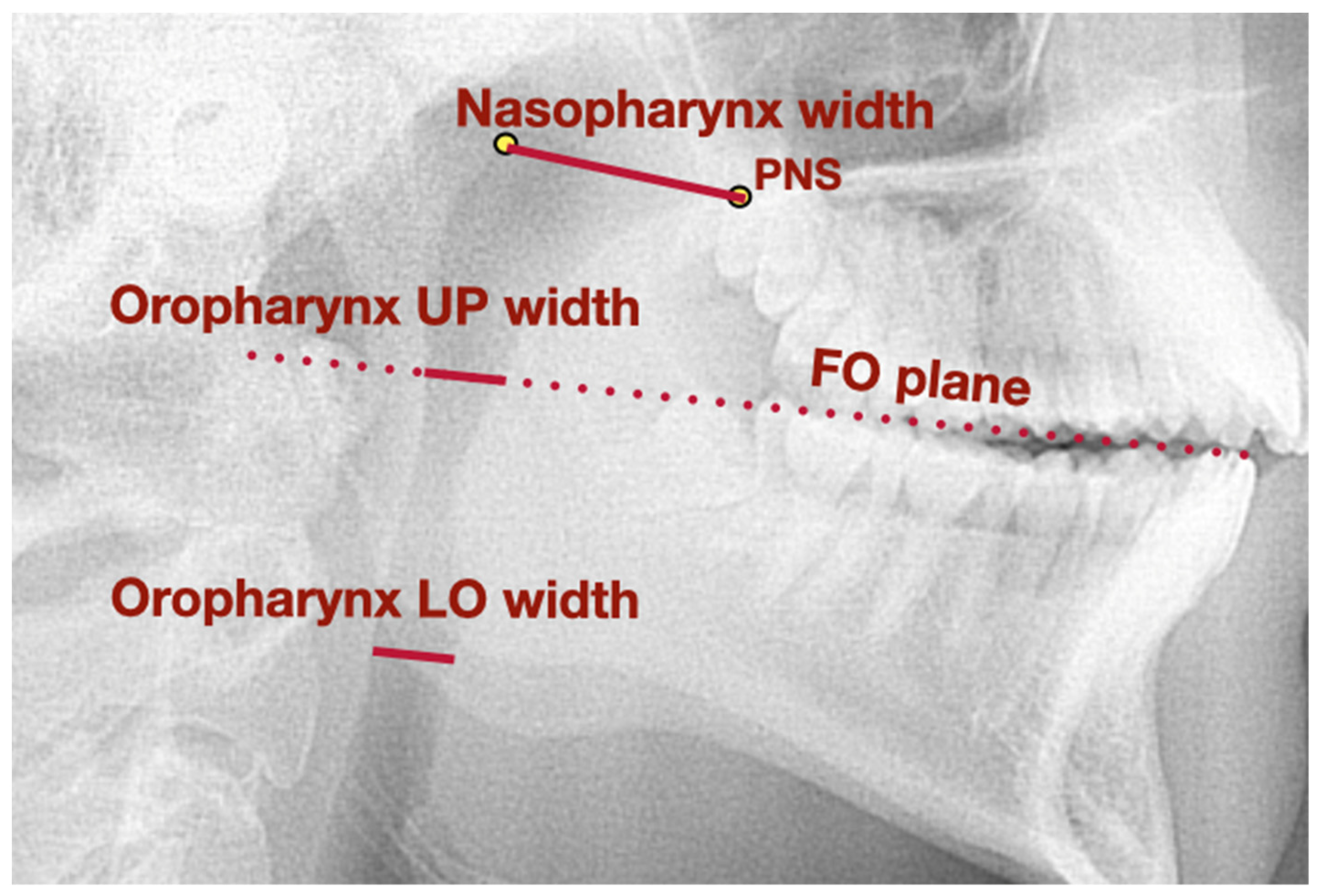
| Airways dimension | Nasopharynx width | The distance measured between posterior nasal spine and the posterior superior point in the nasopharynx |
| Oropharynx UP width | The distance measured between the intersection of the functional occlusal plane with the posterior border of the mandibular ramus and the posterior wall of the oropharynx | |
| Oropharynx LO width | The distance measured between the mandibular angle with the tongue and the posterior wall of the oropharynx |
| Comparable Characteristic | Study Group av. ± SD (95% CI) | Control Group av. ± SD (95% CI) | p–Value | |
|---|---|---|---|---|
| Hyoid triangle | H-C3 distance (mm) | 31.8 ± 4.4 (29.9 to 32.6) | 33.0 ± 4.8 (30.3 to 35.6) | 0.0784 b |
| H-RGN distance (mm) | 36.3 ± 5.2 (34.4 to 37.8) | 39.3 ± 5.7 (36.2 to 42.5) | 0.0686 a | |
| C3-RGN distance (mm) | 64.1 ± 8.6 (61.1 to 67.7) | 70.6 ± 8.3 (66.0 to 75.1) | 0.0104 b | |
| H-H’ distance (mm) | 5.5 ± 5.4 (4.2 to 7.1) | 5.8 ± 6.4 (2.2 to 9.3) | 0.8358 b | |
| Hyoid bone topography | H-MGP distance (mm) | 58.0 ± 7.3 (55.4 to 60.9) | 57.5 ± 6.6 (53.8 to 61.2) | 0.5935 b |
| H-N distance (mm) | 121.4 ± 8.9 (117.5 to 124.7) | 121.2 ± 8.3 (116.7 to 125.8) | 0.9145 a | |
| H-ANS distance (mm) | 82.6 ± 8.1 (80.1 to 85.5) | 83.2 ± 5.8 (80.0 to 86.4) | 0.8343 a | |
| H-Pg distance (mm) | 47.8 ± 6.1 (46.0 to 50.3) | 51.9 ± 6.6 (48.3 to 55.6) | 0.0256 a | |
| Airways dimension | Nasopharynx width (mm) | 20.3 ± 3.4 (19.4 to 21.8) | 23.2 ± 3.2 (21.4 to 25.0) | 0.0241 a |
| Oropharynx UP width (mm) | 10.0 ± 2.3 (9.1 to 11.0) | 9.6 ± 2.5 (8.2 to 10.9) | 0.4965 a | |
| Oropharynx LO width (mm) | 9.3 ± 2.9 (8.4 to 10.0) | 10.3 ± 2.1 (9.1 to 11.4) | 0.1868 b | |
| Comparable Characteristic | First Examination av. ± SD (95% CI) | Second Examination (1–2 Years after the Initial One) av. ± SD (95% CI) | p–Value | |
