
An Artificial Neural Network Model for the Prediction of Perioperative Blood Transfusion in Adult Spinal Deformity Surgery

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Patient Selection
2.2. Collected Parameters
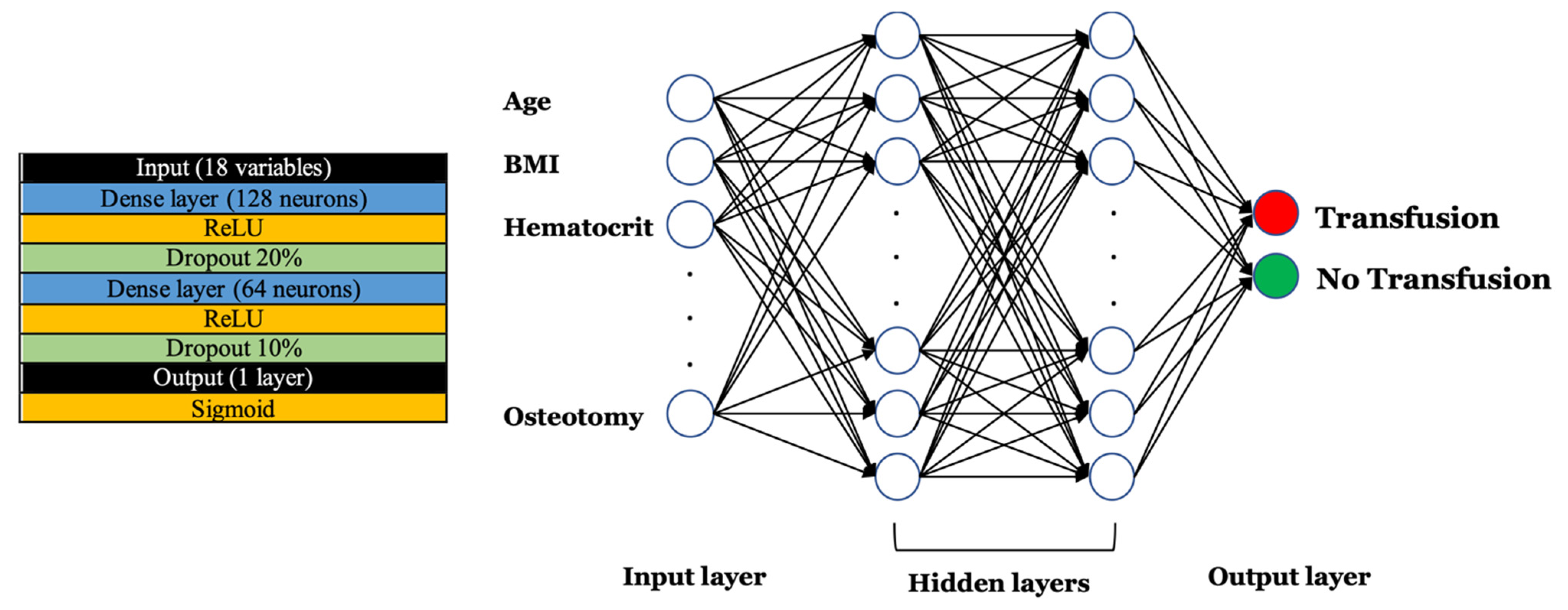
2.3. Model Creation
2.4. Data Analysis and Model Creation
3. Results
3.1. Patient Population
3.2. ANN Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sciubba, D.M.; Yurter, A.; Smith, J.S.; Kelly, M.P.; Scheer, J.K.; Goodwin, C.R.; Lafage, V.; Hart, R.A.; Bess, S.; Kebaish, K.; et al. A Comprehensive Review of Complication Rates after Surgery for Adult Deformity: A Reference for Informed Consent. Spine Deform. 2015, 3, 575–594. [Google Scholar] [CrossRef] [PubMed]
- Durand, W.M.; DePasse, J.M.; Daniels, A.H. Predictive Modeling for Blood Transfusion after Adult Spinal Deformity Surgery: A Tree-Based Machine Learning Approach. Spine 2018, 43, 1058–1066. [Google Scholar] [CrossRef] [PubMed]
- Raman, T.; Vasquez-Montes, D.; Varlotta, C.; Passias, P.G.; Errico, T.J. Decision Tree-based Modelling for Identification of Predictors of Blood Loss and Transfusion Requirement after Adult Spinal Deformity Surgery. Int. J. Spine Surg. 2020, 14, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.J.; Kothari, P.; Kim, J.S.; Shin, J.I.; Phan, K.; Di Capua, J.; Somani, S.; Leven, D.M.; Guzman, J.Z.; Cho, S.K. Early Complications and Outcomes in Adult Spinal Deformity Surgery: An NSQIP Study Based on 5803 Patients. Glob. Spine J. 2017, 7, 432–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puvanesarajah, V.; Rao, S.S.; Hassanzadeh, H.; Kebaish, K.M. Determinants of perioperative transfusion risk in patients with adult spinal deformity. J. Neurosurg. Spine 2018, 28, 429–435. [Google Scholar] [CrossRef]
- Triulzi, D.J.; Vanek, K.; Ryan, D.H.; Blumberg, N. A clinical and immunologic study of blood transfusion and postoperative bacterial infection in spinal surgery. Transfusion 1992, 32, 517–524. [Google Scholar] [CrossRef]
- Kato, S.; Chikuda, H.; Ohya, J.; Oichi, T.; Matsui, H.; Fushimi, K.; Takeshita, K.; Tanaka, S.; Yasunaga, H. Risk of infectious complications associated with blood transfusion in elective spinal surgery—A propensity score matched analysis. Spine J. 2016, 16, 55–60. [Google Scholar] [CrossRef]
- Aoude, A.; Nooh, A.; Fortin, M.; Aldebeyan, S.; Jarzem, P.; Ouellet, J.; Weber, M.H. Incidence, Predictors, and Postoperative Complications of Blood Transfusion in Thoracic and Lumbar Fusion Surgery: An Analysis of 13,695 Patients from the American College of Surgeons National Surgical Quality Improvement Program Database. Glob. Spine J. 2016, 6, 756–764. [Google Scholar] [CrossRef] [Green Version]
- Veeravagu, A.; Patil, C.G.; Lad, S.P.; Boakye, M. Risk factors for postoperative spinal wound infections after spinal decompression and fusion surgeries. Spine 2009, 34, 1869–1872. [Google Scholar] [CrossRef] [Green Version]
