
The Effect of Stabilization Procedures on Sports Discipline and Performance Level in Non-Elite Athletes after Acute Syndesmotic Injury: A Prospective Randomized Trial

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
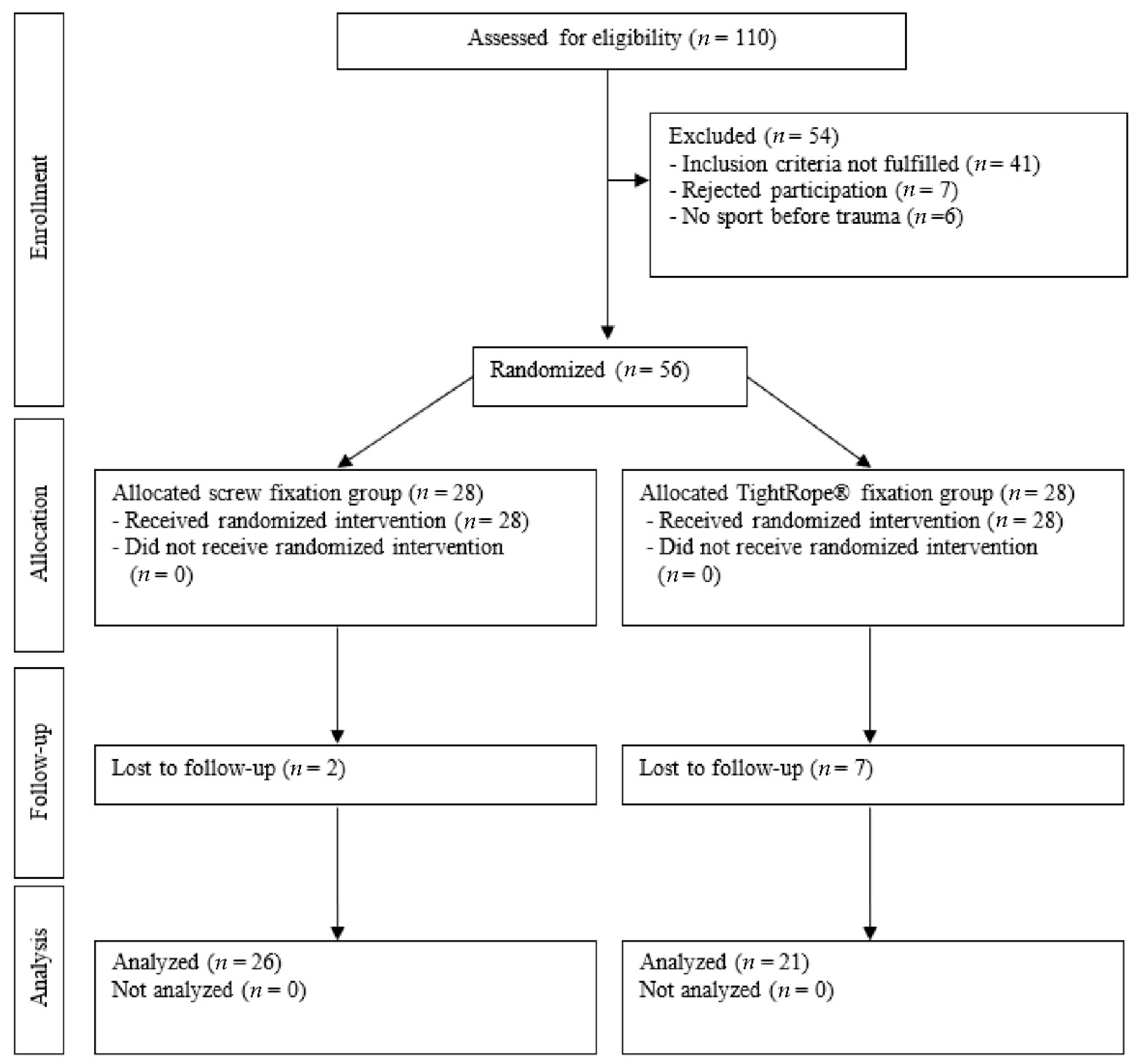
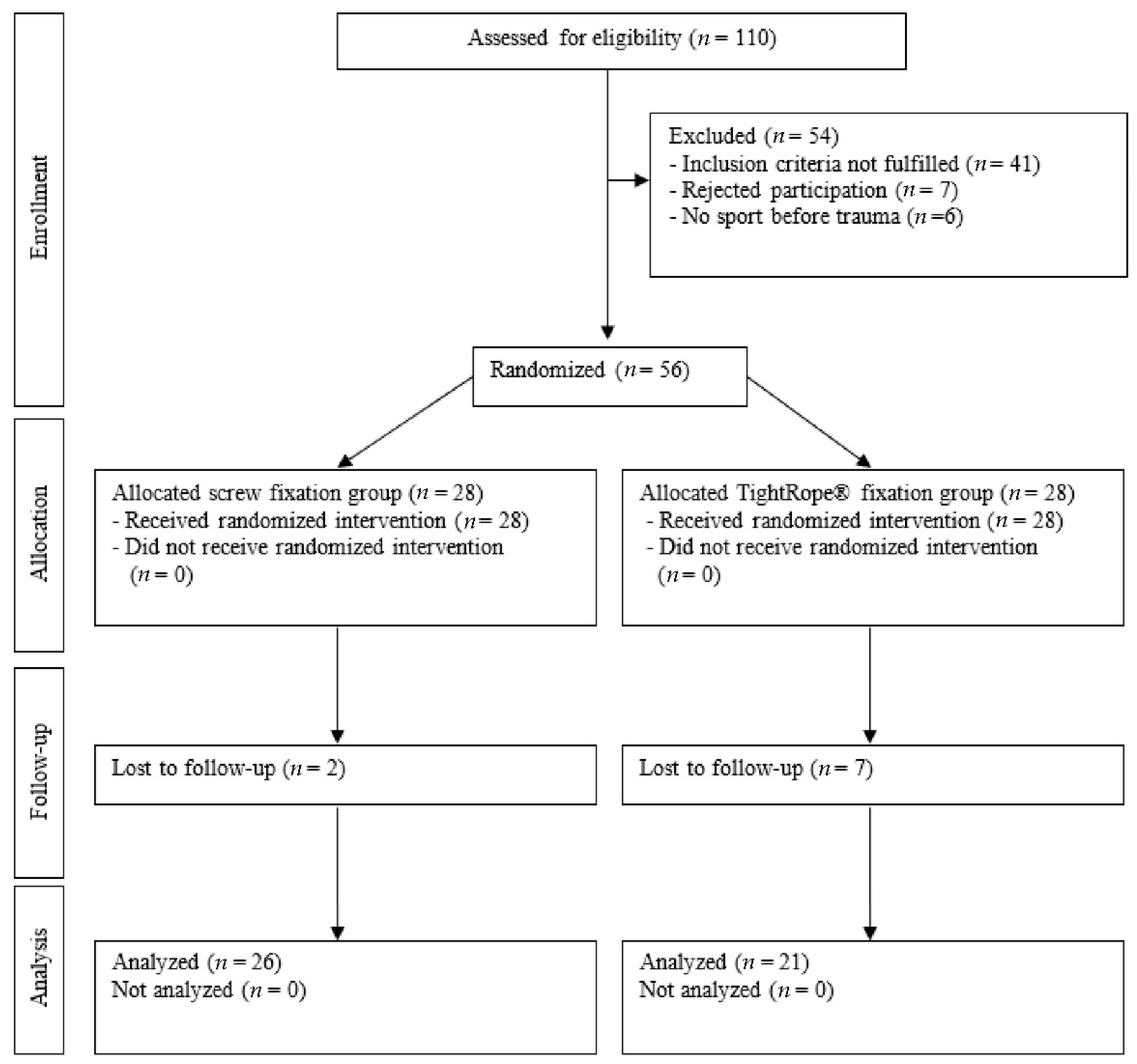
2.1. Patient Selection
2.2. Randomization Procedure
2.3. Surgical Technique
2.4. Postoperative Protocol
2.5. Outcomes Assessment
2.6. Statistical Analysis
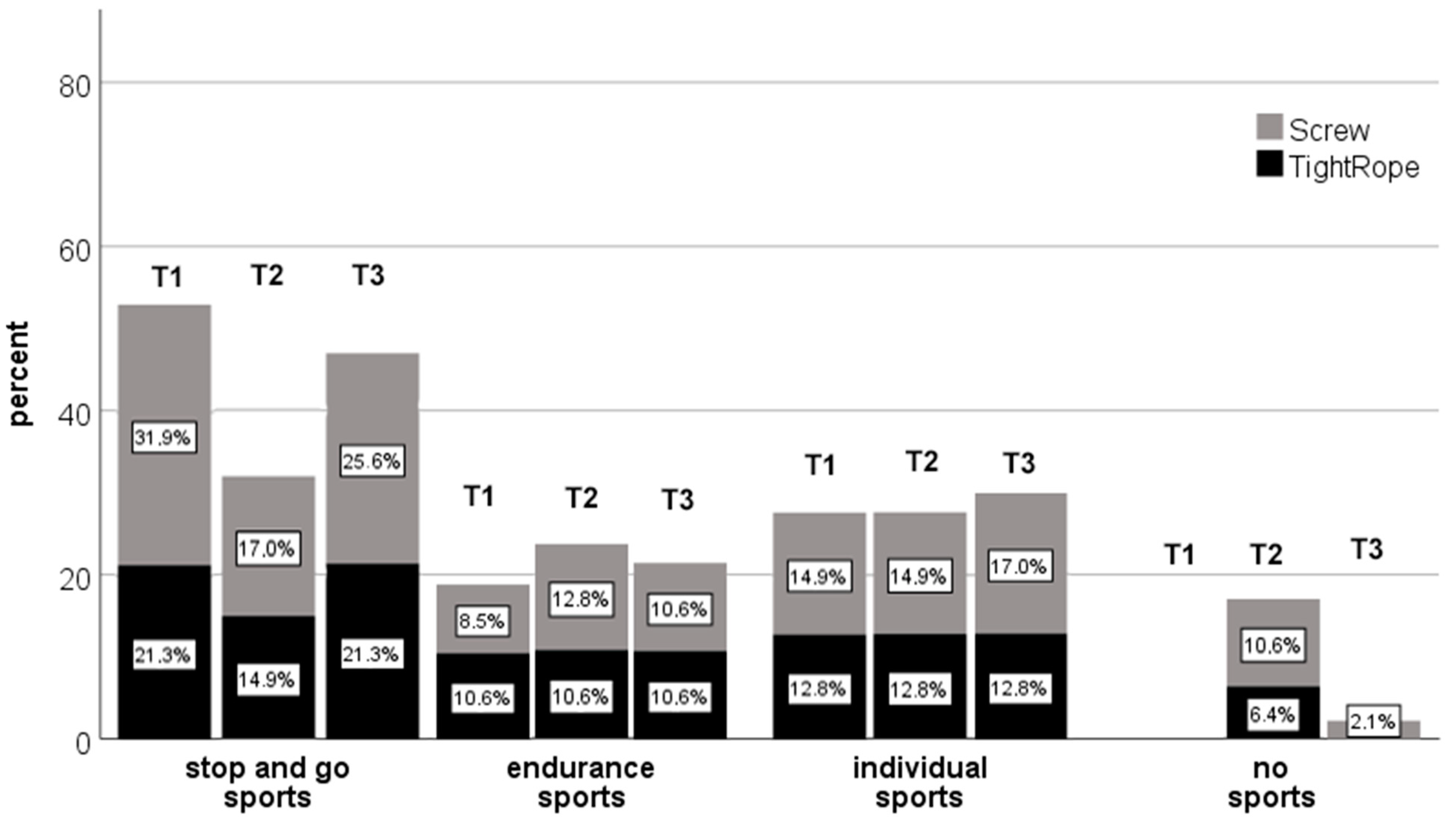
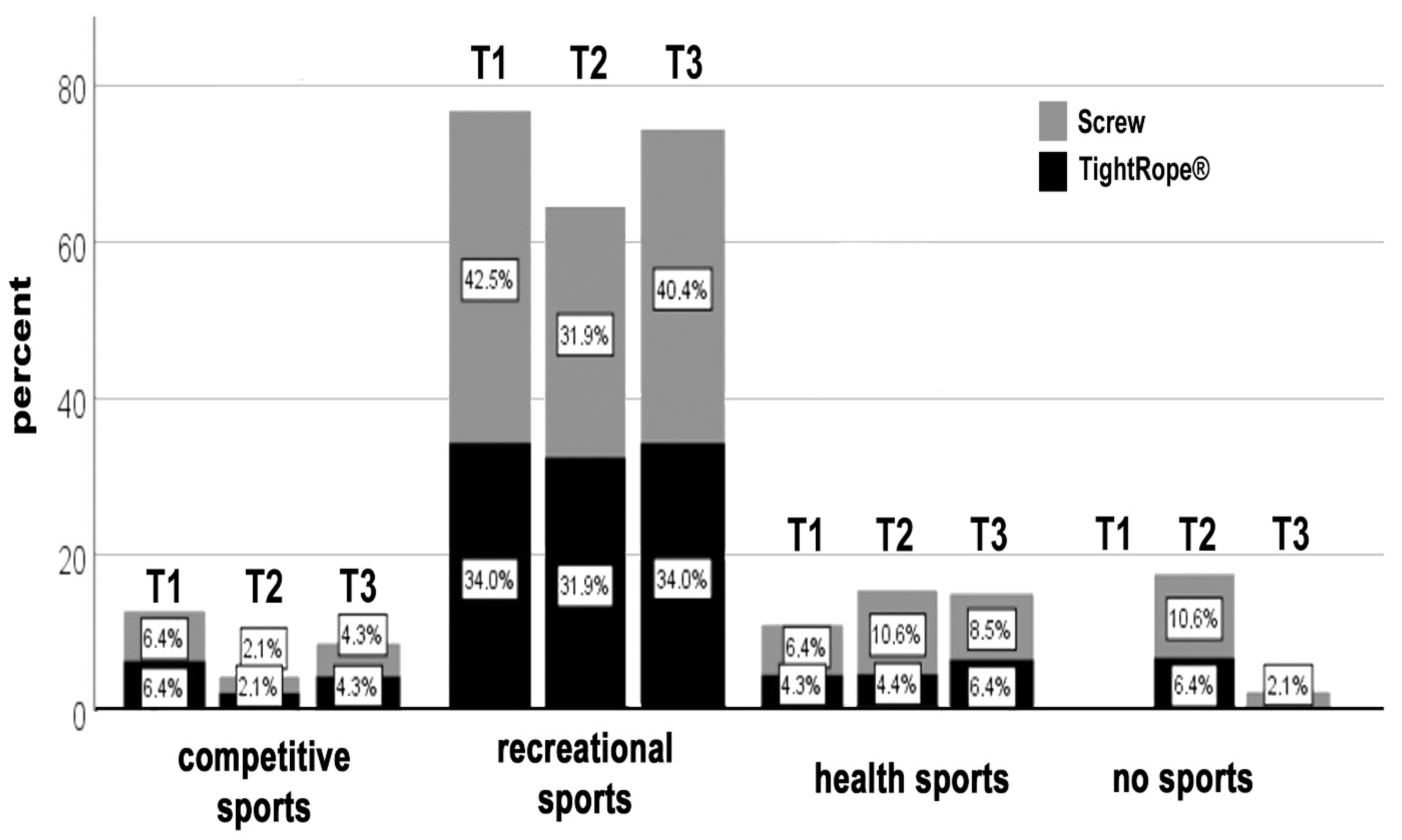
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boytim, M.J.; Fischer, D.A.; Neumann, L. Syndesmotic ankle sprains. Am. J. Sports Med. 1991, 19, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Gerber, J.P.; Williams, G.N.; Scoville, C.R.; Arciero, R.A.; Taylor, D.C. Persistent disability associated with ankle sprains: A prospective examination of an athletic population. Foot Ankle Int. 1998, 19, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Hunt, K.J.; George, E.; Harris, A.H.; Dragoo, J.L. Epidemiology of syndesmosis injuries in intercollegiate football: Incidence and risk factors from National Collegiate Athletic Association injury surveillance system data from 2004–2005 to 2008–2009. Clin. J. Sport Med. 2013, 23, 278–282. [Google Scholar] [CrossRef]
