
Effectiveness of Nootropics in Combination with Cholinesterase Inhibitors on Cognitive Function in Mild-to-Moderate Dementia: A Study Using Real-World Data


Abstract
:1. Introduction
2. Materials and Methods
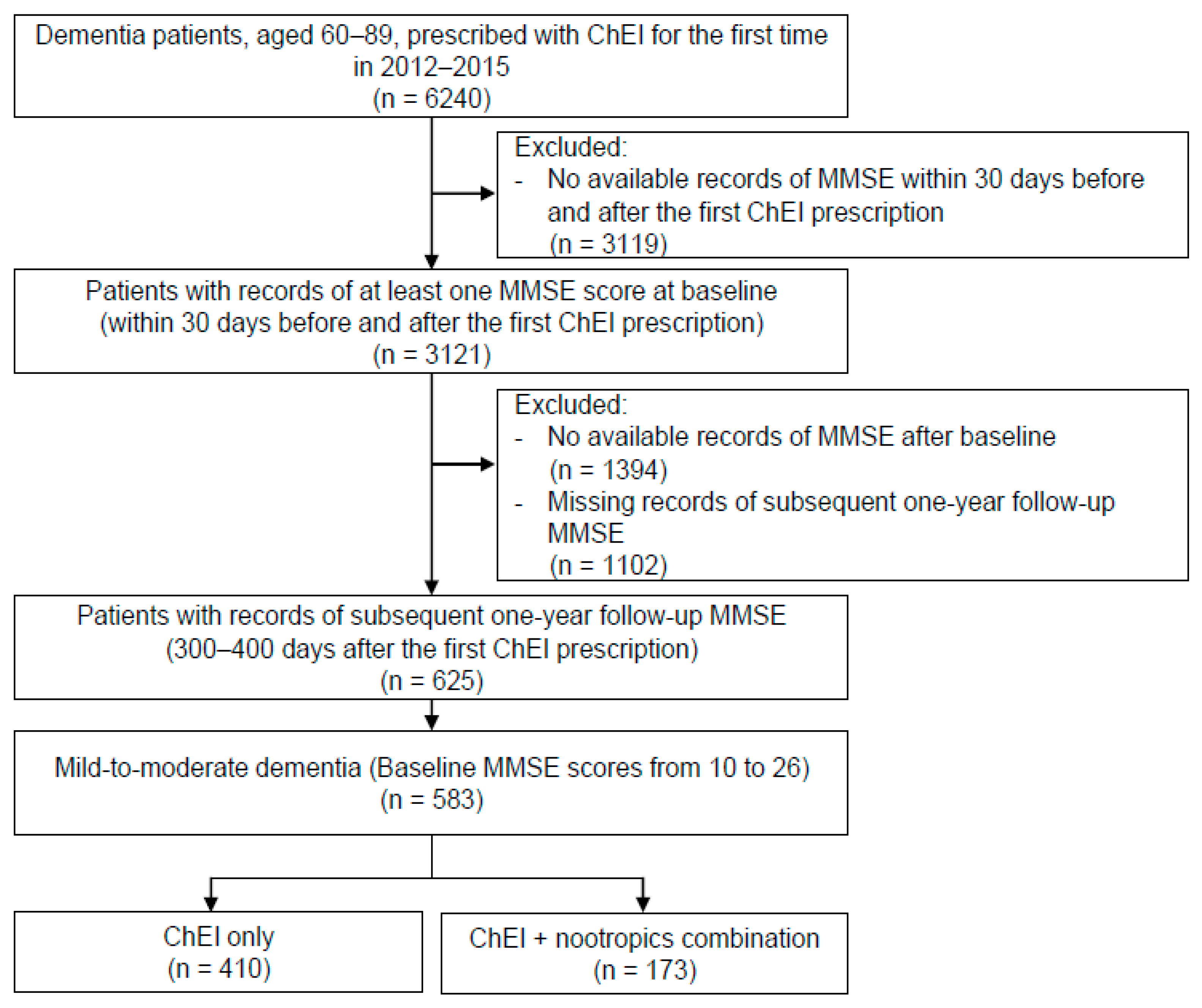
2.1. Study Population
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Change in Cognitive Function: ChEI Only vs. ChEI and Nootropics Combination Group
3.3. Change in Cognitive Function for Each Type of Dementia: Alzheimer’s Dementia, Vascular Dementia, and Other Dementia
3.4. Subgroup Analysis within the ChEI and Nootropics Combination Group in Alzheimer’s Dementia: Choline Alfoscerate vs. Ginkgo Biloba Extract vs. Other Nootropics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Dementia. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 18 September 2021).
