
Do Elderly Patients with Atrial Fibrillation Have Comparable Ablation Outcomes Compared to Younger Ones? Evidence from Pooled Clinical Studies

Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Search Strategy
2.3. Search Design
2.4. Data Extraction and Quality Assessment
2.5. Statistical Analysis
3. Results
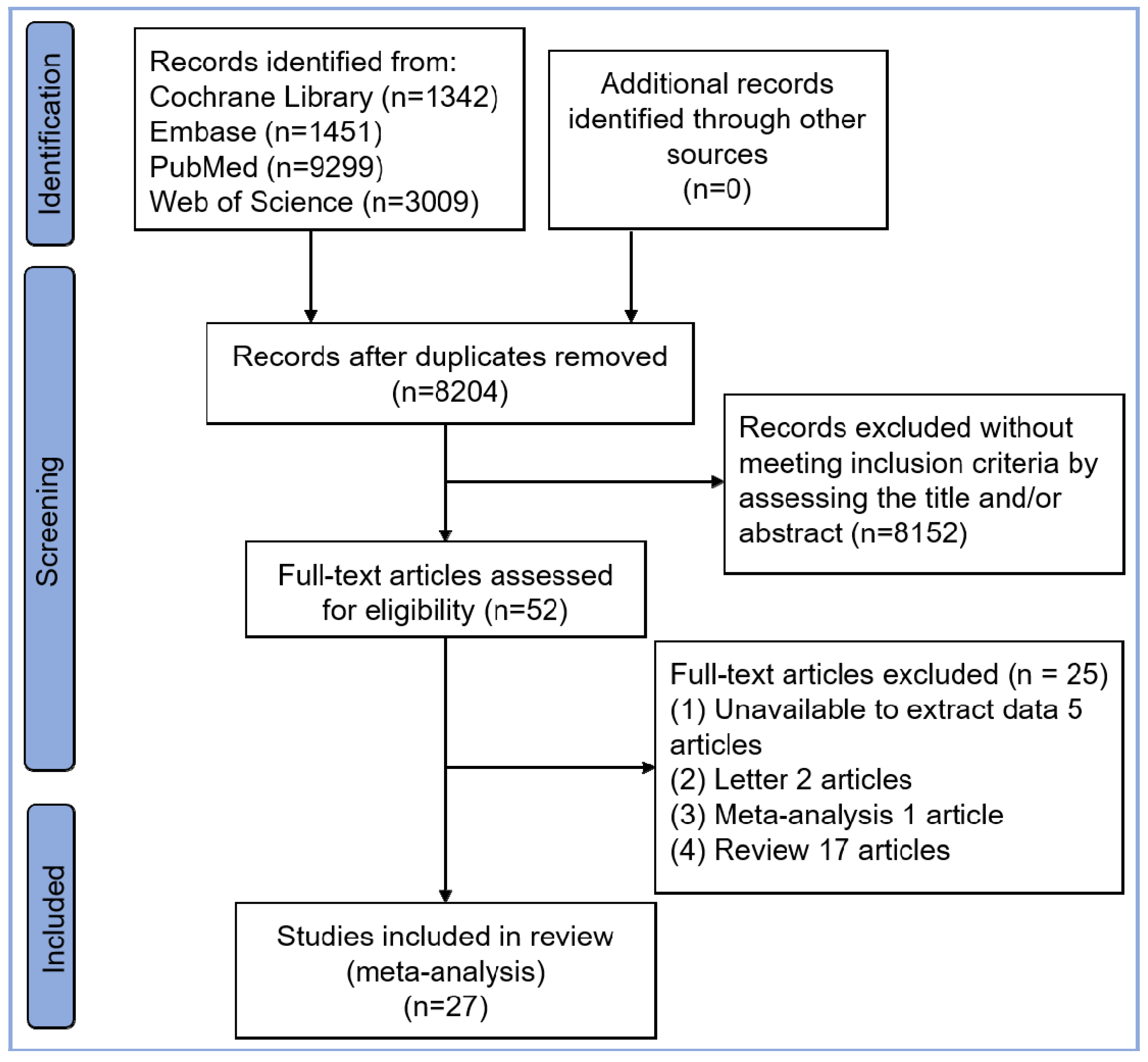
3.1. Study Selection and Quality Assessment
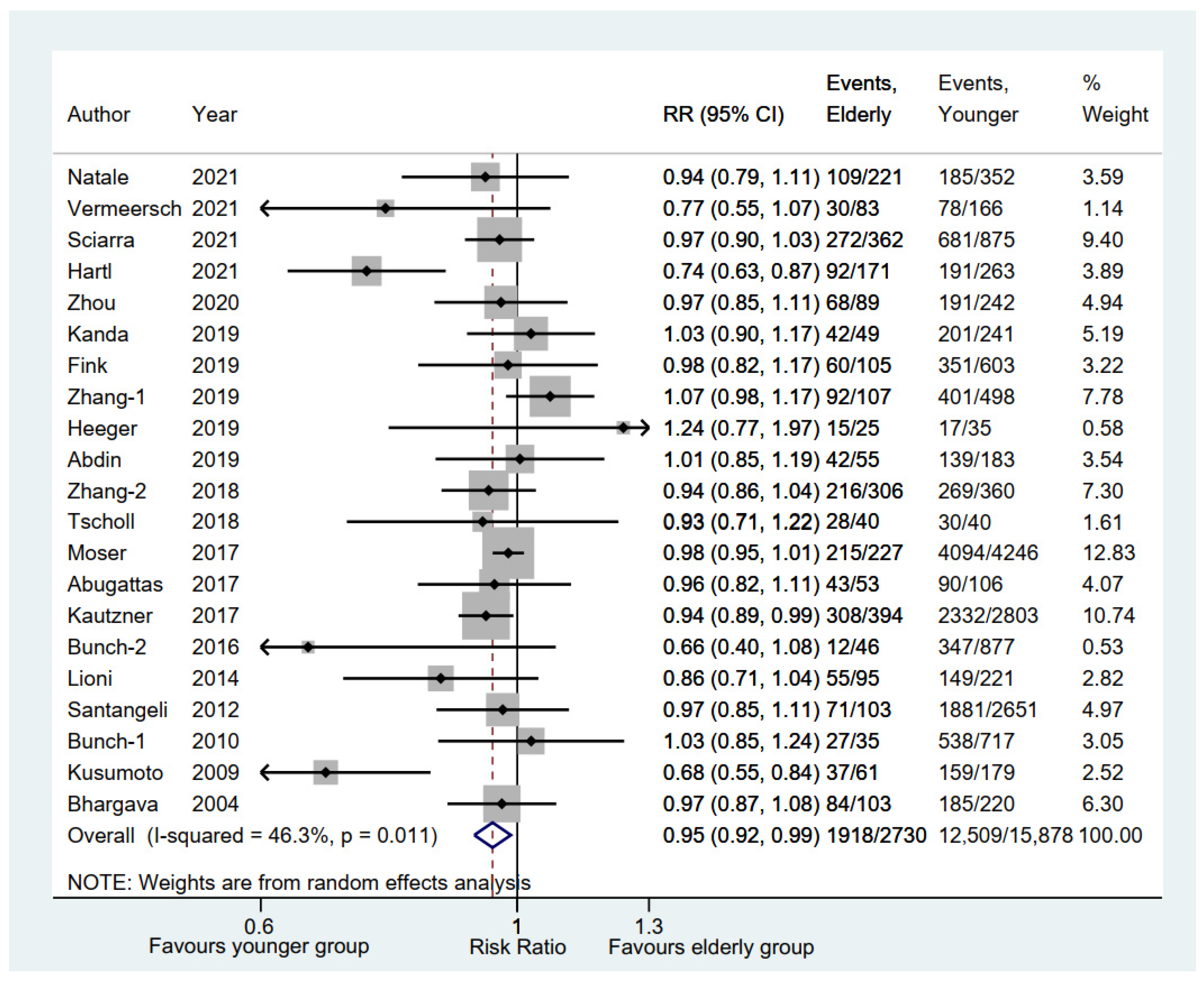
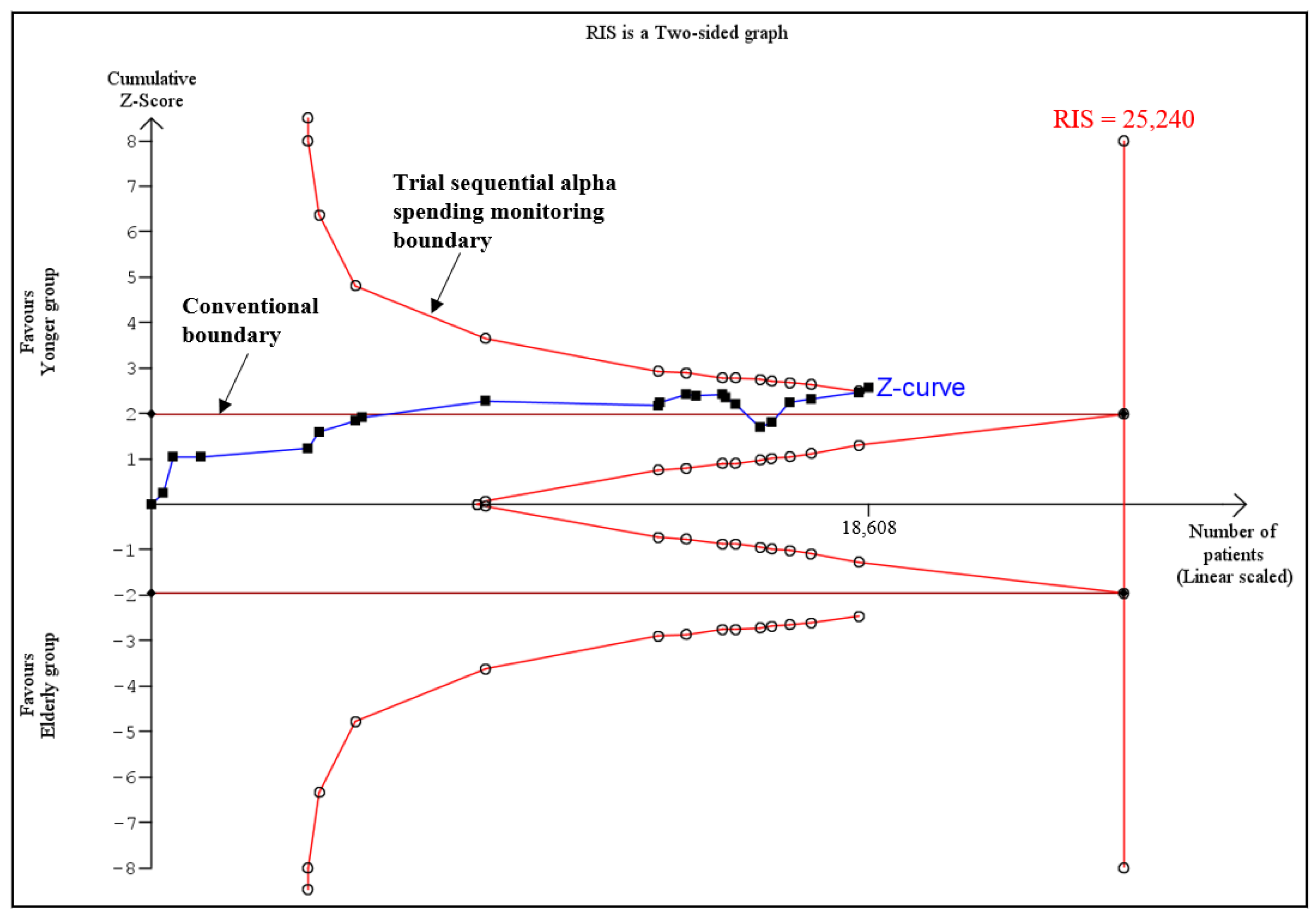
3.2. Rate of Freedom from AF between Elderly and Younger Groups
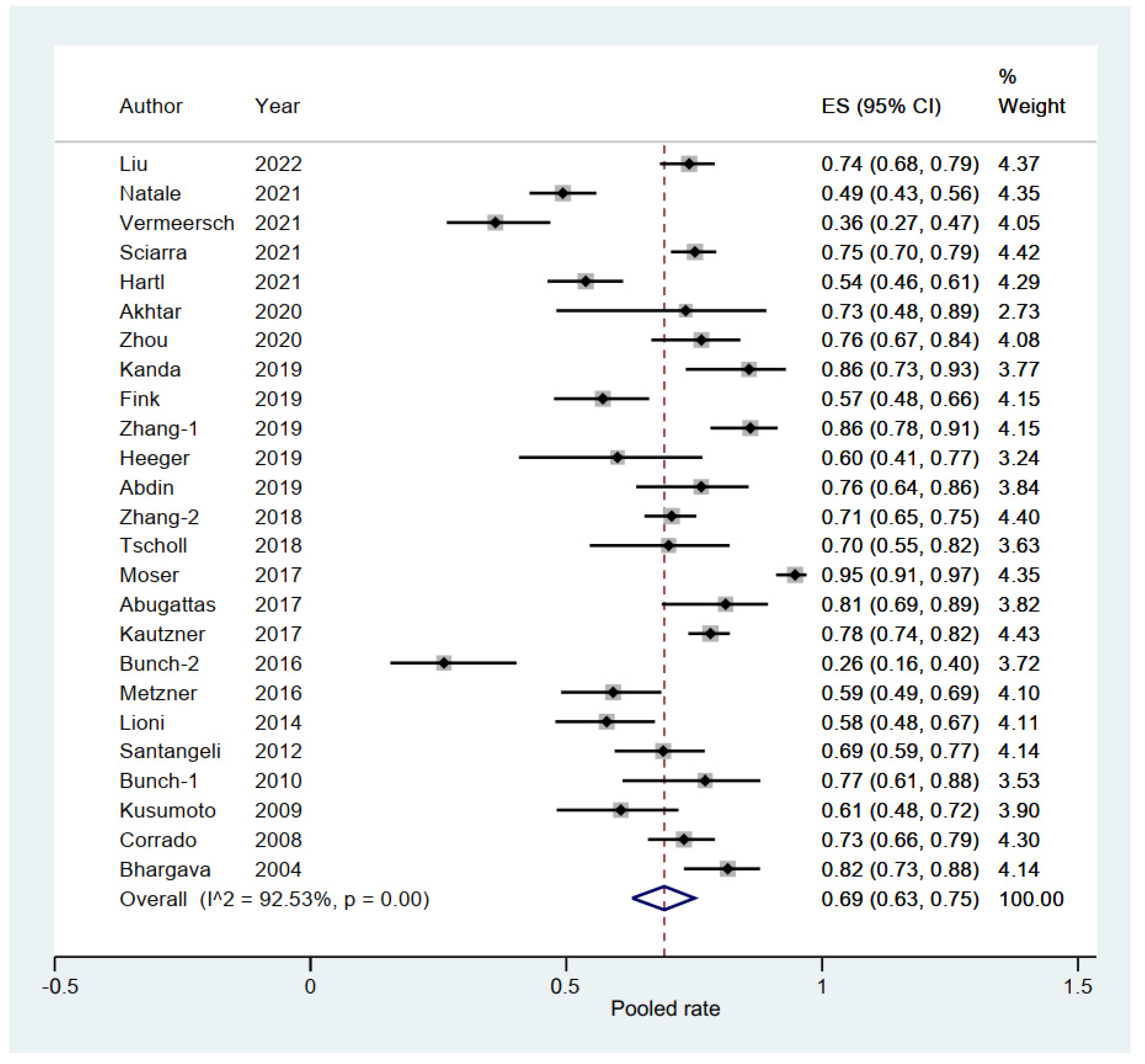
3.3. Pooled Rate of Freedom from AF in Elderly Group
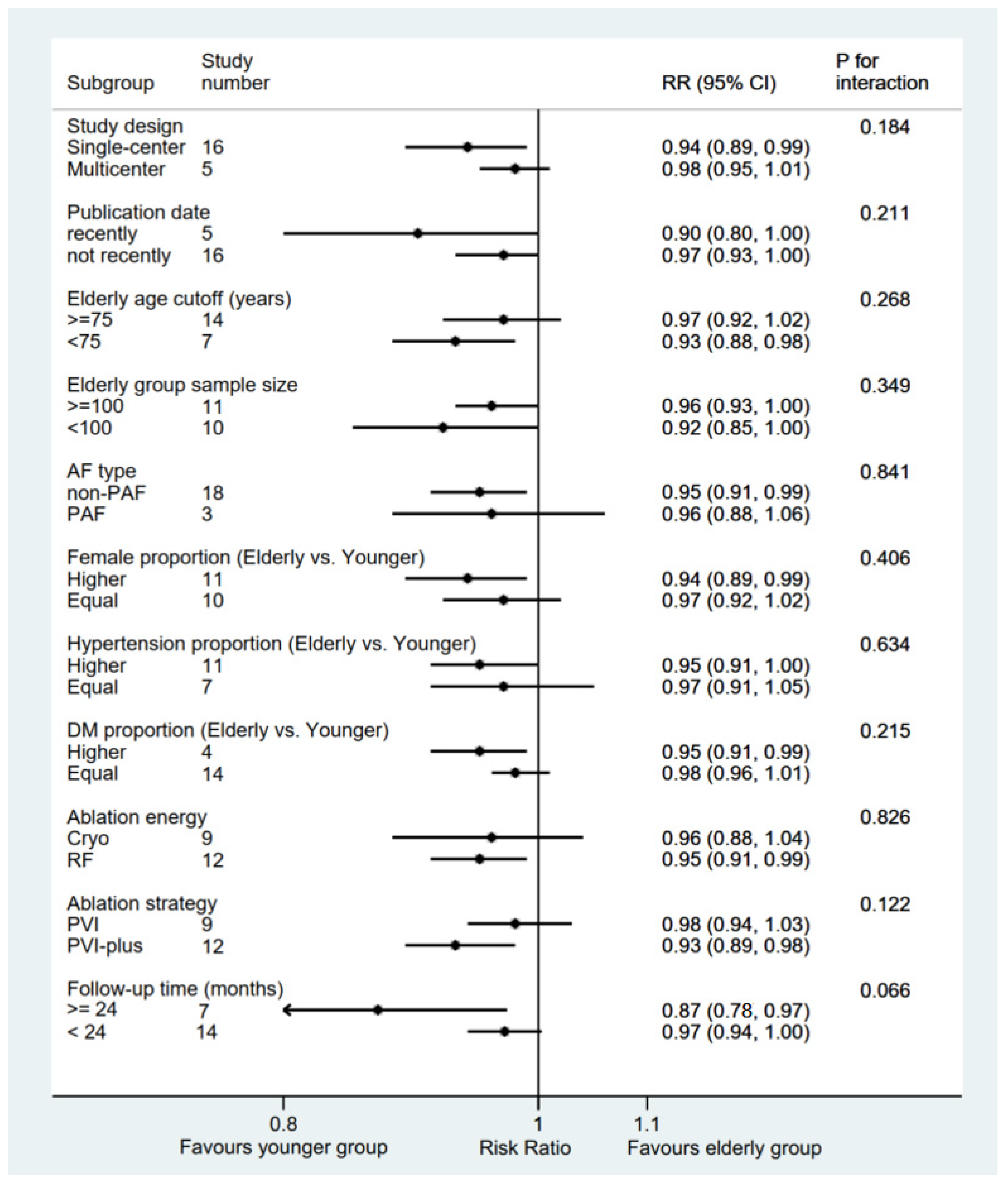
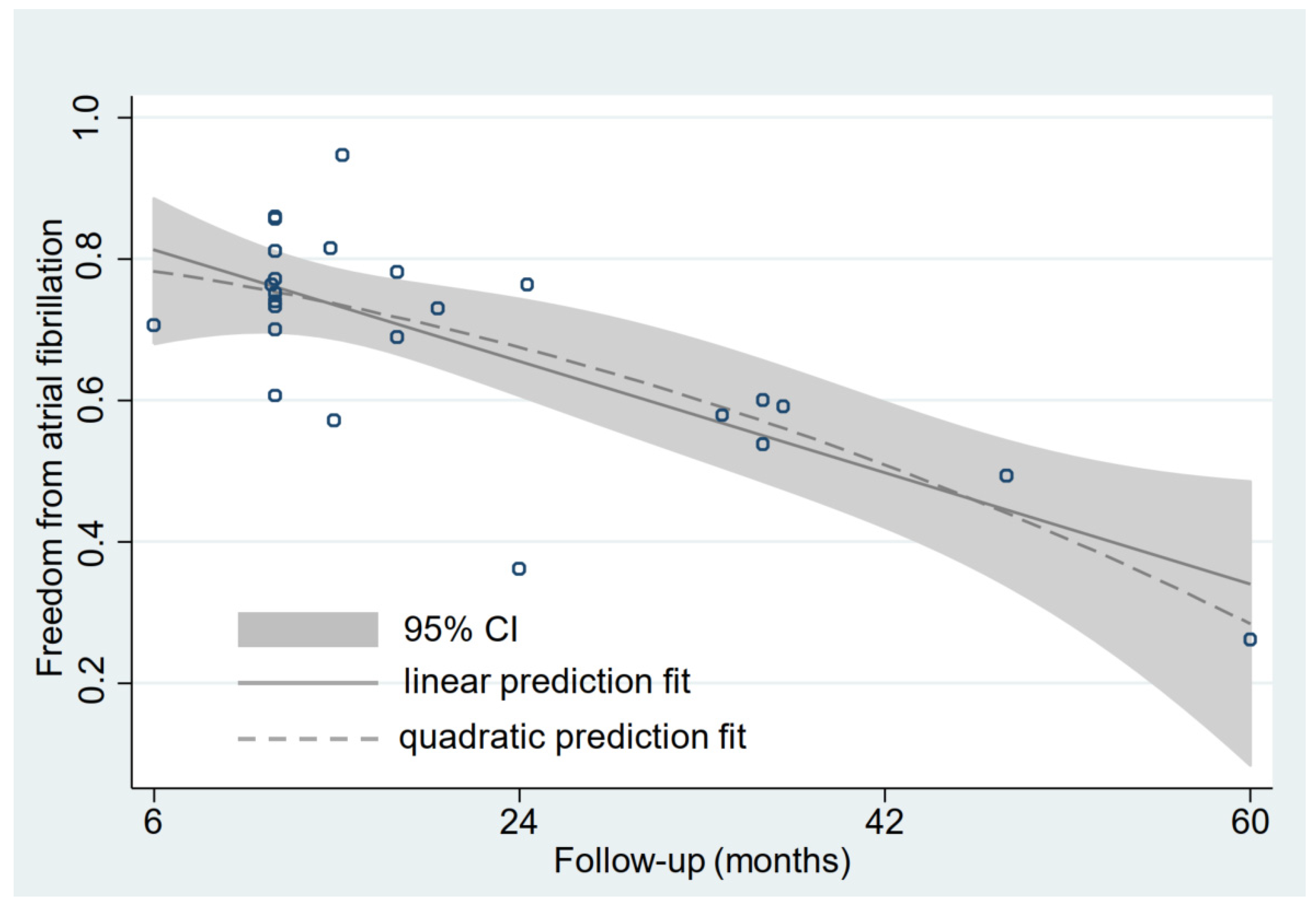
3.4. Relationship between Follow-Up Time and Rate of Freedom from AF
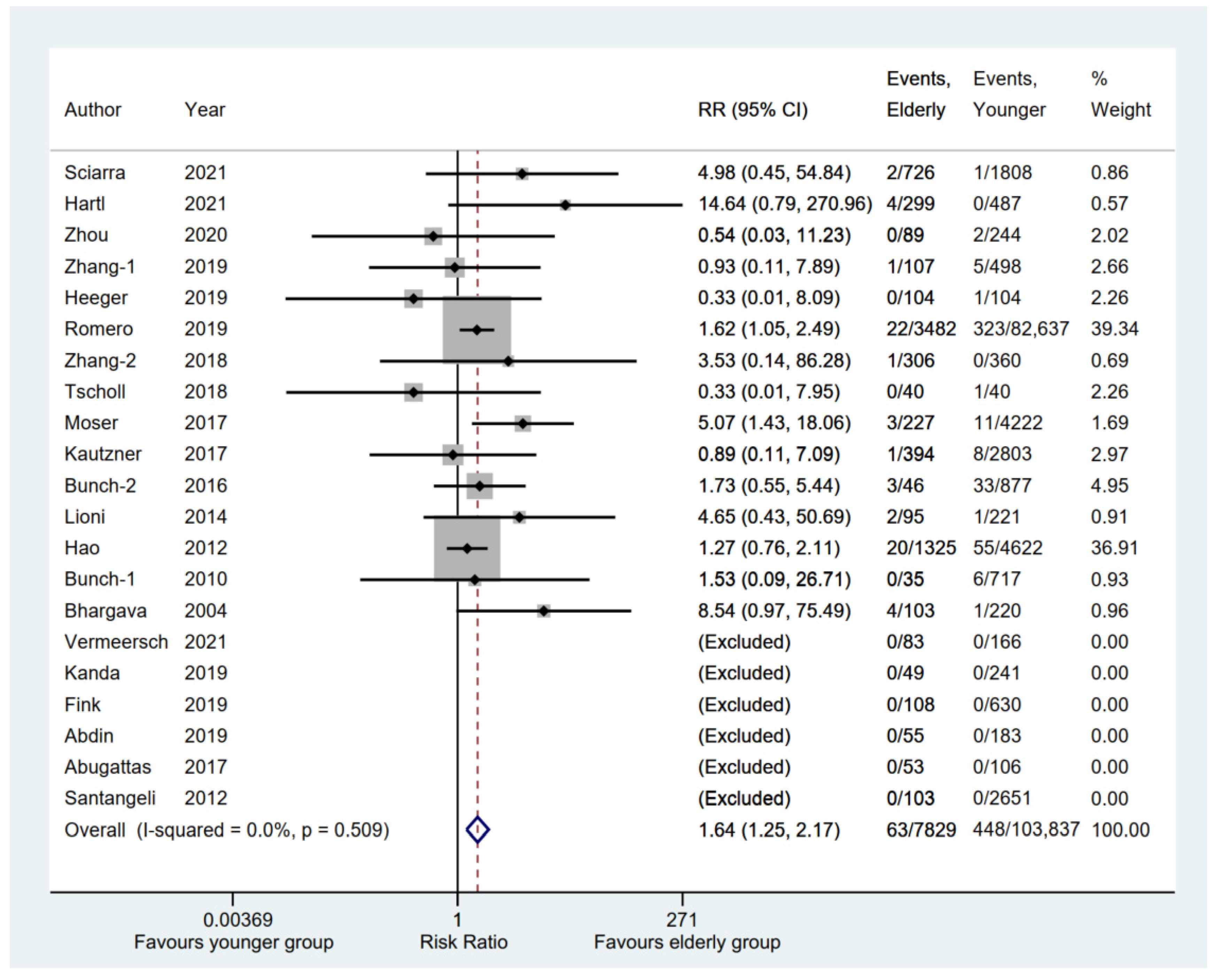
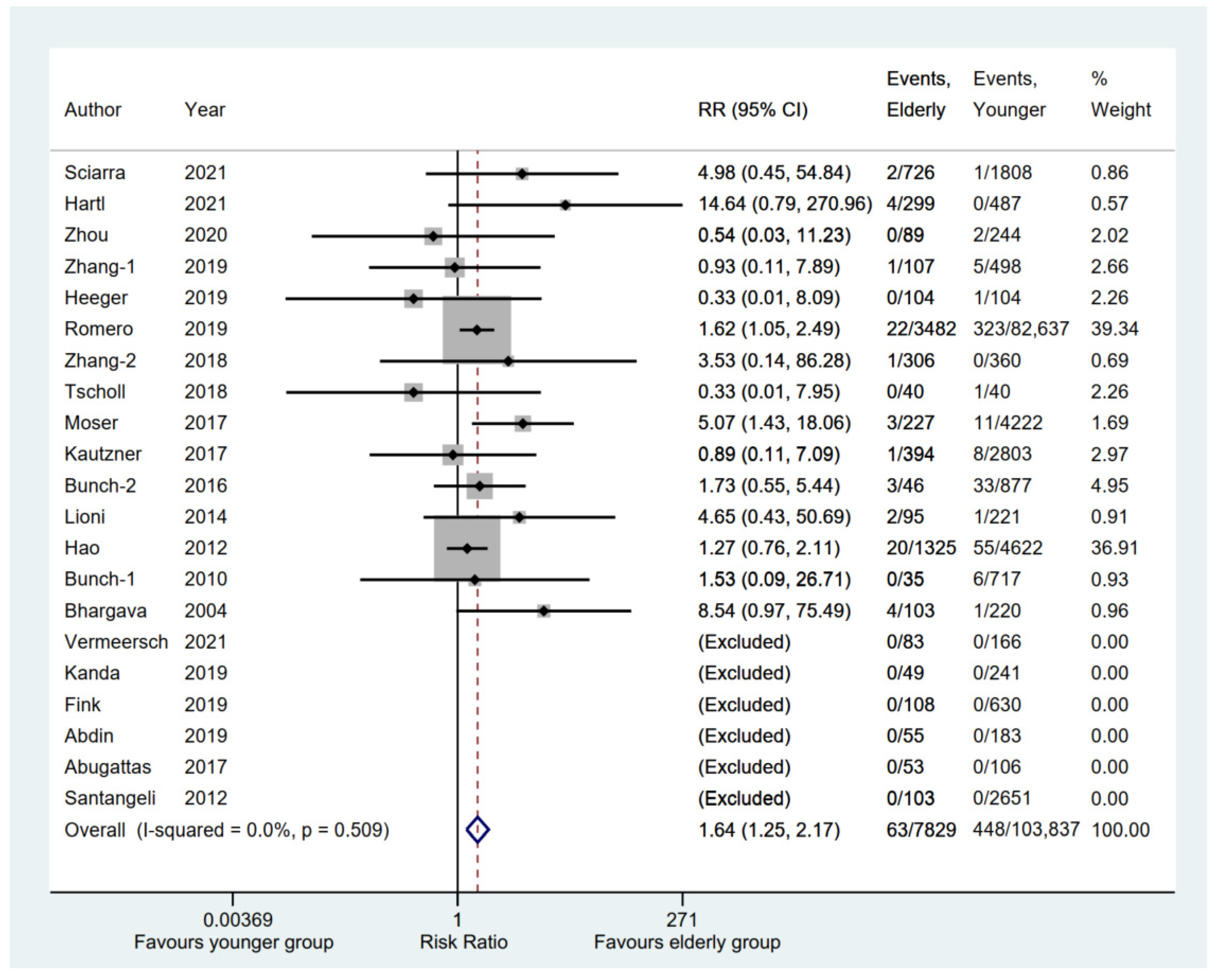
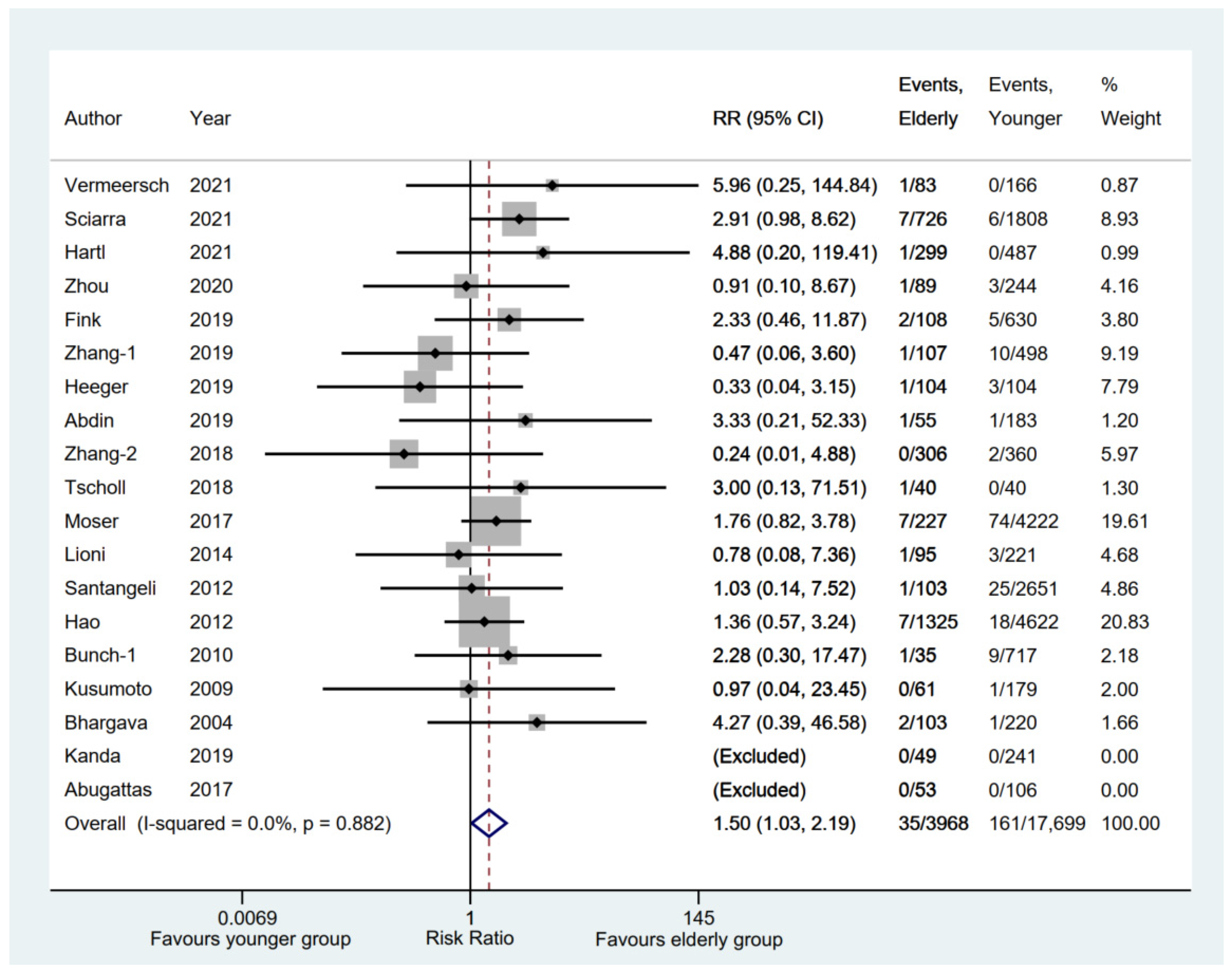
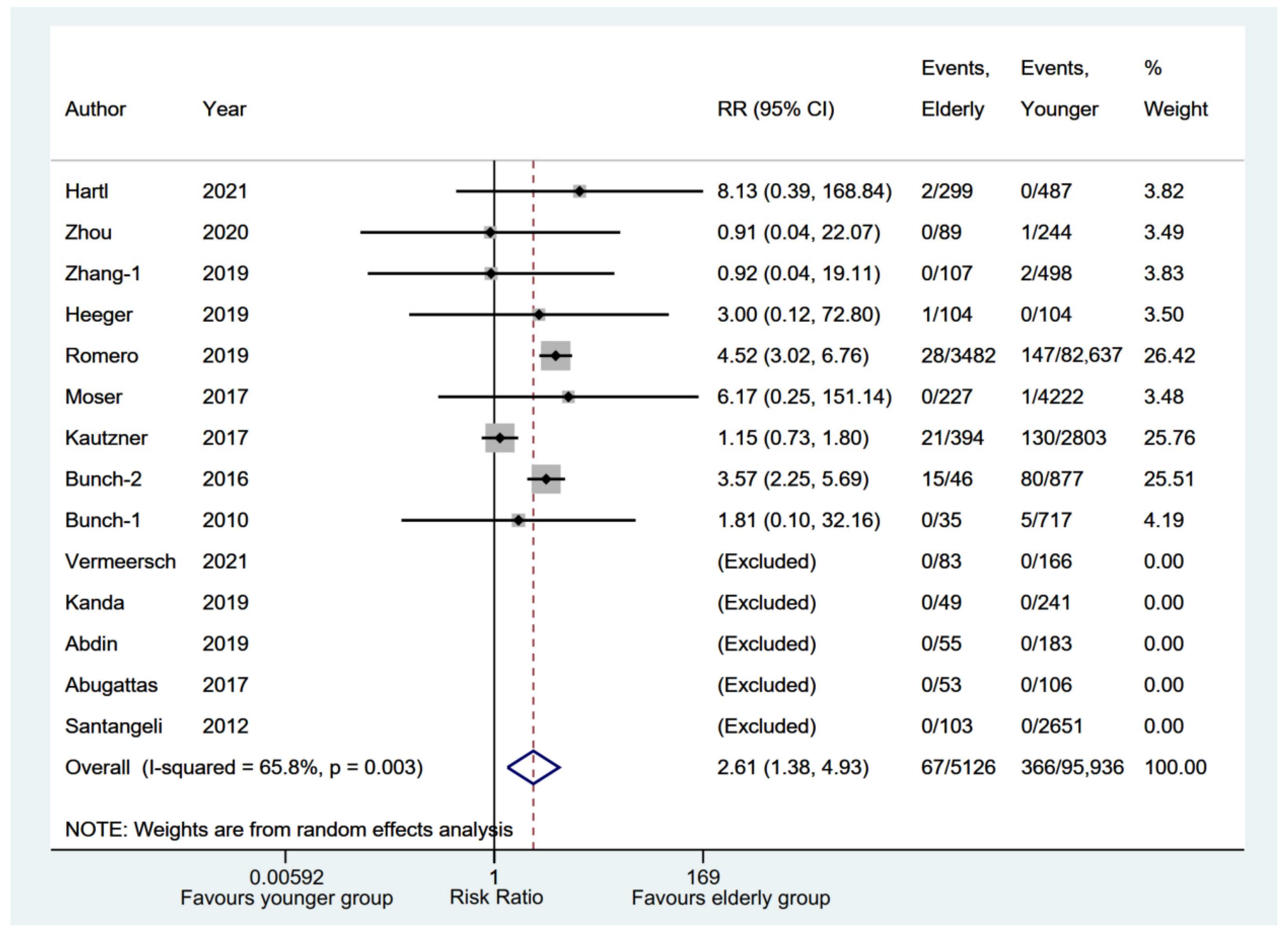
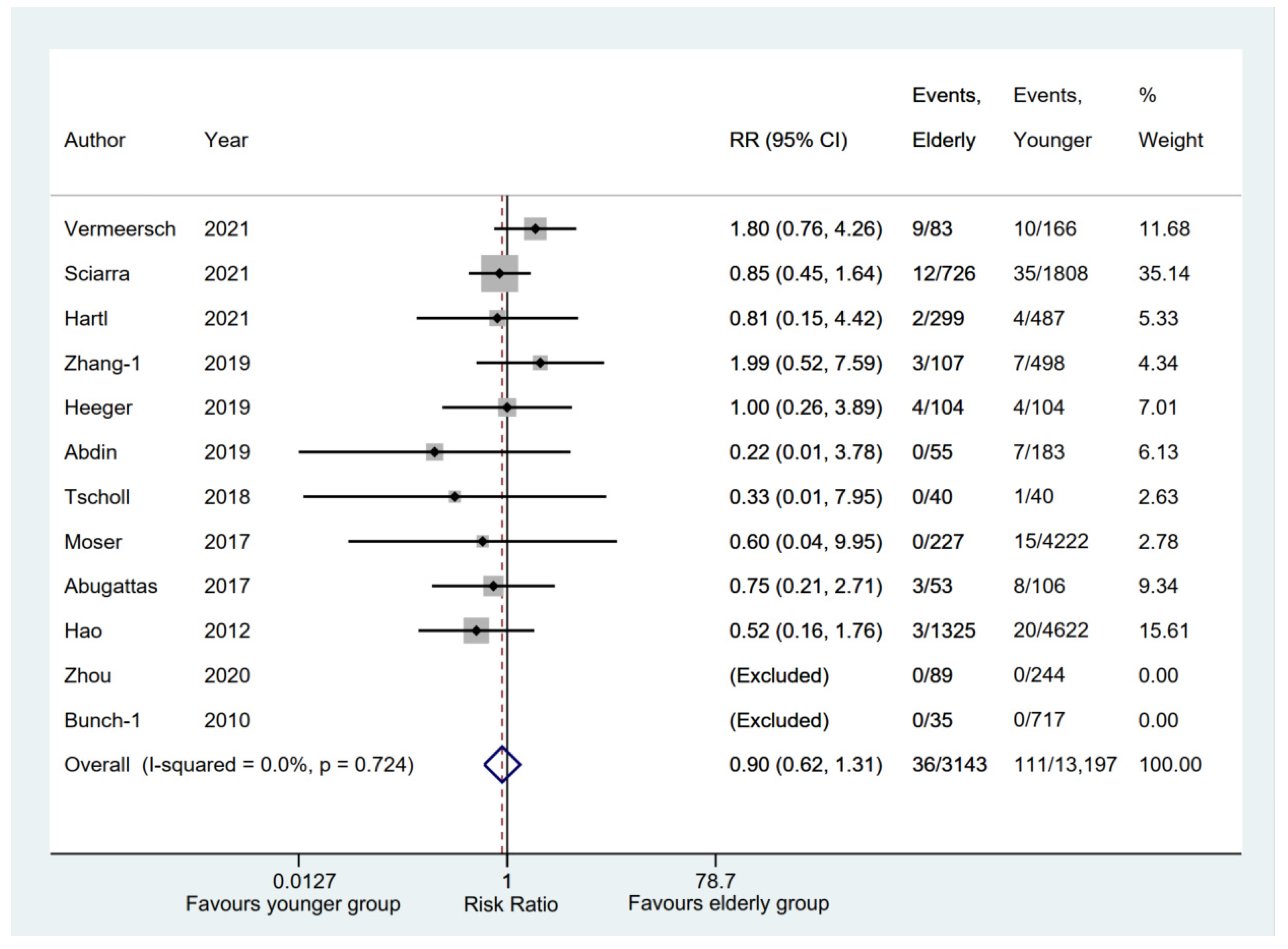
3.5. Safety Outcomes between Elderly and Younger Groups
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge. Int. J. Stroke 2021, 16, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Volgman, A.S.; Nair, G.; Lyubarova, R.; Merchant, F.M.; Mason, P.; Curtis, A.B.; Wenger, N.K.; Aggarwal, N.T.; Kirkpatrick, J.N.; Benjamin, E.J. Management of atrial fibrillation in patients 75 years and older: JACC state-of-the-art review. J. Am. Coll. Cardiol. 2022, 79, 166–179. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Yang, P.S.; Sung, J.H.; Kim, D.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Pak, H.-N.; Lee, M.-H.; et al. Frailty and the effect of catheter ablation in the elderly population with atrial fibrillation-a real-world analysis. Circ. J. 2021, 85, 1305–1313. [Google Scholar] [CrossRef]
- Kim, D.; Yang, P.-S.; You, S.C.; Jang, E.; Yu, H.T.; Kim, T.-H.; Pak, H.-N.; Lee, M.-H.; Lip, G.Y.H.; Sung, J.-H.; et al. Age and outcomes of early rhythm control in patients with atrial fibrillation: Nationwide cohort study. JACC Clin. Electrophysiol. 2022, 8, 619–632. [Google Scholar] [CrossRef]
- Vermeersch, G.; Abugattas, J.-P.; Varnavas, V.; De Cocker, J.; Schwagten, B.; Sieira, J.; De Asmundis, C.; Chierchia, G.-B.; De Greef, Y. Efficacy and safety of the second-generation cryoballoon ablation for the treatment of persistent atrial fibrillation in elderly patients. J. Arrhythm. 2021, 37, 626–634. [Google Scholar] [CrossRef]
- Furlan, A.D.; Pennick, V.; Bombardier, C.; van Tulde, M.; Editorial Board; Cochrane Back Review Group. 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine (Phila Pa 1976) 2009, 34, 1929–1941. [Google Scholar] [CrossRef] [PubMed]
- Guo, B.; Moga, C.; Harstall, C.; Schopflocher, D. A principal component analysis is conducted for a case series quality appraisal checklist. J. Clin. Epidemiol. 2016, 69, 199–207.e2. [Google Scholar] [CrossRef]
- Brok, J.; Thorlund, K.; Gluud, C.; Wetterslev, J. Trial sequential analysis reveals insufficient information size and potentially false positive results in many meta-analyses. J. Clin. Epidemiol. 2008, 61, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Natale, V.; Mohanty, S.; Trivedi, C.; Baqai, F.M.; Gallinghouse, J.; Rocca, D.G.D.; Gianni, C.; MacDonald, B.; Mayedo, A.; Burkhardt, J.D.; et al. Arrhythmia profile and ablation-outcome in elderly women with atrial fibrillation undergoing first catheter ablation. Pacing Clin. Electrophysiol. 2021, 44, 835–842. [Google Scholar] [CrossRef]