- Court-Brown, C.M.; McBirnie, J.; Wilson, G. Adult ankle fractures--an increasing problem? Acta Orthop. Scand. 1998, 69, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Beumer, A.; Valstar, E.R.; Garling, E.H.; Niesing, R.; Ginai, A.Z.; Ranstam, J.; Swierstra, B.A. Effects of ligament sectioning on the kinematics of the distal tibiofibular syndesmosis: A radiostereometric study of 10 cadaveric specimens based on presumed trauma mechanisms with suggestions for treatment. Acta Orthop. 2006, 77, 531–540. [Google Scholar] [CrossRef]
- Rammelt, S.; Schneiders, W.; Grass, R.; Rein, S.; Zwipp, H. Ligamentous injuries to the ankle joint. Z. Orthop. Unf. 2011, 149, e45–e67. [Google Scholar] [CrossRef]
- Wright, R.W.; Barile, R.J.; Surprenant, D.A.; Matava, M.J. Ankle syndesmosis sprains in national hockey league players. Am. J. Sports Med. 2004, 32, 1941–1945. [Google Scholar] [CrossRef]
- Guise, E.R. Rotational ligamentous injuries to the ankle in football. Am. J. Sports Med. 1976, 4, 1–6. [Google Scholar] [CrossRef]
- Taylor, D.C.; Tenuta, J.J.; Uhorchak, J.M.; Arciero, R.A. Aggressive surgical treatment and early return to sports in athletes with grade III syndesmosis sprains. Am. J. Sports Med. 2007, 35, 1833–1838. [Google Scholar] [CrossRef]
- Hinds, R.M.; Lazaro, L.E.; Burket, J.C.; Lorich, D.G. Risk factors for posttraumatic synostosis and outcomes following operative treatment of ankle fractures. Foot Ankle Int. 2014, 35, 141–147. [Google Scholar] [CrossRef]
