
Latanoprostene Bunod 0.024% in the Treatment of Open-Angle Glaucoma and Ocular Hypertension: A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Extraction of Variables
2.4. Statistical Analysis
3. Results
3.1. Search Results
3.2. Characteristics of Included Studies
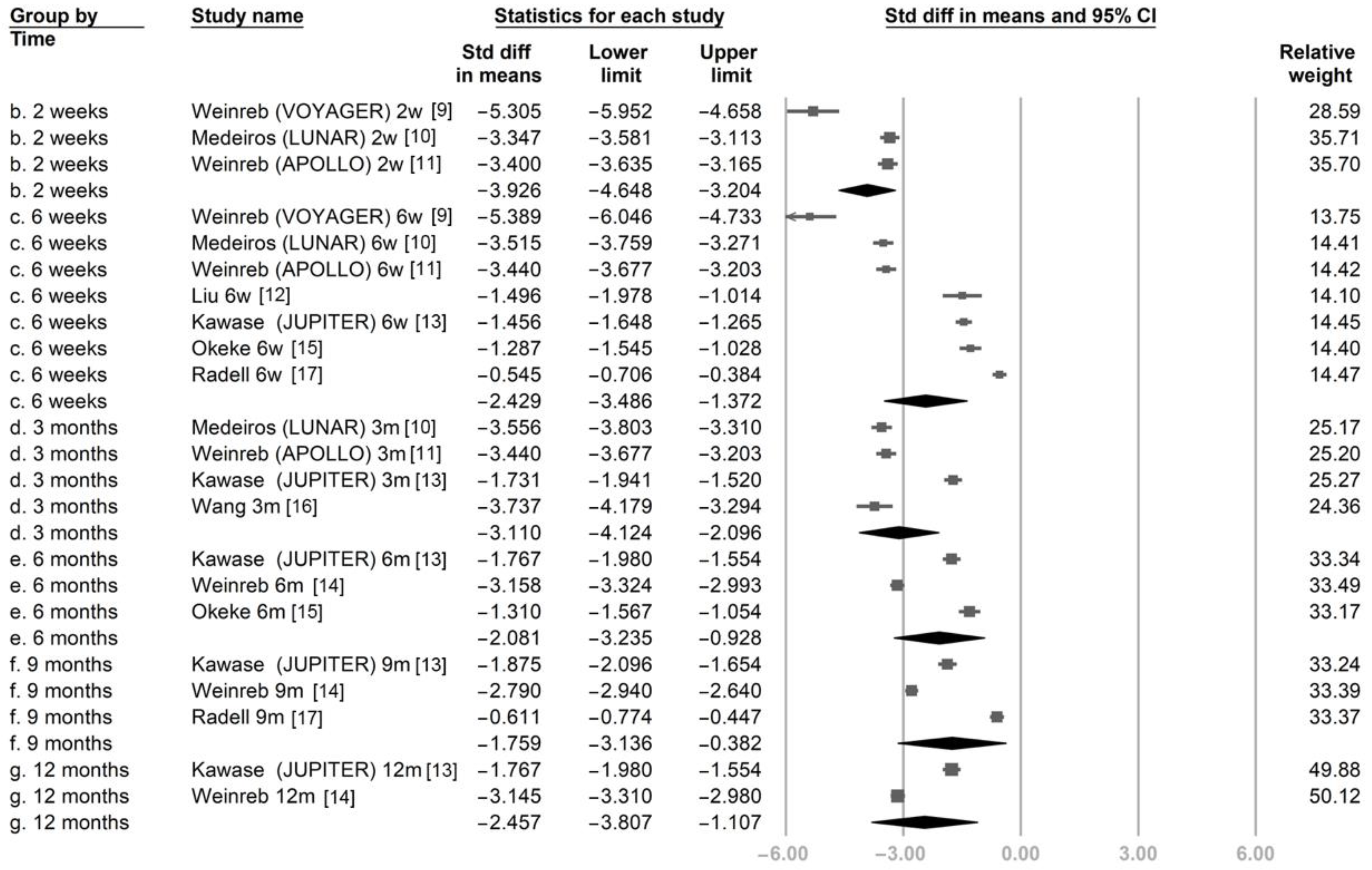
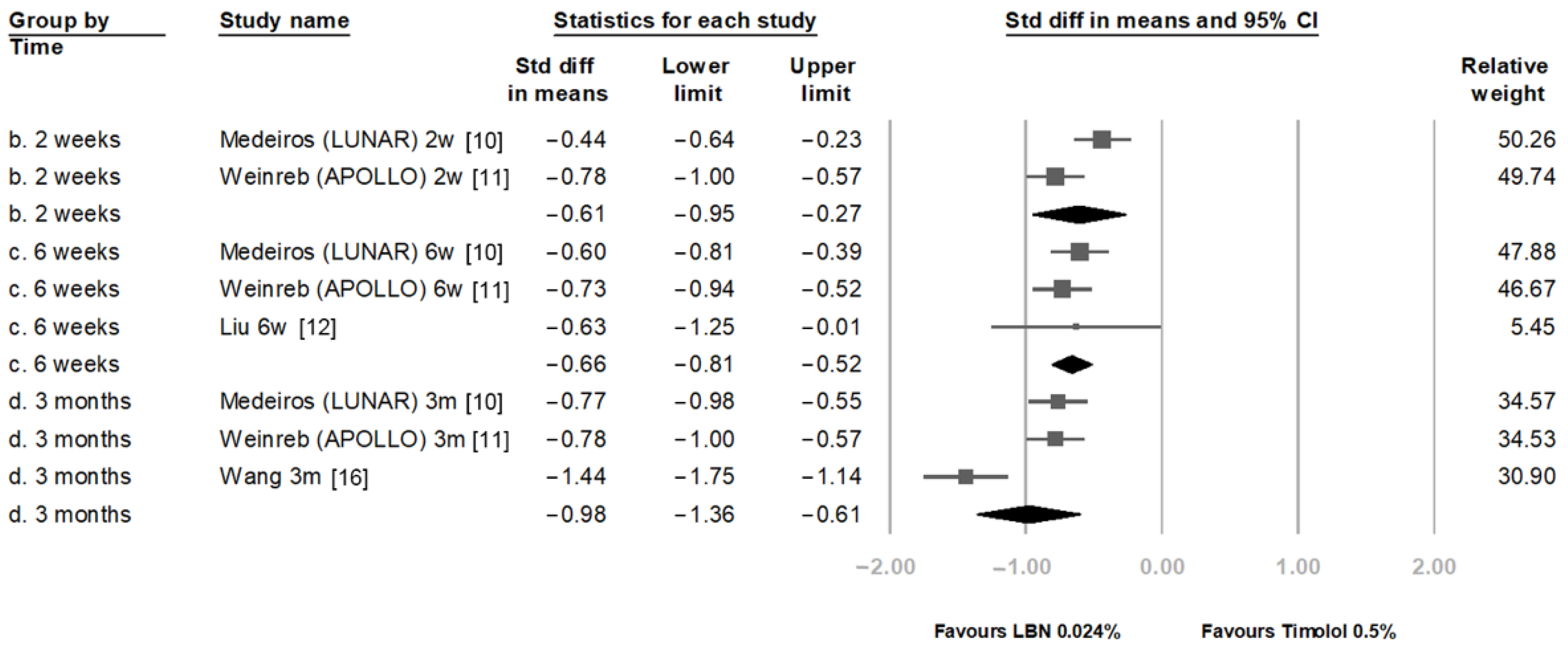
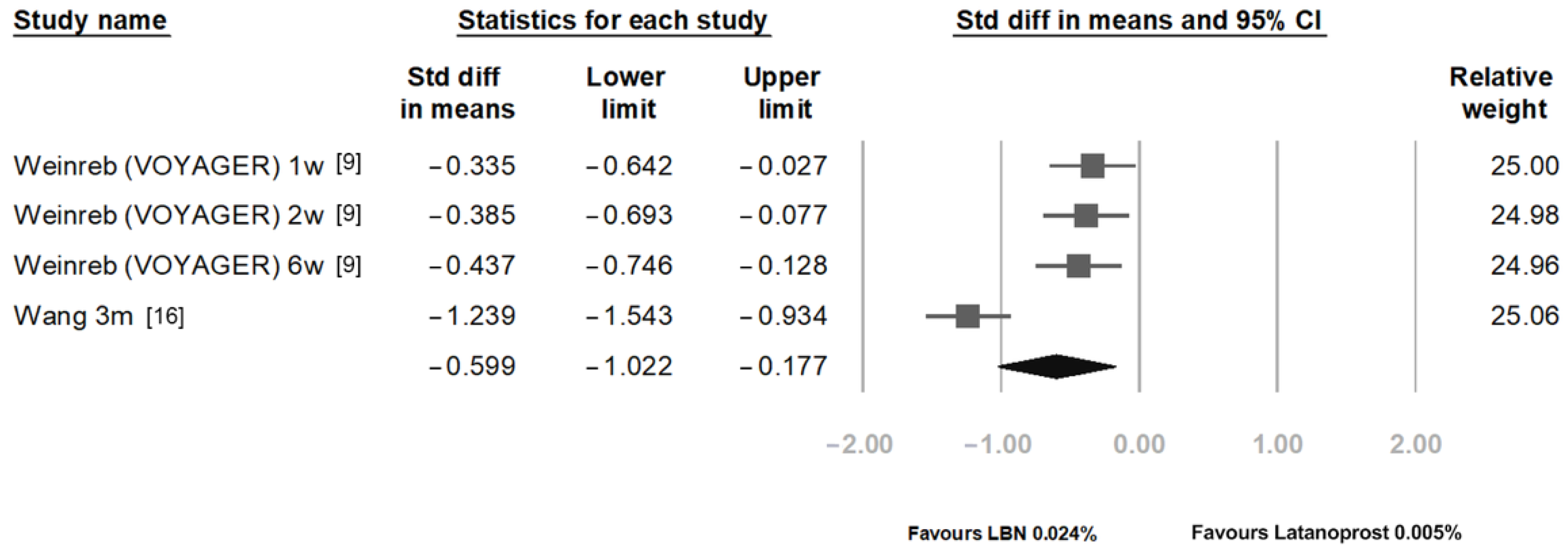
3.3. Outcome Assessment
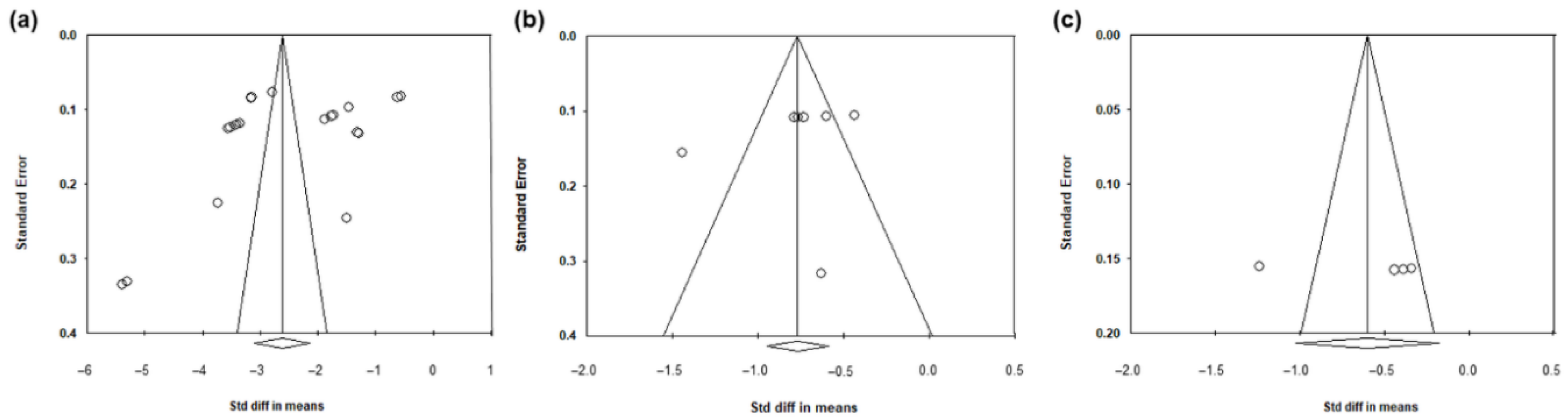
3.4. Heterogeneity and Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heijl, A.; Leske, M.C.; Bengtsson, B.; Hyman, L.; Bengtsson, B.; Hussein, M. Reduction of intraocular pressure and glaucoma progression: Results from the early manifest glaucoma trial. Arch. Ophthalmol. 2002, 120, 1268–1279. [Google Scholar] [CrossRef] [PubMed]
- Leske, M.C.; Heijl, A.; Hussein, M.; Bengtsson, B.; Hyman, L.; Komaroff, E. Factors for glaucoma progression and the effect of treatment: The early manifest glaucoma trial. Arch. Ophthalmol. 2003, 121, 48–56. [Google Scholar] [CrossRef]
- Prum, B.E., Jr.; Lim, M.C.; Mansberger, S.L.; Stein, J.D.; Moroi, S.E.; Gedde, S.J.; Herndon, L.W., Jr.; Rosenberg, L.F.; Williams, R.D. Primary open-angle glaucoma suspect preferred practice pattern® guidelines. Ophthalmology 2016, 123, P112–P151. [Google Scholar] [CrossRef]
- Li, T.; Lindsley, K.; Rouse, B.; Hong, H.; Shi, Q.; Friedman, D.S.; Wormald, R.; Dickersin, K. Comparative effectiveness of first-line medications for primary open-angle glaucoma: A systematic review and network meta-analysis. Ophthalmology 2016, 123, 129–140. [Google Scholar] [CrossRef] [Green Version]
- Garway-Heath, D.F.; Crabb, D.P.; Bunce, C.; Lascaratos, G.; Amalfitano, F.; Anand, N.; Azuara-Blanco, A.; Bourne, R.R.; Broadway, D.C.; Cunliffe, I.A.; et al. Latanoprost for open-angle glaucoma (ukgts): A randomised, multicentre, placebo-controlled trial. Lancet 2015, 385, 1295–1304. [Google Scholar] [CrossRef] [Green Version]
