
The Effects of a Therapeutic Strategy Guided by Lung Ultrasound on 6-Month Outcomes in Patients with Heart Failure: Results from the EPICC Randomized Controlled Trial

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
Ethical Aspects
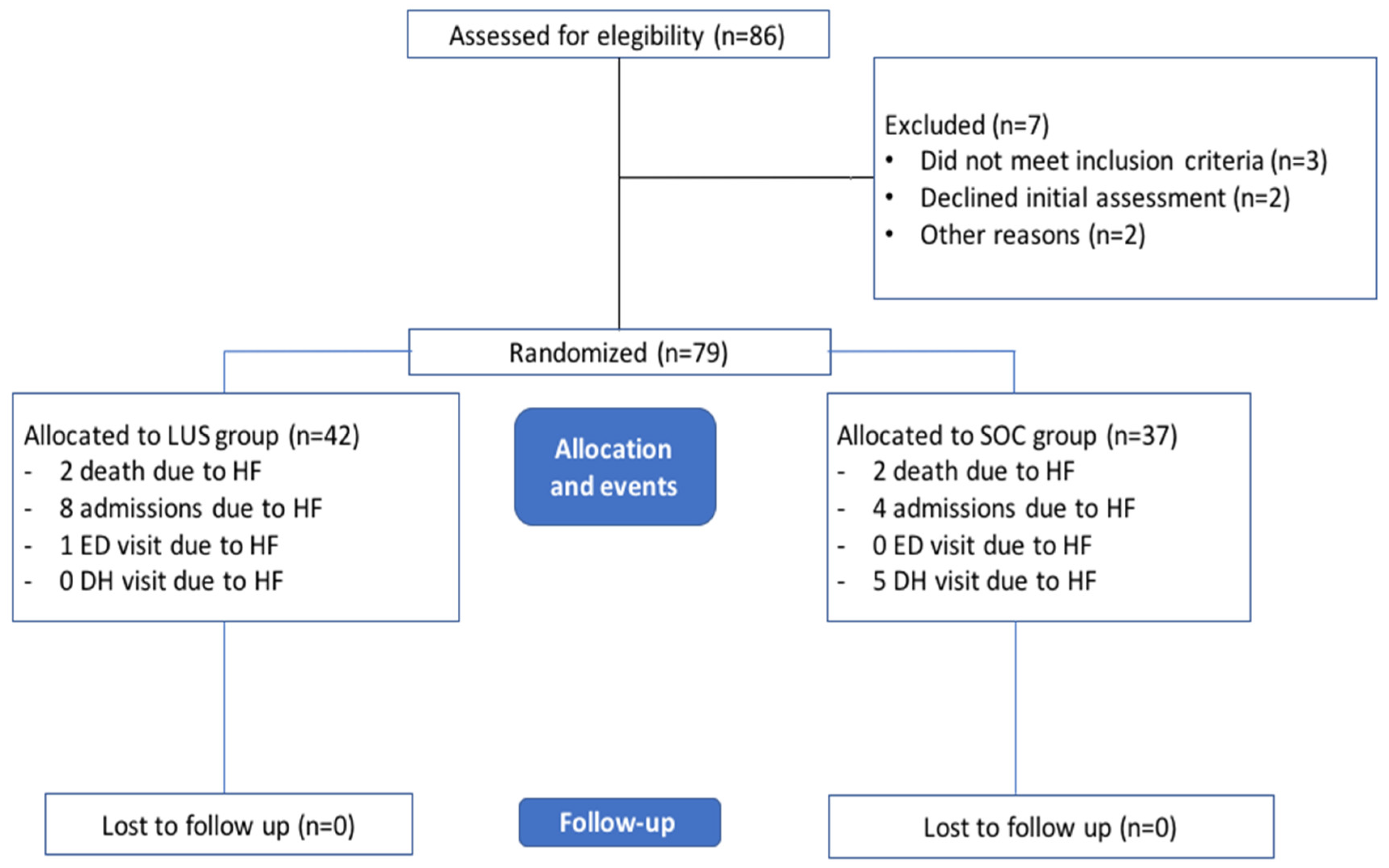
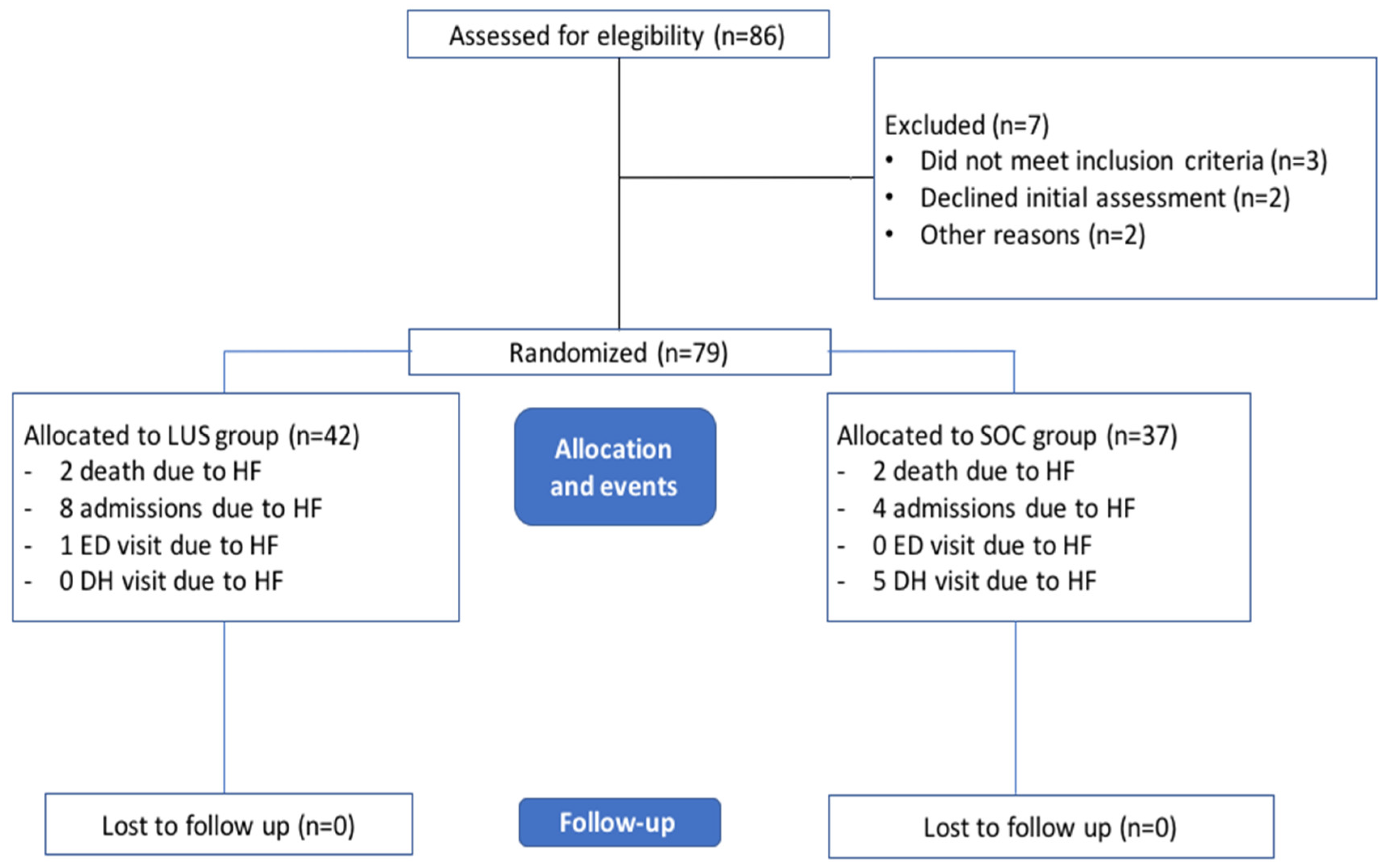
3. Results
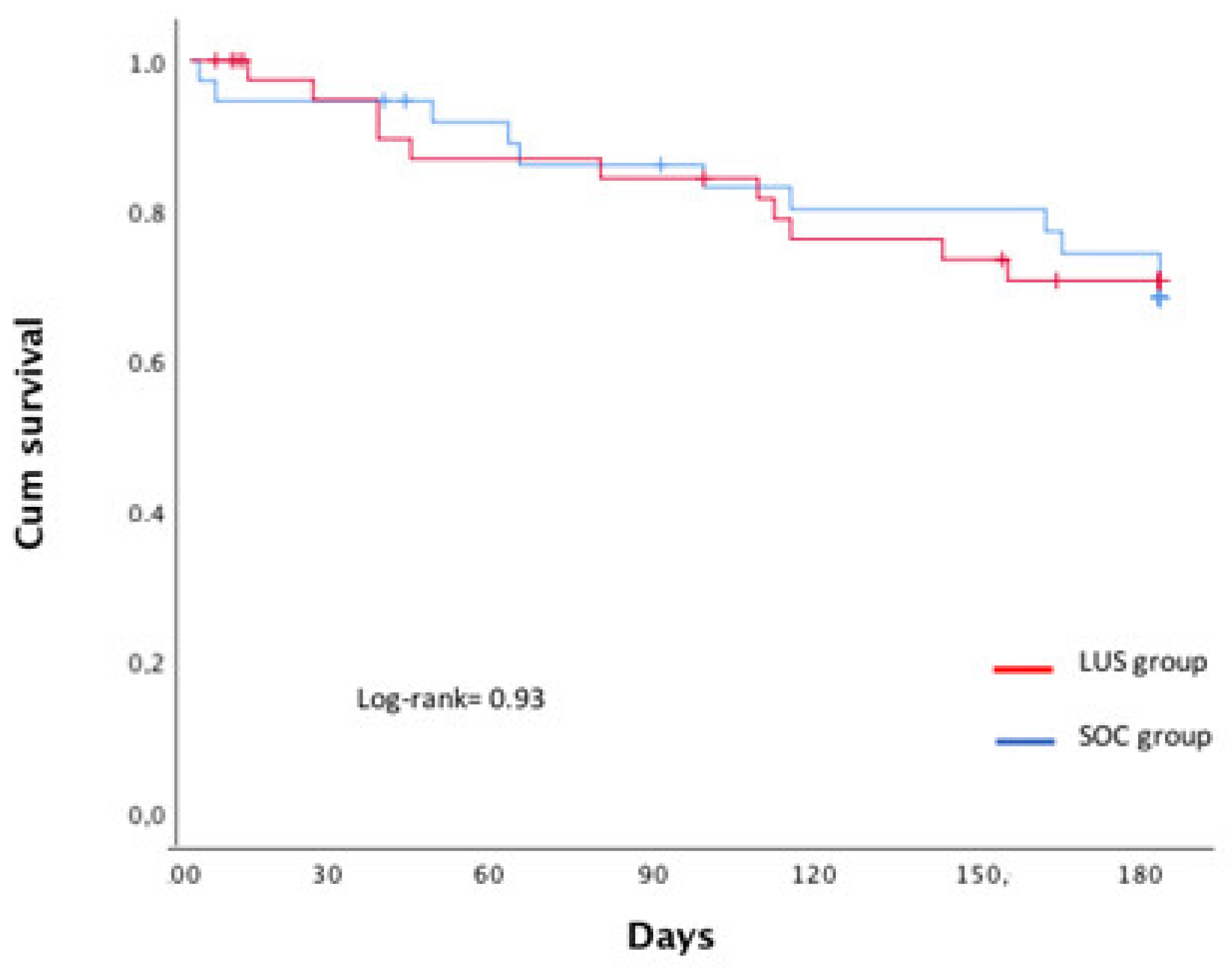
3.1. Study Outcomes
3.2. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mullens, W.; Damman, K.; Harjola, V.P.; Mebazaa, A.; Brunner-La Rocca, H.P.; Martens, P.; Testani, J.M.; Tang, W.H.W.; Orso, F.; Rossignol, P.; et al. The use of diuretics in heart failure with congestion—A position statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 137–155. [Google Scholar] [CrossRef] [PubMed]
- Fonarow, G.C.; Heywood, J.T.; Heidenreich, P.A.; Lopatin, M.; Yancy, C.W.; ADHERE Scientific Advisory Committee and Investigators. Temporal trends in clinical characteristics, treatments and outcomes for heart failure hospitalizations. 2002 to 2004: Findings from acute decomensated heart failure national registry (ADHERE). Am. Heart J. 2007, 153, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, C.M.; Abraham, W.T.; Albert, N.M.; Clare, R.; Stough, W.G.; Gheorghiade, M.; Greenberg, B.H.; Yancy, C.W.; Young, J.B.; Fanarow, G.C. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am. Heart J. 2008, 156, 662–673. [Google Scholar] [CrossRef] [PubMed]
- Gheorghiade, M.; Filippatos, G.; De Luca, L.; Burnett, J. Congestion in Acute Heart Failure Syndromes: An Essential Target of Evaluation and Treatment. Am. J. Med. 2006, 119, S3–S10. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Follath, F.; Ponikowski, P.; Barsuk, J.H.; Blair, J.E.; Cleland, J.G.; Dickstein, K.; Drazner, M.H.; Fonarow, G.C.; Jaarsma, T.; et al. Assessing and grading congestion in acute heart failure: A scientific statement from the Acute Heart Failure Committee of the Heart Failure Association of the European Society of Cardiology and endorsed by the European Society of Intensive Care Medicine. Eur. J. Heart Fail. 2010, 12, 423–433. [Google Scholar] [CrossRef]
