
How Does the COVID-19 Pandemic Affect Pediatric Patients with Intussusception Treated by Ultrasound-Guided Hydrostatic Enema Reduction?


Abstract
:1. Introduction
2. Materials and Methods
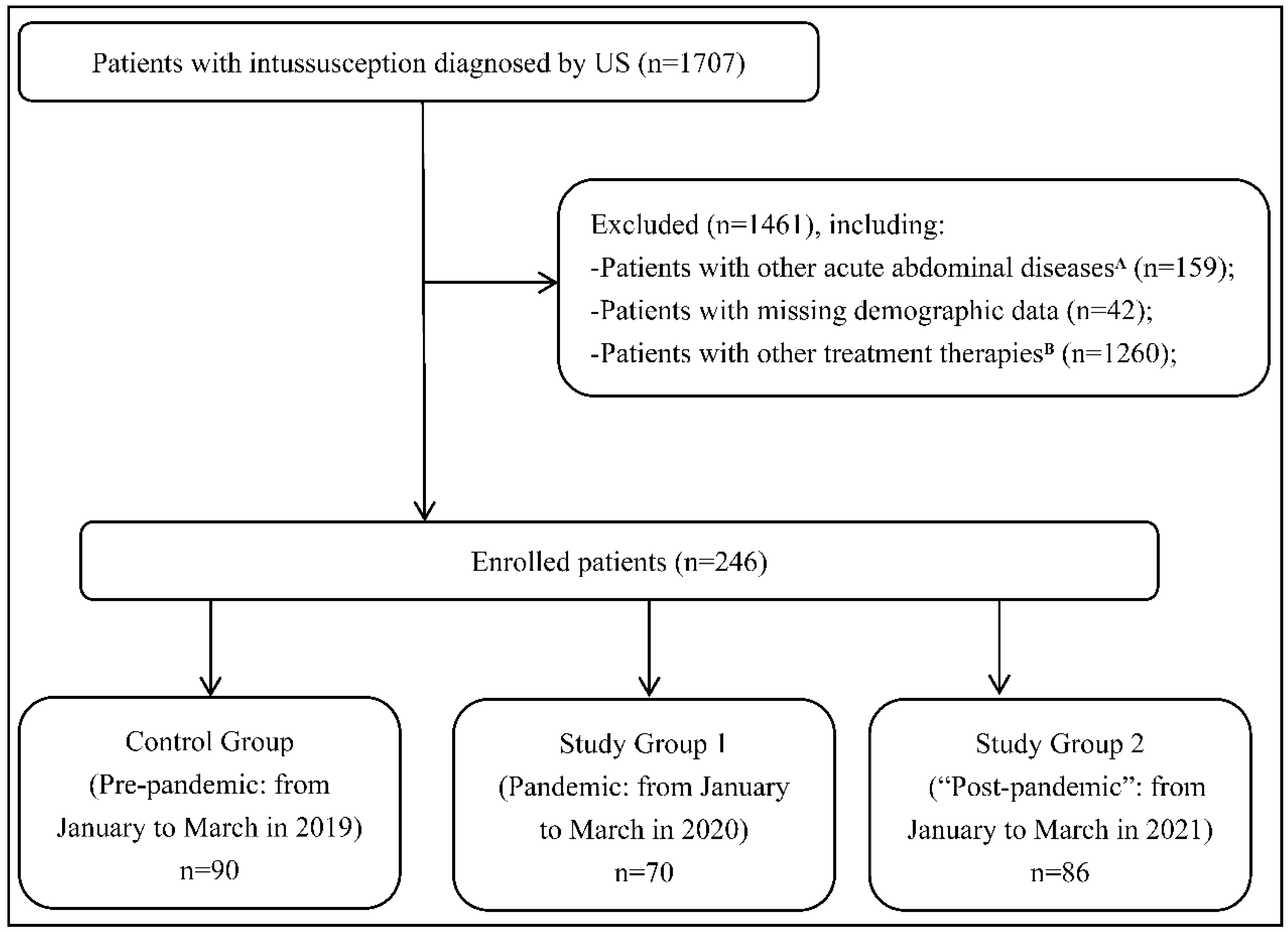
2.1. Patient Enrollment and Study Design
2.2. Data Collection and Outcome Measurement
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. J. Am. Med. Assoc. 2020, 323, 1239. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Timeline: WHO’s COVID-19 Response. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline (accessed on 27 June 2022).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 27 June 2022).