- Colcuc, C.; Blank, M.; Stein, T.; Raimann, F.; Weber-Spickschen, S.; Fischer, S.; Hoffmann, R. Lower complication rate and faster return to sports in patients with acute syndesmotic rupture treated with a new knotless suture button device. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3156–3164. [Google Scholar] [CrossRef] [PubMed]
- Pakarinen, H.J.; Flinkkila, T.E.; Ohtonen, P.P.; Hyvonen, P.H.; Lakovaara, M.T.; Leppilahti, J.I.; Ristiniemi, J.Y. Syndesmotic fixation in supination-external rotation ankle fractures: A prospective randomized study. Foot Ankle Int. 2011, 32, 1103–1109. [Google Scholar] [CrossRef]
- Martin, R.L.; Irrgang, J.J.; Burdett, R.G.; Conti, S.F.; Van Swearingen, J.M. Evidence of validity for the Foot and Ankle Ability Measure (FAAM). Foot Ankle Int. 2005, 26, 968–983. [Google Scholar] [CrossRef]
- Calder, J.D.; Bamford, R.; Petrie, A.; McCollum, G.A. Stable Versus Unstable Grade II High Ankle Sprains: A Prospective Study Predicting the Need for Surgical Stabilization and Time to Return to Sports. Arthroscopy 2016, 32, 634–642. [Google Scholar] [CrossRef] [PubMed]
- D’Hooghe, P.; Grassi, A.; Alkhelaifi, K.; Calder, J.; Baltes, T.P.A.; Zaffagnini, S.; Ekstrand, J. Return to play after surgery for isolated unstable syndesmotic ankle injuries (West Point grade IIB and III) in 110 male professional football players: A retrospective cohort study. Br. J. Sports Med. 2020, 54, 1168–1173. [Google Scholar] [CrossRef] [Green Version]
- Thornes, B.; Shannon, F.; Guiney, A.M.; Hession, P.; Masterson, E. Suture-button syndesmosis fixation: Accelerated rehabilitation and improved outcomes. Clin. Orthop. Relat. Res. 2005, 431, 207–212. [Google Scholar] [CrossRef]