- Krauss, A.H.; Impagnatiello, F.; Toris, C.B.; Gale, D.C.; Prasanna, G.; Borghi, V.; Chiroli, V.; Chong, W.K.; Carreiro, S.T.; Ongini, E. Ocular hypotensive activity of bol-303259-x, a nitric oxide donating prostaglandin f2α agonist, in preclinical models. Exp. Eye Res. 2011, 93, 250–255. [Google Scholar] [CrossRef]
- Kaufman, P.L. Latanoprostene bunod ophthalmic solution 0.024% for iop lowering in glaucoma and ocular hypertension. Expert Opin. Pharmacother. 2017, 18, 433–444. [Google Scholar] [CrossRef] [Green Version]
- Cavet, M.E.; Vittitow, J.L.; Impagnatiello, F.; Ongini, E.; Bastia, E. Nitric oxide (no): An emerging target for the treatment of glaucoma. Investig. Ophthalmol. Vis. Sci. 2014, 55, 5005–5015. [Google Scholar] [CrossRef] [Green Version]
- Weinreb, R.N.; Ong, T.; Scassellati Sforzolini, B.; Vittitow, J.L.; Singh, K.; Kaufman, P.L. A randomised, controlled comparison of latanoprostene bunod and latanoprost 0.005% in the treatment of ocular hypertension and open angle glaucoma: The voyager study. Br. J. Ophthalmol. 2015, 99, 738–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medeiros, F.A.; Martin, K.R.; Peace, J.; Scassellati Sforzolini, B.; Vittitow, J.L.; Weinreb, R.N. Comparison of latanoprostene bunod 0.024% and timolol maleate 0.5% in open-angle glaucoma or ocular hypertension: The lunar study. Am. J. Ophthalmol. 2016, 168, 250–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinreb, R.N.; Scassellati Sforzolini, B.; Vittitow, J.; Liebmann, J. Latanoprostene bunod 0.024% versus timolol maleate 0.5% in subjects with open-angle glaucoma or ocular hypertension: The apollo study. Ophthalmology 2016, 123, 965–973. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.H.K.; Slight, J.R.; Vittitow, J.L.; Scassellati Sforzolini, B.; Weinreb, R.N. Efficacy of latanoprostene bunod 0.024% compared with timolol 0.5% in lowering intraocular pressure over 24 hours. Am. J. Ophthalmol. 2016, 169, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawase, K.; Vittitow, J.L.; Weinreb, R.N.; Araie, M. Long-term safety and efficacy of latanoprostene bunod 0.024% in japanese subjects with open-angle glaucoma or ocular hypertension: The jupiter study. Adv. Ther. 2016, 33, 1612–1627. [Google Scholar] [CrossRef] [Green Version]
- Weinreb, R.N.; Liebmann, J.M.; Martin, K.R.; Kaufman, P.L.; Vittitow, J.L. Latanoprostene bunod 0.024% in subjects with open-angle glaucoma or ocular hypertension: Pooled phase 3 study findings. J. Glaucoma 2018, 27, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Okeke, C.O.; Burstein, E.S.; Trubnik, V.; Deom, J.E.; Cooper, M.S.; Brinkley, D.A.; Thimons, J.J.; Kabiri, A.J.; Gelb, K.M. Retrospective chart review on real-world use of latanoprostene bunod 0.024% in treatment-naïve patients with open-angle glaucoma. Ophthalmol. Ther. 2020, 9, 1041–1053. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liao, Y.; Nie, X. Comparative evaluation of latanoprostene bunod, timolol maleate, and latanoprost ophthalmic solutions to assess their safety and efficacy in lowering intraocular pressure for the management of open-angle glaucoma. Clinics 2020, 75, e1874. [Google Scholar] [CrossRef]
- Radell, J.E.; Sharma, H.K.; Auyeung, K.L.; Paul, M.E.; Gagliuso, D.J.; Chadha, N.; Tsai, J.C.; Serle, J.B. Two-year experience with latanoprostene bunod in clinical practice. J. Glaucoma 2021, 30, 776–780. [Google Scholar] [CrossRef] [PubMed]
- MacIver, S.; Stout, N.; Ricci, O. New considerations for the clinical efficacy of old and new topical glaucoma medications. Clin. Exp. Optom. 2021, 104, 350–366. [Google Scholar] [CrossRef]