- Platz, E.; Merz, A.; Jhund, P.; Vazir, A.; Campbell, R.; Mcmurray, J. Dynamic changes and prognostic value of pulmonary congestion by lung ultrasound in acute and chronic heart failure: A systematic review. Eur. J. Heart Fail. 2017, 19, 1154–1163. [Google Scholar] [CrossRef]
- Cotter, G.; Metra, M.; Milo-Cotter, O.; Dittrich, H.C.; Gheorghiade, M. Fluid overload in acute heart failure—Re-distribution and other mechanisms beyond fluid accumulation. Eur. J. Heart Fail. 2008, 10, 165–169. [Google Scholar] [CrossRef]
- Curbelo, J.; Rodriguez-Cortes, P.; Aguilera, M.; Gil-Martinez, P.; Martín, D.; Suarez Fernandez, C. Comparison between inferior vena cava ultrasound, lung ultrasound, bioelectric impedance analysis, and natriuretic peptides in chronic heart failure. Curr. Med. Res. Opin. 2019, 35, 705–713. [Google Scholar] [CrossRef]
- Di Somma, S.; Navarin, S.; Giordano, S.; Spadini, F.; Lippi, G.; Cervellin, G.; Dieffenbach, B.V.; Maisel, A.S. The emerging role of biomarkers and bio-impedance in evaluating hydration status in patients with acute heart failure. Clin. Chem. Lab. Med. (CCLM) 2012, 50, 2093–2105. [Google Scholar] [CrossRef]
- Platz, E.; Lewis, E.F.; Uno, H.; Peck, J.; Pivetta, E.; Merz, A.A.; Hempel, D.; Wilson, C.; Frasure, S.E.; Jhund, P.S.; et al. Detection and prognostic value of pulmonary conges-tion by lung ultrasound in ambulatory heart failure patients. Eur. Heart J. 2016, 36, 1244–1251. [Google Scholar] [CrossRef] [Green Version]
- Coiro, S.; Rossignol, P.; Ambrosio, G.; Carluccio, E.; Alunni, G.; Murrone, A.; Tritto, I.; Zannad, F.; Girerd, N. Prognostic value of residual pulmonary congestion at discharge assessed by lung ultrasound imaging in heart failure. Eur. Heart J. 2015, 17, 1172–1181. [Google Scholar] [CrossRef] [PubMed]
