
Incidence and Risk Factors Affecting the Recurrence of Primary Retinal Detachment in a Tertiary Hospital in Spain

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Steel, D. Retinal detachment. BMJ Clin. Evid. 2014, 2014, 0710. [Google Scholar]
- Znaor, L.; Medic, A.; Binder, S.; Vucinovic, A.; Lovric, J.M.; Puljak, L. Pars plana vitrectomy versus scleral buckling for repairing simple rhegmatogenous retinal detachments. Cochrane. Database. Syst. Rev. 2019, 3, 1–51. [Google Scholar] [CrossRef] [PubMed]
- Dunnington, J.H.; Macnie, J.P. Detachment of the retina. Arch. Ophthalmol. 1935, 13, 191–200. [Google Scholar] [CrossRef]
- Hughes, H.W., Jr. Evaluation of results of retinal detachment surgery. Trans. Am. Acad. Ophthalmol. Otolaryngol. 1952, 56, 439–448. [Google Scholar]
- Rachal, W.F.; Burton, T.C. Changing concepts of failures after retinal detachment surgery. Arch. Ophthalmol. 1979, 97, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Pastor, J.C.; Rojas, J.; Pastor-Idoate, S.; Di Lauro, S.; Gonzalez-Buendia, L.; Delgado-Tirado, S. Proliferative vitreoretinopathy: A new concept of disease pathogenesis and practical consequences. Prog. Retin. Eye Res. 2016, 51, 125–155. [Google Scholar] [CrossRef]
- Hilton, G.; Machemer, R.; Michels, R.; Okun, E.; Schepens, C.; Schwartz, A. The classification of retinal detachment with proliferative vitreoretinopathy. Ophthalmology 1983, 90, 121–125. [Google Scholar] [CrossRef]
- Idrees, S.; Sridhar, J.; Kuriyan, A.E. Proliferative vitreoretinopathy: A review. Int. Ophthalmol. Clin. 2019, 59, 221–240. [Google Scholar] [CrossRef]
- Aaberg, T.M., Sr. Surgery as the primary management of proliferative vitreoretinopathy: A history reflecting my experiences and biases. Arch. Ophthalmol. 2010, 128, 1068–1070. [Google Scholar] [CrossRef] [Green Version]
- Pastor, J.C.; de la Rúa, E.R.; Martín, F. Proliferative vitreoretinopathy: Risk factors and pathobiology. Prog. Retin. Eye Res. 2002, 21, 127–144. [Google Scholar] [CrossRef]
- Williamson, T.H.; Lee, E.J.; Shunmugam, M. Characteristics of rhegmatogenous retinal detachment and their relationship to success rates of surgery. Retina 2014, 34, 1421–1427. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, C.D.; Peto, T.; Grauslund, J.; Green, A. Epidemiologic characteristics of retinal detachment surgery at a specialized unit in Denmark. Acta Ophthalmol. 2016, 94, 548–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerstenberger, E.; Stoffelns, B.; Nickels, S.; Münzel, T.; Wild, P.S.; Beutel, M.E.; Schmidtmann, I.; Lackner, K.J.; Pfeiffer, N.; Schuster, A.K. Incidence of retinal detachment in germany: Results from the gutenberg health study. Ophthalmologica 2021, 244, 133–140. [Google Scholar] [CrossRef]