- Sciarra, L.; Iacopino, S.; Arena, G.; Tondo, C.; Pieragnoli, P.; Molon, G.; Manfrin, M.; Curnis, A.; Russo, A.D.; Rovaris, G.; et al. Safety and efficacy of Cryoballoon ablation of atrial fibrillation in relation to the patients’ age: Results from a large real-world multicenter observational project. Cardiol. Res. Pract. 2021, 2021, 9996047. [Google Scholar] [CrossRef]
- Hartl, S.; Dorwarth, U.; Pongratz, J.; Aurich, F.; Brück, B.; Tesche, C.; Ebersberger, U.; Wankerl, M.; Hoffmann, E.; Straube, F. Impact of age on the outcome of cryoballoon ablation as the primary approach in the interventional treatment of atrial fibrillation: Insights from a large all-comer study. J. Cardiovasc. Electrophysiol. 2021, 32, 949–957. [Google Scholar] [CrossRef]
- Zhou, G.; Cai, L.; Wu, X.; Zhang, L.; Chen, S.; Lu, X.; Xu, J.; Ding, Y.; Peng, S.; Wei, Y.; et al. Clinical efficacy and safety of radiofrequency catheter ablation for atrial fibrillation in patients aged ≥80 years. Pacing Clin. Electrophysiol. 2020, 43, 814–821. [Google Scholar] [CrossRef]
- Kanda, T.; Masuda, M.; Kurata, N.; Asai, M.; Iida, O.; Okamoto, S.; Ishihara, T.; Nanto, K.; Tsujimura, T.; Okuno, S.; et al. Efficacy and safety of the cryoballoon-based atrial fibrillation ablation in patients aged ≥80 years. J. Cardiovasc. Electrophysiol. 2019, 30, 2242–2247. [Google Scholar] [CrossRef] [PubMed]
- Fink, T.; Metzner, A.; Willems, S.; Eckardt, L.; Ince, H.; Brachmann, J.; Spitzer, S.G.; Deneke, T.; Schmitt, C.; Hochadel, M.; et al. Procedural success, safety and patients satisfaction after second ablation of atrial fibrillation in the elderly: Results from the German Ablation Registry. Clin. Res. Cardiol. 2019, 108, 1354–1363. [Google Scholar] [CrossRef]
- Zhang, J.; Ren, Z.; Wang, S.; Zhang, J.; Yang, H.; Zheng, Y.; Meng, W.; Zhao, D.; Xu, Y. Efficacy and safety of cryoballoon ablation for Chinese patients over 75 years old: A comparison with a younger cohort. J. Cardiovasc. Electrophysiol. 2019, 30, 2734–2742. [Google Scholar] [CrossRef]
- Heeger, C.-H.; Bellmann, B.; Fink, T.; Bohnen, J.E.; Wissner, E.; Wohlmuth, P.; Rottner, L.; Sohns, C.; Tilz, R.R.; Mathew, S.; et al. Efficacy and safety of cryoballoon ablation in the elderly: A multicenter study. Int. J. Cardiol. 2019, 278, 108–113. [Google Scholar] [CrossRef]
- Romero, J.; Ogunbayo, G.; Elayi, S.C.; Darrat, Y.; Rios, S.A.; Diaz, J.C.; Alviz, I.; Cerna, L.; Gabr, M.; Chernobelsky, E.; et al. Safety of catheter ablation for atrial fibrillation in the octogenarian population. J. Cardiovasc. Electrophysiol. 2019, 30, 2686–2693. [Google Scholar] [CrossRef]
- Abdin, A.; Yalin, K.; Lyan, E.; Sawan, N.; Liosis, S.; Meyer-Saraei, R.; Elsner, C.; Lange, S.A.; Heeger, C.; Eitel, C.; et al. Safety and efficacy of cryoballoon ablation for the treatment of atrial fibrillation in elderly patients. Clin. Res. Cardiol. 2019, 108, 167–174. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Yu, R.H.; Dong, J.Z. Clinical characteristics and efficacy of radiofrequency catheter ablation in the treatment of elderly patients with atrial fibrillation. Am. J. Med. Sci. 2018, 355, 357–361. [Google Scholar] [CrossRef]
- Tscholl, V.; Lin, T.; Lsharaf, A.K.; Bellmann, B.; Nagel, P.; Lenz, K.; Landmesser, U.; Roser, M.; Rillig, A. Cryoballoon ablation in the elderly: One year outcome and safety of the second-generation 28mm cryoballoon in patients over 75 years old. Ep Eur. 2018, 20, 772–777. [Google Scholar] [CrossRef]
