
Influences of Increasing Pedicle Screw Diameter on Widening Vertebral Pedicle Size during Surgery in Spinal Deformities in Children and Adolescents without Higher Risk of Pedicle and Vertebral Breaches



Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Patients
2.2. Outcome Parameters
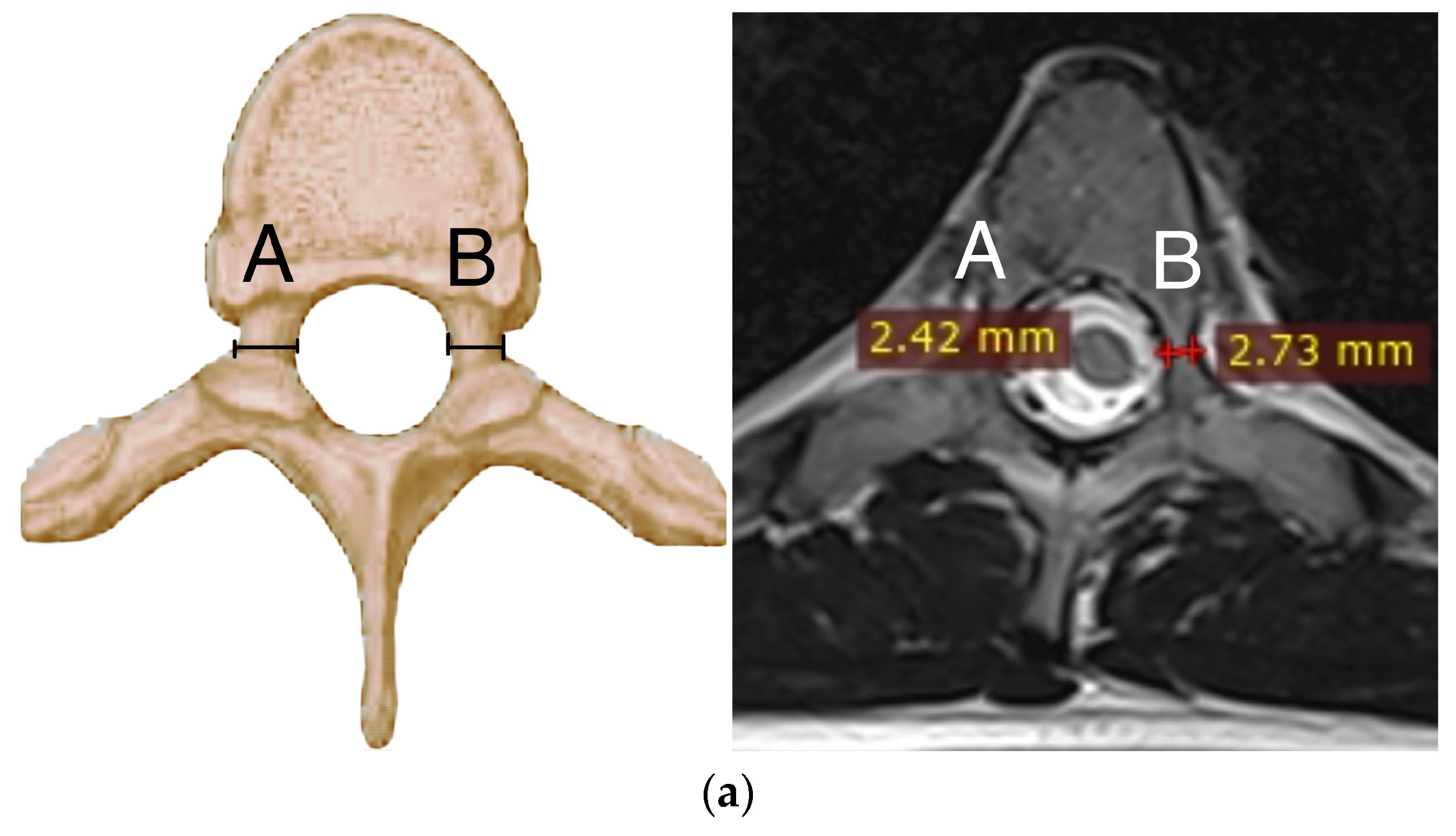
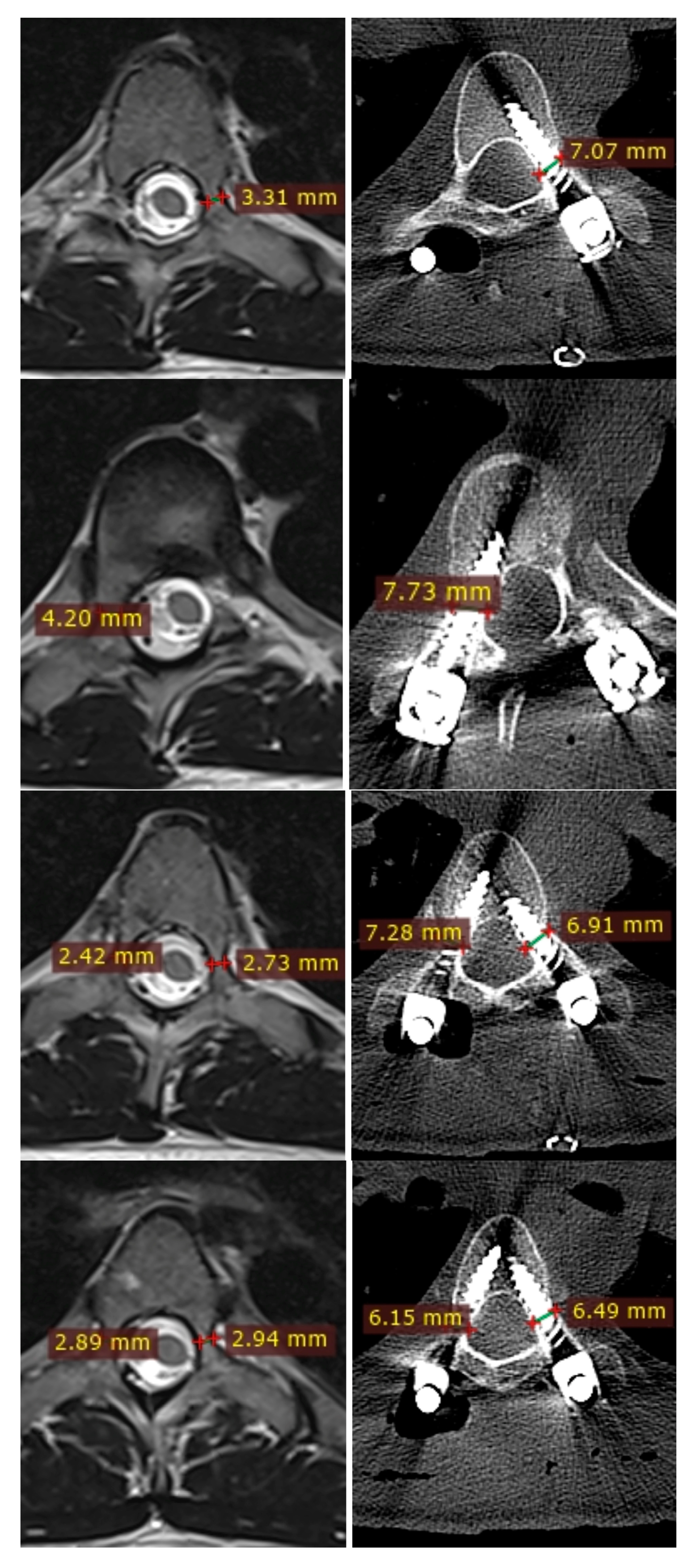
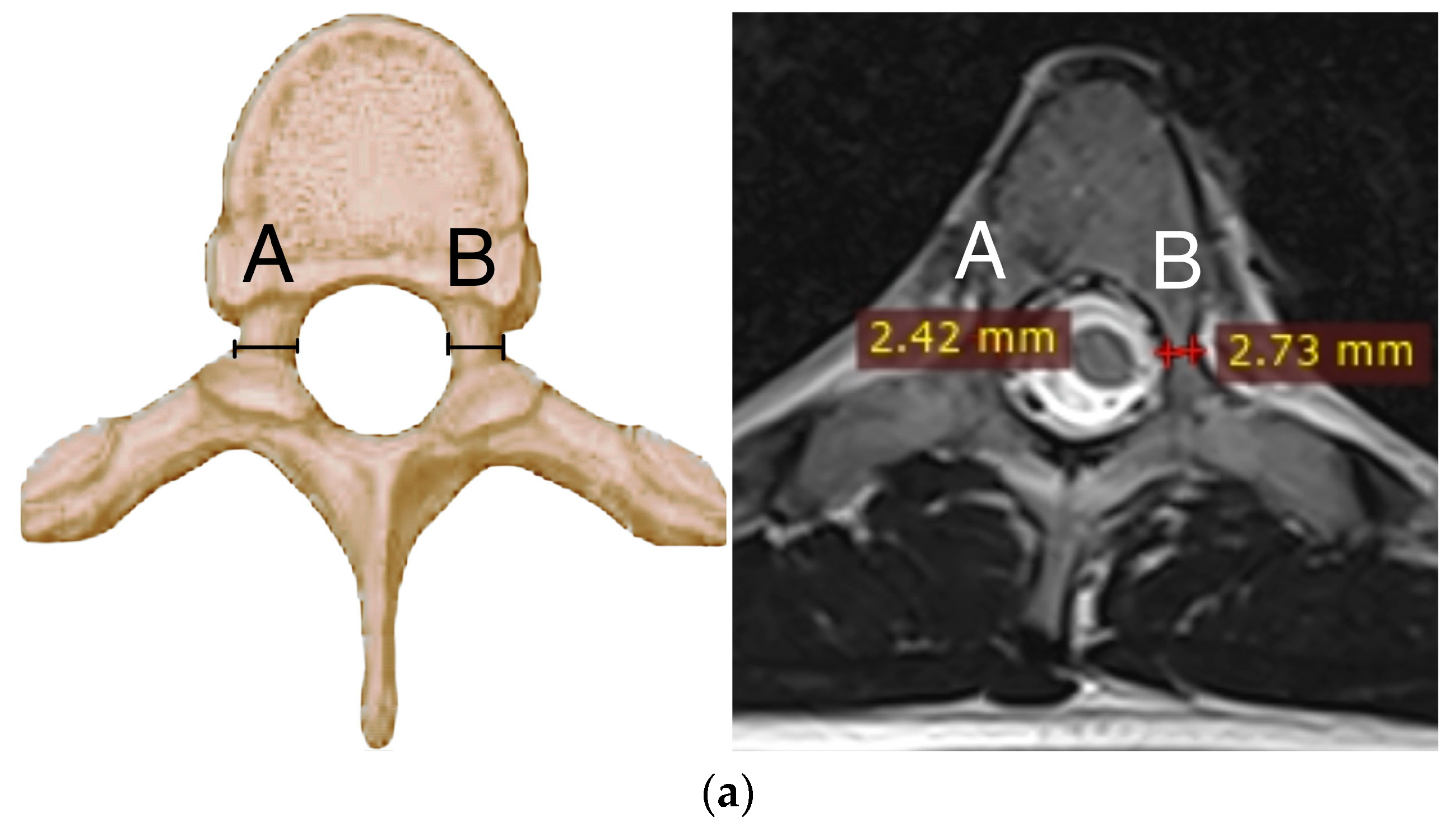
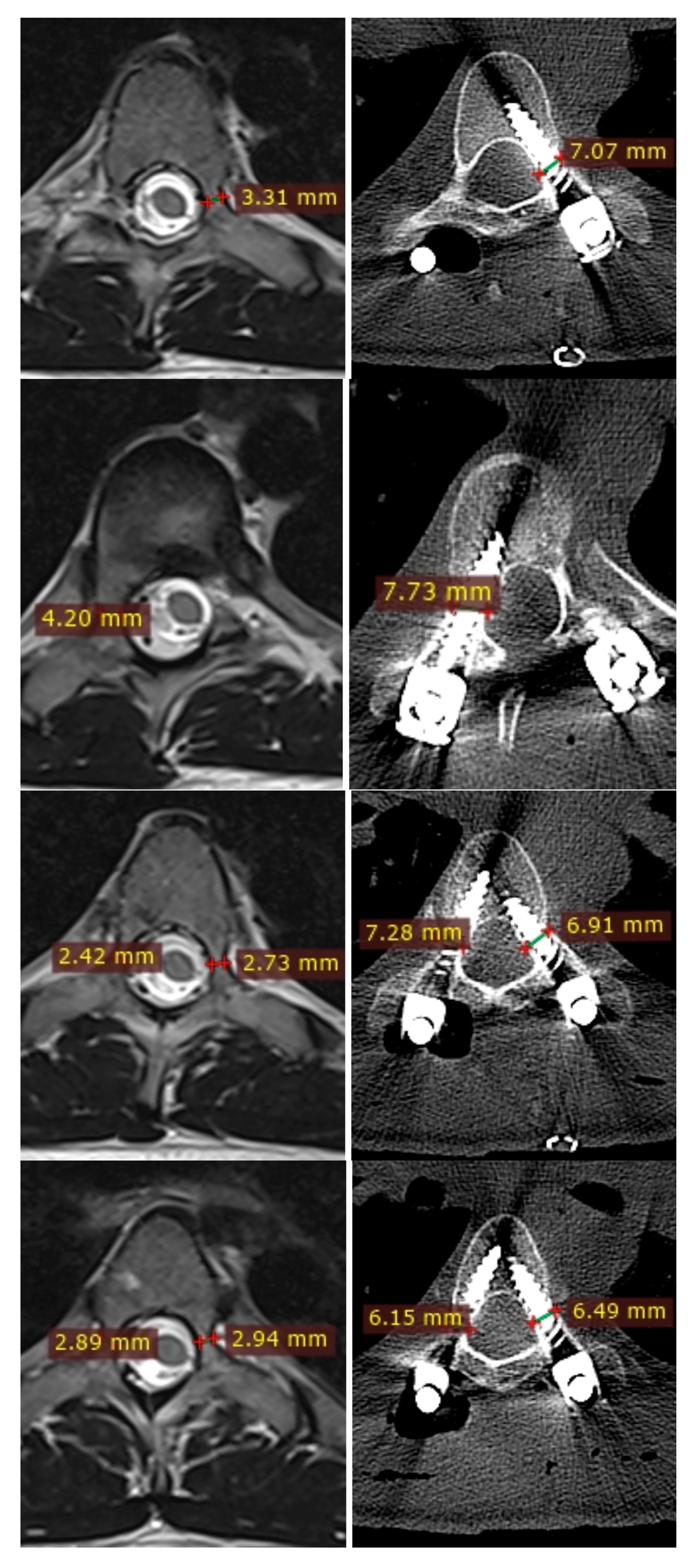
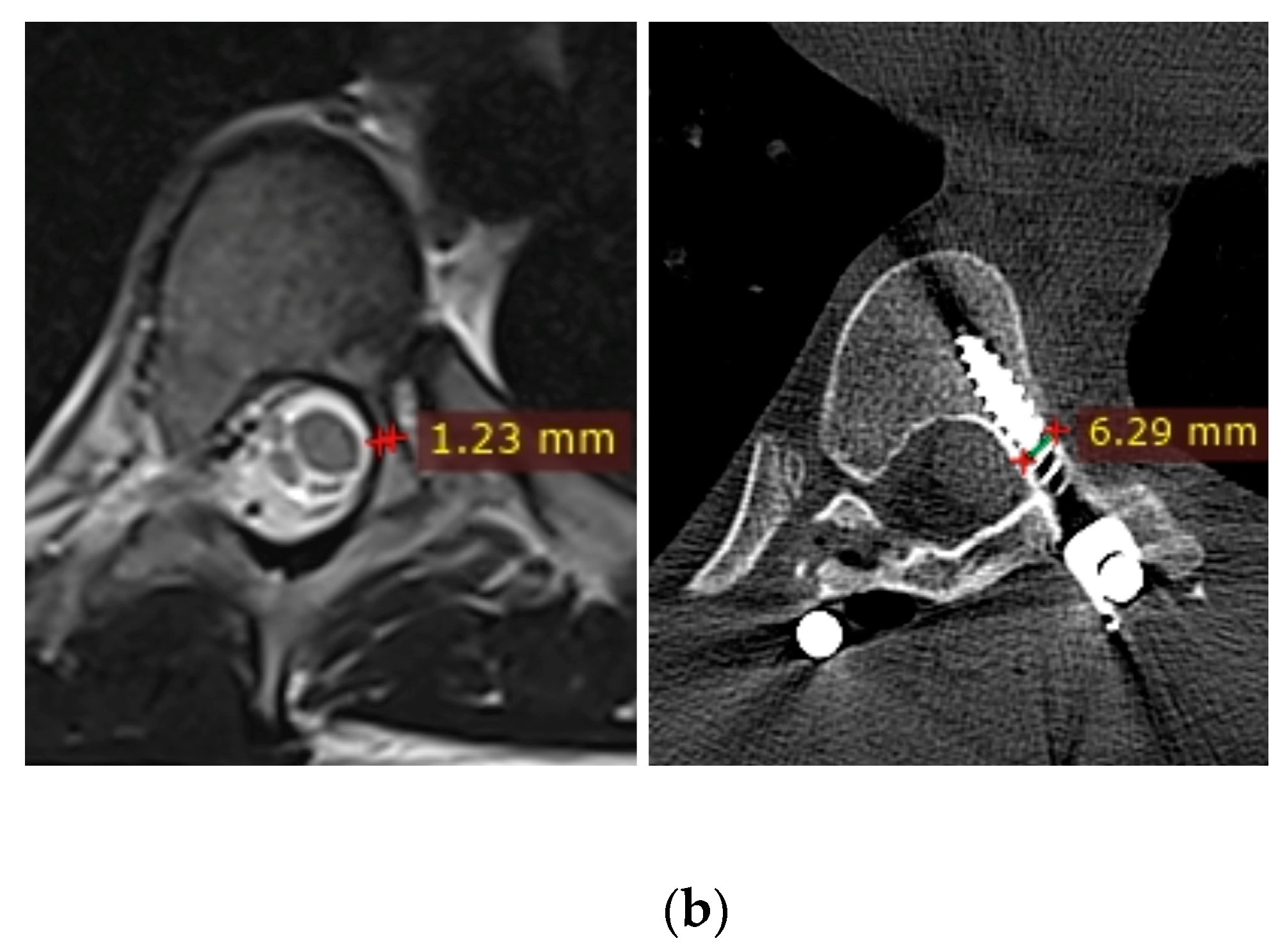
2.3. Radiographic Parameters
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. MRI vs. CT for Evaluating Pedicles and Pedicle Screws
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Suk, S.I.; Kim, W.J.; Lee, S.M.; Kim, J.H.; Chung, E.R. Thoracic pedicle screw fixation in spinal deformities: Are they really safe? Spine 2001, 26, 2049–2057. [Google Scholar] [CrossRef] [PubMed]
- Suk, S.-I.; Kim, J.-H.; Kim, S.-S.; Lim, D.-J. Pedicle screw instrumentation in adolescent idiopathic scoliosis (AIS). Eur. Spine J. 2011, 21, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Lenke, L.G.; Kim, Y.J. Thoracic pedicle screw placement: Free-hand technique. Neurol. India 2005, 53, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Lowenstein, J.E.; Matsumoto, H.; Vitale, M.G.; Weidenbaum, M.; Gomez, J.A.; Lee, F.Y.; Hyman, J.E.; Roye, D.P., Jr. Coronal and sagittal plane correction in adolescent idiopathic scoliosis: A comparison between all pedicle screw versus hybrid thoracic hook lumbar screw constructs. Spine 2007, 32, 448–452. [Google Scholar] [CrossRef]
- Yilmaz, G.; Borkhuu, B.; Dhawale, A.A.; Oto, M.; Littleton, A.G.; Mason, D.E.; Gabos, P.G.; Shah, S.A. Comparative analysis of hook, hybrid, and pedicle screw instrumentation in the posterior treatment of adolescent idiopathic scoliosis. J. Pediatr. Orthop. 2012, 32, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Lamerain, M.; Bachy, M.; Dubory, A.; Kabbaj, R.; Scemama, C.; Vialle, R. All-Pedicle Screw Fixation With 6-mm-Diameter Cobalt-Chromium Rods Provides Optimized Sagittal Correction of Adolescent Idiopathic Scoliosis. Clin. Spine Surg. 2017, 30, E857–E863. [Google Scholar] [CrossRef]
- Kim, Y.J.; Lenke, L.G.; Cho, S.K.; Bridwell, K.H.; Sides, B.; Blanke, K. Comparative analysis of pedicle screw versus hook instrumentation in posterior spinal fusion of adolescent idiopathic scoliosis. Spine 2004, 29, 2040–2048. [Google Scholar] [CrossRef]
- Sarwahi, V.; Hasan, S.; Koutsogiannis, P.; Visahan, K.; Rao, H.; Patil, A.; Lo, Y.; Amaral, T.; Di Mauro, J.P. Effect of Pedicle Screw Size on Surgical Outcomes Following Surgery for Adolescent Idiopathic Scoliosis. Spine 2023. ahead of print. [Google Scholar] [CrossRef]