- Cvenkel, B.; Kolko, M. Current medical therapy and future trends in the management of glaucoma treatment. J. Ophthalmol. 2020, 2020, 6138132. [Google Scholar] [CrossRef]
- Arnal, J.F.; Dinh-Xuan, A.T.; Pueyo, M.; Darblade, B.; Rami, J. Endothelium-derived nitric oxide and vascular physiology and pathology. Cell. Mol. Life Sci. 1999, 55, 1078–1087. [Google Scholar] [CrossRef]
- Dismuke, W.M.; Mbadugha, C.C.; Ellis, D.Z. No-induced regulation of human trabecular meshwork cell volume and aqueous humor outflow facility involve the bkca ion channel. Am. J. Physiol. Cell Physiol. 2008, 294, C1378–C1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneemann, A.; Dijkstra, B.G.; van den Berg, T.J.; Kamphuis, W.; Hoyng, P.F. Nitric oxide/guanylate cyclase pathways and flow in anterior segment perfusion. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie 2002, 240, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Heimark, R.L.; Kaochar, S.; Stamer, W.D. Human schlemm’s canal cells express the endothelial adherens proteins, ve-cadherin and pecam-1. Curr. Eye Res. 2002, 25, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Cavet, M.E.; Vollmer, T.R.; Harrington, K.L.; VanDerMeid, K.; Richardson, M.E. Regulation of endothelin-1-induced trabecular meshwork cell contractility by latanoprostene bunod. Investig. Ophthalmol. Vis. Sci. 2015, 56, 4108–4116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harasymowycz, P.; Royer, C.; Cui, A.X.; Barbeau, M.; Jobin-Gervais, K.; Mathurin, K.; Lachaine, J.; Beauchemin, C. Short-term efficacy of latanoprostene bunod for the treatment of open-angle glaucoma and ocular hypertension: A systematic literature review and a network meta-analysis. Br. J. Ophthalmol. 2022, 106, 640–647. [Google Scholar] [CrossRef]
- Mao, Y.J.; Wu, J.B.; Yang, Z.Q.; Zhang, Y.H.; Huang, Z.J. Nitric oxide donating anti-glaucoma drugs: Advances and prospects. Chin. J. Nat. Med. 2020, 18, 275–283. [Google Scholar] [CrossRef]