- Moser, J.M.; Willems, S.; Andresen, D.; Brachmann, J.; Eckardt, L.; Hoffmann, E.; Kuck, K.; Lewalter, T.; Schumacher, B.; Spitzer, S.G.; et al. Complication rates of catheter ablation of atrial fibrillation in patients aged ≥75 years versus <75 years-results from the German ablation registry. J. Cardiovasc. Electrophysiol. 2017, 28, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Abugattas, J.P.; Iacopino, S.; Moran, D.; de Regibus, V.; Takarada, K.; Mugnai, G.; Ströker, E.; Coutiño-Moreno, H.E.; Choudhury, R.; Storti, C.; et al. Efficacy and safety of the second generation cryoballoon ablation for the treatment of paroxysmal atrial fibrillation in patients over 75 years: A comparison with a younger cohort. Europace 2017, 19, 1798–1803. [Google Scholar] [CrossRef] [PubMed]
- Kautzner, J.; Peichl, P.; Sramko, M.; Cihak, R.; Aldhoon, B.; Wichterle, D. Catheter ablation of atrial fibrillation in elderly population. J. Geriatr. Cardiol. 2017, 14, 563–568. [Google Scholar]
- Bunch, T.J.; May, H.T.; Bair, T.L.; Jacobs, V.; Crandall, B.G.; Cutler, M.; Weiss, J.P.; Mallender, C.; Osborn, J.S.; Anderson, J.L.; et al. The impact of age on 5-year outcomes after atrial fibrillation catheter ablation. J Cardiovasc. Electrophysiol. 2016, 27, 141–146. [Google Scholar] [CrossRef]
- Lioni, L.; Letsas, K.P.; Efremidis, M.; Vlachos, K.; Giannopoulos, G.; Kareliotis, V.; Deftereos, S.; Sideris, A. Catheter ablation of atrial fibrillation in the elderly. J. Geriatr. Cardiol. 2014, 11, 291–295. [Google Scholar]
- Santangeli, P.; Di Biase, L.; Mohanty, P.; Burkhardt, J.D.; Horton, R.; Bai, R.; Mohanty, S.; Pump, A.; Gibson, D.; Couts, L.; et al. Catheter ablation of atrial fibrillation in octogenarians: Safety and outcomes. J. Cardiovasc. Electrophysiol. 2012, 23, 687–693. [Google Scholar] [CrossRef]
- Hao, S.C.; Hunter, T.D.; Gunnarsson, C.; March, J.L.; White, S.A.; Ladapo, J.A.; Reynolds, M.R. Acute safety outcomes in younger and older patients with atrial fibrillation treated with catheter ablation. J. Interv. Card Electrophysiol. 2012, 35, 173–182. [Google Scholar] [CrossRef]
- Bunch, T.J.; Weiss, J.P.; Crandall, B.G.; May, H.T.; Bair, T.L.; Osborn, J.S.; Anderson, J.L.; Lappe, D.L.; Muhlestein, J.B.; Nelson, J.; et al. Long-term clinical efficacy and risk of catheter ablation for atrial fibrillation in octogenarians. Pacing Clin. Electrophysiol. 2010, 33, 146–152. [Google Scholar] [CrossRef]
- Kusumoto, F.; Prussak, K.; Wiesinger, M.; Pullen, T.; Lynady, C. Radiofrequency catheter ablation of atrial fibrillation in older patients: Outcomes and complications. J. Interv. Card Electrophysiol. 2009, 25, 31–35. [Google Scholar] [CrossRef]
- Bhargava, M.; Marrouche, N.F.; Martin, D.O.; Schweikert, R.A.; Saliba, W.; Saad, E.B.; Bash, D.; Williams-Andrews, M.I.C.H.E.L.L.E.; Rossillo, A.; Erciyes, D.; et al. Impact of age on the outcome of pulmonary vein isolation for atrial fibrillation using circular mapping technique and cooled-tip ablation catheter. J. Cardiovasc. Electrophysiol. 2004, 15, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.Y.; Du, X.; He, L.; Liu, T.; Chen, N.; Hu, R.; Ning, M.; Lv, Q.; Dong, J.; Ma, C. Evaluation of safety and effectiveness on catheter ablation of atrial fibrillation in patients aged ≥80 years. Heart Lung Circ. 2022, 31, 1006–1014. [Google Scholar] [CrossRef]