- Watanabe, K.; Lenke, L.G.; Matsumoto, M.; Harimaya, K.; Kim, Y.J.; Hensley, M.R.; Stobbs, G.R.; Toyama, Y.; Chiba, K. A Novel Pedicle Channel Classification Describing Osseous Anatomy: How many thoracic scoliotic pedicles have cancellous channels? Spine 2010, 35, 1836–1842. [Google Scholar] [CrossRef]
- Ledonio, C.G.; Polly, D.W., Jr.; Vitale, M.G.; Wang, Q. Pediatric pedicle screws: Comparative effectiveness and safety: A systematic literature review from the Scoliosis Research Society and the Pediatric Orthopaedic Society of North America task force. J. Bone Jt. Surg. Am. 2011, 93, 1227–1234. [Google Scholar] [CrossRef]
- Kuklo, T.R.; Lenke, L.G.; O’brien, M.F.; Lehman, R.A., Jr.; Polly, D.W., Jr.; Schroeder, T.M. Accuracy and Efficacy of Thoracic Pedicle Screws in Curves More Than 90°. Spine 2005, 30, 222–226. [Google Scholar] [CrossRef]
- Lehman, R.A., Jr.; Lenke, L.G.; Keeler, K.A.; Kim, Y.J.; Cheh, G. Computed tomography evaluation of pedicle screw placed in the pediatric deformed spine over an 8-year period. Spine 2007, 32, 2679–2684. [Google Scholar] [CrossRef] [PubMed]
- Grabala, P.; Helenius, I.J.; Kowalski, P.; Grabala, M.; Zacha, S.; Deszczynski, J.M.; Albrewczynski, T.; Galgano, M.A.; Buchowski, J.M.; Chamberlin, K.; et al. The Child’s Age and the Size of the Curvature Do Not Affect the Accuracy of Screw Placement with the Free-Hand Technique in Spinal Deformities in Children and Adolescents. J. Clin. Med. 2023, 12, 3954. [Google Scholar] [CrossRef]
- Catan, H.; Buluç, L.; Anik, Y.; Ayyildiz, E.; Sarlak, A.Y. Pedicle morphology of the thoracic spine in preadolescent idiopathic scoliosis: Magnetic resonance supported analysis. Eur. Spine J. 2007, 16, 1203–1208. [Google Scholar] [CrossRef] [PubMed]
- Duchaussoy, T.; Lacoste, M.; Norberciak, L.; Decaudain, J.; Verclytte, S.; Budzik, J.F. Preoperative assessment of idiopathic scoliosis in adolescent and young adult with three-dimensional T2-weighted spin-echo MRI. Diagn. Interv. Imaging 2019, 100, 371–379. [Google Scholar] [CrossRef]
- Sawakami, K.; Yamazaki, A.; Ishikawa, S.; Ito, T.; Watanabe, K.; Endo, N. Polymethylmethacrylate augmentation of pedicle screws increases the initial fixa- tion in osteoporotic spine patients. J. Spinal Disord. Tech. 2012, 25, E28–E35. [Google Scholar] [CrossRef]