- O’Brien, J.T.; Holmes, C.; Jones, M.; Jones, R.; Livingston, G.; McKeith, I.; Mittler, P.; Passmore, P.; Ritchie, C.; Robinson, L.; et al. Clinical practice with anti-dementia drugs: A revised (third) consensus statement from the British association for psychopharmacology. J. Psychopharmacol. 2017, 31, 147–168. [Google Scholar] [CrossRef] [PubMed]
- Birks, J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database Syst. Rev. 2006, 1, CD005593. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, C.D. Pharmacology of nootropics and metabolically active compounds in relation to their use in dementia. Psychopharmacology 1990, 101, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Moreno, M.D. Cognitive improvement in mild to moderate Alzheimer’s dementia after treatment with the acetylcholine precursor choline alfoscerate: A multicenter, double-blind, randomized, placebo-controlled trial. Clin. Ther. 2003, 25, 178–193. [Google Scholar] [CrossRef]
- Montgomery, S.A.; Thal, L.J.; Amrein, R. Meta-analysis of double blind randomized controlled clinical trials of acetyl-L-carnitine versus placebo in the treatment of mild cognitive impairment and mild Alzheimer’s disease. Int. Clin. Psychopharmacol. 2003, 18, 61–71. [Google Scholar] [CrossRef]
- Parnetti, L.; Amenta, F.; Gallai, V. Choline alphoscerate in cognitive decline and in acute cerebrovascular disease: An analysis of published clinical data. Mech. Ageing Dev. 2001, 122, 2041–2055. [Google Scholar] [CrossRef]
- Parnetti, L.; Abate, G.; Bartorelli, L.; Cucinotta, D.; Cuzzupoli, M.; Maggioni, M.; Villardita, C.; Senin, U. Multicentre study of l-alpha-glyceryl-phosphorylcholine vs. ST200 among patients with probable senile dementia of Alzheimer’s type. Drugs Aging 1993, 3, 159–164. [Google Scholar] [CrossRef]
- Parnetti, L.; Mignini, F.; Tomassoni, D.; Traini, E.; Amenta, F. Cholinergic precursors in the treatment of cognitive impairment of vascular origin: Ineffective approaches or need for re-evaluation? J. Neurol. Sci. 2007, 257, 264–269. [Google Scholar] [CrossRef]
- DeKosky, S.T.; Williamson, J.D.; Fitzpatrick, A.L.; Kronmal, R.A.; Ives, D.G.; Saxton, J.A.; Lopez, O.L.; Burke, G.; Carlson, M.C.; Fried, L.P.; et al. Ginkgo biloba for prevention of dementia: A randomized controlled trial. JAMA 2008, 300, 2253–2262. [Google Scholar] [CrossRef]
- Gschwind, Y.J.; Bridenbaugh, S.A.; Reinhard, S.; Granacher, U.; Monsch, A.U.; Kressig, R.W. Ginkgo biloba special extract LI 1370 improves dual-task walking in patients with MCI: A randomised, double-blind, placebo-controlled exploratory study. Aging Clin. Exp. Res. 2017, 29, 609–619. [Google Scholar] [CrossRef] [Green Version]
- Spagnoli, A.; Lucca, U.; Menasce, G.; Bandera, L.; Cizza, G.; Forloni, G. Long-term acetyl-L-carnitine treatment in Alzheimer’s disease. Neurology 1991, 41, 1726–1732. [Google Scholar] [CrossRef] [PubMed]