|---|---|---|---|---|
| Hyoid triangle | H-C3 distance (mm) | 33.0 ± 4.8 (30.3 to 35.6) | 33.0 ± 4.8 (30.4 to 35.7) | 0.5752 a |
| H-RGN distance (mm) | 39.3 ± 5.7 (36.2 to 42.5) | 39.5 ± 5.9 (36.2 to 42.8) | 0.3176 a | |
| C3-RGN distance (mm) | 70.6 ± 8.3 (66.0 to 75.1) | 71.0 ± 8.4 (66.4 to 75.6) | 0.1820 b | |
| H-H’ distance (mm) | 5.8 ± 6.4 (2.2 to 9.3) | 5.7 ± 6.3 (2.2 to 9.2) | 0.3464 b | |
| Hyoid bone topography | H-MGP distance (mm) | 57.5 ± 6.6 (53.8 to 61.2) | 57.5 ± 6.7 (53.8 to 61.2) | 0.7557 b |
| H-N distance (mm) | 121.2 ± 8.3 (116.7 to 125.8) | 121.3 ± 8.3 (116.7 to 125.9) | 0.5225 a | |
| H-ANS distance (mm) | 83.2 ± 5.8 (80.0 to 86.4) | 83.3 ± 5.9 (80.1 to 86.6) | 0.4616 a | |
| H-Pg distance (mm) | 51.9 ± 6.6 (48.3 to 55.6) | 52.1 ± 6.5 (48.5 to 55.7) | 0.1813 a | |
| Airways dimension | Nasopharynx width (mm) | 23.2 ± 3.2 (21.4 to 25.0) | 23.3 ± 3.2 (21.5 to 25.1) | 0.1551 a |
| Oropharynx UP width (mm) | 9.6 ± 2.5 (8.2 to 10.9) | 9.5 ± 2.5 (8.1 to 10.9) | 0.0733 a | |
| Oropharynx LO width (mm) | 10.3 ± 2.1 (9.1 to 11.4) | 10.3 ± 2.1 (9.1 to 11.4) | 0.8447 a | |
| Comparable Characteristic | Before Treatment av. ± SD (95% CI) | After Treatment av. ± SD (95% CI) | p–Value | |
|---|---|---|---|---|
| Hyoid triangle | H-C3 distance (mm) | 31.8 ± 4.4 (29.9 to 32.6) | 31.6 ± 4.8 (29.8 to 33.1) | 0.5136 b |
| H-RGN distance (mm) | 36.3 ± 5.2 (34.4 to 37.8) | 36.8 ± 5.4 (34.9 to 38.7) | 0.2468 a | |
| C3-RGN distance (mm) | 64.1 ± 8.6 (61.1 to 67.7) | 64.6 ± 6.6 (61.7 to 67.0) | 0.8453 b | |
| H-H’ distance (mm) | 5.5 ± 5.4 (4.2 to 7.1) | 7.8 ± 6.4 (5.8 to 9.9) | <0.0001 b | |
| Hyoid bone topography | H-MGP distance (mm) | 58.0 ± 7.3 (55.4 to 60.9) | 61.4 ± 8.2 (58.6 to 64.2) | <0.0001 a |