- Zhan, X.; Zhan, X.; Yu, J.; Moore, G.; Li, F.; Xi, X.; Zeng, Z.; Yin, S.; Yu, Y.; Cheng, L. Correlation between direction of pedicle screw and restoration of lumbar degenerative scoliosis in degenerative lumbar spondylolisthesis: A retrospective study. Quant. Imaging Med. Surg. 2023, 13, 1740–1752. [Google Scholar] [CrossRef]
- Lai, D.M.; Shih, Y.T.; Chen, Y.H.; Chien, A.; Wang, J.L. Effect of pedicle screw diameter on screw fixation efficacy in human osteoporotic thoracic vertebrae. J. Biomech. 2018, 70, 196–203. [Google Scholar] [CrossRef]
- Matsukawa, K.; Yato, Y.; Imabayashi, H. Impact of Screw Diameter and Length on Pedicle Screw Fixation Strength in Osteoporotic Vertebrae: A Finite Element Analysis. Asian Spine J. 2021, 15, 566–574. [Google Scholar] [CrossRef]
- Oda, K.; Ohba, T.; Hiroshi, Y.; Fujita, K.; Tanaka, N.; Koyma, K.; Haro, H. Factors Affecting Pedicle Screw Insertional Torque in Spine Deformity Surgery. Spine 2021, 46, E932–E938. [Google Scholar] [CrossRef]
- Inceoglu, S.; Ferrara, L.; McLain, R.F. Pedicle screw fixation strength: Pullout versus insertional torque. Spine J. 2004, 4, 513–518. [Google Scholar] [CrossRef]
- Cho, W.; Cho, S.K.; Wu, C. The biomechanics of pedicle screw-based instrumentation. J. Bone Jt. Surg. Br. 2010, 92, 1061–1065. [Google Scholar] [CrossRef]
- Kwok, A.W.; Finkelstein, J.A.; Woodside, T.; Hearn, T.C.; Hu, R.W. Insertional torque and pull-out strengths of conical and cylindrical pedicle screws in cadaveric bone. Spine 1996, 21, 2429–2434. [Google Scholar] [CrossRef]
- Vora, V.; Crawford, A.; Babekhir, N.; Boachie-Adjei, O.; Lenke, L.; Peskin, M.; Charles, G.; Kim, Y. A pedicle screw construct gives an enhanced posterior correction of adolescent idiopathic scoliosis when compared with other constructs: Myth or reality. Spine 2007, 32, 1869–1874. [Google Scholar] [CrossRef]
- Kothe, R.; O’Holleran, J.D.; Liu, W.; Panjabi, M.M. Internal architecture of the thoracic pedicle. An anatomic study. Spine 1996, 21, 264–270. [Google Scholar] [CrossRef]
- Rinella, A.S.; Cahill, P.; Ghanayem, A. Thoracic pedicle expansion after pedicle screw placement in a pediatric cadaveric spine. In Proceedings of the Podium presentation: Scoliosis Research Society (SRS) 2004 Annual Meeting, Buenos Aires, Argentina, 6 September 2004. [Google Scholar]
- Cho, S.K.; Skovrlj, B.; Lu, Y.; Caridi, J.M.; Lenke, L.G. The effect of increasing pedicle screw size on thoracic spinal canal dimensions: An anatomic study. Spine 2014, 39, E1195–E1200. [Google Scholar] [CrossRef]
- Yazici, M.; Pekmezci, M.; Cil, A.; Alanay, A.; Acaroglu, E.; Oner, F.C. The effect of pedicle expansion on pedicle morphology and biomechanical stability in the immature porcine spine. Spine 2006, 31, E826–E829. [Google Scholar] [CrossRef]
