

Persistence of Depression and Anxiety despite Short-Term Disease Activity Improvement in Patients with Systemic Lupus Erythematosus: A Single-Centre, Prospective Study


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Monitoring Protocol, Disease Evaluation, and Data Collection
2.3. Assessment of Anxiety, Depression, and Treatment Adherence
2.4. Statistical Analysis
2.5. Ethical Aspects
3. Results
3.1. Patients with Active SLE Manifest Increased Anxiety and Depression Levels That Persist over Time
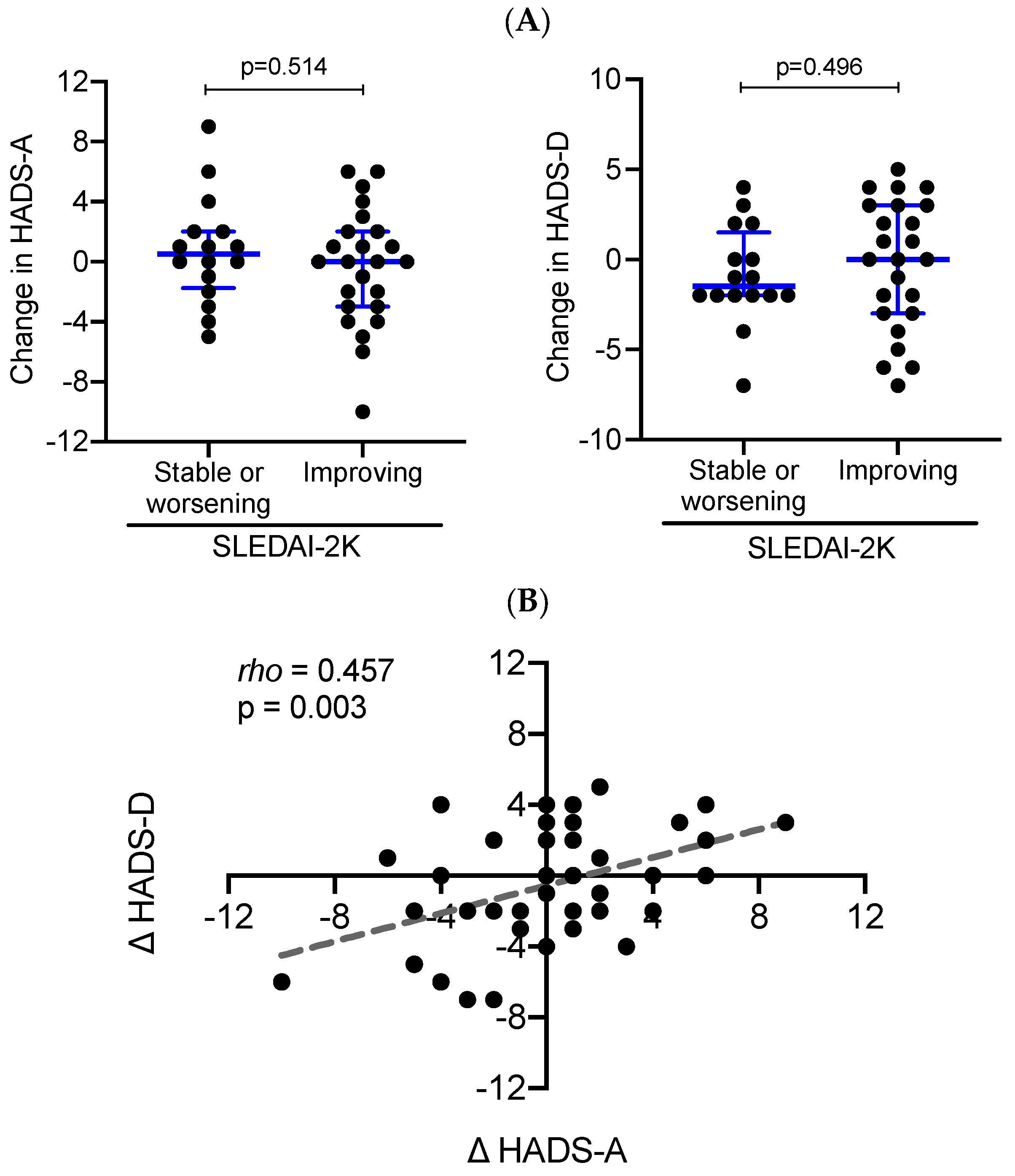
3.2. Lack of Correlation between Longitudinal Changes in Disease Activity and Mental Disorders in SLE Patients
3.3. Association of Mental Disorders with Sociodemographic Characteristics in SLE Patients
3.4. Increased Anxiety and Depression Levels Are Associated with Lower Adherence to Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gergianaki, I.; Garantziotis, P.; Adamichou, C.; Saridakis, I.; Spyrou, G.; Sidiropoulos, P.; Bertsias, G. High Comorbidity Burden in Patients with SLE: Data from the Community-Based Lupus Registry of Crete. J. Clin. Med. 2021, 10, 998. [Google Scholar] [CrossRef] [PubMed]
- Rees, F.; Doherty, M.; Grainge, M.; Lanyon, P.; Davenport, G.; Zhang, W. Burden of Comorbidity in Systemic Lupus Erythematosus in the UK, 1999–2012. Arthritis Care Res. 2016, 68, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, A.T.; Moazzami, M.; Engel, L.; Bangert, E.; Hassanein, M.; Marzouk, S.; Kravtsenyuk, M.; Fung, W.; Eder, L.; Su, J.; et al. Prevalence and metric of depression and anxiety in systemic lupus erythematosus: A systematic review and meta-analysis. Semin. Arthritis Rheum. 2020, 50, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Fu, T.; Yin, R.; Zhang, Q.; Shen, B. Prevalence of depression and anxiety in systemic lupus erythematosus: A systematic review and meta-analysis. BMC Psychiatry 2017, 17, 70. [Google Scholar] [CrossRef]
- McCormick, N.; Trupin, L.; Yelin, E.H.; Katz, P.P. Socioeconomic Predictors of Incident Depression in Systemic Lupus Erythematosus. Arthritis Care Res. 2018, 70, 104–113. [Google Scholar] [CrossRef]
- Patterson, S.L.; Trupin, L.; Yazdany, J.; Dall’Era, M.; Lanata, C.; Dequattro, K.; Hartogensis, W.; Katz, P. Physical Inactivity Independently Predicts Incident Depression in a Multi-Racial/Ethnic Systemic Lupus Cohort. Arthritis Care Res. 2021, 74, 1098–1104. [Google Scholar] [CrossRef]
- Figueiredo-Braga, M.; Cornaby, C.; Cortez, A.; Bernardes, M.; Terroso, G.; Figueiredo, M.; Mesquita, C.D.S.; Costa, L.; Poole, B.D. Depression and anxiety in systemic lupus erythematosus: The crosstalk between immunological, clinical, and psychosocial factors. Medicine 2018, 97, e11376. [Google Scholar] [CrossRef]