- Coiro, S.; Rossignol, P.; Ambrosio, G.; Carluccio, E.; Alunni, G.; Murrone, A.; Tritto, I.; Zannad, F.; Girerd, N. Prognostic value of pulmonary congestion assessed by lung ultrasound imaging during heart failure hospitalitation: A two-centre cohort study. Sci. Rep. 2016, 6, 39426. [Google Scholar] [CrossRef] [Green Version]
- Villanueva, M.D.C.T.; López, M.F.; Lebrato, J.C.; Bartolomé, J.S.; Prado, A.S.M.; Gaviria, A.Z. Utilidad pronóstica de la ecografía pulmonar en el seguimiento ambulatorio de pacientes con insuficiencia cardiaca. Med. Clin. 2016, 147, 13–15. [Google Scholar] [CrossRef]
- Trezzi, M.; Torzillo, D.; Ceriani, E. Lung ultrasonography for the assessment of rapid extravascular water variation: Evidence from hemodialysis patients. Intern. Emerg. Med. 2013, 8, 409–415. [Google Scholar] [CrossRef]
- Cortellaro, F.; Ceriani, E.; Spinelli, M.; Campanella, C.; Bossi, I.; Coen, D.; Casazza, G.; Cogliati, C. Lung ultrasound for monitoring cardiogenic pulmonary edema. Intern. Emerg. Med. 2016, 12, 1011–1017. [Google Scholar] [CrossRef]
- Gustafsson, M.; Alehagen, U.; Johansson, P. Imaging congestion with a pocket ultrasound device: Prognostic implications in patients with chronic heart failure. J. Card Fail. 2015, 21, 548–554. [Google Scholar] [CrossRef]
- Aras, M.A.; Teerlink, J.R. Lung ultrasound: A “B-Line” to the prediction of decompensated heart failure. Eur. Heart J. 2016, 14, 1252–1254. [Google Scholar] [CrossRef] [Green Version]
- Picano, E.; Pellikka, P.A. Ultrasound of extravascular lung water: A new standard for pulmonary congestion. Eur. Heart J. 2016, 37, 2097–2104. [Google Scholar] [CrossRef] [Green Version]
- Gundersen, G.H.; Norekvål, T.M.; Graven, T.; Haug, H.H.; Skjetne, K.; Kleinau, J.O.; Gustad, L.T.; Dalen, H. Patient-reported outcomes and associations with pleural effusion in outpatients with heart failure: An observational cohort study. BMJ Open 2017, 7, e013734. [Google Scholar] [CrossRef]
- Ohman, J.; Harjola, V.; Karjalainen, P.; Lassus, J. Focused echocardiography and lung ultrasound protocol for guiding treatment in acute heart failure. ESC Heart Fail. 2017, 5, 120–128. [Google Scholar] [CrossRef]