- Matsou, A.; Anastasopoulos, E. Investigational drugs targeting prostaglandin receptors for the treatment of glaucoma. Expert Opin. Investig. Drugs 2018, 27, 777–785. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Country | Study Design | Diagnosis | Groups | Num of pts | Num of Eyes | Age (Mean ± SD) | Male, n (%) |
|---|---|---|---|---|---|---|---|---|---|
| Weinreb (VOYAGER) [9] | 2015 | USA, Europe | Multicenter RCT | POAG, OHT | LBN | 83 | 83 | 60.8 ± 11.47 | 26 (31.3) |
| Latanoprost | 82 | 82 | 61.2 ± 11.92 | 29 (35.4) | |||||
| Medeiros (LUNAR) [10] | 2016 | USA, Europe | Multicenter RCT | POAG, OHT | LBN | 259 | 278 | 65.0 ± 9.77 | 116 (41.7) |
| Timolol | 128 | 136 | 64.1 ± 9.71 | 57 (41.9) | |||||
| Weinreb (APOLLO) [11] | 2016 | USA, Europe | Multicenter RCT | POAG, OHT | LBN | 284 | 284 | 64.7 ± 10.3 | 118 (41.5) |
| Timolol | 133 | 133 | 63.1 ± 11.2 | 56 (42.1) | |||||
| Liu (CONSTELLATION) [12] | 2016 | USA | Prospective, open-label, RCT | POAG, OHT | LBN | 25 | 25 | 60.3 ± 10.6 | 7(28) |
| Timolol | 25 | 25 | 60.3 ± 10.6 | 7(28) | |||||
| Kawase (JUPITER) [13] | 2016 | Japan | single-arm, multicenter, open-label, clinical study | OAG, OHT | LBN | 130 | 130 | 62.5 ± 18.9 | 56(43.1) |
| Weinreb (Pooled) [14] | 2018 | USA, Europe | Pooled analysis of APOLLO and LUNAR | POAG, OHT | LBN | 562 | 562 | 64.9 ± 10.04 | 234 (41.6) |
| Timolol * | 269 | 269 | 63.7 ± 10.47 | 113 (42.0) | |||||
| Okeke [15] | 2020 | USA | Multi-center retrospective | POAG, LTG, others | LBN | 65 | 65 | 59.3 ± 14.4 | 30 (46.2) |
| Wang [16] | 2020 | China | Retrospective | POAG, OHT | Latanoprost | 104 | NR | 58.42 ± 6.12 | 55 (53) |
| LBN | 94 | NR | 57.65 ± 6.01 | 49 (52) | |||||
| Timolol | 115 | NR | 57.99 ± 6.44 | 53 (46) | |||||