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc. Health 2020, 4, e10–e11. [Google Scholar] [CrossRef]
- Wilder, J.L.; Parsons, C.R.; Growdon, A.S.; Toomey, S.L.; Mansbach, J.M. Pediatric hospitalizations during the COVID-19 pandemic. Pediatrics 2020, 146, e2020005983. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, H.; Song, K.H.; Kim, E.S.; Park, J.S.; Jung, J.; Ahn, S.; Jeong, E.K.; Park, H.; Kim, H.B. Impact of public health interventions on seasonal influenza activity during the COVID-19 outbreak in Korea. Clin. Infect. Dis. 2021, 73, e132–e140. [Google Scholar] [CrossRef] [PubMed]
- Saalabian, K.; Rolle, U.; Friedmacher, F. Impact of the Global COVID-19 Pandemic on the Incidence, Presentation, and Management of Pediatric Appendicitis: Lessons Learned from the First Wave. Eur. J. Pediatr. Surg. 2021, 31, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Applegate, K.E. Intussusception in children: Evidence-based diagnosis and treatment. Pediatr. Radiol. 2009, 39, 140–143. [Google Scholar] [CrossRef] [PubMed]
- Eng, P.M.; Mast, T.C.; Loughlin, J.; Clifford, C.R.; Wong, J.; Seeger, J.D. Incidence of intussusception among infants in a large commercially insured population in the United States. Pediatr. Infect. Dis. J. 2012, 31, 287–291. [Google Scholar] [PubMed]
- Gluckman, S.; Karpelowsky, J.; Webster, A.C.; McGee, R.G. Management for intussusception in children. Cochrane Database Syst. Rev. 2017, 6, CD006476. [Google Scholar] [CrossRef]
- Xie, X.; Wu, Y.; Wang, Q.; Zhao, Y.; Chen, G.; Xiang, B. A randomized trial of pneumatic reduction versus hydrostatic reduction for intussusception in pediatric patients. J. Pediatr. Surg. 2018, 53, 1464–1468. [Google Scholar] [CrossRef]
- Otero, H.J.; White, A.M.; Khwaja, A.B.; Griffis, H.; Katcoff, H.; Bresnahan, B.W. Imaging intussusception in children’s hospitals in the United States: Trends, outcomes, and costs. J. Am. Coll. Radiol. 2019, 16, 1636–1644. [Google Scholar] [CrossRef]
- Cho, M.J.; Nam, C.W.; Choi, S.H.; Hwang, E.H. Management of recurrent ileocolic intussusception. J. Pediatr. Surg. 2020, 55, 2150–2153. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Ye, Y.; Liao, Y.; Wang, B. Fewer pediatric intussusception cases during the COVID-19 pandemic. J. Paediatr. Child Health 2020, 56, 1165. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.; Suda, K.; Kato, H.; Abe, E.; Kosaka, S.; Fujiwara, K.; Ochi, T.; Koga, H.; Urao, M.; Okazaki, T.; et al. Decreased incidence of intussusception during the COVID-19 pandemic. Trends in pediatric surgical emergencies. Pediatr. Surg. Int. 2021, 37, 1761–1764. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Byun, Y.-H.; Choi, S.J.; Lee, J.S.; Ryu, J.-M.; Lee, J.-Y. Decreased Incidence of Pediatric Intussusception during COVID-19. Children 2021, 8, 1072. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Ro, Y.S.; Kwon, H.; Suh, D.; Moon, S. Impact of the COVID-19 Pandemic on Emergency Care Utilization and Outcomes in Pediatric Patients with Intussusception. Children 2022, 9, 277. [Google Scholar] [CrossRef]