- Mitry, D.; Chalmers, J.; Anderson, K.; Williams, L.; Fleck, B.W.; Wright, A.; Campbell, H. Temporal trends in retinal detachment incidence in Scotland between 1987 and 2006. Br. J. Ophthalmol. 2011, 95, 365–369. [Google Scholar] [CrossRef] [Green Version]
- Smretschnig, E.; Falkner-Radler, C.I.; Spörl, J.; Kivaranovic, D.; Binder, S.; Krepler, K. Primary retinal detachment surgery: Changes in treatment and outcome in an austrian tertiary eye center. Ophthalmologica 2017, 237, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Ryan, E.H.; Ryan, C.M.; Forbes, N.J.; Yonekawa, Y.; Wagley, S.; Mittra, R.A.; Parke, D.W.; Joseph, D.P.; Emerson, G.G.; Shah, G.K.; et al. Primary retinal detachment outcomes study report number 2: Phakic retinal detachment outcomes. Ophthalmology 2020, 127, 1077–1785. [Google Scholar] [CrossRef] [PubMed]
- Ryan, E.H.; Joseph, D.P.; Ryan, C.M.; Forbes, N.J.K.; Yonekawa, Y.; Mittra, R.A.; Parke, D.W.; Ringeisen, A.; Emerson, G.G.; Shah, G.K.; et al. Primary retinal detachment outcomes study: Methodology and overall outcomes—primary retinal detachment outcomes study report number 1. Ophthalmol. Retin. 2020, 4, 814–822. [Google Scholar] [CrossRef]
- Scott, I.U.; Murray, T.G.; Flynn, H.W.; Feuer, W.J.; Schiffman, J.C. Outcomes and complications associated with giant retinal tear management using perfluoro-n-octane. Ophthalmology 2002, 109, 1828–1833. [Google Scholar] [CrossRef]
- Li, K.K.; Tang, E.W.; Li, P.S.; Wong, D. Double peel using triamcinolone acetonide and trypan blue in the management of myopic macular hole with retinal detachment: A case-control study. Clin. Exp. Ophthalmol. 2010, 38, 664–668. [Google Scholar] [CrossRef]
- Sen, P.; Sharma, U.; Panda, S.; Balekudaru, S.; Lingam, V.; Bhende, P. Outcomes of rhegmatogenous retinal detachment surgery in eyes with pre-existing glaucoma drainage devices. Indian J. Ophthalmol. 2018, 66, 1820–1824. [Google Scholar] [CrossRef]
- James, M.; O’Doherty, M.; Beatty, S. The prognostic influence of chronicity of rhegmatogenous retinal detachment on anatomic success after reattachment surgery. Am. J. Ophthalmol. 2007, 143, 1032–1034. [Google Scholar] [CrossRef] [PubMed]
- Orban, M.; Islam, Y.F.K.; Haddock, L.J. Timing and outcomes of vitreoretinal surgery after traumatic retinal detachment. J. Ophthalmol. 2016, 2016, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.Y.; Lee, M.W.; Won, Y.K.; Lim, H.B.; Kim, J.Y. Clinical characteristics and prognosis of total rhegmatogenous retinal detachment: A matched case-control study. BMC Ophthalmol. 2020, 20, 286. [Google Scholar] [CrossRef]
- Azen, S.P.; Scott, I.U.; Flynn, H.W.; Lai, M.Y., Jr.; Topping, T.M.; Benati, L.; Trask, D.K.; Rogus, L.A. Silicone oil in the repair of complex retinal detachments: A prospective observational multicenter study. Ophthalmology 1998, 105, 1587–1597. [Google Scholar] [CrossRef]