- Zang, G.; Fang, L.; Chen, L.; Wang, C. Ameliorative effect of nicergoline on cognitive function through the PI3K/AKT signaling pathway in mouse models of Alzheimer’s disease. Mol. Med. Rep. 2018, 17, 7293–7300. [Google Scholar] [CrossRef] [PubMed]
- Nappi, G.; Bono, G.; Merlo, P.; Borromei, A.; Caltagirone, C.; Lomeo, C.; Martucci, N.; Fabbrini, G.; Annoni, K.; Battaglia, A. Long-Term nicergoline treatment of mild to moderate senile dementia. Clin. Drug Investig. 1997, 13, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.; Coley, N.; Ousset, P.-J.; Berrut, G.; Dartigues, J.-F.; Dubois, B.; Grandjean, H.; Pasquier, F.; Piette, F.; Robert, P.; et al. Long-term use of standardised ginkgo biloba extract for the prevention of Alzheimer’s disease (GuidAge): A randomised placebo-controlled trial. Lancet Neurol. 2012, 11, 851–859. [Google Scholar] [CrossRef]
- Snitz, B.E.; O’Meara, E.S.; Carlson, M.C.; Arnold, A.M.; Ives, D.G.; Rapp, S.R.; Saxton, J.; Lopez, O.L.; Dunn, L.O.; Sink, K.M.; et al. Ginkgo biloba for preventing cognitive decline in older adults: A randomized trial. JAMA 2009, 302, 2663–2670. [Google Scholar] [CrossRef] [Green Version]
- Hudson, S.; Tabet, N. Acetyl-L-carnitine for dementia. Cochrane Database Syst. Rev. 2003, 2003, CD003158. [Google Scholar] [CrossRef]
- Fioravanti, M.; Flicker, L. Efficacy of nicergoline in dementia and other age associated forms of cognitive impairment. Cochrane Database of Syst. Rev. 2001, 4, CD003159. [Google Scholar]
- Amenta, F.; Carotenuto, A.; Fasanaro, A.M.; Rea, R.; Traini, E. The ASCOMALVA trial: Association between the cholinesterase inhibitor donepezil and the cholinergic precursor choline alphoscerate in Alzheimer’s disease with cerebrovascular injury: Interim results. J. Neurol. Sci. 2012, 322, 96–101. [Google Scholar] [CrossRef]
- Amenta, F.; Tayebati, S.K.; Vitali, D.; di Tullio, M.A. Association with the cholinergic precursor choline alphoscerate and the cholinesterase inhibitor rivastigmine: An approach for enhancing cholinergic neurotransmission. Mech. Ageing Dev. 2006, 127, 173–179. [Google Scholar] [CrossRef]
- Traini, E.; Carotenuto, A.; Fasanaro, A.M.; Amenta, F. Volume analysis of brain cognitive areas in Alzheimer’s disease: Interim 3-year results from the ASCOMALVA trial. J. Alzheimers Dis. 2020, 76, 317–329. [Google Scholar] [CrossRef]
- Dao, N.; Lee, S.; Hata, M.; Sarino, L. Impact of appointment-based medication synchronization on proportion of days covered for chronic medications. Pharmacy 2018, 6, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Flicker, L. Lecithin for dementia and cognitive impairment. Cochrane Database Syst. Rev. 2003, 3, CD001015. [Google Scholar] [CrossRef] [PubMed]
- Birks, J.; Grimley Evans, J. Ginkgo biloba for cognitive impairment and dementia. Cochrane Database Syst. Rev. 2009, 1, CD003120. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Xie, Y.; Qi, M.; Zhang, L.; Wang, W.; Zhang, W.; Sha, L.; Wu, J.; Li, W.; Wu, T. Ginkgo biloba extract is comparable with donepezil in improving functional recovery in Alzheimer’s disease: Results from a multilevel characterized study based on clinical features and resting-state functional magnetic resonance imaging. Front. Pharmacol. 2021, 12, 721216. [Google Scholar] [CrossRef]