- Rivas-Lasarte, M.; Alvarez-Garcia, J.; Fernández-Martínez, J.; Maestro, A.; López-López, L.; Solé-González, E.; Pirla, M.J.; Mesado, N.; Mirabet, S.; Fluvià, P.; et al. Lung ultrasound-guided treatment in ambulatory patients with heart failure: A randomized controlled clinical trial (LUS-HF study). Eur. J. Heart Fail. 2019, 21, 1605–1613. [Google Scholar] [CrossRef] [PubMed]
- Marini, C.; Fragasso, G.; Italia, L.; Sisakian, H.; Tufaro, V.; Ingallina, G.; Stella, S.; Ancona, F.; Loiacono, F.; Inelli, P.; et al. Lung ultrasound-guided therapy reduces acute decompensation events in chronic heart failure. Heart 2020, 106, 1934–1939. [Google Scholar] [CrossRef] [PubMed]
- Araiza-Garaygordobil, D.; Gopar-Nieto, R.; Martinez-Amezcua, P.; Cabello-López, A.; Alanis-Estrada, G.; Luna-Herbert, A.; González-Pacheco, H.; Paredes-Paucar, C.P.; Sierra-Lara, M.D.; Briseño-De la Cruz, J.L.; et al. A randomized controlled trial of lung ultrasound-guided therapy in heart failure (CLUSTER-HF study). Am. Heart J. 2020, 227, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Bailón, M.M.; Rodrigo, J.M.C.; Lorenzo-Villalba, N.; Cerqueiro, J.M.; García, J.C.; Manuel, E.C.; Martín-Sánchez, F.J.; Freire, R.B.; Romano, P.C.; Espinosa, L.M.; et al. Effect of a Therapeutic Strategy Guided by Lung Ultrasound on 6-Month Outcomes in Patients with Heart Failure: Randomized, Multicenter Trial (EPICC Study). Cardiovasc. Drugs Ther. 2019, 33, 453–459. [Google Scholar] [CrossRef]
- Ambrosy, A.P.; Pang, P.S.; Khan, S.; Konstam, M.A.; Fonarow, G.C.; Traver, B.; Maggioni, A.P.; Cook, T.; Swedberg, K.; Everest Trial Investigators. Clinical course and predictive value of congestion during hospitalization in patients admitted for worsening signs and symptoms of heart failure with reduced ejection fraction: Findings from the EVEREST trial. Eur. Heart J. 2013, 34, 835–843. [Google Scholar] [CrossRef] [Green Version]