- Scott, I.U.; Flynn, H.W., Jr.; Murray, T.G.; Smiddy, W.E.; Davis, J.L.; Feuer, W.J. Outcomes of complex retinal detachment repair using 1000- vs. 5000-centistoke silicone oil. Arch. Ophthalmol. 2005, 123, 473–478. [Google Scholar] [CrossRef]
- Joseph, D.P.; Ryan, E.H.; Ryan, C.M.; Forbes, N.J.K.; Wagley, S.; Yonekawa, Y.; Mittra, R.A.; Parke, D.W.; Emerson, G.G.; Shah, G.K.; et al. Primary retinal detachment outcomes study: Pseudophakic retinal detachment outcomes: Primary retinal detachment outcomes study report number 3. Ophthalmology 2020, 127, 1507–1514. [Google Scholar] [CrossRef]
- Starr, M.R.; Obeid, A.; Ryan, E.H.; Ryan, C.; Ammar, M.; Patel, L.G.; Forbes, N.J.; Capone, A., Jr.; Emerson, G.G.; Joseph, D.P.; et al. Retinal detachment with inferior retinal breaks: Primary vitrectomy versus vitrectomy with scleral buckle (PRO Study Report No. 9). Retina 2021, 41, 525–530. [Google Scholar] [CrossRef]
- Churashov, S.V.; Shevalova, T.N.; Kulikov, A.N.; Maltsev, D.S. Surgical outcomes in inferior recurrences of rhegmatogenous retinal detachment. Int. J. Ophthalmol. 2021, 14, 1909–1914. [Google Scholar] [CrossRef]
- Qureshi, M.H.; Steel, D.H.W. Retinal detachment following cataract phacoemulsification—A review of the literature. Eye 2019, 34, 616–631. [Google Scholar] [CrossRef]
- Salicone, A.; Smiddy, W.E.; Venkatraman, A.; Feuer, W. Management of retinal detachment when no break is found. Ophthalmology 2006, 113, 398–403. [Google Scholar] [CrossRef]
- Callaway, N.F.; Vail, D.; Al-Moujahed, A.; Ludwig, C.; Ji, M.H.; Mahajan, V.B.; Pershing, S.; Moshfeghi, D.M. Sex differences in the repair of retinal detachments in the united states. Am. J. Ophthalmol. 2020, 219, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Shimada, Y.; Seno, Y.; Mizuguchi, T.; Tanikawa, A.; Horiguchi, M. Adherence to the face-down positioning after vitrectomy and gas tamponade: A time series analysis. BMC Res. Notes 2018, 11, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tieger, M.G.; Rodriguez, M.; Wang, J.C.; Obeid, A.; Ryan, C.; Gao, X.; Kakulavarapu, S.; Mardis, P.J.; Madhava, M.L.; Maloney, S.M.; et al. Impact of contact versus non-contact wide-angle viewing systems on outcomes of primary retinal detachment repair (PRO study report number 5). Br. J. Ophthalmol. 2021, 105, 410–413. [Google Scholar] [CrossRef]
- Mazinani, B.A.; Rajendram, A.; Walter, P.; Roessler, G.F. Does surgical experience have an effect on the success of retinal detachment surgery? Retina 2012, 32, 32–37. [Google Scholar] [CrossRef]
- Yorston, D.; Donachie, P.H.J.; Laidlaw, D.A.; Steel, D.H.; Sparrow, J.M.; Aylward, G.W.; Williamson, T.H.; Casswell, A.G.; Morris, A.H.C.; Jalil, A.; et al. Factors affecting visual recovery after successful repair of macula-off retinal detachments: Findings from a large prospective UK cohort study. Eye 2020, 35, 1431–1439. [Google Scholar] [CrossRef]