- Catanesi, M.; d’Angelo, M.; Antonosante, A.; Castelli, V.; Alfonsetti, M.; Benedetti, E.; Desideri, G.; Ferri, C.; Cimini, A. Neuroprotective potential of choline alfoscerate against β-amyloid injury: Involvement of neurotrophic signals. Cell Biol. Int. 2020, 44, 1734–1744. [Google Scholar] [CrossRef]
- Sigala, S.; Imperato, A.; Rizzonelli, P.; Casolini, P.; Missale, C.; Spano, P. L-alpha-glycerylphosphorylcholine antagonizes scopolamine-induced amnesia and enhances hippocampal cholinergic transmission in the rat. Eur. J. Pharmacol. 1992, 211, 351–358. [Google Scholar] [CrossRef]
- Tayebati, S.K.; di Tullio, M.A.; Tomassoni, D.; Amenta, F. Neuroprotective effect of treatment with galantamine and choline alphoscerate on brain microanatomy in spontaneously hypertensive rats. J. Neurol. Sci. 2009, 283, 187–194. [Google Scholar] [CrossRef]
- Lee, S.H.; Choi, B.Y.; Kim, J.H.; Kho, A.R.; Sohn, M.; Song, H.K.; Choi, H.C.; Suh, S.W. Late treatment with choline alfoscerate (l-alpha glycerylphosphorylcholine, α-GPC) increases hippocampal neurogenesis and provides protection against seizure-induced neuronal death and cognitive impairment. Brain Res. 2017, 1654, 66–76. [Google Scholar] [CrossRef]
- Na, G.; Kwak, S.H.; Jang, S.H.; Noh, H.E.; Kim, J.; Yang, S.; Jung, J. Supplementary effect of choline alfoscerate on speech recognition in patients with age-related hearing loss: A prospective study in 34 patients (57 ears). Front. Aging Neurosci. 2021, 13, 684519. [Google Scholar] [CrossRef]
- Bastianetto, S.; Ramassamy, C.; Doré, S.; Christen, Y.; Poirier, J.; Quirion, R. The ginkgo biloba extract (EGb 761) protects hippocampal neurons against cell death induced by beta-amyloid. Eur. J. Neurosci. 2000, 12, 1882–1890. [Google Scholar] [CrossRef]
- Luo, Y.; Smith, J.V.; Paramasivam, V.; Burdick, A.; Curry, K.J.; Buford, J.P.; Khan, I.; Netzer, W.J.; Xu, H.; Butko, P. Inhibition of amyloid-β aggregation and caspase-3 activation by the ginkgo biloba extract EGb761. Proc. Natl. Acad. Sci. USA 2002, 99, 12197–12202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tchantchou, F.; Xu, Y.; Wu, Y.; Christen, Y.; Luo, Y. EGb 761 enhances adult hippocampal neurogenesis and phosphorylation of CREB in transgenic mouse model of Alzheimer’s disease. FASEB J. 2007, 21, 2400–2408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadjiivanova, C.I.; Petkov, V.V. Effect of Ginkgo biloba extract on β-adrenergic receptors in different rat brain regions. Phytother. Res. 2002, 16, 488–490. [Google Scholar] [CrossRef] [PubMed]
- Van de Ven, V.; Waldorp, L.; Christoffels, I. Hippocampus plays a role in speech feedback processing. Neuroimage 2020, 223, 117319. [Google Scholar] [CrossRef]