| Radell [17] | 2021 | USA | Single center retrospective | POAG, LTG, others | LBN | 56 | 102 | 68.8 ± 12.4 | 28 (50) |
| Post-Treatment IOP | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | Groups | Baseline IOP (Mean ± SD) | 1 Week | 2 Weeks | 6 Weeks | 12 Weeks | 6 Months | 9 Months | 12 Months |
| Weinreb (VOYAGER), 2015 [9] | LBN | 26.01 ± 1.67 | 17.74 | 17.15 | 17.01 | NR | NR | NR | NR |
| Latanoprost | 26.15 ± 1.79 | 18.86 | 18.43 | 18.38 | NR | NR | NR | NR | |
| Medeiros (LUNAR), 2016 [10] | LBN | 26.6 ± 2.39 | NR | 18.6 | 18.2 | 18.1 | NR | NR | NR |
| Timolol | 26.4 ± 2.30 | NR | 19.2 | 19.1 | 19.3 | NR | NR | NR | |
| Weinreb (APOLLO), 2016 [11] | LBN | 26.7 ± 2.5 | NR | 18.2 | 18.1 | 18.1 | NR | NR | NR |
| Timolol | 26.5 ± 2.4 | NR | 19.5 | 19.3 | 19.4 | NR | NR | NR | |
| Liu (CONSTELLATION), 2016 [12] | LBN | 21.6 ± 2.8 | NR | NR | 17.6 ± 2.5 | NR | NR | NR | NR |
| Timolol | 21.6 ± 2.8 | NR | NR | 18.9 ± 2.4 | NR | NR | NR | NR | |
| Kawase (JUPITER), 2016 [13] | LBN | 19.6 ± 2.9 | NR | NR | 15.3 ± 3.0 | 14.8 | 14.7 | 14.4 | 14.7 |
| Weinreb (Pooled), 2018 [14] | LBN * | 26.7 ± 2.43 | NA | NA | NA | NA | 18.1 ± 2.9 | 18.2 ± 3.3 | 17.9 ± 3.0 |
| Okeke, 2020 [15] | LBN | 21.7 ± 5.9 | NR | NR | 14.7 ± 4.1 | NR | 14.4 ± 3.2 | NR | NR |
| Wang, 2020 [16] | Latanoprost | 24.13 ± 1.12 | NR | NR | NR | 19.45 ± 1.01 | NR | NR | NR |
| LBN | 23.98 ± 1.22 | NR | NR | NR | 17.45 ± 1.89 | NR | NR | NR | |
| Timolol | 24.39 ± 1.65 | NR | NR | NR | 19.68 ± 1.08 | NR | NR | NR | |
| Radell, 2021 [17] | LBN | 16.2 ± 4.3 | NR | NR | 14.0 ± 3.6 | NR | NR | 13.7 ± 3.8 | NR |
| Study | Groups | Num of Eyes | ≥1 AE, n (%) | Types of Complication (%) |
|---|---|---|---|---|
| Weinreb(VOYAGER), 2015 [9] | LBN | 83 | 20 (24.1) | Ocular hyperaemia (2.4), Conjunctival hyperaemia (4.8), Eye irritation (3.6), Punctate keratitis (2.4), Dry eye (2.4), Photophobia (2.4), Instillation site pain(12) |