- Akhtar, T.; Berger, R.; Marine, J.E.; Daimee, U.A.; Calkins, H.; Spragg, D. Cryoballoon Ablation of Atrial Fibrillation in Octogenarians. Arrhythm. Electrophysiol. Rev. 2020, 9, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Metzner, I.; Wissner, E.; Tilz, R.R.; Rillig, A.; Mathew, S.; Schmidt, B.; Chun, J.; Wohlmuth, P.; Deiss, S.; Lemes, C.; et al. Ablation of atrial fibrillation in patients ≥75 years: Long-term clinical outcome and safety. Europace 2016, 18, 543–549. [Google Scholar] [CrossRef]
- Corrado, A.; Patel, D.; Riedlbauchova, L.; Fahmy, T.S.; Themistoclakis, S.; Bonso, A.; Rossillo, A.; Hao, S.; Schweikert, R.A.; Cummings, J.E.; et al. Efficacy, safety, and outcome of atrial fibrillation ablation in septuagenarians. J. Cardiovasc. Electrophysiol. 2008, 19, 807–811. [Google Scholar] [CrossRef]
- Brunetti, N.D.; Santoro, F.; Correale, M.; de Gennaro, L.; Conte, G.; di Biase, M. Incidence of atrial fibrillation is associated with age and gender in subjects practicing physical exercise: A meta-analysis and meta-regression analysis. Int. J. Cardiol. 2016, 221, 1056–1060. [Google Scholar] [CrossRef] [PubMed]
- Bahnson, T.D.; Giczewska, A.; Mark, D.B.; Russo, A.M.; Monahan, K.H.; Al-Khalidi, H.R.; Silverstein, A.P.; Poole, J.E.; Lee, K.L.; Packer, D.L. Association between age and outcomes of catheter ablation versus medical therapy for atrial fibrillation: Results from the CABANA trial. Circulation 2022, 145, 796–804. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Huang, H.; Huang, C.; Zhang, S.; Ma, C.; Liu, X.; Yang, Y.; Cao, K.; Wu, S.; Wang, F. Catheter ablation of atrial fibrillation in Chinese elderly patients. Int. J. Cardiol. 2011, 152, 266–267. [Google Scholar] [CrossRef]
- Latchamsetty, R.; Morady, F. Catheter ablation of atrial fibrillation. Heart Fail. Clin. 2016, 12, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Parameswaran, R.; Al-Kaisey, A.M.; Kalman, J.M. Catheter ablation for atrial fibrillation: Current indications and evolving technologies. Nat. Rev. Cardiol. 2021, 18, 210–225. [Google Scholar] [CrossRef]
- Oral, H.; Pappone, C.; Chugh, A.; Good, E.; Bogun, F.; Pelosi, F., Jr.; Bates, E.R.; Lehmann, M.H.; Vicedomini, G.; Augello, G.; et al. Circumferential pulmonary-vein ablation for chronic atrial fibrillation. N. Engl. J. Med. 2006, 354, 934–941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, A.G.; Stiles, M.K.; Laborderie, J.; Lau, D.H.; Kuklik, P.; Shipp, N.J.; Hsu, L.; Sanders, P. Outcomes of long-standing persistent atrial fibrillation ablation: A systematic review. Heart Rhythm. 2010, 7, 835–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latchamsetty, R.; Morady, F. Long-term benefits following catheter ablation of atrial fibrillation. Circ. J. 2013, 77, 1091–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chibber, T.; Baranchuk, A. Sex-related differences in catheter ablation for patients with atrial fibrillation and heart failure. Front. Cardiovasc. Med. 2020, 7, 614031. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.R.; Nalliah, C.J.; Lee, G.; Voskoboinik, A.; Chieng, D.; Prabhu, S.; Parameswaran, R.; Sugumar, H.; Al-Kaisey, A.; McLellan, A.; et al. Sex-related differences in atrial remodeling in patients with atrial fibrillation: Relationship to ablation outcomes. Circ. Arrhythm. Electrophysiol. 2022, 15, e009925. [Google Scholar] [CrossRef] [PubMed]
- Packer, D.L.; Mark, D.B.; Robb, R.A.; Monahan, K.H.; Bahnson, T.D.; Poole, J.E.; Noseworthy, P.A.; Rosenberg, Y.D.; Jeffries, N.; Mitchell, L.B.; et al. Effect of catheter ablation vs. antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: The CABANA randomized clinical Trial. JAMA 2019, 321, 1261–1274. [Google Scholar] [CrossRef]