- Mikhail, C.; Pennington, Z.; Arnold, P.M.; Brodke, D.S.; Chapman, J.R.; Chutkan, N.; Daubs, M.D.; DeVine, J.G.; Fehlings, M.G.; Gelb, D.E.; et al. Minimizing Blood Loss in Spine Surgery. Glob. Spine J. 2020, 10, 71S–83S. [Google Scholar] [CrossRef]
- Porche, K.; Maciel, C.B.; Lucke-Wold, B.; Robicsek, S.A.; Chalouhi, N.; Brennan, M.; Busl, K.M. Preoperative prediction of postoperative urinary retention in lumbar surgery: A comparison of regression to multilayer neural network. J. Neurosurg. Spine 2022, 36, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Ryu, H.; Kim, S.W.; Oh, J.K.; Kim, T.H. Prediction of Recurrence in Pyogenic Vertebral Osteomyelitis by Artificial Neural Network Using Time-series Data of C-Reactive Protein: A Retrospective Cohort Study of 704 Patients. Spine 2021, 46, 1207–1217. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, J.M.; Evans, S.R.; McCarthy, L.; Temperley, H.; Waters, C.; Ahern, D.; Cunniffe, G.; Morris, S.; Synnott, K.; Birch, N.; et al. The diagnostic and prognostic value of artificial intelligence and artificial neural networks in spinal surgery: A narrative review. Bone Jt. J. 2021, 103, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Durand, W.M.; Lafage, R.; Hamilton, D.K.; Passias, P.G.; Kim, H.J.; Protopsaltis, T.; Lafage, V.; Smith, J.S.; Shaffrey, C.; Gupta, M.; et al. Artificial intelligence clustering of adult spinal deformity sagittal plane morphology predicts surgical characteristics, alignment, and outcomes. Eur. Spine J. 2021, 30, 2157–2166. [Google Scholar] [CrossRef]
- Shiloach, M.; Frencher, S.K., Jr.; Steeger, J.E.; Rowell, K.S.; Bartzokis, K.; Tomeh, M.G.; Richards, K.E.; Ko, C.Y.; Hall, B.L. Toward robust information: Data quality and inter-rater reliability in the American College of Surgeons National Surgical Quality Improvement Program. J. Am. Coll. Surg. 2010, 210, 6–16. [Google Scholar] [CrossRef]
- Luo, W.; Phung, D.; Tran, T.; Gupta, S.; Rana, S.; Karmakar, C.; Shilton, A.; Yearwood, J.; Dimitrova, N.; Ho, T.B.; et al. Guidelines for Developing and Reporting Machine Learning Predictive Models in Biomedical Research: A Multidisciplinary View. J. Med. Internet Res. 2016, 18, e323. [Google Scholar] [CrossRef] [Green Version]
- White, S.J.W.; Cheung, Z.B.; Ye, I.; Phan, K.; Xu, J.; Dowdell, J.; Kim, J.S.; Cho, S.K. Risk Factors for Perioperative Blood Transfusions in Adult Spinal Deformity Surgery. World Neurosurg. 2018, 115, e731–e737. [Google Scholar] [CrossRef]
- Hu, S.S. Blood loss in adult spinal surgery. Eur. Spine J. 2004, 13 (Suppl. 1), S3–S5. [Google Scholar] [CrossRef] [Green Version]
- De la Garza Ramos, R.; Gelfand, Y.; Benton, J.A.; Longo, M.; Echt, M.; Yanamadala, V.; Yassari, R. Rates, Risk Factors, and Complications of Red Blood Cell Transfusion in Metastatic Spinal Tumor Surgery: An Analysis of a Prospective Multicenter Surgical Database. World Neurosurg. 2020, 139, e308–e315. [Google Scholar] [CrossRef]