- Khurana, A.; Kumar, A.; Katekar, S.; Kapoor, D.; Vishwakarma, G.; Shah, A.; Singh, M.S. Is routine removal of syndesmotic screw justified? A meta-analysis. Foot 2021, 49, 101776. [Google Scholar] [CrossRef]
- Walley, K.C.; Hofmann, K.J.; Velasco, B.T.; Kwon, J.Y. Removal of Hardware After Syndesmotic Screw Fixation: A Systematic Literature Review. Foot Ankle Spec. 2017, 10, 252–257. [Google Scholar] [CrossRef]
- Laflamme, M.; Belzile, E.L.; Bedard, L.; van den Bekerom, M.P.; Glazebrook, M.; Pelet, S. A prospective randomized multicenter trial comparing clinical outcomes of patients treated surgically with a static or dynamic implant for acute ankle syndesmosis rupture. J. Orthop. Trauma 2015, 29, 216–223. [Google Scholar] [CrossRef]
- Andersen, M.R.; Frihagen, F.; Hellund, J.C.; Madsen, J.E.; Figved, W. Randomized Trial Comparing Suture Button with Single Syndesmotic Screw for Syndesmosis Injury. J. Bone Jt. Surg. Am. 2018, 100, 2–12. [Google Scholar] [CrossRef]
- Grassi, A.; Samuelsson, K.; D’Hooghe, P.; Romagnoli, M.; Mosca, M.; Zaffagnini, S.; Amendola, A. Dynamic Stabilization of Syndesmosis Injuries Reduces Complications and Reoperations as Compared with Screw Fixation: A Meta-analysis of Randomized Controlled Trials. Am. J. Sports Med. 2020, 48, 1000–1013. [Google Scholar] [CrossRef]