- Yilmaz, G.; Demirkiran, G.; Ozkan, C.; Daglioglu, K.; Pekmezci, M.; Alanay, A.; Yazici, M. The effect of dilation of immature pedicles on pullout strength of the screws: Part 2: In vivo study. Spine 2009, 34, 2378–2383. [Google Scholar] [CrossRef]
- Grabala, P.; Helenius, I.J.; Chamberlin, K.; Galgano, M. Less-Invasive Approach to Early-Onset Scoliosis-Surgical Technique for Magnetically Controlled Growing Rod (MCGR) Based on Treatment of 2-Year-Old Child with Severe Scoliosis. Children 2023, 10, 555. [Google Scholar] [CrossRef]
- Charalampidis, A.; Jiang, F.; Wilson, J.R.F.; Badhiwala, J.H.; Brodke, D.S.; Fehlings, M.G. The Use of Intraoperative Neurophysiological Monitoring in Spine Surgery. Glob. Spine J. 2020, 10 (Suppl. S1), 104S–114S. [Google Scholar] [CrossRef]
- Besse, M.; Gaume, M.; Eisermann, M.; Kaminska, A.; Glorion, C.; Miladi, L.; Gitiaux, C.; Ferrero, E. Intraoperative neuromonitoring in non-idiopathic pediatric scoliosis operated with minimally fusionless procedure: A series of 290 patients. Arch. Pediatr. 2022, 29, 588–593. [Google Scholar] [CrossRef]
- Dikmen, P.Y.; Halsey, M.F.; Yucekul, A.; de Kleuver, M.; Hey, L.; Newton, P.O.; Havlucu, I.; Zulemyan, T.; Yilgor, C.; Alanay, A. Intraoperative neuromonitoring practice patterns in spinal deformity surgery: A global survey of the Scoliosis Research Society. Spine Deform. 2021, 9, 315–325. [Google Scholar] [CrossRef]
- Kuraishi, S.; Takahashi, J.; Hirabayashi, H.; Hashidate, H.; Ogihara, N.; Mukaiyama, K.; Kato, H. Pedicle morphology using computed tomography-based navigation system in adolescent idiopathic scoliosis. J. Spinal Disord. Tech. 2013, 26, 22–28. [Google Scholar] [CrossRef]
- Lenke, L.G.; Dobbs, M.B. Management of juvenile idiopathic scoliosis. J. Bone Jt. Surg. Am. 2007, 89 (Suppl. S1), 55–63. [Google Scholar] [CrossRef]
- Gertzbein, S.D.; Robbins, S.E. Accuracy of Pedicular Screw Placement In Vivo. Spine 1990, 15, 11–14. [Google Scholar] [CrossRef]
- Choma, T.J.; Denis, F.; Lonstein, J.E.; Perra, J.H.; Schwender, J.D.; Garvey, T.A.; Mullin, W.J. Stepwise Methodology for Plain Radiographic Assessment of Pedicle Screw Placement: A Comparison with Computed Tomography. J. Spinal Disord. Tech. 2006, 19, 547–553. [Google Scholar] [CrossRef]
- Swany, L.; Larson, A.N.; Garg, S.; Hedequist, D.; Newton, P.; Sponseller, P.; Harms Study Group. 0.4% incidence of return to OR due to screw malposition in a large prospective adolescent idiopathic scoliosis database. Spine Deform. 2021, 10, 361–367. [Google Scholar] [CrossRef]