- Alegret, M.; Peretó, M.; Pérez, A.; Valero, S.; Espinosa, A.; Ortega, G.; Hernández, I.; Mauleón, A.; Rosende-Roca, M.; Vargas, L.; et al. The role of verb fluency in the detection of early cognitive impairment in Alzheimer’s disease. J. Alzheimers Dis. 2018, 62, 611–619. [Google Scholar] [CrossRef] [Green Version]
- Salmon, D.P.; Bondi, M.W. Neuropsychological assessment of dementia. Annu. Rev. Psychol. 2009, 60, 257–282. [Google Scholar] [CrossRef] [Green Version]
- Ryu, D.-R. Introduction to the medical research using national health insurance claims database. Ewha Med. J. 2017, 40, 66–70. [Google Scholar] [CrossRef] [Green Version]
- Colucci, L.; Bosco, M.; Rosario Ziello, A.; Rea, R.; Amenta, F.; Fasanaro, A.M. Effectiveness of nootropic drugs with cholinergic activity in treatment of cognitive deficit: A review. J. Exp. Pharmacol. 2012, 4, 163–172. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | ChEI Only (n = 410) | ChEI + Nootropics (n = 173) | p Value |
|---|---|---|---|
| Age (years) | 75.5 ± 6.5 | 75.5 ± 6.6 | 0.880 |
| Weight (kg) 1 | 56.4 ± 9.8 | 56.7 ± 12.2 | 0.843 |
| Height (cm) 2 | 157.3 ± 10.1 | 156.1 ± 11.5 | 0.274 |
| BMI (kg/m2) 3 | 22.8 ± 3.8 | 23.3 ± 3.8 | 0.265 |
| Blood pressure (mmHg) 4 | |||
| Systolic | 130.3 ± 20.8 | 129.1 ± 22.1 | 0.576 |
| Diastolic | 75.6 ± 12.9 | 75.6 ± 12.9 | 0.962 |
| Sex | |||
| Male | 144 (35.1) | 56 (32.4) | 0.523 |
| Female | 266 (64.9) | 117 (67.6) | |
| Education (years) 5 | |||
| No education | 55 (13.4) | 20 (11.6) | 0.651 |
| Elementary school | 94 (22.9) | 43 (24.9) | |
| Middle/high school | 90 (21.9) | 31 (7.9) | |
| Bachelor’s/master’s degree | 64 (15.6) | 30 (17.3) | |
| Alcohol use 6 | |||
| Yes | 85 (20.7) | 23 (13.3) | 0.011 |
| No | 203 (49.5) | 107 (61.8) | |
| Tobacco use 7 | |||
| Yes | 23 (5.6) | 7 (4.0) | 0.245 |
| No | 224 (54.6) | 114 (65.9) | |
| Psychiatric medication | |||
| Antipsychotics | 73 (17.8) | 34 (19.7) | 0.598 |
| Benzodiazepines, hypnotics | 119 (29.0) | 45 (26.0) | 0.460 |
| Anticholinergics | 83 (20.2) | 43 (24.9) | 0.217 |
| Dementia diagnoses | |||
| Alzheimer’s dementia | 313 (76.3) | 134 (77.5) | 0.771 |
| Vascular dementia | 49 (12.0) | 31 (17.9) | 0.056 |
| Unspecified dementia | 17 (4.1) | 6 (3.5) | 0.701 |
| Frontotemporal dementia | 8 (2.0) | 0 (0) | 0.113 |
| Progressive supranuclear palsy | 16 (3.9) | 0 (0) | 0.004 |
| Alcohol induced persisting dementia | 1 (0.2) | 0 (0) | 1.000 |
| Other specified degenerative disease of nervous system | 6 (1.5) | 2 (1.2) | 1.000 |
| Comorbid diagnoses | |||
| Diabetes mellitus | 81 (19.8) | 50 (28.9) | 0.016 |
| Hypertension | 138 (33.7) | 70 (40.5) | 0.117 |
| Hyperlipidemia | 55 (13.4) | 29 (16.8) | 0.293 |
| Stroke 8 | 36 (8.8) | 36 (20.8) | <0.001 |
| Parkinsonism | 69 (16.8) | 12 (6.9) | 0.002 |
| Visual disturbance/hearing loss | 26 (6.3) | 20 (11.6) | 0.033 |
| Hemiplegia/paraplegia | 3 (0.7) | 6 (3.5) | 0.023 |
| Asthma/COPD | 18 (4.4) | 11 (6.4) | 0.318 |