- Stiene, A.; Renner, C.E.; Chen, T.; Liu, J.; Ebraheim, N.A. Distal Tibiofibular Syndesmosis Dysfunction: A Systematic Literature Review of Dynamic Versus Static Fixation Over the Last 10 Years. J. Foot Ankle Surg. 2019, 58, 320–327. [Google Scholar] [CrossRef]
- Naqvi, G.A.; Cunningham, P.; Lynch, B.; Galvin, R.; Awan, N. Fixation of ankle syndesmotic injuries: Comparison of tightrope fixation and syndesmotic screw fixation for accuracy of syndesmotic reduction. Am. J. Sports Med. 2012, 40, 2828–2835. [Google Scholar] [CrossRef]
- Sagi, H.C.; Shah, A.R.; Sanders, R.W. The functional consequence of syndesmotic joint malreduction at a minimum 2-year follow-up. J. Orthop. Trauma 2012, 26, 439–443. [Google Scholar] [CrossRef]
- Ebraheim, N.A.; Lu, J.; Yang, H.; Mekhail, A.O.; Yeasting, R.A. Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: A cadaver study. Foot Ankle Int. 1997, 18, 693–698. [Google Scholar] [CrossRef]
- Lepojarvi, S.; Pakarinen, H.; Savola, O.; Haapea, M.; Sequeiros, R.B.; Niinimaki, J. Posterior translation of the fibula may indicate malreduction: CT study of normal variation in uninjured ankles. J. Orthop. Trauma 2014, 28, 205–209. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Screw (n = 26) | TightRope (n = 21) | |
|---|---|---|
| Sex | ||
| Female, n (%) | 5 (19) | 5 (24) |
| Male, n (%) | 21 (81) | 16 (76) |
| Age, y, median (range) | 39 (18–60) | 32 (18–60) |
| Affected side | ||
| Right, n (%) | 11 (42) | 12 (57) |
| Left, n (%) | 15 (58) | 9 (43) |
| Mechanism of injury | ||
| Private, n (%) | 8 (31) | 11 (52) |
| Traffic, n (%) | 1 (4) | 0 (0) |