- Piché, M.E.; Tchernof, A.; Després, J.P. Obesity phenotypes, diabetes, and cardiovascular diseases. Circ. Res. 2020, 126, 1477–1500. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Study Design | Country | Sample Size | Elderly Age Cutoff (Years) | Gender (Female, %) | AF Type (PAF, %) | Hypertension (%) | DM (%) | |||||
| Elderly Group | Younger Group | Elderly Group | Younger Group | Elderly Group | Younger Group | Elderly Group | Younger Group | Elderly Group | Younger Group | |||||
| Natale [10] | 2021 | Observational single-center | America | 221 | 352 | 75 | 100.0 | 100.0 | 10.9 | 14.8 | 69.7 $ | 53.4 | 10.9 | 14.8 |
| Vermeersch [6] | 2021 | Retrospective single-center | Belgium | 83 | 166 | 75 | 41.0 | 39.2 | 0 | 0 | 73.5 $ | 55.4 | 14.5 | 13.9 |
| Sciarra [11] | 2021 | Prospective multicenter | Italy | 726 | 1808 | 67 | 37.5 # | 23.4 | 73.6 | 75.5 | 62.8 $ | 41.3 | 7.2 & | 4.7 |
| Hartl [12] | 2021 | Observational single-center | Germany | 299 | 487 | 70 | 44.5 # | 41.9 | 49.2 | 70.0 | 73.6 $ | 60.0 | NA | NA |
| Zhou [13] | 2020 | Observational single-center | China | 89 | 244 | 80 | 55.1 | 59.4 | 64.0 | 62.7 | 75.3 | 64.8 | 36.0 & | 22.1 |
| Kanda [14] | 2019 | Retrospective single-center | Japan | 49 | 241 | 80 | 51.0 | 40 | 100.0 | 100.0 | 63.0 | 56.0 | 14.0 | 16.0 |
| Fink [15] | 2019 | Prospective multicenter | Germany | 108 | 630 | 70 | 38.0 # | 27.6 | 55.6 | 63.0 | NA | NA | 9.3 | 6.3 |
| Zhang-1 [16] | 2019 | Retrospective single-center | China | 127 | 550 | 75 | 55.1 # | 40.5 | 92.9 | 88.2 | 67.2 $ | 59.8 | 18.1 | 15.1 |
| Heeger [17] | 2019 | Prospective multicenter | Germany | 104 | 104 | 75 | 50.0 | 48.1 | 57.7 | 56.7 | 77.9 | 78.9 | 15.4 | 14.4 |
| Romero [18] | 2019 | Retrospective multicenter | America | 3482 | 82,637 | 80 | 61.0 | 31.1 | NA | NA | 65.7 | 55.3 | 19.6 | 14.9 |
| Abdin [19] | 2019 | Retrospective single-center | Germany | 55 | 183 | 75 | 54.6 # | 34.5 | 31.0 | 40.5 | 85.4 $ | 69.3 | 20.0 & | 8.7 |
| Zhang-2 [20] | 2018 | Retrospective single-center | China | 308 | 360 | 60 | 41.5 # | 21.4 | 71.4 | 75.0 | 55.0 $ | 37.0 | 12.6 | 9.9 |
| Tscholl [21] | 2018 | Retrospective single-center | Germany | 40 | 40 | 75 | 50.0 | 35 | 45.0 | 47.5 | 80.0 | 60.0 | 10.0 | 12.5 |
| Moser [22] | 2017 | Retrospective multicenter | Germany | 227 | 4222 | 75 | 48.0 # | 31.1 | 59.9 | 63.3 | NA | NA | 8.8 | 7.6 |
| Abugattas [23] | 2017 | Retrospective single-center | Belgium | 53 | 106 | 75 | 54.7 | 41.5 | 100.0 | 100.0 | 79.2 $ | 41.3 | 11.3 | 8.7 |
| Kautzner [24] | 2017 | Retrospective single-center | Czech Republic | 394 | 2803 | 70 | 49.0 # | 29.4 | 66.5 | 68.2 | 79.2 $ | 56.7 | 15.7 & | 11.2 |
| Bunch-2 [25] | 2016 | Observational multicenter | America | 46 | 877 | 80 | 58.7 # | 40.2 | 52.2 | 54.7 | 82.6 | 70.0 | 17.4 | 22.1 |
| Lioni [26] | 2014 | Retrospective single-center | Greece | 95 | 221 | 65 | 49.5 | 41.2 | 100.0 | 100.0 | 41.1 | 33.5 | 20.0 & | 6.8 |
| Santangeli [27] | 2012 | Retrospective single-center | America | 103 | 2651 | 80 | 41.0 # | 28.0 | 25.0 | 27.0 | 48.0 $ | 37.0 | 15.0 | 11.0 |
| Hao [28] | 2012 | Retrospective multicenter | America | 1325 | 4622 | 65 | 41.0 # | 23.0 | NA | NA | 68.0 | 57.0 | 21.0 | 16.0 |
| Bunch-1 [29] | 2010 | Retrospective single-center | America | 35 | 717 | 80 | 54.3 | 40.7 | 45.7 | 54.1 | 57.1 | 49.2 | 8.6 | 12.4 |