- Monahan, R.C.; Beaart-van de Voorde, L.J.; Eikenboom, J.; Fronczek, R.; Kloppenburg, M.; Middelkoop, H.A.; Terwindt, G.M.; van der Wee, N.J.; Huizinga, T.W.; Steup-Beekman, G.M. Fatigue in patients with systemic lupus erythematosus and neuropsychiatric symptoms is associated with anxiety and depression rather than inflammatory disease activity. Lupus 2021, 30, 1124–1132. [Google Scholar] [CrossRef]
- Lillis, T.A.; Tirone, V.; Gandhi, N.; Weinberg, S.; Nika, A.; Sequeira, W.; Hobfoll, S.E.; Block, J.A.; Jolly, M. Sleep Disturbance and Depression Symptoms Mediate Relationship Between Pain and Cognitive Dysfunction in Lupus. Arthritis Care Res. 2019, 71, 406–412. [Google Scholar] [CrossRef]
- Bingham, K.S.; DiazMartinez, J.; Green, R.; Tartaglia, M.C.; Ruttan, L.; Su, J.; Wither, J.E.; Kakvan, M.; Anderson, N.; Bonilla, D.; et al. Longitudinal relationships between cognitive domains and depression and anxiety symptoms in systemic lupus erythematosus. Semin. Arthritis Rheum. 2021, 51, 1186–1192. [Google Scholar] [CrossRef]
- Jorge, A.; Lertratanakul, A.; Lee, J.; Pearce, W.; McPherson, D.; Thompson, T.; Barinas-Mitchell, E.; Ramsey-Goldman, R. Depression and Progression of Subclinical Cardiovascular Disease in Systemic Lupus Erythematosus. Arthritis Care Res. 2017, 69, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Utset, T.O.; Baskaran, A.; Segal, B.M.; Trupin, L.; Ogale, S.; Herberich, E.; Kalunian, K. Work disability, lost productivity and associated risk factors in patients diagnosed with systemic lupus erythematosus. Lupus Sci. Med. 2015, 2, e000058. [Google Scholar] [CrossRef] [PubMed]
- Sumner, L.A.; Olmstead, R.; Azizoddin, D.R.; Ormseth, S.R.; Draper, T.L.; Ayeroff, J.R.; Zamora-Racaza, G.; Weisman, M.H.; Nicassio, P.M. The contributions of socioeconomic status, perceived stress, and depression to disability in adults with systemic lupus erythematosus. Disabil. Rehabil. 2020, 42, 1264–1269. [Google Scholar] [CrossRef] [PubMed]
- Parperis, K.; Psarelis, S.; Chatzittofis, A.; Michaelides, M.; Nikiforou, D.; Antoniade, E.; Bhattarai, B. Association of clinical characteristics, disease activity and health-related quality of life in SLE patients with major depressive disorder. Rheumatology 2021, 60, 5369–5378. [Google Scholar] [CrossRef]
- Dietz, B.; Katz, P.; Dall’Era, M.; Murphy, L.B.; Lanata, C.; Trupin, L.; Criswell, L.A.; Yazdany, J. Major Depression and Adverse Patient-Reported Outcomes in Systemic Lupus Erythematosus: Results From a Prospective Longitudinal Cohort. Arthritis Care Res. 2021, 73, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Nowicka-Sauer, K.; Hajduk, A.; Kujawska-Danecka, H.; Banaszkiewicz, D.; Smolenska, Z.; Czuszynska, Z.; Siebert, J. Illness perception is significantly determined by depression and anxiety in systemic lupus erythematosus. Lupus 2018, 27, 454–460. [Google Scholar] [CrossRef]