| Work, n (%) | 9 (35) | 3 (14) |
| Sports, n (%) | 8 (31) | 7 (33) |
| Classification | ||
| Weber B, n (%) | 4 (15) | 4 (19) |
| Weber C, n (%) | 4 (15) | 2 (10) |
| Isolated, n (%) | 11 (42) | 11 (52) |
| Maisonneuve, n (%) | 7 (27) | 4 (19) |
| Patient Number | Screw | TightRope® |
|---|---|---|
| 1 | Left the country | |
| 2 | Unable to contact | |
| 3 | Unable to contact | |
| 4 | Left the country | |
| 5 | Left the country | |
| 6 | Withdrawal of participation | |
| 7 | Withdrawal of participation | |
| 8 | Unable to contact | |
| 9 | Unable to contact |
| Presurgery (T1) a | 6 Months (T2) a | 12 Months (T3) a | p Values b | 95% CI c | |
|---|---|---|---|---|---|
| FADI Sports | |||||
| Screw | 100 ± 0 | 83 ± 22 | 86 ± 20 | pT1 = n.s. | T1 = 97–100 |
| TightRope® | 97 ± 7 | 77 ± 23 | 87 ± 16 | pT2 = n.s. | T2 = 74–87 |
| pT3 = n.s. | T3 = 81–91 | ||||
| FAAM Sports | |||||
| Screw | 100 ± 1 | 80 ± 26 | 85 ± 18 | pT1 = n.s. | T1 = 98–100 |
| TightRope® | 98 ± 6 | 79 ± 21 | 89 ± 14 | pT2 = n.s. | T2 = 73–87 |
| pT3 = n.s. | T3 = 82–91 |
| Presurgery (T1) a | 6 Months (T2) a | 12 Months (T3) a | p-Values b | ||||
|---|---|---|---|---|---|---|---|
| Screw | TightRope® | Screw | TightRope® | Screw | TightRope® | ||
| Pain sports | 0 ± 0 | 0 ± 1 | 1 ± 2 | 3 ± 3 | 1 ± 2 | 2 ± 2 | pT1 = 0.194 |
| pT2 = 0.107 | |||||||
| pT3 = 0.519 | |||||||
| Function sports | 0 ± 1 | 0 ± 1 | 2 ± 2 | 3 ± 3 | 2 ± 2 | 2 ± 2 | pT1 = 0.878 |
| pT2 = 0.194 | |||||||