- Wittenberg, R.H.; Lee, K.S.; Shea, M.; White, A.A., III; Hayes, W.C. Effect of screw diameter, insertion technique, and bone cement augmentation of pedicular screw fixation strength. Clin. Orthop. Relat. Res. 1993, 296, 278–287. [Google Scholar] [CrossRef]
- Baghdadi, Y.M.; Larson, A.N.; McIntosh, A.L.; Shaughnessy, W.J.; Dekutoski, M.B.; Stans, A.A. Complications of pedicle screws in children 10 years or younger: A case control study. Spine 2013, 38, E386–E393. [Google Scholar] [CrossRef]
- Hicks, J.; Singla, A.; Arlet, V. Complications of Pedicle Screw Fixation in Scoliosis Surgery: A Systematic Review. Spine J. 2010, 35, E465–E467. [Google Scholar] [CrossRef]
- Kim, Y.J.; Lenke, L.G.; Bridwell, K.H.; Cho, Y.S.; Riew, K.D. Free hand pedicle screw placement in the thoracic spine: Is it safe? Spine 2004, 29, 333–342. [Google Scholar] [CrossRef]
- Liljenqvist, U.R.; Allkemper, T.; Hackenberg, L.; Link, T.; Steinbeck, J.; Halm, H.F. Analysis of vertebral morphology in idiopathic scoliosis with use of magnetic resonance imaging and multiplanar reconstruction. J. Bone Jt. Surg. Am. 2002, 84, 359–368. [Google Scholar] [CrossRef]
- Grabala, P.; Helenius, I.J.; Buchowski, J.M.; Shah, S.A. The Efficacy of a Posterior Approach to Surgical Correction for Neglected Idiopathic Scoliosis: A Comparative Analysis According to Health-Related Quality of Life, Pulmonary Function, Back Pain and Sexual Function. Children 2023, 10, 299. [Google Scholar] [CrossRef]
- Sarwahi, V.; Amaral, T.; Wendolowski, S.; Gecelter, R.; Sugarman, E.; Lo, Y.; Wang, D.; Thornhill, B. MRIs Are Less Accurate Tools for the Most Critically Worrisome Pedicles Compared to CT Scans. Spine Deform. 2016, 4, 400–406. [Google Scholar] [CrossRef]
- Omar Pacha, T.; Omar, M.; Graulich, T.; Suero, E.; Mathis SchrÖder, B.; Krettek, C.; Stubig, T. Comparison of Preoperative Pedicle Screw Measurement Between Computed Tomography and Magnet Resonance Imaging. Int. J. Spine Surg. 2020, 14, 671–680. [Google Scholar] [CrossRef]
- Mitchell, S.L.; Heyer, J.H.; Baldwin, K.D.; Greenhill, D.A.; Flynn, J.M.; Anari, J.B. Preoperative MRI Reliably Predicts Pedicle Dimensions on Intraoperative CT Images in Structural Main Thoracic Curves in Patients with Adolescent Idiopathic Scoliosis. Spine 2022, 47, 1221–1226. [Google Scholar] [CrossRef]
- Sarwahi, V.; Sugarman, E.P.; Wollowick, A.L.; Amaral, T.D.; Lo, Y.; Thornhill, B. Prevalence, distribution, and surgical relevance of abnormal pedicles in spines with adolescent idiopathic scoliosis vs. no deformity: A CT-based study. J. Bone Jt. Surg. Am. 2014, 96, e92. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Group 1 (n = 54) | Group 2 (n = 61) | Group 3 (n = 115) |