- Handa, A.; Callahan, M.J.; Kawai, K.; Tsai, A. The impact of social distancing during the COVID-19 pandemic on rates of pediatric idiopathic intussusception. Pediatric Radiol. 2022, 52, 453–459. [Google Scholar] [CrossRef]
- Bines, J.E.; Ivanoff, B.; Justice, F.; Mulholland, K. Clinical case definition for the diagnosis of acute intussusception. J. Pediatr. Gastroenterol. Nutr. 2004, 39, 511–518. [Google Scholar] [CrossRef]
- Crawley, F.P. The Limits of the Declaration of Helsinki. In Address to Scientific Session; World Medical Association General Assembly: Helsinki, Finland, 2012. [Google Scholar]
- Moazzam, Z.; Salim, A.; Ashraf, A.; Jehan, F.; Arshad, M. Intussusception in an infant as a manifestation of COVID-19. J. Pediatr. Surg. Case Rep. 2020, 59, 101533. [Google Scholar] [CrossRef]
- Makrinioti, H.; Mac Donald, A.; Lu, X.; Wallace, S.; Jobson, M.; Zhang, F.; Shao, J.; Bretherton, J.; Mehmood, T.; Eyre, E.; et al. Intussusception in 2 children with severe acute respiratory syndrome coronavirus-2 infection. J. Pediatr. Infect. Dis. Soc. 2020, 9, 504–506. [Google Scholar] [CrossRef]
- Khan, S.; Hartman, L.; Navarro, Y.J.S.; Rossini, C.J.; Burdett, C.; Pennell, C. Pediatric Covid-19 mesenteric lymphoid hyperplasia associated intussusception: A case report and literature review. J. Pediatr. Surg. Case Rep. 2021, 73, 101988. [Google Scholar] [CrossRef]
- Giovanni, J.E.; Hrapcak, S.; Melgar, M.; Godfred-Cato, S. Global Reports of Intussusception in Infants With SARS-CoV-2 Infection. Pediatr. Infect. Dis. J. 2021, 40, e35–e36. [Google Scholar] [CrossRef] [PubMed]
- Scottoni, F.; Giobbe, G.G.; Zambaiti, E.; Khalaf, S.; Sebire, N.J.; Curry, J.; De Coppi, P.; Gennari, F. Intussusception and COVID-19 in Infants: Evidence for an Etiopathologic Correlation. Pediatrics 2022, 149, e2021054644. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Factor | Control Group | Study Group 1 | Study Group 2 | p A |
|---|---|---|---|---|
| Total cases | 90 | 70 | 86 | 0.042 |
| Sex, male | 60(66.7%) | 45(64.3%) | 55(63.9%) | 0.125 |
| Age, mons. | 0.313 | |||
| Mean | 21.12 ± 11.24 | 22.35 ± 12.46 | 22.15 ± 14.26 | |
| Median (range) | 22.1(2.1–60.5) | 23.1(1.2–54.3) | 23.1(1.7–61.2) | |
| Address, out of Chengdu | 52(57.8%) | 30(42.8%) | 49(56.9%) | 0.027 |
| Past history of intussusception | 9(10.0%) | 6(8.5%) | 8(9.3%) | 0.114 |
| History of treatment in other hospitals | 25(27.7%) | 27(38.6%) | 26(30.2%) | 0.013 |
| Symptoms or signs | ||||
| Vomiting | 55(61.1%) | 41(58.6%) | 52(60.5%) | 0.374 |
| Abdominal pain | 58(64.4%) | 44(62.8%) | 55(63.9%) | 0.153 |
| Bloody stool | 20(22.2%) | 26(37.1%) | 21(24.4%) | 0.007 |
| Palpable mass | 42(46.6%) | 34(48.5%) | 40(46.5%) | 0.318 |
| Fever (T ≥ 37.3 °C) | 19(21.1%) | 15(21.4%) | 18(20.9%) | 0.936 |
| US for intussusception | ||||
| Number, solitary | 85(94.4%) | 66(94.3%) | 80(93.0%) | 0.715 |
| Type, ileocolic | 79(87.8%) | 62(88.6%) | 77(89.5%) | 0.357 |
| Length B, cm. | 0.042 | |||
| Mean | 4.1 ± 1.2 | 5.8 ± 1.3 | 3.9 ± 0.5 | |
| Median (range) | 3.2(2.5–7.5) | 4.1(3.3–9.0) | 3.1(2.6–6.5) | |