| pT3 = 0.608 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colcuc, C.; Wähnert, D.; Raimann, F.J.; Stein, T.; Weber-Spickschen, S.; Hoffmann, R.; Fischer, S. The Effect of Stabilization Procedures on Sports Discipline and Performance Level in Non-Elite Athletes after Acute Syndesmotic Injury: A Prospective Randomized Trial. J. Clin. Med. 2022, 11, 4609. https://doi.org/10.3390/jcm11154609
Colcuc C, Wähnert D, Raimann FJ, Stein T, Weber-Spickschen S, Hoffmann R, Fischer S. The Effect of Stabilization Procedures on Sports Discipline and Performance Level in Non-Elite Athletes after Acute Syndesmotic Injury: A Prospective Randomized Trial. Journal of Clinical Medicine. 2022; 11(15):4609. https://doi.org/10.3390/jcm11154609
Chicago/Turabian StyleColcuc, Christian, Dirk Wähnert, Florian J. Raimann, Thomas Stein, Sanjay Weber-Spickschen, Reinhard Hoffmann, and Sebastian Fischer. 2022. "The Effect of Stabilization Procedures on Sports Discipline and Performance Level in Non-Elite Athletes after Acute Syndesmotic Injury: A Prospective Randomized Trial" Journal of Clinical Medicine 11, no. 15: 4609. https://doi.org/10.3390/jcm11154609
APA StyleColcuc, C., Wähnert, D., Raimann, F. J., Stein, T., Weber-Spickschen, S., Hoffmann, R., & Fischer, S. (2022). The Effect of Stabilization Procedures on Sports Discipline and Performance Level in Non-Elite Athletes after Acute Syndesmotic Injury: A Prospective Randomized Trial. Journal of Clinical Medicine, 11(15), 4609. https://doi.org/10.3390/jcm11154609