- Tay, S.H.; Cheung, P.P.; Mak, A. Active disease is independently associated with more severe anxiety rather than depressive symptoms in patients with systemic lupus erythematosus. Lupus 2015, 24, 1392–1399. [Google Scholar] [CrossRef]
- Abd-Alrasool, Z.A.; Gorial, F.I.; Hashim, M.T. Prevalence and severity of depression among Iraqi patients with systemic lupus erythematosus: A descriptive study. Mediterr. J. Rheumatol. 2017, 28, 142–146. [Google Scholar] [CrossRef]
- Eldeiry, D.; Zandy, M.; Tayer-Shifman, O.E.; Kwan, A.; Marzouk, S.; Su, J.; Bingham, K.; Touma, Z. Association between depression and anxiety with skin and musculoskeletal clinical phenotypes in systemic lupus erythematosus. Rheumatology 2020, 59, 3211–3220. [Google Scholar] [CrossRef]
- Shortall, E.; Isenberg, D.; Newman, S.P. Factors associated with mood and mood disorders in SLE. Lupus 1995, 4, 272–279. [Google Scholar] [CrossRef]
- Segui, J.; Ramos-Casals, M.; Garcia-Carrasco, M.; de Flores, T.; Cervera, R.; Valdes, M.; Font, J.; Ingelmo, M. Psychiatric and psychosocial disorders in patients with systemic lupus erythematosus: A longitudinal study of active and inactive stages of the disease. Lupus 2000, 9, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Jarpa, E.; Babul, M.; Calderon, J.; Gonzalez, M.; Martinez, M.E.; Bravo-Zehnder, M.; Henriquez, C.; Jacobelli, S.; Gonzalez, A.; Massardo, L. Common mental disorders and psychological distress in systemic lupus erythematosus are not associated with disease activity. Lupus 2011, 20, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Narupan, N.; Seeherunwong, A.; Pumpuang, W. Prevalence and biopsychosocial factors associated with depressive symptoms among patients living with systemic lupus erythematosus in clinical settings in urban Thailand. BMC Psychiatry 2022, 22, 103. [Google Scholar] [CrossRef] [PubMed]
- Tisseverasinghe, A.; Peschken, C.; Hitchon, C. Anxiety and Mood Disorders in Systemic Lupus Erythematosus: Current Insights and Future Directions. Curr. Rheumatol. Rep. 2018, 20, 85. [Google Scholar] [CrossRef]
- Alsowaida, N.; Alrasheed, M.; Mayet, A.; Alsuwaida, A.; Omair, M.A. Medication adherence, depression and disease activity among patients with systemic lupus erythematosus. Lupus 2018, 27, 327–332. [Google Scholar] [CrossRef]
- Julian, L.J.; Yelin, E.; Yazdany, J.; Panopalis, P.; Trupin, L.; Criswell, L.A.; Katz, P. Depression, medication adherence, and service utilization in systemic lupus erythematosus. Arthritis Rheum. 2009, 61, 240–246. [Google Scholar] [CrossRef]
- Du, X.; Chen, H.; Zhuang, Y.; Zhao, Q.; Shen, B. Medication Adherence in Chinese Patients With Systemic Lupus Erythematosus. J. Clin. Rheumatol. 2020, 26, 94–98. [Google Scholar] [CrossRef]
- Davis, A.M.; Graham, T.B.; Zhu, Y.; McPheeters, M.L. Depression and medication nonadherence in childhood-onset systemic lupus erythematosus. Lupus 2018, 27, 1532–1541. [Google Scholar] [CrossRef]