- Kurra, S.; DeMercurio, P.; Lavelle, W.J.; Lavelle, W.F.; Tallarico, R.A.; Sun, M.H.; Gorji, R.; Li, F. Impact of liberal intraoperative allogeneic blood transfusion on postoperative morbidity and mortality in major thoracic and lumbar posterior spine instrumentation surgeries. Spine Deform. 2021, 10, 573–579. [Google Scholar] [CrossRef]
- Lee, N.J.; Shin, J.I.; Kothari, P.; Kim, J.S.; Leven, D.M.; Steinberger, J.; Guzman, J.Z.; Skovrlj, B.; Caridi, J.M.; Cho, S.K. Incidence, Impact, and Risk Factors for 30-Day Wound Complications Following Elective Adult Spinal Deformity Surgery. Glob. Spine J. 2017, 7, 417–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisahn, C.; Jeyamohan, S.; Norvell, D.C.; Tubbs, R.S.; Moisi, M.; Chapman, J.R.; Page, J.; Oskouian, R.J. Association between Allogeneic Blood Transfusion and Postoperative Infection in Major Spine Surgery. Clin. Spine Surg. 2017, 30, E988–E992. [Google Scholar] [CrossRef] [PubMed]
- Elsamadicy, A.A.; Adil, S.M.; Charalambous, L.; Drysdale, N.; Koo, A.B.; Lee, M.; Kundishora, A.J.; Camara-Quintana, J.; Kolb, L.; Laurans, M.; et al. Independent Association Between Type of Intraoperative Blood Transfusion and Postoperative Delirium after Complex Spinal Fusion for Adult Deformity Correction. Spine 2020, 45, 268–274. [Google Scholar] [CrossRef]
- Hassan, A. U.S. blood banks are experiencing their biggest shortage in a decade. The New York Times, 25 December 2021.
- Lobo, J.M.; Jiménez-Valverde, A.; Real, R. AUC: A misleading measure of the performance of predictive distribution models. Glob. Ecol. Biogeogr. 2008, 17, 145–151. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Value |
|---|---|
| Age (mean, standard deviation) | 55.7 (18.9) |
| Sex | |
| Male | 435 (37.1%) |
| Female | 738 (62.9%) |
| ASA Class | |
| 1 | 56 (4.8%) |
| 2 | 420 (35.8%) |
| 3 | 666 (56.8%) |
| 4 | 31 (2.6%) |
| Smoker | 175 (14.9%) |
| Chronic steroid use | 56 (4.8%) |
| Bleeding disorder | 35 (3.0%) |
| Dependent functional status | 62 (5.3%) |
| Body weight (mean kg, standard deviation) | 77.8 (20.9) |
| Preoperative hematocrit (mean, standard deviation) | 40.6 (4.5) |
| Orthopedic surgeon as attending | 617 (52.6%) |
| Surgery duration (mean hours, standard deviation) | 5.8 (2.7) |
| Pelvic fixation | 250 (21.3%) |
| Interbody graft | 254 (21.7%) |
| Any osteotomy | 345 (29.4%) |
| 3CO | 229 (19.5%) |
| 6–12 posterior levels fused | 263 (22.4%) |
| 13+ posterior levels fused | 240 (20.5%) |
| Revision surgery | 119 (10.1%) |
| Parameter | No Transfusion | Transfusion | p-Value |
|---|---|---|---|
| Age (mean, standard deviation) | 54.1 (19.2) | 57.2 (18.6) | 0.005 * |
| Sex | |||
| Male | 231 (39.4%) | 204 (34.8%) | 0.107 |
| Female | 356 (60.6%) | 382 (65.2%) | |
| ASA Class | |||
| 1 | 38 (6.5%) | 18 (3.1%) | <0.001 * |
| 2 | 244 (41.6%) | 176 (30.0%) | |
| 3 | 294 (50.1%) | 372 (63.5%) | |
| 4 | 11 (1.9%) | 20 (3.4%) | |