- Grabowska, A.; Neffendorf, J.E.; Yorston, D.; Williamson, T.H. Urgency of retinal detachment repair: Is it time to re-think our priorities? Eye 2021, 35, 1035–1036. [Google Scholar] [CrossRef] [PubMed]
- Ross, W.H.; Kozy, D.W. Visual recovery in macula-off rhegmatogenous retinal detachments. Ophthalmology 1998, 105, 2149–2153. [Google Scholar] [CrossRef]
- Heath Jeffery, R.C.; Young, B.; Atkins, W.; Shadbolt, B.; Allen, P.J.; Essex, R.W. Analysis of time to failure after retinal detachment surgery. Retina 2020, 40, 1909–1917. [Google Scholar] [CrossRef]


{kind=link}
| Year | Population Examined (n) | Primary RD Cases (n) | Annual Incidence Per 100,000 Inhabitants |
|---|---|---|---|
| 2017 | 649,075 | 148 | 22.8 |
| 2018 | 651,201 | 162 | 24.8 |
| 2019 | 654,027 | 147 | 22.5 |
| 2020 | 657,145 | 113 | 17.2 |
| Mean population studied = 652,862 Total primary RD cases = 570 Incidence = 21.8 cases per 100,000 per year | |||
| Characteristics | n (%) | |
|---|---|---|
| Sex | Female | 208 (36.5) |
| Male | 362 (63.5) | |
| Age (years) | <50 | 103 (18.1) |
| 50–69 | 306 (53.7) | |
| 70–79 | 106 (18.6) | |
| ≥80 | 55 (9.6) | |
| Laterality | Right | 310 (54.4) |
| Left | 260 (45.6) | |
| Lens status | Phakic | 298 (52.3) |
| Pseudophakic | 256 (44.9) | |
| Aphakic | 8 (1.4) | |
| IOL phakic | 8 (1.4) | |
| Pre-operative visual acuity (logMAR) | ≤0.30 | 178 (31.2) |
| <1.00–>0.30 | 105 (18.4) | |
| ≤1.30–≥1.00 | 80 (14.0) | |
| CF–NPL | 196 (34.4) | |
| Post-operative visual acuity (logMAR) | ≤0.30 | 333 (58.4) |
| ≤1.00–>0.30 | 116 (20.4) | |
| >1.00 | 108 (18.9) | |
| Myopia | No | 188 (33.0) |
| <3 Diopters | 80 (14.0) | |
| 3–6 Diopters | 49 (8.6) | |
| >6 Diopters | 100 (17.5) | |
| Ocular comorbidity | No | 299 (52.5) |
| Yes | 269 (47.2) | |
| Duration of central vision loss | 0 | 216 (37.9) |
| 1 | 4 (0.7) | |
| 2 | 15 (2.6) | |
| 3 | 34 (6.0) | |
| 4 | 41 (7.2) | |
| 5 | 35 (6.1) | |
| 6 | 36 (6.3) | |
| 7 | 24 (4.2) | |
| 8–14 | 59 (10.4) | |
| 15–30 | 44 (7.7) | |
| 31–90 | 26 (4.6) | |
| >90 | 9 (1.6) | |
| Macular status | On | 254 (44.6) |
| Off | 308 (54.0) | |
| Number of breaks | 0 | 60 (10.5) |
| 1 | 289 (50.7) | |
| 2 | 120 (21.1) | |
| 3 | 48 (8.4) | |
| 4 | 23 (4.0) | |
| 5 | 6 (1.1) | |
| 6 | 4 (0.7) | |
| 7 | 1 (0.2) | |
| 8 | 0 (0.0) | |
| 9 | 1 (0.2) | |
| Quadrants involved | ST | 329 (57.7) |
| IT | 289 (50.7) | |
| SN | 238 (41.8) | |
| IN | 224 (39.3) | |
| Inferior breaks | No | 363 (63.7) |
| Yes | 195 (34.2) | |
| No data | 12 (2.1) | |
| Proliferative vitreoretinopathy | No | 488 (85.6) |
| Yes | 82 (14.4) | |
| Complex retinal detachment | No | 262 (46.0) |
| Yes | 308 (54.0) | |
| Surgical technique | 23G PPV | 128 (22.5) |
| 25G PPV | 428 (75.1) | |