|---|---|---|---|
| Age (years, range) Mean (SD) age at surgery | 2–5 4.2 (0.8) | 6–10 7.6 (2.2) | 11–18 13.8 (3.2) |
| p value | p = 0.33 (1 vs. 2) | p = 0.41 (2 vs. 3) | p = 0.27 (1 vs. 3) |
| Sex | |||
| Male | 8 | 11 | 9 |
| Female | 46 | 50 | 106 |
| Etiology: | |||
| Congenital (n) | 8 | 6 | 11 |
| Neuromuscular (n) | 6 | 8 | 9 |
| Syndromic (n) | 5 | 6 | 7 |
| Idiopathic (n) | 35 | 41 | 88 |
| Main curve magnitude (degrees, range) preoperative Mean (SD) values | 70–125 88 (13.2) | 65–128 85 (18.9) | 50–165 81 (29.2) |
| p value | p = 0.13 (1 vs. 2) | p = 0.09 (2 vs. 3) | p = 0.08 (1 vs. 3) |
| Main curve magnitude (degrees, range) postoperative Mean (SD) values | 21–81 35 (18) | 25–67 32 (15) | 5–88 28 (22) |
| p value | p = 0.83 (1 vs. 2) | p = 0.66 (2 vs. 3) | p = 0.78 (1 vs. 3) |
| Thoracic kyphosis (degrees, range) preoperative Mean (SD) values | 21–105 49 (26) | 31–121 52 (28) | 17–154 78 (48) |
| p value | p = 0.69 (1 vs. 2) | p = 0.52 (2 vs. 3) | p = 0.79 (1 vs. 3) |
| Thoracic kyphosis (degrees, range) postoperative Mean (SD) values | 18–72 47 (14) | 26–68 49 (12) | 15–82 36 (17) |
| p value | p = 0.26 (1 vs. 2) | p = 0.29 (2 vs. 3) | p = 0.18 (1 vs. 3) |
| Number of screw placements | 689 | 1251 | 3140 |
| Blood loss (range, cc) Mean (SD) values | 120–620 282 (148) | 90–820 547 (328) | 280–1800 680 (392) |
| p value | p = 0.88 (1 vs. 2) | p = 0.91 (2 vs. 3) | p = 0.48 (1 vs. 3) |
| Operation time (range, min.) Mean (SD) values | 75–420 212 (68) | 88–880 244 (72) | 152–820 348 (168) |
| p value | p = 0.39 (1 vs. 2) | p = 0.28 (2 vs. 3) | p = 0.53 (1 vs. 3) |
| Pedicle Type | All Pedicles Preop | Group S Postop | Group L Postop | Postop Lateral Breaches (n = 248) | Postop Medial Breaches (n = 170) |
|---|---|---|---|---|---|
| A | 55.2% | 52.8% | 54.1% | 22 (0.43%) | 15 (0.29%) |
| N.A. | p = 0.471 | p = 0.547 | |||
| B | 33.8% | 35.6% | 37.2% | 39 (0.76%) | 22 (0.43%) |
| N.A. | p = 0.377 | p = 0.113 | |||
| C | 4.7% | 3.8% | 4.2% | 89 (1.75%) | 55 (1.08%) |
| N.A. | p = 0.213 | p = 0.08 | |||
| D | 6.3% | 7.8% | 4.5% | 98 (1.92%) | 78 (1.53%) |
| N.A. | p = 0.188 | p = 0.09 | |||
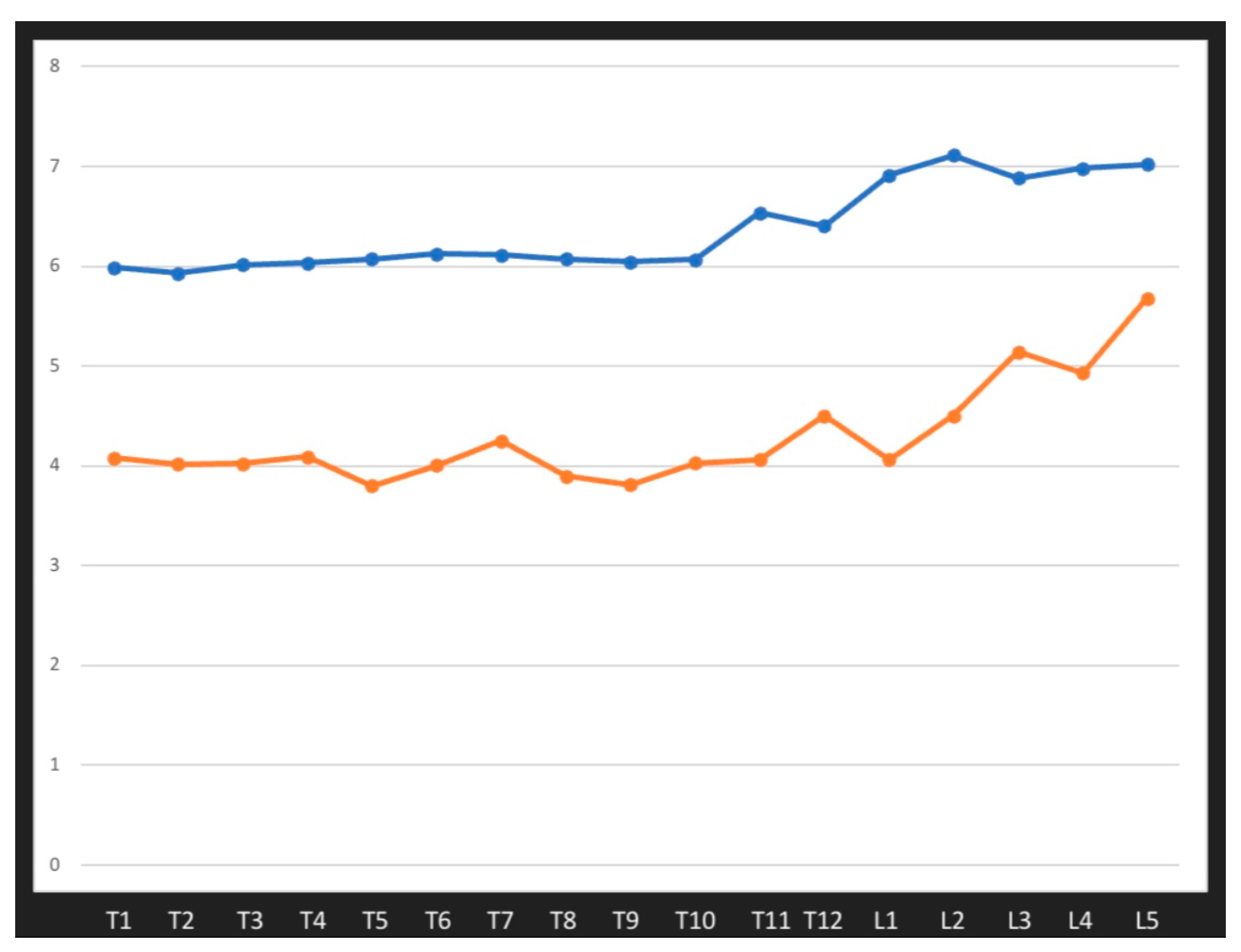
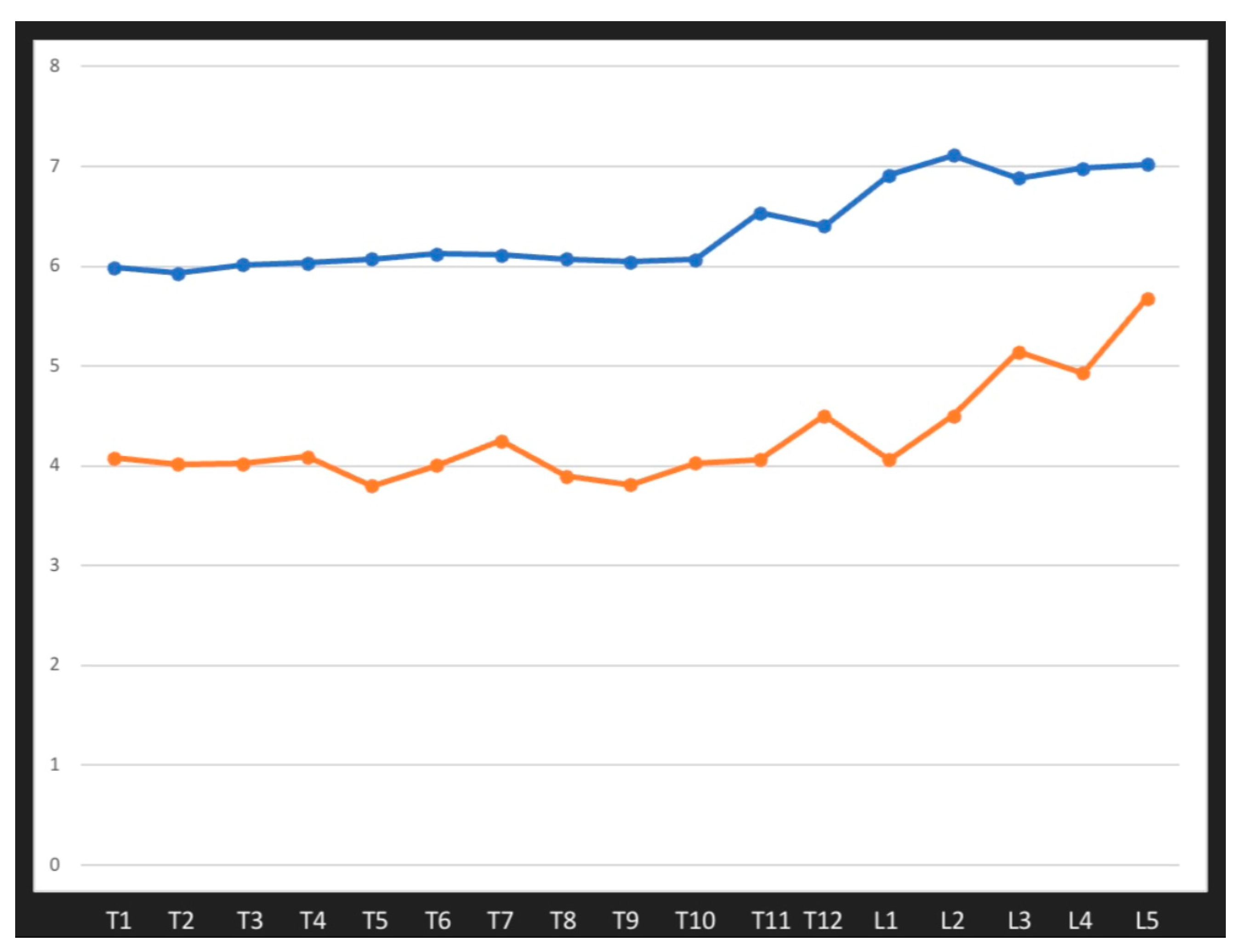
| Levels, Patients n = 234 | Mean Pedicle Preop N = 7956 | Mean Pedicle Postop N = 5080 | Mean Expanding (mm) | Mean Expanding % |
|---|---|---|---|---|
| T1 | 4.07 (0.96) | 5.98 (0.38) | 1.90 (0.32) | 48% (3.4) |