- González-Franco, Á.; González, J.C.; Arévalo-Lorido, J.; Álvarez-Rocha, P.; Carrascosa-García, S.; Armengou, A.; Guzmán-García, M.; Trullàs, J.; Montero-Pérez-Barquero, M.; Manzano, L. Morbidity and mortality in elderly patients with heart failure managed with a comprehensive care model vs. usual care: The UMIPIC program. Rev. Clin. Esp. (Barc.) 2022, 222, 123–130. [Google Scholar] [CrossRef]
- Palazzuoli, A.; Evangelista, I.; Beltrami, M.; Pirrotta, F.; Tavera, M.C.; Gennari, L.; Ruocco, G. Clinical, Laboratory and Lung Ultrasound Assessment of Congestion in Patients with Acute Heart Failure. J. Clin. Med. 2022, 11, 1642. [Google Scholar] [CrossRef]
- Domingo, M.; Conangla, L.; Lupón, J.; Wilke, A.; Juncà, G.; Revuelta-López, E.; Tejenor, X.; Bayes-Genis, A. Lung ultrasound and biomarkers in primary care: Partners for a better management of patients with heart failure? J. Circ. Biomark 2020, 9, 8–12. [Google Scholar] [CrossRef]
- Rivas-Lasarte, M.; Maestro, A.; Fernández-Martínez, J.; López-López, L.; Solé-González, E.; Vives-Borrás, M.; Montero, S.; Mesado, N.; Pirla, M.J.; Mirabet, S.; et al. Prevalence and prognostic impact of subclinical pulmonary congestion at discharge in patients with acute heart failure. ESC Heart Fail. 2020, 7, 2621–2628. [Google Scholar] [CrossRef]
- Mhanna, M.; Beran, A.; Nazir, S.; Sajdeya, O.; Srour, O.; Ayesh, H.; Eltahawy, E.A. Lung ultrasound-guided management to reduce hospitalization in chronic heart failure: A systematic review and meta-analysis. Heart Fail. Rev. 2021, 16, 79–96. [Google Scholar] [CrossRef]
- Pang, P.S.; Russell, F.M.; Ehrman, R.; Ferre, R.; Gargani, L.; Levy, P.D.; Noble, V.; Lane, K.A.; Li, X.; Collins, S.P. Lung Ultrasound–Guided Emergency Department Management of Acute Heart Failure (BLUSHED-AHF). JACC Heart Fail. 2021, 9, 638–648. [Google Scholar] [CrossRef]