| Scleral buckle surgery | 10 (1.8) | |
| Laser | No | 134 (23.5) |
| Yes | 435 (76.3) | |
| Cryotherapy | No | 349 (61.2) |
| Yes | 220 (38.6) | |
| Scleral buckle | No | 530 (93.0) |
| Yes | 39 (6.8) | |
| Type of tamponade | SF6 | 373 (65.4) |
| C3F8 | 83 (14.6) | |
| Silicone oil | 72 (12.6) | |
| Air | 22 (3.9) | |
| Sub-retinal fluid drainage | Break | 516 (90.5) |
| Retinotomy | 53 (9.3) | |
| Redetachment | No | 405 (71.1) |
| Yes | 165 (28.9) | |
| Characteristics | Mean | Standard Deviation | Median | Minimum | Maximum |
|---|---|---|---|---|---|
| Age (years) | 61.14 | 14.29 | 62 | 0 | 95 |
| Follow up (days) | 465 | 410.55 | 360 | 23 | 1800 |
| Years from cataract surgery to RD | 3.44 | 4.43 | 2 | 0 | 25 |
| Days from primary RD surgery to re-detachment | 114.42 | 215.78 | 35 | 1 | 1225 |
| Cause of Complex RD | No Redetachment n(%) | Redetachment n(%) | Total |
|---|---|---|---|
| High myopia (≥−6D) | 66 (66.0) | 34 (34.0) | 100 |
| Proliferative vitreoretinopathy | 55 (67.1) | 27 (32.9) | 82 |
| Vitreous haemorrhage | 59 (72.0) | 23 (28.0) | 82 |
| Traumatic RD | 30 (69.8) | 13 (30.2) | 43 |
| Total RD | 25 (59.5) | 17 (40.5) | 42 |
| Complex cataract | 14 (53.8) | 12 (46.2) | 26 |
| Choroidal detachment | 11 (47.8) | 12 (52.2) | 23 |
| Giant break (≥90), | 11 (52.4) | 10 (47.6) | 21 |
| Macular hole | 11 (61.1) | 7 (38.9) | 18 |
| Proliferative diabetic retinopathy | 9 (60.0) | 6 (40.0) | 15 |
| Previous glaucoma surgery | 6 (46.2) | 7 (53.8) | 13 |
| Retinal dialysis | 10 (83.3) | 2 (16.7) | 12 |
| Chronic RD (≥3 months) | 7 (77.8) | 2 (22.2) | 9 |
| Uveitis | 4 (50.0) | 4 (50.0) | 8 |
| Endophtalmitis | 1 (33.3) | 2 (66.7) | 3 |
| Variable | No Redetachment n(%) | Redetachment n(%) | Total | p Value | |
|---|---|---|---|---|---|
| Sex | Female | 163 (78.4) | 45 (21.6) | 208 | 0.04 |
| Male | 242 (66.9) | 120 (33.1) | 362 | ||
| Age (years) | <50 | 71 (68.9) | 32 (31.1) | 103 | 0.170 |
| 50–69 | 227 (74.2) | 79 (25.8) | 306 | ||
| 70–79 | 74 (69.8) | 32 (30.2) | 106 | ||
| ≥80 | 33 (60.0) | 22 (40.0) | 55 | ||
| Laterality | Right | 211 (68.1) | 99 (31.9) | 310 | 0.086 |
| Left | 194 (74.6) | 260 (25.4) | 260 | ||
| Lens status | Phakic | 214 (71.8) | 84 (28.2) | 298 | 0.920 |
| Pseudophakic | 180 (70.3) | 76 (29.7) | 256 | ||
| Aphakic | 5 (62.5) | 3 (37.5) | 8 | ||
| Phakic intraocular lens | 6 (75.0) | 2 (25.0) | 8 | ||
| Pre-operative VA (logMAR) | ≤0.30 | 136 (76.4) | 42 (23.6) | 178 | 0.232 |
| <1.00–>0.30 | 73 (69.5) | 32 (30.5) | 105 | ||
| ≤1.30–≥1.00 | 57 (71.3) | 23 (28.7) | 80 | ||
| CF–NPL | 131 (66.8) | 65 (33.2) | 196 | ||
| Post-operative VA (logMAR) | ≤0.30 | 279 (83.8) | 54 (16.2) | 333 | <0.001 |
| ≤1.00–>0.30 | 79 (68.1) | 37 (31.9) | 116 | ||
| >1.00 | 37 (34.3) | 71 (65.7) | 108 | ||
| Myopia | No | 137 (45.5) | 51 (44.0) | 188 | 0.157 |