| H-N distance (mm) | 121.4 ± 8.9 (117.5 to 124.7) | 125.5 ± 9.8 (122.5 to 128.3) | <0.0001 b | |
| H-ANS distance (mm) | 82.6 ± 8.1 (80.1 to 85.5) | 86.4 ± 7.7 (83.9 to 88.6) | <0.0001 b | |
| H-Pg distance (mm) | 47.8 ± 6.1 (46.0 to 50.3) | 48.4 ± 5.7 (46.9 to 50.3) | 0.2867 b | |
| Airways dimension | Nasopharynx width (mm) | 20.3 ± 3.4 (19.4 to 21.8) | 20.2 ± 3.1 (19.7 to 20.6) | 0.5365 a |
| Oropharynx UP width (mm) | 10.0 ± 2.3 (9.1 to 11.0) | 9.7 ± 2.9 (9.0 to 10.6) | 0.2986 a | |
| Oropharynx LO width (mm) | 9.3 ± 2.9 (8.4 to 10.0) | 8.3 ± 2.6 (7.6 to 9.0) | 0.0104 a | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Derwich, M.; Pawlowska, E. Position of the Hyoid Bone and Dimension of Nasopharynx and Oropharynx after Occlusal Splint Therapy and Physiotherapy in Patients Diagnosed with Temporomandibular Disorders. J. Clin. Med. 2022, 11, 4939. https://doi.org/10.3390/jcm11174939
Derwich M, Pawlowska E. Position of the Hyoid Bone and Dimension of Nasopharynx and Oropharynx after Occlusal Splint Therapy and Physiotherapy in Patients Diagnosed with Temporomandibular Disorders. Journal of Clinical Medicine. 2022; 11(17):4939. https://doi.org/10.3390/jcm11174939
Chicago/Turabian StyleDerwich, Marcin, and Elzbieta Pawlowska. 2022. "Position of the Hyoid Bone and Dimension of Nasopharynx and Oropharynx after Occlusal Splint Therapy and Physiotherapy in Patients Diagnosed with Temporomandibular Disorders" Journal of Clinical Medicine 11, no. 17: 4939. https://doi.org/10.3390/jcm11174939
APA StyleDerwich, M., & Pawlowska, E. (2022). Position of the Hyoid Bone and Dimension of Nasopharynx and Oropharynx after Occlusal Splint Therapy and Physiotherapy in Patients Diagnosed with Temporomandibular Disorders. Journal of Clinical Medicine, 11(17), 4939. https://doi.org/10.3390/jcm11174939