| Renal insufficiency | 25 (6.1) | 14 (8.1) | 0.378 |
| Mood/anxiety disorder | 141 (34.4) | 75 (43.4) | 0.041 |
| Other psychiatric disorder 9 | 26 (6.3) | 12 (6.9) | 0.790 |
| Any malignancy | 26 (6.3) | 10 (5.8) | 0.797 |
| Baseline | Endpoint | Difference in Scores | Group-Time Interaction 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| MMSE | ChEI Only | ChEI + Nootropics | p Value 3 | ChEI Only | ChEI + Nootropics | p Value 3 | ChEI Only | ChEI + Nootropics | p Value 3 | F | p Value 4 |
| Total | 20.00 ± 4.30 | 20.27 ± 4.26 | 0.487 | 18.87 ± 5.43 | 19.56 ± 5.13 | 0.152 | −1.13 ± 3.98 | −0.71 ± 3.47 | 0.199 | 1.48 | 0.224 |
| Orientation | 6.81 ± 2.33 | 6.94 ± 2.23 | 0.533 | 6.28 ± 2.70 | 6.54 ± 2.57 | 0.276 | −0.53 ± 2.21 | −0.40 ± 2.15 | 0.504 | 0.45 | 0.504 |
| Immediate recall | 2.83 ± 0.47 | 2.84 ± 0.47 | 0.925 | 2.74 ± 0.63 | 2.77 ± 0.59 | 0.526 | −0.10 ± 0.66 | −0.06 ± 0.63 | 0.594 | 0.28 | 0.594 |
| Attention & calculation | 1.99 ± 1.58 | 2.01 ± 1.57 | 0.881 | 1.81 ± 1.58 | 1.95 ± 1.62 | 0.327 | −0.18 ± 1.53 | −0.06 ± 1.29 | 0.364 | 0.83 | 0.364 |
| Delayed recall | 0.92 ± 1.00 | 1.10 ± 1.11 | 0.064 | 0.90 ± 1.06 | 0.93 ± 1.10 | 0.715 | −0.03 ± 1.02 | −0.17 ± 1.16 | 0.150 | 2.29 | 0.131 |
| Language | 6.97 ± 1.22 | 6.87 ± 1.41 | 0.387 | 6.70 ± 1.46 | 6.84 ± 1.55 | 0.295 | −0.27 ± 1.45 | −0.03 ± 1.43 | 0.065 | 3.43 | 0.065 |
| Visuospatial construction | 0.47 ± 0.50 | 0.50 ± 0.50 | 0.561 | 0.44 ± 0.50 | 0.51 ± 0.50 | 0.111 | −0.03 ± 0.56 | 0.01 ± 0.58 | 0.375 | 0.79 | 0.375 |
| Alzheimer’s Dementia (n = 447) | Vascular Dementia (n = 80) | Others (n = 56) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Difference in Scores | Group-Time Interaction | Difference in Scores | Group-Time Interaction | Difference in Scores | Group-Time Interaction | |||||||
| MMSE | ChEI Only (n = 313) | ChEI + Nootropics (n = 134) | F | p Value | ChEI Only (n = 49) | ChEI + Nootropics (n = 31) | F | p Value | ChEI Only (n = 48) | ChEI + Nootropics (n = 8) | F | p Value |
| Total | −1.30 ± 3.87 | −0.75 ± 3.27 | 2.10 | 0.148 | −0.88 ± 3.46 | −0.35 ± 4.06 | 0.38 | 0.540 | −0.27 ± 5.04 | −1.38 ± 4.66 | 0.04 | 0.906 |
| Orientation | −0.62 ± 2.16 | −0.45 ± 1.91 | 0.66 | 0.417 | −0.33 ± 2.04 | −0.16 ± 3.03 | 0.09 | 0.771 | −0.15 ± 2.67 | −0.50 ± 1.93 | 0.14 | 0.707 |
| Immediate recall | −0.08 ± 0.65 | −0.09 ± 0.62 | 0.01 | 0.922 | −0.12 ± 0.81 | 0.10 ± 0.70 | 1.55 | 0.217 | −0.15 ± 0.62 | −0.25 ± 0.46 | 0.01 | 0.937 |
| Attention & calculation | −0.18 ± 1.50 | −0.11 ± 1.28 | 0.21 | 0.651 | −0.59 ± 1.38 | 0.06 ± 1.32 | 4.44 | 0.038 | 0.25 ± 1.77 | 0.38 ± 1.41 | 1.13 | 0.293 |
| Delayed recall | −0.02 ± 1.05 | −0.19 ± 1.15 | 2.46 | 0.117 | 0.00 ± 0.94 | −0.13 ± 1.15 | 0.30 | 0.584 | −0.10 ± 0.99 | 0.00 ± 1.51 | 1.35 | 0.252 |
| Language | −0.34 ± 1.45 | 0.04 ± 1.39 | 6.86 | 0.009 | 0.14 ± 1.04 | −0.10 ± 1.11 | 0.96 | 0.331 | −0.23 ± 1.72 | −1.00 ± 2.67 | 1.90 | 0.175 |