| ≤3 Diopters | 57 (71.3) | 23 (28.7) | 80 | ||
| 3–6 Diopters | 41 (83.7) | 8 (16.3) | 49 | ||
| ≥6 Diopters | 66 (66.0) | 34 (34.0) | 100 | ||
| Ocular comorbidity | No | 233 (77.9) | 66 (22.1) | 299 | <0.001 |
| Yes | 170 (63.2) | 99 (36.8) | 269 | ||
| Duration of central vision loss (days) | 0 | 157 (72.7) | 59 (27.3) | 216 | 0.300 |
| 1 | 2 (50.0) | 2 (50.0) | 4 | ||
| 2 | 13 (86.7) | 2 (13.3) | 15 | ||
| 3 | 28 (82.4) | 6 (17.6) | 34 | ||
| 4 | 25 (61.0) | 16 (39.0) | 41 | ||
| 5 | 20 (57.1) | 15 (42.9) | 35 | ||
| 6 | 27 (75.0) | 9 (25.0) | 36 | ||
| 7 | 19 (79.2) | 5 (20.8) | 24 | ||
| 8–14 | 41 (69.5) | 18 (30.5) | 59 | ||
| 15–30 | 32 (72.7) | 12 (27.3) | 44 | ||
| 31–90 | 16 (61.5) | 10 (38.5) | 26 | ||
| >90 | 7 (77.8) | 2 (22.2) | 9 | ||
| Macular status | On | 189 (74.4) | 65 (25.6) | 254 | 0.124 |
| Off | 211 (68.5) | 97 (31.5) | 308 | ||
| Number of breaks | 0 | 38 (63.3) | 22 (36.7) | 60 | 0.485 |
| 1 | 211 (73.0) | 78 (27.0) | 289 | ||
| 2 | 87 (72.5) | 33 (27.5) | 120 | ||
| 3 | 33 (68.8) | 15 (31.2) | 48 | ||
| 4 | 16 (69.6) | 7 (30.4) | 23 | ||
| 5 | 5 (83.3) | 1 (16.7) | 6 | ||
| 6 | 4 (100) | 0 (0) | 4 | ||
| 7 | 1 (100) | 0 (0) | 1 | ||
| 8 | 0 | 0 | 0 | ||
| 9 | 0 (0) | 1 (100) | 1 | ||
| Quadrands involved | ST no | 164 (68.6) | 75 (31.4) | 239 | 0.261 |
| ST yes | 240 (72.9) | 89 (27.1) | 329 | ||
| IT no | 210 (75.3) | 69 (24.7) | 279 | 0.032 | |
| IT yes | 194 (67.1) | 95 (32.9) | 289 | ||
| SN no | 235 (71.2) | 95 (28.8) | 330 | 0.958 | |
| SN yes | 169 (71.0) | 69 (29.0) | 238 | ||
| IN no | 261 (75.9) | 83 (24.1) | 344 | 0.002 | |
| IN yes | 143 (63.8) | 81 (36.2) | 224 | ||
| Inferior breaks | No | 263 (72.5) | 100 (27.5) | 363 | 0.499 |
| Yes | 136 (69.7) | 59 (30.3) | 195 | ||
| Proliferative vitreoretinopathy | No | 350 (71.7) | 138 (28.3) | 488 | 0.390 |
| Yes | 55 (67.1) | 27 (32.9) | 82 | ||
| Complex RD | No | 204 (77.9) | 58 (22.1) | 262 | <0.001 |
| Yes | 201 (65.3) | 107 (34.7) | 308 | ||
| Surgical technique | 23G PPV | 91 (71.1) | 37 (28.9) | 128 | 0.825 |
| 25G PPV | 304 (71.0) | 124 (29.0) | 428 | ||
| Classic surgery | 8 (80.0) | 2 (20.0) | 10 | ||
| Laser | No | 99 (73.9) | 35 (26.1) | 134 | 0.401 |
| Yes | 305 (70.1) | 130 (29.9) | 435 | ||
| Cryotherapy | No | 239 (68.5) | 110 (31.5) | 349 | 0.095 |
| Yes | 165 (75.0) | 55 (25.0) | 220 | ||
| Scleral buckle | No | 375 (70.8) | 155 (29.2) | 530 | 0.632 |
| Yes | 29 (74.4) | 10 (25.6) | 39 | ||
| Tamponade method | SF6 | 278 (74.5) | 95 (25.5) | 373 | 0.01 |
| C3F8 | 55 (66.3) | 28 (33.7) | 83 | ||
| Silicone oil | 40 (55.6) | 32 (44.4) | 72 | ||
| Air | 16 (72.7) | 6 (27.3) | 22 | ||
| Sub-retinal fluid drainage | Break | 370 (71.7) | 146 (28.3) | 516 | 0.248 |
| Retinotomy | 34 (64.2) | 19 (35.8) | 53 | ||
| Surgeon | 1 | 20 (80) | 5 (20) | 25 | 0.035 |