| Latanoprost | 82 | 10 (12.2) | Ocular hyperaemia (8.5), Punctate keratitis (1.2), Instillation site pain(6.1) | |
| Medeiros(LUNAR), 2016 [10] | LBN | 277 | 66 (23.8) | Conjunctival hyperemia(9), Eye irritation (7.2), Eye pain (5.8), Ocular hyperemia (2.5), Vision blurred (1.8), Eye pruritis (1.4), Dry eye (1.1), Punctate keratitis (1.1), Foreign body sensation (1.1), Instillation site pain(1.4) |
| Timolol | 135 | 18 (13.3) | Conjunctival hyperemia(0.7), Eye irritation (4.4), Eye pain (3.7), Ocular hyperemia (0.7), Vision blurred (2.2), Eye pruritis (0.7), Dry eye (0.7) | |
| Weinreb(APOLLO), 2016 [11] | LBN | 283 | 38 (13.4) | Eye irritation (3.9), Conjunctival hyperemia (2.8), Eye pain (1.4), Dry eye (1.1), Foreign body sensation (1.1), Instillation site pain (1.1) |
| Timolol | 135 | 16 (11.9) | Eye irritation (2.2), Conjunctival hyperemia (1.5), Eye pain (2.2), Dry eye (0.7), Instillation site pain (1.5) | |
| Liu, 2016 [12] | LBN | 23 | 2(8.7) | Punctate keratitis (4.3) Instillation site erythema (4.3) |
| Timolol | 23 | 4(17.4) | Punctate keratitis (13), Instillation site irritation (4.3) | |
| Kawase (JUPITER), 2016 [13] | LBN | 130 | 76 (58.5) | conjunctival hyperemia (17.7), growth of eyelashes (16.2 ), eye irritation (11.5), eye pain (10 ), Iris hyperpigmentation(3.8), Blepharal pigmentation(3.1), Blepharitis (2.3), Eye pruritus(2.3), Asthenopia(2.3), Conjunctival hemorrhage (1.5), Punctate keratitis(2.3), Trichiasis(2.3), Cataract(0.8), Hordeolum(0.8), Visual impairment (0.8), Vitreous floaters (0.8), Foreign body sensation(1.5) |
| Weinreb (Pooled), 2018 [14] | LBN(LBN + Timolol cross over to LBN) | 811 | 175 (21.6) | Conjunctival hyperemia(5.9), Eye irritation (4.6), Eye pain (3.6), Ocular hyperemia (2), Instillation site pain (2) |