| T2 | 4.01 (1.2) | 5.93 (0.46) | 1.92 (0.39) | 47% (4.1) |
| T3 | 4.02 (1.92) | 6.01 (0.27) | 2.01 (0.26) | 50% (2.7) |
| T4 | 4.09 (1.76) | 6.02 (0.26) | 2.04 (0.28) | 49.5% (2.8) |
| T5 | 3.79 (1.44) | 6.07 (0.23) | 2.55 (0.22) | 68% (2.2) |
| T6 | 4.00 (1.83) | 6.12 (0.43) | 2.44 (0.18) | 61% (2.1) |
| T7 | 4.25 (1.55) | 6.12 (0.44) | 2.18 (0.21) | 52% (2.2) |
| T8 | 3.90 (1.58) | 6.07 (0.36) | 2.11 (0.29) | 54% (3.2) |
| T9 | 3.81 (1.73) | 6.04 (0.36) | 2.51 (0.33) | 66% (3.8) |
| T10 | 4.02 (1.59) | 6.06 (0.38) | 2.21 (0.32) | 55% (3.6) |
| T11 | 4.06 (1.67) | 6.53 (0.37) | 2.53 (0.39) | 62% (3.7) |
| T12 | 4.18 (1.48) | 6.40 (0.45) | 2.39 (0.36) | 57% (3.7) |
| L1 | 4.06 (1.59) | 6.91 (0.22) | 2.88 (0.29) | 71% (3.0) |
| L2 | 4.5 (1.38) | 7.11 (0.33) | 2.67 (0.28) | 59% (2.9) |
| L3 | 5.14 (1.2) | 6.88 (0.38) | 2.89 (0.34) | 56% (3.3) |
| L4 | 4.93 (1.5) | 6.98 (0.24) | 2.92 (0.28) | 59% (2.7) |
| L5 | 5.68 (1.64) | 7.02 (0.34) | 2.68 (0.29) | 47% (3.0) |
| Variable | Group 1 (n = 54) | Group 2 (n = 61) | Group 1 vs. Group 2, p | Group 3 (n = 115) | Group 2 vs. Group 3, p | Group 1 vs. Group 3, p |
|---|---|---|---|---|---|---|
| Mean pedicle expansion% | 49% (2.5) | 52% (3.5) | p = 0.43 | 62% (3.8) | p = 0.12 | p = 0.07 |
| Breaches lat. by age | 61 (1.2%) | 68 (1.33%) | p = 0.82 | 119 (2.34%) | p = 0.92 | p = 0.03 |
| Breaches med. by age | 52 (1.02%) | 47 (0.92%) | p = 0.79 | 71 (1.4%) | p = 0.79 | p = 0.12 |
| Level (n = 5080 Inserted Screws) | Mean Pedicle Expansion Postop (%) Group S | Postop Breaches (Medial/Lateral) Group S | Mean Pedicle Expansion Postop (%) Group L | Postop Breaches (Medial/Lateral) Group L | Expansion L. vs. S, p | Breaches L vs. S, p |
|---|---|---|---|---|---|---|
| T1 | 34% (2.8) | 3/8 | 50% (2.8) | 3/8 | p = 0.031 | N. S. |
| T2 | 36% (3.2) | 2/7 | 49% (3.4) | 3/7 | p = 0.038 | N. S. |
| T3 | 40% (2.8) | 3/9 | 52% (3.2) | 4/9 | p = 0.042 | N. S. |
| T4 | 36% (3.1) | 4/9 | 52.5% (3.2) | 4/10 | p = 0.022 | N. S. |
| T5 | 50% (4.1) | 5/9 | 70% (2.2) | 5/10 | p = 0.001 | N. S. |
| T6 | 42% (3.2) | 4/9 | 61% (2.6) | 6/9 | p = 0.041 | N. S. |
| T7 | 35% (2.8) | 6/10 | 54% (2.6) | 8/12 | p = 0.039 | N. S. |
| T8 | 50% (3.6) | 6/11 | 55% (3.5) | 9/12 | p = 0.039 | N. S. |
| T9 | 52% (2.8) | 5/9 | 67% (3.4) | 9/10 | p = 0.012 | N. S. |
| T10 | 46% (3.2) | 7/8 | 57% (3.8) | 8/9 | p = 0.019 | N. S. |
| T11 | 45% (1.9) | 9/9 | 65% (3.9) | 9/8 | p = 0.011 | N. S. |
| T12 | 39% (4.2) | 4/5 | 59% (3.2) | 6/4 | p = 0.039 | N. S. |
| L1 | 38% (3.8) | 4/6 | 73% (3.4) | 7/7 | p = 0.001 | N. S. |