| Smoker | 102 (17.4%) | 73 (12.5%) | 0.018 * |
| Chronic steroid use | 23 (3.9%) | 33 (5.6%) | 0.169 |
| Bleeding disorder | 12 (2.0%) | 23 (3.9%) | 0.058 |
| Dependent functional status | 15 (2.6%) | 47 (8.0%) | <0.001 * |
| Body weight (mean kg, standard deviation) | 79.3 (20.9) | 76.3 (20.9) | 0.016 * |
| Preoperative hematocrit (mean, standard deviation) | 41.2 (4.4) | 39.9 (4.6) | <0.001 * |
| Orthopedic surgeon as attending | 327 (55.7%) | 290 (49.5%) | 0.033 * |
| Surgery duration (mean hours, standard deviation) | 4.4 (2.3) | 7.1 (2.4) | <0.001 * |
| Pelvic fixation | 43 (7.3%) | 207 (35.3%) | <0.001 * |
| Interbody graft | 147 (25.0%) | 107 (18.3%) | 0.005 * |
| Any osteotomy | 114 (19.4%) | 231 (39.4%) | <0.001 * |
| 3CO | 63 (10.7%) | 166 (28.3%) | <0.001 * |
| 6–12 posterior levels fused | 163 (27.8%) | 100 (17.1%) | <0.001* |
| 13+ posterior levels fused | 63 (10.7%) | 177 (30.2%) | <0.001 * |
| Revision surgery | 41 (7.0%) | 78 (13.3%) | <0.001 * |
| Parameter | Model 1 | Model 2 | Model 3 | Model 4 |
|---|---|---|---|---|
| Input features | 18 | 18 | 18 | 18 |
| Hidden layers | 4 | 4 | 2 | 2 |
| Activation function | Sigmoid | ReLU | ReLU | Sigmoid |
| Accuracy metrics | ||||
| Sensitivity | 0.79 | 0.76 | 0.80 | 0.71 |
| Positive predictive value | 0.72 | 0.73 | 0.76 | 0.75 |
| F1-Score | 0.76 | 0.75 | 0.78 | 0.73 |
| Accuracy (ACC) | 0.74 | 0.74 | 0.77 | 0.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De la Garza Ramos, R.; Hamad, M.K.; Ryvlin, J.; Krol, O.; Passias, P.G.; Fourman, M.S.; Shin, J.H.; Yanamadala, V.; Gelfand, Y.; Murthy, S.; et al. An Artificial Neural Network Model for the Prediction of Perioperative Blood Transfusion in Adult Spinal Deformity Surgery. J. Clin. Med. 2022, 11, 4436. https://doi.org/10.3390/jcm11154436
De la Garza Ramos R, Hamad MK, Ryvlin J, Krol O, Passias PG, Fourman MS, Shin JH, Yanamadala V, Gelfand Y, Murthy S, et al. An Artificial Neural Network Model for the Prediction of Perioperative Blood Transfusion in Adult Spinal Deformity Surgery. Journal of Clinical Medicine. 2022; 11(15):4436. https://doi.org/10.3390/jcm11154436
Chicago/Turabian StyleDe la Garza Ramos, Rafael, Mousa K. Hamad, Jessica Ryvlin, Oscar Krol, Peter G. Passias, Mitchell S. Fourman, John H. Shin, Vijay Yanamadala, Yaroslav Gelfand, Saikiran Murthy, and et al. 2022. "An Artificial Neural Network Model for the Prediction of Perioperative Blood Transfusion in Adult Spinal Deformity Surgery" Journal of Clinical Medicine 11, no. 15: 4436. https://doi.org/10.3390/jcm11154436
APA StyleDe la Garza Ramos, R., Hamad, M. K., Ryvlin, J., Krol, O., Passias, P. G., Fourman, M. S., Shin, J. H., Yanamadala, V., Gelfand, Y., Murthy, S., & Yassari, R. (2022). An Artificial Neural Network Model for the Prediction of Perioperative Blood Transfusion in Adult Spinal Deformity Surgery. Journal of Clinical Medicine, 11(15), 4436. https://doi.org/10.3390/jcm11154436