- Mendoza-Pinto, C.; Garcia-Carrasco, M.; Campos-Rivera, S.; Munguia-Realpozo, P.; Etchegaray-Morales, I.; Ayon-Aguilar, J.; Alonso-Garcia, N.E.; Mendez-Martinez, S. Medication adherence is influenced by resilience in patients with systemic lupus erythematosus. Lupus 2021, 30, 1051–1057. [Google Scholar] [CrossRef]
- Chang, J.C.; Davis, A.M.; Klein-Gitelman, M.S.; Cidav, Z.; Mandell, D.S.; Knight, A.M. Impact of Psychiatric Diagnosis and Treatment on Medication Adherence in Youth With Systemic Lupus Erythematosus. Arthritis Care Res. 2021, 73, 30–38. [Google Scholar] [CrossRef]
- Geraldino-Pardilla, L.; Perel-Winkler, A.; Miceli, J.; Neville, K.; Danias, G.; Nguyen, S.; Dervieux, T.; Kapoor, T.; Giles, J.; Askanase, A. Association between hydroxychloroquine levels and disease activity in a predominantly Hispanic systemic lupus erythematosus cohort. Lupus 2019, 28, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Mosley-Williams, A.; Lumley, M.A.; Gillis, M.; Leisen, J.; Guice, D. Barriers to treatment adherence among African American and white women with systemic lupus erythematosus. Arthritis Rheum. 2002, 47, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Adamichou, C.; Nikolopoulos, D.; Genitsaridi, I.; Bortoluzzi, A.; Fanouriakis, A.; Papastefanakis, E.; Kalogiannaki, E.; Gergianaki, I.; Sidiropoulos, P.; Boumpas, D.T.; et al. In an early SLE cohort the ACR-1997, SLICC-2012 and EULAR/ACR-2019 criteria classify non-overlapping groups of patients: Use of all three criteria ensures optimal capture for clinical studies while their modification earlier classification and treatment. Ann. Rheum. Dis. 2020, 79, 232–241. [Google Scholar] [CrossRef]
- Gergianaki, I.; Fanouriakis, A.; Repa, A.; Tzanakakis, M.; Adamichou, C.; Pompieri, A.; Spirou, G.; Bertsias, A.; Kabouraki, E.; Tzanakis, I.; et al. Epidemiology and burden of systemic lupus erythematosus in a Southern European population: Data from the community-based lupus registry of Crete, Greece. Ann. Rheum. Dis. 2017, 76, 1992–2000. [Google Scholar] [CrossRef] [PubMed]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 1151–1159. [Google Scholar] [CrossRef]
- Polachek, A.; Gladman, D.D.; Su, J.; Urowitz, M.B. Defining Low Disease Activity in Systemic Lupus Erythematosus. Arthritis Care Res. 2017, 69, 997–1003. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Pamfil, C.; Rednic, S.; Sidiropoulos, P.; Bertsias, G.; Boumpas, D.T. Is it primary neuropsychiatric systemic lupus erythematosus? Performance of existing attribution models using physician judgment as the gold standard. Clin. Exp. Rheumatol. 2016, 34, 910–917. [Google Scholar]
- Gladman, D.D.; Ibanez, D.; Urowitz, M.B. Systemic lupus erythematosus disease activity index 2000. J. Rheumatol. 2002, 29, 288–291. [Google Scholar]