| 2 | 51 (63) | 30 (37) | 81 | ||
| 3 | 68 (84) | 13 (16) | 81 | ||
| 4 | 55 (66.3) | 28 (33.7) | 83 | ||
| 5 | 81 (75.7) | 26 (24.3) | 107 | ||
| 6 | 90 (70.9) | 37 (29.1) | 127 | ||
| 7 | 38 (60.3) | 25 (39.7) | 63 | ||
| Variable | Odds Ratio | p Value | 95% Confidence Interval | |
|---|---|---|---|---|
| Sex | Female | Reference | - | - |
| Male | 2 | 0.002 | 1.4–5.7 | |
| Ocular comorbidity | No | Reference | - | - |
| Yes | 1.9 | 0.015 | 1.2–2.9 | |
| Variable | VA > 1.0 logMAR n(%) | VA 1.0–0.3 logMAR n(%) | VA ≤ 0.30 logMAR n(%) | Total | p Value | |
|---|---|---|---|---|---|---|
| Age (years) | <50 | 5 (7.7) | 18 (26.5) | 45 (66.2) | 68 | <0.001 |
| 50–69 | 13 (5.8) | 32 (14.3) | 178 (79.8) | 223 | ||
| 70–79 | 9 (12.5) | 17 (23.6) | 46 (63.9) | 72 | ||
| ≥80 | 10 (31.3) | 12 (37.5) | 10 (31.3) | 32 | ||
| Laterality | Right | 18 (8.6) | 42 (20.1) | 149 (71.3) | 209 | 0.861 |
| Left | 19 (10.2) | 37 (19.9) | 130 (69.9) | 186 | ||
| Lens | Phakic | 16 (7.6) | 37 (17.6) | 157 (74.8) | 210 | 0.351 |
| Pseudophakic | 20 | 38 | 116 | 174 | ||
| Aphakic | 1 (20.0) | 2 (40.0) | 2 (40.0) | 5 | ||
| IOL phakic | 0 (0.0) | 2 (33.3) | 4 (66.7) | 6 | ||
| Myopia | No | 7 (5.3) | 24 (18.0) | 102 (76.7) | 133 | <0.001 |
| ≤3 Diopters | 3 (5.4) | 11 (19.6) | 42 (75.0) | 56 | ||
| 3–6 Diopters | 0 (0.0) | 1 (2.4) | 40 (97.6) | 41 | ||
| ≥6 Diopters | 13 (20.0) | 15 (23.1) | 37 (56.9) | 65 | ||
| Ocular comorbidities | No | 7 (3.0) | 39 (17.0) | 184 (80.0) | 230 | <0.001 |
| Yes | 30 (18.4) | 40 (24.5) | 93 (57.1) | 163 | ||
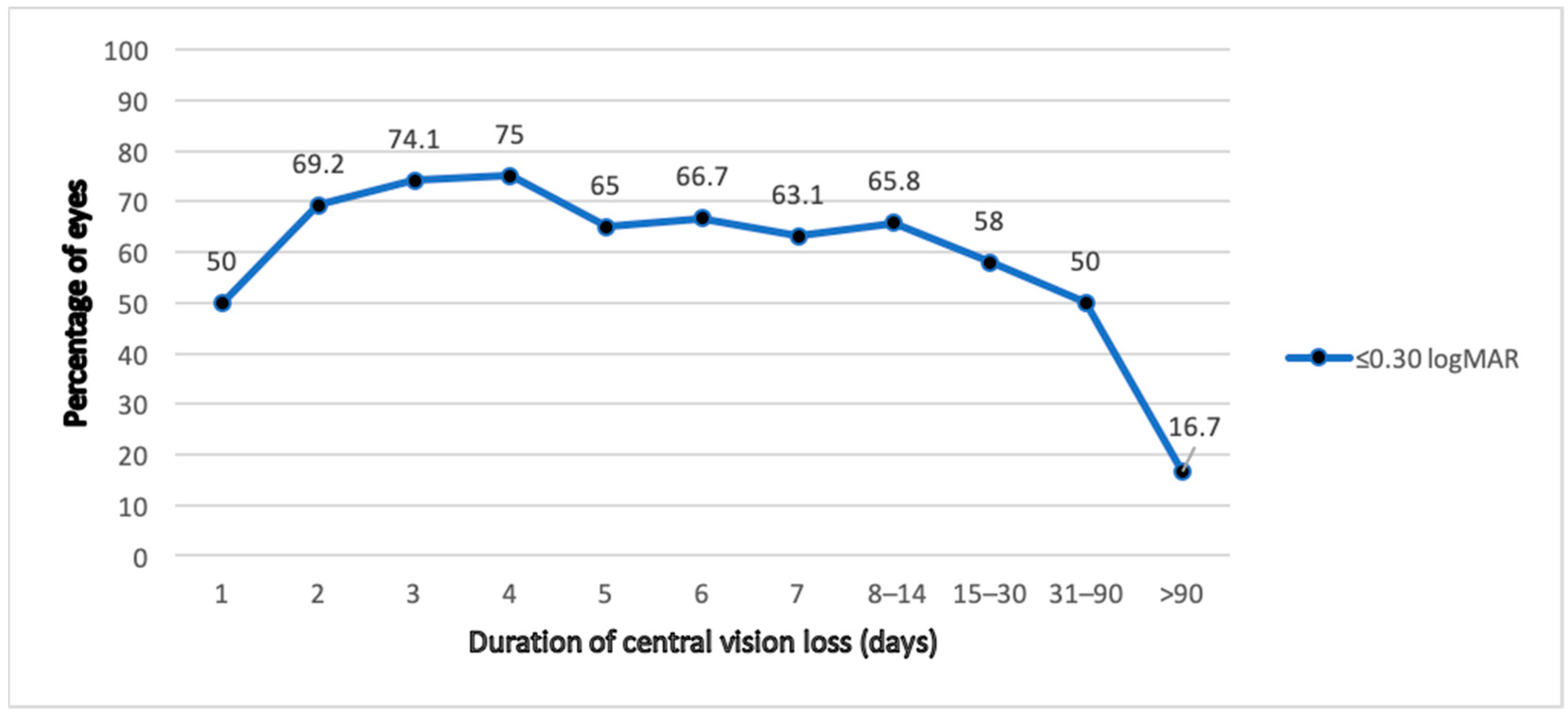
| Days of central vision loss | 0 | 14 (9.1) | 17 (11) | 123 (79.9) | 154 | 0.004 |
| 1 | 1 (50.0) | 0 (0.0) | 1 (50.0) | 2 | ||
| 2 | 0 (0.0) | 4 (30.8) | 9 (69.2) | 13 | ||
| 3 | 2 (7.41) | 5 (18.5) | 20 (74.1) | 27 | ||
| 4 | 0 (0.0) | 6 (25.0) | 18 (75.0) | 24 | ||
| 5 | 2 (10.0) | 5 (25.0) | 13 (65.0) | 20 | ||
| 6 | 4 (14.8) | 5 (18.5) | 18 (66.7) | 27 | ||
| 7 | 1 (5.3) | 6 (31.6) | 12 (63.1) | 19 | ||
| 8–14 | 2 (4.9) | 12 (29.3) | 27 (65.8) | 41 | ||
| 15–30 | 3 (9.7) | 10 (32.3) | 18 (58.0) | 31 | ||
| 31–90 | 2 (12.5) | 6 (37.5) | 8 (50.0) | 16 | ||
| >90 | 3 (50.0) | 2 (33.3) | 1 (16.7) | 6 | ||
| Macular status | On | 13 (7.0) | 20 (10.7) | 153 (82.3) | 186 | <0.001 |
| Off | 24 (11.7) | 56 (27.3) | 125 (61.0) | 205 | ||
| Number of breaks | 0 | 16 (44.4) | 5 (13.9) | 15 (41.7) | 36 | <0.001 |
| 1–4 | 18 (5.3) | 68 (19.9) | 255 (74.8) | 341 | ||
| 5–9 | 0 (0.0) | 3 (30.0) | 7 (70.0) | 10 | ||
| Involvement | ST no | 18 (11.3) | 28 (17.6) | 113 (71.1) | 159 | 0.427 |
| ST yes | 19 (8.1) | 50 (21.3) | 116 (70.6) | 235 | ||
| IT no | 10 (4.8) | 43 (20.6) | 156 (75.6) | 209 | 0.004 | |
| IT yes | 27 (14.6) | 35 (18.9) | 123 (66.5) | 185 | ||
| SN no | 19 (8.3) | 42 (18.3) | 169 (73.5) | 230 | 0.374 | |