| Kusumoto [30] | 2009 | Retrospective single-center | America | 61 | 179 | 75 | 39.3 # | 24.1 | 34.0 | 70.9 | NA | NA | NA | NA |
| Bhargava [31] | 2004 | Retrospective single-center | America | 103 | 220 | 60 | 23.3 | 18.2 | 52.4 | 54.5 | 35.0 $ | 20.9 | NA | NA |
| Liu [32] | 2022 | Multicenter single-arm | China | 270 | - | 80 | 42.6 | - | 65.6 | - | 73.7 | - | 29.3 | - |
| Akhtar [33] | 2020 | Single-center single-arm | America | 15 | - | 80 | 40.0 | - | 87.0 | - | 80.0 | - | 20.0 | - |
| Metzner [34] | 2016 | Single-center single-arm | Germany | 94 | - | 75 | 41.5 | - | 58.5 | - | 88.3 | - | 4.3 | - |
| Corrado [35] | 2008 | Single-center single-arm | America | 174 | - | 75 | 36.8 | - | 55.0 | - | 56.0 | - | 13.0 | - |
| First Author | LVEF | CHA2DS2-VASc Score | LAD (mm) | AF History Duration | AADs Usage (Elderly vs. Younger) | |||||||||
| Elderly Group | Younger Group | Elderly Group | Younger Group | Elderly Group | Younger Group | Elderly Group | Younger Group | |||||||
| Natale [10] | 58.2 ± 9.6 | 57.8 ± 9.4 | NA | NA | 42.6 ± 7.8 | 41.9 ± 7.6 | NA | NA | NA | |||||
| Vermeersch [6] | 53.2 ± 9.4 | 54.4 ± 9.0 | NA | NA | 45.8 ± 7.8 | 45.6 ± 7.0 | 45.7 ± 46.2 M | 52.4 ± 61.1 M | NA | |||||
| Sciarra [11] | 58.8 ± 7.2 | 59.3 ± 6.9 | 2.4 ± 0.7 | 1.1 ± 0.9 | 22.9 ± 6.2 cm2 * | 21.8 ± 6.0 cm2 | 62.0 ± 107.1 M ξ | 52.0 ± 105.8 M | Failed ≥2 AADs (higher) | |||||
| Hartl [12] | 56.2 ± 5.9 | 56.8 ± 6.5 | NA | NA | 46.1 ± 7.0 * | 43.5 ± 6.9 | NA | NA | The proportion of AADs at baseline (equal) | |||||
| Zhou [13] | 62.7 ± 5.4 | 63.1 ± 5.7 | 4.3 ± 1.3 | 3.3 ± 1.4 | 41.2 ± 4.8 | 41.5 ± 6.2 | 12.0 (2.5-36.0) M | 24.0 (5.0-48.0) M | NA | |||||
| Kanda [14] | NA | NA | 3.8 ± 0.9 | 2.2 ± 1.4 | 40.0 ± 6.0 | 38.0 ± 6.0 | NA | NA | The proportion of AADs at baseline: Class I (lower), other classes (equal) | |||||
| Fink [15] | NA | NA | NA | NA | NA | NA | NA | NA | NA | |||||
| Zhang-1 [16] | 58.7 ± 9.0 | 61.5 ± 6.5 | 4.8 ± 1.6 | 2.6 ± 1.7 | 41.0 ± 5.3 | 41.3 ± 5.6 | NA | NA | The proportion of AADs at baseline, Class I, I and III (equal) | |||||
| Heeger [17] | NA | NA | 3.8 ± 1.1 | 2.1 ± 1.3 | 44.5 ± 5.6 | 44.5 ± 5.6 | NA | NA | NA | |||||
| Romero [18] | NA | NA | NA | NA | 40.8 ± 5.5 | 40.8 ± 6.6 | 24.6 ± 34.1 M | 21.9 ± 34.6 M | NA | |||||
| Abdin [19] | 51.6 ± 8.3 | 52.5 ± 8.0 | 4.0 ± 1.3 | 2.0 ± 1.3 | 49.2 ± 5.8 | 38.6 ± 6.1 | NA | NA | NA | |||||
| Zhang-2 [20] | 66.3 ± 5.7 | 69.1 ± 8.9 | NA | NA | NA | NA | NA | NA | NA | |||||
| Tscholl [21] | 63.0 (60.0, 66.0) | 65.0 (60.0, 70.0) | 4.0 (4.0, 5.0) | 2.0 (1.0, 3.0) | NA | NA | NA | NA | NA | |||||
| Moser [22] | NA | NA | 3.7 ± 1.0 | 1.7 ± 1.2 | 41.4 ± 7.2 | 40.9 ± 6.6 | NA | NA | NA | |||||
| Abugattas [23] | 59.2 ± 5.2 | 59.9 ± 6.4 | 4.0 ± 1.3 | 1.3 ± 1.2 | 42.5 ± 5.4 | 42.3 ± 5.7 | NA | NA | NA | |||||
| Kautzner [24] | 55.8 ± 8.8 | 56.4 ± 7.6 | 3.1 ± 1.3 | 1.5 ± 1.2 | NA | NA | NA | NA | The proportion of AADs at baseline (equal) | |||||
| Bunch-2 [25] | 53.8 ± 13.3 | 52.5 ± 11.4 | NA | NA | 41.2 ± 4.8 | 41.5 ± 6.2 | 12.0 (2.5-36) M | 24.0 (5.0-48.0) M | NA | |||||
| Lioni [26] | 60.0 ± 3.8 | 61.1 ± 4.0 | NA | NA | 42.6 ± 4.5 * | 39.5 ± 4.3 | 5.9 ± 5.1 Y ξ | 4.7 ± 4.4 Y | The proportion of AADs after ablation, Class I and III (equal) | |||||
| Santangeli [27] | 55.0 ± 12.0 | 57.0 ± 9.0 | NA | NA | 46.0 ± 5.0 | 45.0 ± 8.0 | 52.0 (24.0-78.0) M | 58.0 (31.0-96.0) M | Failed AADs (equal) | |||||