- Petri, M.; Kim, M.Y.; Kalunian, K.C.; Grossman, J.; Hahn, B.H.; Sammaritano, L.R.; Lockshin, M.; Merrill, J.T.; Belmont, H.M.; Askanase, A.D.; et al. Combined oral contraceptives in women with systemic lupus erythematosus. N. Engl. J. Med. 2005, 353, 2550–2558. [Google Scholar] [CrossRef]
- Gladman, D.; Ginzler, E.; Goldsmith, C.; Fortin, P.; Liang, M.; Urowitz, M.; Bacon, P.; Bombardieri, S.; Hanly, J.; Hay, E.; et al. The development and initial validation of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index for systemic lupus erythematosus. Arthritis Rheum. 1996, 39, 363–369. [Google Scholar] [CrossRef]
- Bultink, I.E.; Turkstra, F.; Dijkmans, B.A.; Voskuyl, A.E. High prevalence of unemployment in patients with systemic lupus erythematosus: Association with organ damage and health-related quality of life. J. Rheumatol. 2008, 35, 1053–1057. [Google Scholar] [PubMed]
- de Almeida Macedo, E.; Appenzeller, S.; Lavras Costallat, L.T. Assessment of the Hospital Anxiety and Depression Scale (HADS) performance for the diagnosis of anxiety in patients with systemic lupus erythematosus. Rheumatol. Int. 2017, 37, 1999–2004. [Google Scholar] [CrossRef] [PubMed]
- Michopoulos, I.; Douzenis, A.; Kalkavoura, C.; Christodoulou, C.; Michalopoulou, P.; Kalemi, G.; Fineti, K.; Patapis, P.; Protopapas, K.; Lykouras, L. Hospital Anxiety and Depression Scale (HADS): Validation in a Greek general hospital sample. Ann. Gen. Psychiatry 2008, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Chatzitheodorou, D.; Kabitsis, C.; Papadopoulos, N.G.; Galanopoulou, V. Assessing disability in patients with rheumatic diseases: Translation, reliability and validity testing of a Greek version of the Stanford Health Assessment Questionnaire (HAQ). Rheumatol. Int. 2008, 28, 1091–1097. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulou, C. Perceived information needs and non-adherence: Evidence from Greek patients with hypertension. Health Expect. 2012, 15, 187–196. [Google Scholar] [CrossRef]
- Franklyn, K.; Lau, C.S.; Navarra, S.V.; Louthrenoo, W.; Lateef, A.; Hamijoyo, L.; Wahono, C.S.; Chen, S.L.; Jin, O.; Morton, S.; et al. Definition and initial validation of a Lupus Low Disease Activity State (LLDAS). Ann. Rheum. Dis. 2016, 75, 1615–1621. [Google Scholar] [CrossRef]
- Adamichou, C.; Bertsias, G. Flares in systemic lupus erythematosus: Diagnosis, risk factors and preventive strategies. Mediterr. J. Rheumatol. 2017, 28, 4–12. [Google Scholar] [CrossRef]
- Costedoat-Chalumeau, N.; Pouchot, J.; Guettrot-Imbert, G.; Le Guern, V.; Leroux, G.; Marra, D.; Morel, N.; Piette, J.C. Adherence to treatment in systemic lupus erythematosus patients. Best Pract. Res. Clin. Rheumatol. 2013, 27, 329–340. [Google Scholar] [CrossRef]
- Kwan, A.; Marzouk, S.; Ghanean, H.; Kishwar, A.; Anderson, N.; Bonilla, D.; Vitti, M.; Su, J.; Touma, Z. Assessment of the psychometric properties of patient-reported outcomes of depression and anxiety in systemic lupus erythematosus. Semin. Arthritis Rheum. 2019, 49, 260–266. [Google Scholar] [CrossRef]