| SN yes | 18 (11.0) | 36 (21.9) | 110 (67.1) | 164 | ||
| IN no | 11 (4.3) | 52 (20.2) | 195 (75.6) | 258 | <0.001 | |
| IN yes | 26 (19.1) | 26 (19.1) | 84 (61.8) | 136 | ||
| Inferior breaks | No | 32 (12.4) | 53 (20.5) | 173 (67.1) | 258 | 0.003 |
| Yes | 3 (2.3) | 25 (18.9) | 104 (78.8) | 132 | ||
| PVR | No | 24 (7.0) | 59 (17.2) | 260 (75.8) | 343 | <0.001 |
| Yes | 13 (25.0) | 20 (38.5) | 19 (36.5) | 52 | ||
| Complex RD | No | 10 (5.0) | 34 (16.8) | 158 (78.2) | 202 | 0.001 |
| Yes | 27 (14.0) | 45 (23.3) | 121 (62.7) | 193 | ||
| Surgical technique | 23G PPV | 11 (12.4) | 19 (21.3) | 59 (66.3) | 89 | 0.543 |
| 25G PPV | 26 (8.8) | 57 (19.2) | 213 (72.0) | 296 | ||
| Classic surgery | 0 (0.0) | 3 (33.3) | 6 (66.7) | 9 | ||
| Laser | No | 4 (4.2) | 20 (20.8) | 72 (75.0) | 96 | 0.130 |
| Yes | 33 (11.1) | 59 (19.8) | 206 (69.1) | 298 | ||
| Cryotherapy | No | 30 (12.9) | 41 (17.7) | 161 (69.4) | 232 | 0.01 |
| Yes | 7 (4.3) | 38 (23.5) | 117 (72.2) | 162 | ||
| Scleral buckle | No | 33 (8.9) | 73 (19.7) | 265 (71.4) | 371 | 0.248 |
| Yes | 4 (17.4) | 6 (26.1) | 13 (56.5) | 23 | ||
| Tamponade method | SF6 | 12 (4.4) | 53 (19.4) | 208 (76.2) | 273 | <0.001 |
| C3F8 | 1 (1.8) | 12 (22.2) | 41 (76) | 54 | ||
| Silicone oil | 24 (64.9) | 9 (24.3) | 4 (10.8) | 37 | ||
| Air | 0 (0.0) | 1 (6.2) | 15 (93.8) | 16 | ||
| Sub-retinal fluid drainage | Break | 28 (7.8) | 70 (19.4) | 262 (72.8) | 360 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Irigoyen, C.; Goikoetxea-Zubeldia, A.; Sanchez-Molina, J.; Amenabar Alonso, A.; Ruiz-Miguel, M.; Iglesias-Gaspar, M.T. Incidence and Risk Factors Affecting the Recurrence of Primary Retinal Detachment in a Tertiary Hospital in Spain. J. Clin. Med. 2022, 11, 4551. https://doi.org/10.3390/jcm11154551
Irigoyen C, Goikoetxea-Zubeldia A, Sanchez-Molina J, Amenabar Alonso A, Ruiz-Miguel M, Iglesias-Gaspar MT. Incidence and Risk Factors Affecting the Recurrence of Primary Retinal Detachment in a Tertiary Hospital in Spain. Journal of Clinical Medicine. 2022; 11(15):4551. https://doi.org/10.3390/jcm11154551
Chicago/Turabian StyleIrigoyen, Cristina, Ainhoa Goikoetxea-Zubeldia, Jorge Sanchez-Molina, Asier Amenabar Alonso, Miguel Ruiz-Miguel, and Maria Teresa Iglesias-Gaspar. 2022. "Incidence and Risk Factors Affecting the Recurrence of Primary Retinal Detachment in a Tertiary Hospital in Spain" Journal of Clinical Medicine 11, no. 15: 4551. https://doi.org/10.3390/jcm11154551
APA StyleIrigoyen, C., Goikoetxea-Zubeldia, A., Sanchez-Molina, J., Amenabar Alonso, A., Ruiz-Miguel, M., & Iglesias-Gaspar, M. T. (2022). Incidence and Risk Factors Affecting the Recurrence of Primary Retinal Detachment in a Tertiary Hospital in Spain. Journal of Clinical Medicine, 11(15), 4551. https://doi.org/10.3390/jcm11154551