| Hao [28] | NA | NA | NA | NA | 24.8 ± 9.1 cm2 | 28.7 ± 9.5 cm2 | NA | NA | NA | |||||
| Bunch-1 [29] | 52.7 ± 13.2 | 51.3 ± 13.1 | NA | NA | NA | NA | NA | NA | NA | |||||
| Kusumoto [30] | NA | NA | NA | NA | 42.6 ± 4.5 | 39.1 ± 4.3 | 5.9 ± 5.1 Y | 4.7 ± 4.4 Y | The proportion of AADs after ablation, Class I and III (equal) | |||||
| Bhargava [31] | 51.4 ± 9.8 | 53.4 ± 7.6 | NA | NA | 43.4 ± 6.5 | 43.3 ± 13.2 | 6.5 ± 3.7 Y | 6.0 ± 4.8 Y | Failed AADs (equal) | |||||
| Liu [32] | 63.7 ± 7.2 | - | 3.9 ± 1.2 | - | 39.9 ± 6.3 | - | 2.9 ± 5.2 Y | - | - | |||||
| Akhtar [33] | 63.7 ± 3.5 | - | 4.2 ± 1.7 | - | 45.0 ± 1.2 | - | 8.9 ± 8.2 Y | - | - | |||||
| Metzner [34] | NA | - | 4.0 ± 1.0 | - | 44.8 ± 6.2 | - | 75.0 M Median | - | - | |||||
| Corrado [35] | 53.0 ± 7.0 | - | NA | - | 46.0 ± 6.0 | - | 7.0 ± 4.0 Y | - | - | |||||
| First Author | Key Points of Ablation Procedure | Ablation Strategy | Ablation Energy | Follow-Up (Months) | ||||||||||
| Natale [10] | Isolation of pulmonary veins, posterior wall and superior vena cava was performed in all patients. Non-pulmonary vein triggers from other areas were ablated based on operator’s discretion | PVI-plus | RF | 48.0 | ||||||||||
| Vermeersch [6] | PVI only | PVI | Cryo | 24.0 (18.4-25.5) | ||||||||||
| Sciarra [11] | PVI only | PVI | Cryo | 12.0 | ||||||||||
| Hartl [12] | PVI with or without additional linear ablation based on decision | PVI-plus | Cryo | 36.0 | ||||||||||
| Zhou [13] | After PVI, additional linear ablation was performed when necessary | PVI-plus | RF | 24.4 ± 9.6 | ||||||||||
| Kanda [14] | PVI with or without additional linear ablation based on decision | PVI-plus | Cryo | 12.0 | ||||||||||
| Fink [15] | PVI first, and then additional ablation strategies including the creation of right atrial and left atrial linear lesions including block of the cavo-tricuspid isthmus, or ablation of complex fractionated atrial electrograms were at the discretion of the operator | PVI-plus | RF | 14.9 | ||||||||||
| Zhang-1 [16] | PVI only | PVI | Cryo | 12.0 | ||||||||||
| Heeger [17] | PVI only | PVI | Cryo | 36.0 | ||||||||||
| Romero [18] | NA | NA | NA | NA | ||||||||||
| Abdin [19] | PVI only | PVI | Cryo | 11.8 ± 5.4 | ||||||||||
| Zhang-2 [20] | PVI with linear ablation | PVI-plus | RF | 6.0 | ||||||||||
| Tscholl [21] | PVI only | PVI | Cryo | 12.0 (6.0, 18.0) | ||||||||||
| Moser [22] | PVI first, and then ablation of fragmented signals and/or lines in the left atrial (mitral isthmus line, roof line, anterior line) were performed in order to achieve termination to sinus rhythm | PVI-plus | RF | 15.3 | ||||||||||
| Abugattas [23] | PVI only | PVI | Cryo | 12.0 | ||||||||||
| Kautzner [24] | All patients underwent PVI first, and then additional left atrial linear lesions, coronary sinus ablation, or electrogram-guided ablations were performed empirically according to the clinical presentation and inducibility of the arrhythmia during the procedure | PVI-plus | RF | 18.0-21.0 | ||||||||||
| Bunch-2 [25] | All patients underwent PVI first, and then additional ablation beyond PVI was performed based upon individual operator choice | PVI-plus | RF | 60.0 | ||||||||||
| Lioni [26] | PVI only | PVI | RF | 34.0 ± 15.1 | ||||||||||
| Santangeli [27] | Isolation of all the pulmonary vein antra and the posterior wall contained between the pulmonary veins first; then the ablation catheter was positioned at right atrium-superior vena cava junction, where mapping and ablation was performed. | PVI-plus | RF | 18.0 ± 6.0 | ||||||||||