- Xie, X.; Wu, D.; Chen, H. Prevalence and risk factors of anxiety and depression in patients with systemic lupus erythematosus in Southwest China. Rheumatol. Int. 2016, 36, 1705–1710. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, H.; Cevallos, A.; Jimbo Sotomayor, R.; Naranjo-Saltos, F.; Mera Orces, D.; Basantes, E. Mental disorders in systemic lupus erythematosus: A cohort study. Rheumatol. Int. 2019, 39, 1689–1695. [Google Scholar] [CrossRef]
- Gholizadeh, S.; Azizoddin, D.R.; Mills, S.D.; Zamora, G.; Potemra, H.M.K.; Hirz, A.E.; Wallace, D.J.; Weisman, M.H.; Nicassio, P.M. Body image mediates the impact of pain on depressive symptoms in patients with systemic lupus erythematosus. Lupus 2019, 28, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- Hesselvig, J.H.; Egeberg, A.; Kofoed, K.; Gislason, G.; Dreyer, L. Increased risk of depression in patients with cutaneous lupus erythematosus and systemic lupus erythematosus: A Danish nationwide cohort study. Br. J. Dermatol. 2018, 179, 1095–1101. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.L.; Kubzansky, L.D.; Malspeis, S.; Feldman, C.H.; Costenbader, K.H. Association of Depression With Risk of Incident Systemic Lupus Erythematosus in Women Assessed Across 2 Decades. JAMA Psychiatry 2018, 75, 1225–1233. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, E.; Kavroulakis, E.; Bertsias, G.; Fanouriakis, A.; Karageorgou, D.; Sidiropoulos, P.; Papastefanakis, E.; Boumpas, D.T.; Simos, P. Regional cerebral perfusion correlates with anxiety in neuropsychiatric SLE: Evidence for a mechanism distinct from depression. Lupus 2019, 28, 1678–1689. [Google Scholar] [CrossRef]
- Miyawaki, Y.; Shimizu, S.; Ogawa, Y.; Sada, K.E.; Katayama, Y.; Asano, Y.; Hayashi, K.; Yamamura, Y.; Hiramatsu-Asano, S.; Ohashi, K.; et al. Association of glucocorticoid doses and emotional health in lupus low disease activity state (LLDAS): A cross-sectional study. Arthritis Res. Ther. 2021, 23, 79. [Google Scholar] [CrossRef]
- Lew, D.; Huang, X.; Kellahan, S.R.; Xian, H.; Eisen, S.; Kim, A.H.J. Anxiety Symptoms Among Patients With Systemic Lupus Erythematosus Persist Over Time and Are Independent of SLE Disease Activity. ACR Open Rheumatol. 2022, 4, 432–440. [Google Scholar] [CrossRef]
- Kellahan, S.R.; Huang, X.; Lew, D.; Xian, H.; Eisen, S.; Kim, A.H.J. Depressed Symptomatology Persists Over Time in Systemic Lupus Erythematosus Patients. Arthritis Care Res. 2021. [Google Scholar] [CrossRef]
- Margiotta, D.P.E.; Fasano, S.; Basta, F.; Pierro, L.; Riccardi, A.; Navarini, L.; Valentini, G.; Afeltra, A. The association between duration of remission, fatigue, depression and health-related quality of life in Italian patients with systemic lupus erythematosus. Lupus 2019, 28, 1705–1711. [Google Scholar] [CrossRef]