- Pérez-Herrero, S.; Lorenzo-Villalba, N.; Urbano, E.; Sánchez-Sauce, B.; Aguilar-Rodríguez, F.; Bernabeu-Wittel, M.; Garcia-Alonso, R.; Soler-Rangel, L.; Trapiello-Valbuena, F.; Garcia-García, A.; et al. Prognostic Significance of Lung and Cava Vein Ultrasound in Elderly Patients Admitted for Acute Heart Failure: PROFUND-IC Registry Analysis. J. Clin. Med. 2022, 11, 4591. [Google Scholar] [CrossRef]
- Feijen, M.; Egorova, A.D.; Treskes, R.W.; Mertens, B.J.A.; Jukema, J.W.; Schalij, M.J.; Beeres, S.L.M.A. Performance of a HeartLogicTM Based Care Path in the Management of a Real-World Chronic Heart Failure Population. Front. Cardiovasc. Med. 2022, 9, 883873. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | Overall Sample (n = 79) | SOC Group (n = 37) | LUS Group (n = 42) | p Value |
|---|---|---|---|---|
| Age (years) (mean, SD) | 81.2 (8.9) | 82.8 (6.9) | 79.8 (10.2) | 0.13 |
| Male (n,%) | 36 (45.5) | 17 (45.9) | 19 (45.2) | 0.7 |
| Barthel index (n,%) | 81.8 (20.4) | 82.6 (21.3) | 81.1 (19.9) | 0.7 |
| HF aetiology | ||||
| Ischemic (n,%) | 20 (25.3) | 9 (24.3) | 11 (26.1) | 0.2 |
| Hypertension (n,%) | 38 (52.7) | 18 (48.6) | 20 (47.6) | 0.1 |
| Dilated (n,%) | 4 (5.5) | 1 (2.7) | 3 (7.1) | 0.09 |
| Alcohol (n,%) | 2 (2.5) | 0 (0) | 2 (4.7) | 0.3 |
| Other (n,%) | 22 (27.8) | 8 (21.6) | 14 (33.3) | 0.07 |
| Comorbidities | ||||
| Hypertension (n,%) | 69 (87.3%) | 31(83.7%) | 38 (90.4%) | 0.2 |
| Atrial fibrillation (n,%) | 41(51.8%) | 19(51.3%) | 22(52.3%) | 0.7 |
| Diabetes Mellitus (n,%) | 21 (26.5%) | 8 (21.6%) | 13 (30.9%) | 0.3 |
| CKD (n,%) | 33 (41.7%) | 13 (35.1%) | 20 (47.6%) | 0.2 |
| COPD (n,%) | 7 (8.85) | 4 (10.85) | 3 (7.1%) | 0.5 |
| Charlson index (n,%) | 4.14 (2.01) | 3.83 (2.04) | 4.4 (2.06) | 0.2 |
| NYHA class (n,%) | ||||
| I | 1 (1.25) | 1 (2.7%) | 0 (0%) | |
| II | 35 (44.3%) | 15 (40.5%) | 20 (47.6%) | |
| III | 40 (50.6%) | 19 (51.3%) | 21 (50%) | |
| IV | 3 (3.7%) | 2 (5.4%) | 1 (2.3%) | |
| Everest score (n,%) | 2.15 (1.83) | 2.19 (1.85) | 2.12 (1.86) | 0.85 |
| Treatment | ||||
| ACE-I/ARB (n,%) | 77 (97.4%) | 36 (97.2%) | 41 (97.6%) | 0.9 |