| Visuospatial construction | −0.05 ± 0.57 | 0.05 ± 0.58 | 3.28 | 0.071 | −0.04 ± 0.54 | −0.16 ± 0.53 | 0.97 | 0.327 | 0.56 ± 0.08 | 0.76 ± 0.27 | 0.18 | 0.677 |
| Alzheimer’s Dementia (n = 412) | Vascular Dementia (n = 72) | Others (n = 53) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Difference in Scores | Group-Time Interaction | Difference in Scores | Group-Time Interaction | Difference in Scores | Group-Time Interaction | |||||||
| MMSE | ChEI Only (n = 300) | ChEI + Nootropics (n = 112) | F | p Value | ChEI Only (n = 45) | ChEI + Nootropics (n = 27) | F | p Value | ChEI Only (n = 45) | ChEI + Nootropics (n = 8) | F | p Value |
| Total | −1.36 ± 3.87 | −0.77 ± 2.85 | 2.18 | 0.141 | −0.78 ± 3.51 | −0.59 ± 4.17 | 0.04 | 0.841 | −0.36 ± 5.19 | −1.38 ± 4.66 | 0.27 | 0.606 |
| Orientation | −0.64 ± 2.16 | −0.54 ± 1.82 | 0.22 | 0.640 | −0.38 ± 1.84 | −0.22 ± 3.23 | 0.07 | 0.795 | −0.18 ± 2.76 | −0.50 ± 1.93 | 0.10 | 0.753 |
| Immediate recall | −0.08 ± 0.66 | −0.07 ± 0.57 | 0.03 | 0.865 | −0.13 ± 0.84 | 0.11 ± 0.75 | 1.54 | 0.219 | −0.16 ± 0.64 | −0.25 ± 0.46 | 0.16 | 0.692 |
| Attention & calculation | −0.18 ± 1.49 | −0.12 ± 1.32 | 0.16 | 0.689 | −0.58 ± 1.42 | 0.04 ± 1.22 | 0.04 | 0.841 | 0.13 ± 1.75 | 0.38 ± 1.41 | 0.14 | 0.714 |
| Delayed recall | −0.01 ± 1.03 | −0.22 ± 1.11 | 3.35 | 0.068 | 0.07 ± 0.92 | −0.19 ± 1.15 | 1.06 | 0.307 | −0.07 ± 0.99 | 0.00 ± 1.51 | 0.03 | 0.872 |
| Language | −0.38 ± 1.46 | 0.12 ± 1.26 | 10.16 | 0.002 | 0.20 ± 1.04 | −0.14 ± 1.11 | 2.21 | 0.142 | −0.22 ± 1.74 | −1.00 ± 2.67 | 1.14 | 0.291 |
| Visuospatial construction | −0.06 ± 0.56 | 0.06 ± 0.59 | 4.00 | 0.046 | −0.02 ± 0.54 | −0.15 ± 0.53 | 0.92 | 0.341 | 0.13 ± 0.55 | 0.00 ± 0.76 | 0.36 | 0.552 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, M.; Lee, D.B.; Kwon, S.; Lee, E.; Kim, W.J. Effectiveness of Nootropics in Combination with Cholinesterase Inhibitors on Cognitive Function in Mild-to-Moderate Dementia: A Study Using Real-World Data. J. Clin. Med. 2022, 11, 4661. https://doi.org/10.3390/jcm11164661
Kang M, Lee DB, Kwon S, Lee E, Kim WJ. Effectiveness of Nootropics in Combination with Cholinesterase Inhibitors on Cognitive Function in Mild-to-Moderate Dementia: A Study Using Real-World Data. Journal of Clinical Medicine. 2022; 11(16):4661. https://doi.org/10.3390/jcm11164661
Chicago/Turabian StyleKang, Minjae, Dan Bee Lee, Sungchan Kwon, Eun Lee, and Woo Jung Kim. 2022. "Effectiveness of Nootropics in Combination with Cholinesterase Inhibitors on Cognitive Function in Mild-to-Moderate Dementia: A Study Using Real-World Data" Journal of Clinical Medicine 11, no. 16: 4661. https://doi.org/10.3390/jcm11164661
APA StyleKang, M., Lee, D. B., Kwon, S., Lee, E., & Kim, W. J. (2022). Effectiveness of Nootropics in Combination with Cholinesterase Inhibitors on Cognitive Function in Mild-to-Moderate Dementia: A Study Using Real-World Data. Journal of Clinical Medicine, 11(16), 4661. https://doi.org/10.3390/jcm11164661