| Width C, cm. | 0.354 | |||
| Mean | 3.6 ± 0.5 | 3.3 ± 0.6 | 3.6 ± 0.4 | |
| Median (range) | 3.4(2.4–4.5) | 3.5(2.5–4.6) | 3.3(2.5–4.3) | |
| Swollen lymph nodes D | 25(27.7%) | 20(28.6%) | 26(30.2%) | 0.147 |
| USGHER | ||||
| Pressure, cmH2O | 0.091 | |||
| Mean | 102.1 ± 22.3 | 108.6 ± 24.2 | 103.8 ± 21.5 | |
| Median (range) | 100(80–120) | 100 (80–140) | 100 (80–140) | |
| Time of duration, min. | 0.085 | |||
| Mean | 4.3 ± 0.8 | 4.9 ± 1.5 | 4.4 ± 1.1 | |
| Median (range) | 4.1(1.5–15.2) | 4.4(2.5–20.4) | 4.1(2.1–18.5) | |
| Success to reduction | 87(96.7%) | 67(95.7%) | 83(96.5%) | 0.823 |
| Perforation | 0 | 0 | 0 | NA |
| Recurrence | 3(3.3%) | 2(2.9%) | 3(3.5%) | NA |
| Expense in ED, RMB | 0.072 | |||
| Mean | 4355.2 ± 357.1 | 4863.1 ± 331.4 | 4536.3 ± 401.7 | |
| Median (range) | 4255(4112.5–5237.6) | 4530(4168.2–5486.9) | 4436(4143.5–5343.8) | |
| Time span E, hours | ||||
| TTI 1 | 15.2 ± 6.1 | 22.5 ± 4.5 | 14.5 ± 7.8 | 0.036 |
| TTI 2 | 1.1 ± 0.4 | 2.2 ± 0.9 | 1.3 ± 0.7 | 0.031 |
| TTI 3 | 0.6 ± 0.2 | 0.8 ± 0.4 | 0.7 ± 0.4 | 0.334 |
| TTI 4 | 2.5 ± 0.7 | 3.1 ± 1.1 | 2.7 ± 1.4 | 0.518 |
| Time span | Fever Group (n = 33) | Non-fever Group (n = 123) | p |
|---|---|---|---|
| TTI 1, hours | 12.5 ± 3.2 | 20.1 ± 5.4 | 0.034 |
| TTI 2, hours | 2.3 ± 1.2 | 1.4 ± 0.5 | 0.028 |
| TTI 3, hours | 0.9 ± 0.4 | 0.8 ± 0.2 | 0.256 |
| TTI 4, hours | 4.2 ± 1.2 | 3.1 ± 0.8 | 0.041 |
| Factor | Study Group 1 (n = 70) | Study Group 2 (n = 86) |
|---|---|---|
| Fever (T ≥ 37.3 °C) | 15 (21.4%) | 18(20.9%) |
| Non-gastrointestinal Symptoms A | 12 (17.1%) | 14(16.3%) |
| Inquiring the COVID-19 epidemiological history | 100 | 100 |
| Chest CT scan | 20 (28.6%) | 15(17.4%) |
| Detection of antibodies against SARS-CoV-2 | 11(15.7%) | 6(6.9%) |
| Detection of nucleic acid against SARS-CoV-2 | 7 (10%) | 23 (26.7%) |
| History of COVID-19 exposure or touch | 0(0%) | 0(0%) |
| COVID-19 confirmed | 0(0%) | 0(0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, M.; Gou, Z.-H.; Wang, J.; Liu, J.-X.; Xiang, B. How Does the COVID-19 Pandemic Affect Pediatric Patients with Intussusception Treated by Ultrasound-Guided Hydrostatic Enema Reduction? J. Clin. Med. 2022, 11, 4473. https://doi.org/10.3390/jcm11154473
Yang M, Gou Z-H, Wang J, Liu J-X, Xiang B. How Does the COVID-19 Pandemic Affect Pediatric Patients with Intussusception Treated by Ultrasound-Guided Hydrostatic Enema Reduction? Journal of Clinical Medicine. 2022; 11(15):4473. https://doi.org/10.3390/jcm11154473
Chicago/Turabian StyleYang, Min, Ze-Hui Gou, Jun Wang, Ju-Xian Liu, and Bo Xiang. 2022. "How Does the COVID-19 Pandemic Affect Pediatric Patients with Intussusception Treated by Ultrasound-Guided Hydrostatic Enema Reduction?" Journal of Clinical Medicine 11, no. 15: 4473. https://doi.org/10.3390/jcm11154473
APA StyleYang, M., Gou, Z.-H., Wang, J., Liu, J.-X., & Xiang, B. (2022). How Does the COVID-19 Pandemic Affect Pediatric Patients with Intussusception Treated by Ultrasound-Guided Hydrostatic Enema Reduction? Journal of Clinical Medicine, 11(15), 4473. https://doi.org/10.3390/jcm11154473