| L2 | 34% (2.6) | 3/8 | 63% (2.8) | 6/7 | p = 0.001 | N. S. |
| L3 | 37% (3.2) | 3/7 | 59% (3.8) | 8/8 | p = 0.012 | N. S. |
| L4 | 31% (3.2) | 2/1 | 62% (3.8) | 4/1 | p = 0.001 | N. S. |
| L5 | 29% (2.8) | 1/1 | 49% (3.8) | 1/1 | p = 0.031 | N. S. |
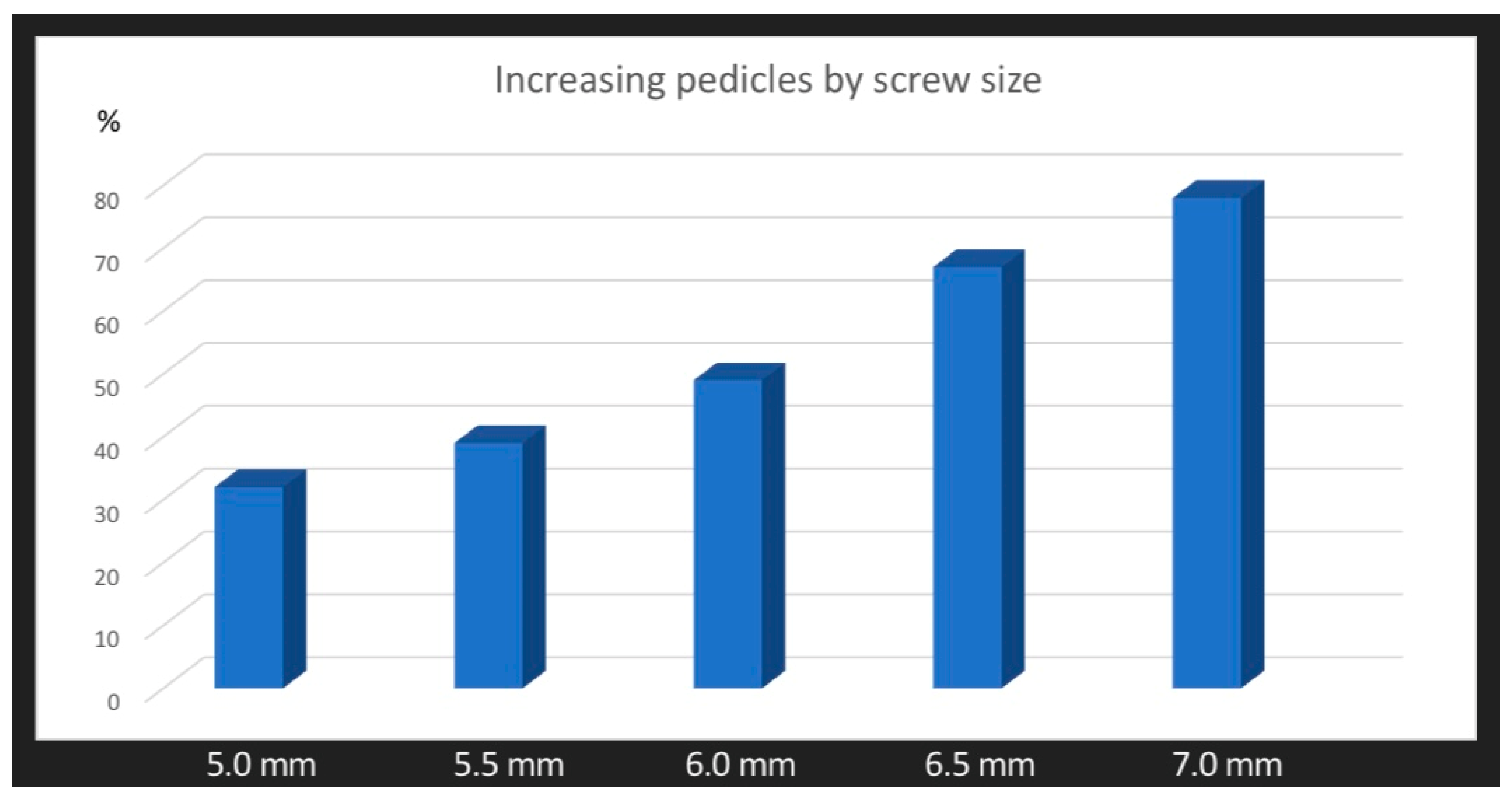
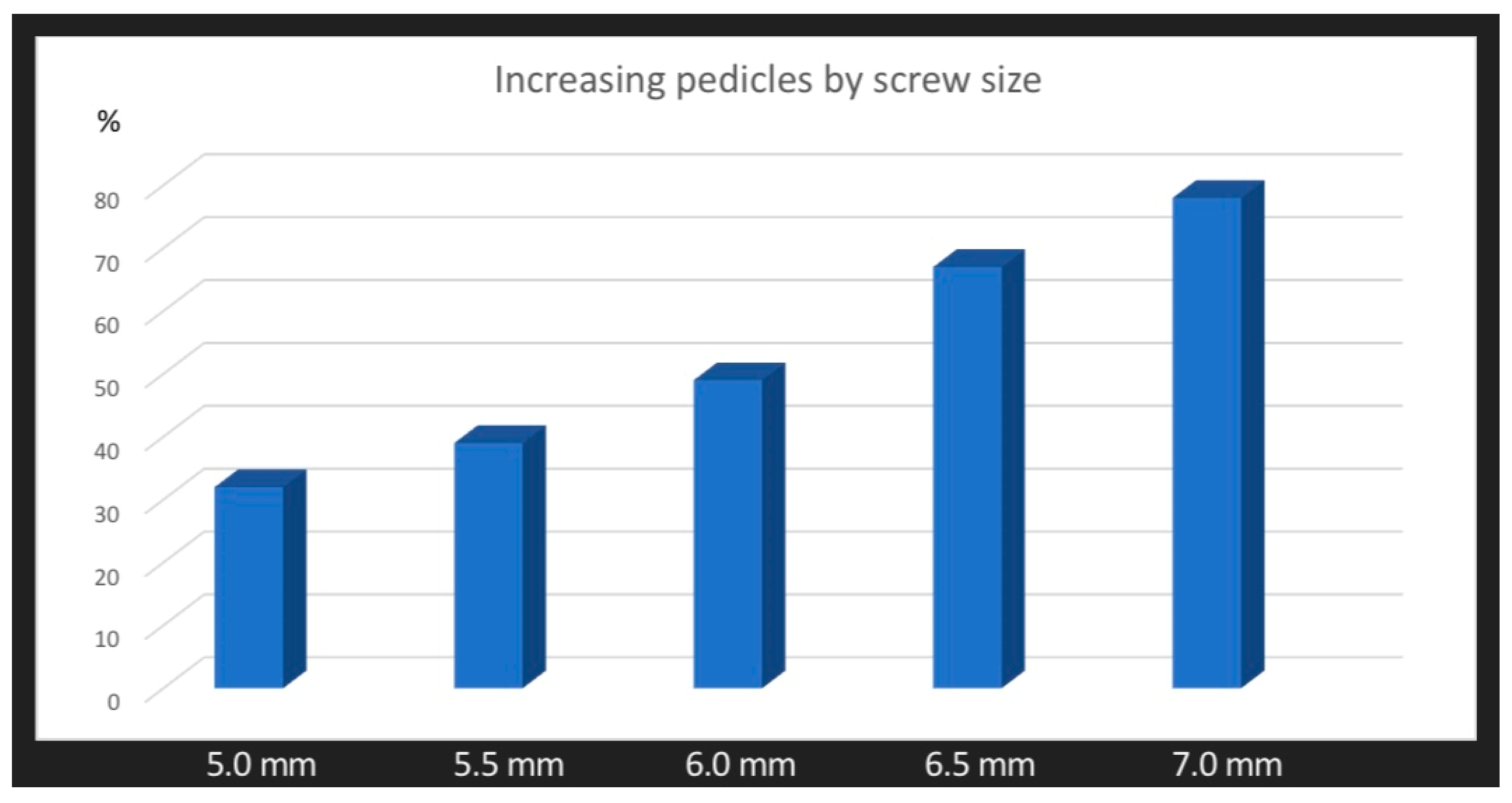
| Variable | 5.0 mm | 5.5 mm | 6.0 mm | 6.5 mm | 7.0 mm |
|---|---|---|---|---|---|
| Mean pedicle expansion % by screw size | 32% (4.6) | 39% (5.8) | 49% (6.6) | 67% (8.2) | 78% (8.8) |
| 5.0 vs. 6.0 p = 0.03 | 5.0 vs. 5.5 p = 0.661 | 5.5 vs. 6.0 p = 0.227 | 6.0 vs. 6.5 p = 0.113 | 6.5 vs. 7.0 p = 0.121 | 5.5 vs. 6.5 p = 0.03 |
| 5.0 vs. 6.5 p = 0.01 | 5.0 vs. 7.0 p = 0.01 | 5.5 vs. 7.0 p = 0.01 | 6.0 vs. 7.0 p = 0.01 | ||
| Breaches lat. by screw size | 49 (0.96%) | 49 (0.96%) | 48 (0.94%) | 55 (1.08%) | 47 (0.92%) |
| Breaches med. by screw size | 28 (0.55%) | 32 (0.63%) | 34 (0.67%) | 39 (0.76%) | 37 (0.72%) |
| Total breaches | 77 (1.51%) | 81 (1.59%) | 82 (1.61%) | 94 (1.85%) | 84 (1.65%) |
| p Breaches lat. vs. med. | p = 0.39 | p = 0.221 | p = 0.132 | p = 0.07 | p = 0.119 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grabala, P.; Helenius, I.J.; Grabala, M.; Shah, S.A. Influences of Increasing Pedicle Screw Diameter on Widening Vertebral Pedicle Size during Surgery in Spinal Deformities in Children and Adolescents without Higher Risk of Pedicle and Vertebral Breaches. J. Clin. Med. 2023, 12, 5368. https://doi.org/10.3390/jcm12165368
Grabala P, Helenius IJ, Grabala M, Shah SA. Influences of Increasing Pedicle Screw Diameter on Widening Vertebral Pedicle Size during Surgery in Spinal Deformities in Children and Adolescents without Higher Risk of Pedicle and Vertebral Breaches. Journal of Clinical Medicine. 2023; 12(16):5368. https://doi.org/10.3390/jcm12165368
Chicago/Turabian StyleGrabala, Pawel, Ilkka J. Helenius, Michal Grabala, and Suken A. Shah. 2023. "Influences of Increasing Pedicle Screw Diameter on Widening Vertebral Pedicle Size during Surgery in Spinal Deformities in Children and Adolescents without Higher Risk of Pedicle and Vertebral Breaches" Journal of Clinical Medicine 12, no. 16: 5368. https://doi.org/10.3390/jcm12165368
APA StyleGrabala, P., Helenius, I. J., Grabala, M., & Shah, S. A. (2023). Influences of Increasing Pedicle Screw Diameter on Widening Vertebral Pedicle Size during Surgery in Spinal Deformities in Children and Adolescents without Higher Risk of Pedicle and Vertebral Breaches. Journal of Clinical Medicine, 12(16), 5368. https://doi.org/10.3390/jcm12165368