- Azizoddin, D.R.; Zamora-Racaza, G.; Ormseth, S.R.; Sumner, L.A.; Cost, C.; Ayeroff, J.R.; Weisman, M.H.; Nicassio, P.M. Psychological Factors that Link Socioeconomic Status to Depression/Anxiety in Patients with Systemic Lupus Erythematosus. J. Clin. Psychol. Med. Settings 2017, 24, 302–315. [Google Scholar] [CrossRef] [PubMed]
- Mehat, P.; Atiquzzaman, M.; Esdaile, J.M.; AviNa-Zubieta, A.; De Vera, M.A. Medication Nonadherence in Systemic Lupus Erythematosus: A Systematic Review. Arthritis Care Res. 2017, 69, 1706–1713. [Google Scholar] [CrossRef] [PubMed]
- Heiman, E.; Lim, S.S.; Bao, G.; Drenkard, C. Depressive Symptoms Are Associated With Low Treatment Adherence in African American Individuals With Systemic Lupus Erythematosus. J. Clin. Rheumatol. 2018, 24, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Shenavandeh, S.; Mani, A.; Eazadnegahdar, M.; Nekooeian, A. Medication Adherence of Patients with Systemic Lupus Erythematosus and Rheumatoid Arthritis Considering the Psychosocial Factors, Health Literacy and Current Life Concerns of Patients. Curr. Rheumatol. Rev. 2021, 17, 412–420. [Google Scholar] [CrossRef]
- Gomez, A.; Soukka, S.; Johansson, P.; Akerstrom, E.; Emamikia, S.; Enman, Y.; Chatzidionysiou, K.; Parodis, I. Use of Antimalarial Agents is Associated with Favourable Physical Functioning in Patients with Systemic Lupus Erythematosus. J. Clin. Med. 2020, 9, 1813. [Google Scholar] [CrossRef]

{kind=link}
| No. (%) or Mean (SD) 1 | |
|---|---|
| Gender (female) | 39 (97.5%) |
| Race (white) | 40 (100.0%) |
| Age (years) | 50.5 (10.3) |
| Disease duration | 10.3 (7.0) |
| Education level | |
| Basic or primary | 6 (15.0%) |
| Secondary | 19 (47.5%) |
| High or tertiary | 14 (35.0%) |
| Employment status (working) | 21 (52.5%) |
| Comorbidities | |
| Hypertension | 7 (17.5%) |
| Dyslipidemia | 11 (27.5%) |
| Osteoporosis | 9 (22.5%) |
| Thyroiditis | 7 (17.5%) |
| Hypothyroidism | 5 (12.5%) |
| COPD 2 or bronchial asthma | 2 (5.0%) |
| Diabetes mellitus | 2 (5.0%) |
| Fibromyalgia | 15 (37.5%) |
| Mental disorder | 16 (40.0%) |
| Depression | 13 (32.5%) |
| Anxiety disorder | 5 (12.5%) |
| Organ damage (SDI) 3 | 18 (45.0%) |
| Baseline 1 | Follow-Up | p-Value 2 | |
|---|---|---|---|
| SLEDAI-2K 3 | 6.0 (4.0) | 4.0 (2.0) | 0.001 |
| 0 | 0 (0.0%) | 5 (12.5%) | |
| 1–4 | 14 (35.0%) | 22 (55.0%) | |
| 5–8 | 22 (55.0%) | 13 (32.5%) | |
| ≥9 | 4 (10.0%) | 9 (0.0%) | |
| HADS-Anxiety | 11.0 (7.8) | 11.0 (5.5) | 0.964 |
| Normal (≤7) | 12 (30.0%) | 8 (20.0%) | |
| Mild (8–10) | 7 (17.5%) | 9 (22.5%) | |
| Moderate (11–14) | 11 (27.5%) | 13 (32.5%) | |
| Severe (≥15) | 10 (25.0%) | 10 (25.0%) | |
| HADS-Depression | 8.0 (4.8) | 8.0 (6.8) | 0.463 |
| Normal (≤7) | 19 (47.5%) | 19 (47.5%) | |
| Mild (8–10) | 12 (30.0%) | 13 (32.5%) | |
| Moderate (11–14) | 6 (15.0%) | 7 (17.5%) | |