| B-blocker (n,%) | 64 (81%) | 30 (81%) | 34 (80.9%) | 0.78 |
| Loop diuretics (n,%) | 74 (93.6%) | 36 (97.2%) | 38 (90.4%) | 0.16 |
| Spironolactone (n,%) | 26 (32.9%) | 12 (32.4%) | 14 (33.3%) | 0.11 |
| Other diuretics (n,%) | 13 (16.4%) | 4 (10.8%) | 9 (21.4%) | 0.6 |
| Digoxin (n,%) | 3 (3.7%) | 0 (0%) | 3 (6.3%) | 0.11 |
| Anticoagulation (n,%) | 44 (55.6%) | 22 (59.4%) | 24 (57.1%) | 0.61 |
| B-lines (>3) | ||||
| RUC | 14 (35.9%) | |||
| LUC | 10 (25.7%) | |||
| RLC | 17 (53.6%) | |||
| LLC | 15 (38.4%) | |||
| Pleural effusion (n, %) | 8 (20.5%) | |||
| LVEF > 50% (n, %) | 41 (51.8) | 18 (48.6%) | 23 (54.7%) | 0.7 |
| Laboratory results | ||||
| NT-proBNP (pg/mL) Median (IQR 25–75) | 4159 (2218–8073) | 3818 (2124–7553) | 4938 (2403–8780) | 0.9 |
| Creatinine (mg/dL) (mean, SD) | 1.34 (0.53) | 1.23 (0.51) | 1.43 (0.55) | 0.14 |
| eGFR (mL/min) (mean, SD) | 49.2 (20.9) | 53.1 (19.8) | 46 (21.5) | 0.14 |
| Haemoglobin (mg/dL) (mean, SD) | 11.9 (1.7) | 11.7 (1.7) | 12 (1.7) | 0.49 |
| Variable | SOC Group | LUS Group | p Value |
|---|---|---|---|
| Diuretic Therapy titration (mg) | |||
| MDD at baseline | 76.1 (6.7) | 80.3 (12.2) | 0.76 |
| MDD at visit 1 (7 days) | 64.6 (5.3) | 75.6 (8.3) | 0.28 |
| MDD at visit 2 (30 days) | 65.6 (6.2) | 80.7 (18.1) | 0.4 |
| MDD at visit 3 (90 days) | 68 (6.9) | 80 (18.6) | 0.54 |
| MDD at visit 4 (180 days) | 74.7 (5.2) | 66.6 (20.2) | 0.5 |
| Endpoint | SOC Group | LUS Group | Relative Risk | p Value |
|---|---|---|---|---|
| Admission due to ADHF | 4 (10.8%) | 8 (19%) | 1.9 (0.53–7.06) | 0.3 |
| ED visit due to ADHF | 0 (0%) | 1 (2.3%) | 1.96 (1.56–2.43) | 0.33 |
| Furosemide at HD | 5 (13.5%) | 0 (0%) | 0.4 (0.33–0.56) | 0.019 |
| Death due to ADHF | 2 (5.4%) | 2 (4.7%) | 0.87 (0.11–6.54) | 0.89 |
| Composite endpoint | 11 (29.7%) | 11 (26.1%) | 0.83 (0.31–2.24) | 0.72 |
| Adverse Events | SOC Group | LUS Group | p-Value |
|---|---|---|---|
| Acute renal failure | 7 (18.9%) | 9 (21.4%) | 0.7 |