| Hao [28] | NA | NA | RF | 1.0 W | ||||||||||
| Bunch-1 [29] | PVI with or without additional linear ablation based on decision | PVI-plus | RF | 12.0 | ||||||||||
| Kusumoto [30] | PVI with linear ablations (not routinely performed) | PVI-plus | RF | 12.0 | ||||||||||
| Bhargava [31] | PVI only | PVI | RF | 14.7 ± 5.2 | ||||||||||
| Liu [32] | PVI with or without additional linear ablation based on decision | PVI-plus | RF | 12.0 | ||||||||||
| Akhtar [33] | PVI first, then additional cavo-tricuspid isthmus ablation based on the discretion of the operator | PVI-plus | Cryo | 12.0 | ||||||||||
| Metzner [34] | Circumferential PVI was performed in all patients, then ablation of complex fractionated atrial electrograms and/or linear lesions were performed based on decision | PVI-plus | RF | 37.0 ± 20.0 | ||||||||||
| Corrado [35] | PVI and superior vena isolation | PVI-plus | RF | 20.0 ± 14.0 | ||||||||||
| Subgroup Factors | Numbers in Study | Pooled Incidence | 95% CI | I2 (%) | p for Interaction |
|---|---|---|---|---|---|
| Study design | 0.893 | ||||
| Multicenter | 7 | 0.68 | 0.54–0.81 | 95.74 | |
| Single-center | 18 | 0.69 | 0.63–0.76 | 89.38 | |
| Publication date | 0.189 | ||||
| recently | 7 | 0.63 | 0.51–0.74 | 93.52 | |
| not recently | 18 | 0.72 | 0.65–0.78 | 91.20 | |
| Elderly age cutoff (years) | 0.911 | ||||
| ≥75 | 18 | 0.69 | 0.60–0.78 | 93.54 | |
| <75 | 7 | 0.69 | 0.61–0.76 | 89.64 | |
| Elderly group sample size | 0.264 | ||||
| ≥100 | 13 | 0.72 | 0.65–0.79 | 94.17 | |
| <100 | 12 | 0.65 | 0.55–0.75 | 87.76 | |
| AF type | 0.484 | ||||
| PAF | 3 | 0.75 | 0.56-0.91 | - | |
| non-PAF | 22 | 0.68 | 0.62–0.75 | 93.12 | |
| Ablation strategy | 0.771 | ||||
| PVI-plus | 16 | 0.68 | 0.60–0.76 | 93.85 | |
| PVI | 9 | 0.70 | 0.60–0.80 | 89.60 | |
| Ablation energy | 0.765 | ||||
| RF | 15 | 0.68 | 0.60–0.76 | 93.88 | |
| Cryo | 10 | 0.71 | 0.60–0.80 | 90.15 | |
| Follow-up time (months) | 0.000 | ||||
| ≥24 | 8 | 0.53 | 0.43–0.62 | 85.67 | |
| <24 | 17 | 0.76 | 0.71–0.81 | 86.11 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, F.; Zhang, L.; Wu, L.-D.; Zhang, Z.-Y.; Liu, H.-H.; Zhang, Z.-Y.; Zhang, J.; Qian, L.-L.; Wang, R.-X. Do Elderly Patients with Atrial Fibrillation Have Comparable Ablation Outcomes Compared to Younger Ones? Evidence from Pooled Clinical Studies. J. Clin. Med. 2022, 11, 4468. https://doi.org/10.3390/jcm11154468
Li F, Zhang L, Wu L-D, Zhang Z-Y, Liu H-H, Zhang Z-Y, Zhang J, Qian L-L, Wang R-X. Do Elderly Patients with Atrial Fibrillation Have Comparable Ablation Outcomes Compared to Younger Ones? Evidence from Pooled Clinical Studies. Journal of Clinical Medicine. 2022; 11(15):4468. https://doi.org/10.3390/jcm11154468
Chicago/Turabian StyleLi, Feng, Lei Zhang, Li-Da Wu, Zhi-Yuan Zhang, Huan-Huan Liu, Zhen-Ye Zhang, Jie Zhang, Ling-Ling Qian, and Ru-Xing Wang. 2022. "Do Elderly Patients with Atrial Fibrillation Have Comparable Ablation Outcomes Compared to Younger Ones? Evidence from Pooled Clinical Studies" Journal of Clinical Medicine 11, no. 15: 4468. https://doi.org/10.3390/jcm11154468
APA StyleLi, F., Zhang, L., Wu, L.-D., Zhang, Z.-Y., Liu, H.-H., Zhang, Z.-Y., Zhang, J., Qian, L.-L., & Wang, R.-X. (2022). Do Elderly Patients with Atrial Fibrillation Have Comparable Ablation Outcomes Compared to Younger Ones? Evidence from Pooled Clinical Studies. Journal of Clinical Medicine, 11(15), 4468. https://doi.org/10.3390/jcm11154468