| Severe (≥15) | 3 (7.5%) | 1 (2.5%) |
| Anxiety Level (HADS-A) | Depression Level (HADS-D) | |||
|---|---|---|---|---|
| Univariate Analysis | Standardized β Coefficient; p-Value 1 | |||
| Age (years) | 0.05 | 0.771 | 0.04 | 0.812 |
| Education 2 | −0.14 | 0.389 | −0.22 | 0.172 |
| SLE duration (years) | 0.10 | 0.528 | 0.06 | 0.721 |
| Employment 3 | −0.42 | 0.007 | −0.27 | 0.093 |
| Comorbidities (no.) | 0.12 | 0.466 | 0.22 | 0.167 |
| SLEDAI-2K | −0.04 | 0.786 | −0.15 | 0.353 |
| Organ damage (SDI) | 0.08 | 0.632 | −0.22 | 0.174 |
| SLE treatment | ||||
| HCQ 4,5 | −0.07 | 0.632 | 0.11 | 0.489 |
| Glucocorticoids 4 | −0.06 | 0.372 | −0.22 | 0.180 |
| Immunosuppressives 4 | −0.45 | 0.003 | −0.17 | 0.284 |
| Biologics 4 | −0.05 | 0.765 | 0.07 | 0.686 |
| Multivariable-adjusted 5 | ||||
| Employment (working) 3 | −0.35 | 0.017 | −0.27 | 0.093 |
| Immunosuppressives 4 | −0.39 | 0.008 | – | – |
| Treatment Adherence (Self-Reported): Highest to Lowest | ||||
|---|---|---|---|---|
| 0–1 | 2 | 3–4 | p-Value 1 | |
| Anxiety level | ||||
| No or low | 13 (68.4%) | 6 (31.6%) | 0 (0.0%) | |
| Moderate or severe 2 | 8 (38.1%) | 8 (38.1%) | 5 (23.8%) | 0.041 |
| Depression level | ||||
| No or low | 18 (58.1%) | 11 (35.5%) | 2 (6.5%) | 0.088 |
| Moderate or severe 3 | 3 (33.3%) | 3 (33.3%) | 3 (33.3%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikoloudaki, M.; Repa, A.; Pitsigavdaki, S.; Molla Ismail Sali, A.; Sidiropoulos, P.; Lionis, C.; Bertsias, G. Persistence of Depression and Anxiety despite Short-Term Disease Activity Improvement in Patients with Systemic Lupus Erythematosus: A Single-Centre, Prospective Study. J. Clin. Med. 2022, 11, 4316. https://doi.org/10.3390/jcm11154316
Nikoloudaki M, Repa A, Pitsigavdaki S, Molla Ismail Sali A, Sidiropoulos P, Lionis C, Bertsias G. Persistence of Depression and Anxiety despite Short-Term Disease Activity Improvement in Patients with Systemic Lupus Erythematosus: A Single-Centre, Prospective Study. Journal of Clinical Medicine. 2022; 11(15):4316. https://doi.org/10.3390/jcm11154316
Chicago/Turabian StyleNikoloudaki, Myrto, Argyro Repa, Sofia Pitsigavdaki, Ainour Molla Ismail Sali, Prodromos Sidiropoulos, Christos Lionis, and George Bertsias. 2022. "Persistence of Depression and Anxiety despite Short-Term Disease Activity Improvement in Patients with Systemic Lupus Erythematosus: A Single-Centre, Prospective Study" Journal of Clinical Medicine 11, no. 15: 4316. https://doi.org/10.3390/jcm11154316
APA StyleNikoloudaki, M., Repa, A., Pitsigavdaki, S., Molla Ismail Sali, A., Sidiropoulos, P., Lionis, C., & Bertsias, G. (2022). Persistence of Depression and Anxiety despite Short-Term Disease Activity Improvement in Patients with Systemic Lupus Erythematosus: A Single-Centre, Prospective Study. Journal of Clinical Medicine, 11(15), 4316. https://doi.org/10.3390/jcm11154316