| Hypotension | 1 (2.7%) | 4 (9.5%) | 0.2 |
| Hyponatremia | 1 (2.7%) | 1 (2.3%) | 0.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torres-Macho, J.; Cerqueiro-González, J.M.; Arévalo-Lorido, J.C.; Llácer-Iborra, P.; Cepeda-Rodrigo, J.M.; Cubo-Romano, P.; Casas-Rojo, J.M.; Ruiz-Ortega, R.; Manzano-Espinosa, L.; Lorenzo-Villalba, N.; et al. The Effects of a Therapeutic Strategy Guided by Lung Ultrasound on 6-Month Outcomes in Patients with Heart Failure: Results from the EPICC Randomized Controlled Trial. J. Clin. Med. 2022, 11, 4930. https://doi.org/10.3390/jcm11164930
Torres-Macho J, Cerqueiro-González JM, Arévalo-Lorido JC, Llácer-Iborra P, Cepeda-Rodrigo JM, Cubo-Romano P, Casas-Rojo JM, Ruiz-Ortega R, Manzano-Espinosa L, Lorenzo-Villalba N, et al. The Effects of a Therapeutic Strategy Guided by Lung Ultrasound on 6-Month Outcomes in Patients with Heart Failure: Results from the EPICC Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(16):4930. https://doi.org/10.3390/jcm11164930
Chicago/Turabian StyleTorres-Macho, Juan, Jose Manuel Cerqueiro-González, Jose Carlos Arévalo-Lorido, Pau Llácer-Iborra, Jose María Cepeda-Rodrigo, Pilar Cubo-Romano, Jose Manuel Casas-Rojo, Raúl Ruiz-Ortega, Luis Manzano-Espinosa, Noel Lorenzo-Villalba, and et al. 2022. "The Effects of a Therapeutic Strategy Guided by Lung Ultrasound on 6-Month Outcomes in Patients with Heart Failure: Results from the EPICC Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 16: 4930. https://doi.org/10.3390/jcm11164930
APA StyleTorres-Macho, J., Cerqueiro-González, J. M., Arévalo-Lorido, J. C., Llácer-Iborra, P., Cepeda-Rodrigo, J. M., Cubo-Romano, P., Casas-Rojo, J. M., Ruiz-Ortega, R., Manzano-Espinosa, L., Lorenzo-Villalba, N., & Méndez-Bailón, M. (2022). The Effects of a Therapeutic Strategy Guided by Lung Ultrasound on 6-Month Outcomes in Patients with Heart Failure: Results from the EPICC Randomized Controlled Trial. Journal of Clinical Medicine, 11(16), 4930. https://doi.org/10.3390/jcm11164930