| Timolol | 271 | 34 (12.5) | Conjunctival hyperemia(1.1), Eye irritation (2.6), Eye pain (2.2), Ocular hyperemia (0.7), Instillation site pain (1.8) | |
| Okeke, 2020 [15] | LBN | 65 | 33 (50.8) | Blurred vision (15.4), Dryness (12.3), Irritation(7.7), Itching (7.7), Light sensitivity (7.7), Burning (6.2), Eye pain (4.6), Tearing (4.6), Change in vision (3.1), Keratitis (3.1), Macular degeneration (3.1) |
| Wang, 2020 [16] | Latanoprost | 104 | NR | Eye irritation (4), Dry eye(2), Eye pain(3), Conjunctival hyperemia(4), Foreign body sensation(3) |
| LBN | 94 | NR | Eye irritation (4), Dry eye(2), Eye pain(3), Conjunctival hyperemia(3), Foreign body sensation(2) | |
| Timolol | 115 | NR | Eye irritation (2), Dry eye(1), Eye pain(1), Conjunctival hyperemia(1), Foreign body sensation(1) | |
| Radell, 2021 [17] | LBN | 56 | 8(14) | pain, itching (14) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo, T.-C.; Chen, Y.-Y.; Hung, M.-C.; Chou, P. Latanoprostene Bunod 0.024% in the Treatment of Open-Angle Glaucoma and Ocular Hypertension: A Meta-Analysis. J. Clin. Med. 2022, 11, 4325. https://doi.org/10.3390/jcm11154325
Lo T-C, Chen Y-Y, Hung M-C, Chou P. Latanoprostene Bunod 0.024% in the Treatment of Open-Angle Glaucoma and Ocular Hypertension: A Meta-Analysis. Journal of Clinical Medicine. 2022; 11(15):4325. https://doi.org/10.3390/jcm11154325
Chicago/Turabian StyleLo, Tzu-Chen, Yu-Yen Chen, Man-Chen Hung, and Pesus Chou. 2022. "Latanoprostene Bunod 0.024% in the Treatment of Open-Angle Glaucoma and Ocular Hypertension: A Meta-Analysis" Journal of Clinical Medicine 11, no. 15: 4325. https://doi.org/10.3390/jcm11154325
APA StyleLo, T.-C., Chen, Y.-Y., Hung, M.-C., & Chou, P. (2022). Latanoprostene Bunod 0.024% in the Treatment of Open-Angle Glaucoma and Ocular Hypertension: A Meta-Analysis. Journal of Clinical Medicine, 11(15), 4325. https://doi.org/10.3390/jcm11154325