
Evaluating the Roles of Different Types of Laser Therapy in Becker’s Nevus Treatment

 , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Treatment Protocol
2.3. Randomization
2.4. Efficacy Evaluation
- The visual analogue scale (VAS), scored from 0 to 10, represented increasing levels of lesional hyperpigmentation and was used to assess the level of lesional pigmentation and monitor the improvement following therapy. The grade of hyperpigmentation for each part of the lesion was recorded at the baseline, at the end of the last session, and for the follow-up period. A score of (0) indicated that lesion color was close to the color of the surrounding nonlesional skin, while a score of (10) meant the lesion color was extremely dark brown.
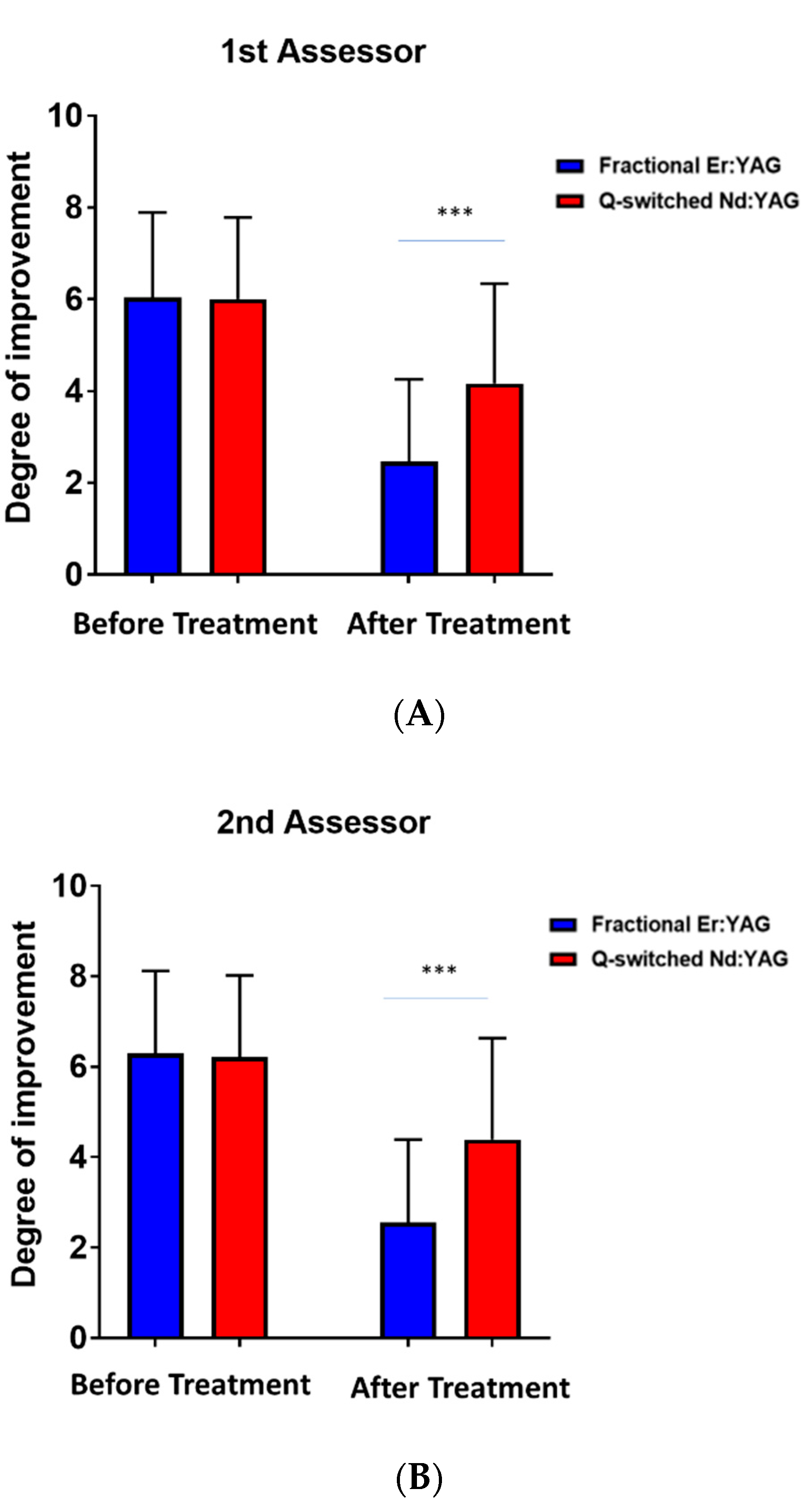
- The degree of improvement was evaluated using a six-point scale, where failure = 0% improvement, mild = 1–25% improvement, moderate = 26–50% improvement, good = 51–75% improvement, excellent = 76–99% improvement, and perfect = 100% improvement
- The degree of repigmentation was examined using a five-point scale: Grade 1 (no repigmentation), Grade 2 (mild (1–39%) repigmentation), Grade 3 (moderate (40–69%) repigmentation), Grade 4 (severe (70–100%) repigmentation), and Grade 5 (worsening of hyperpigmentation)
3. Results
3.1. Grade of Improvement
3.2. Degree of Improvement
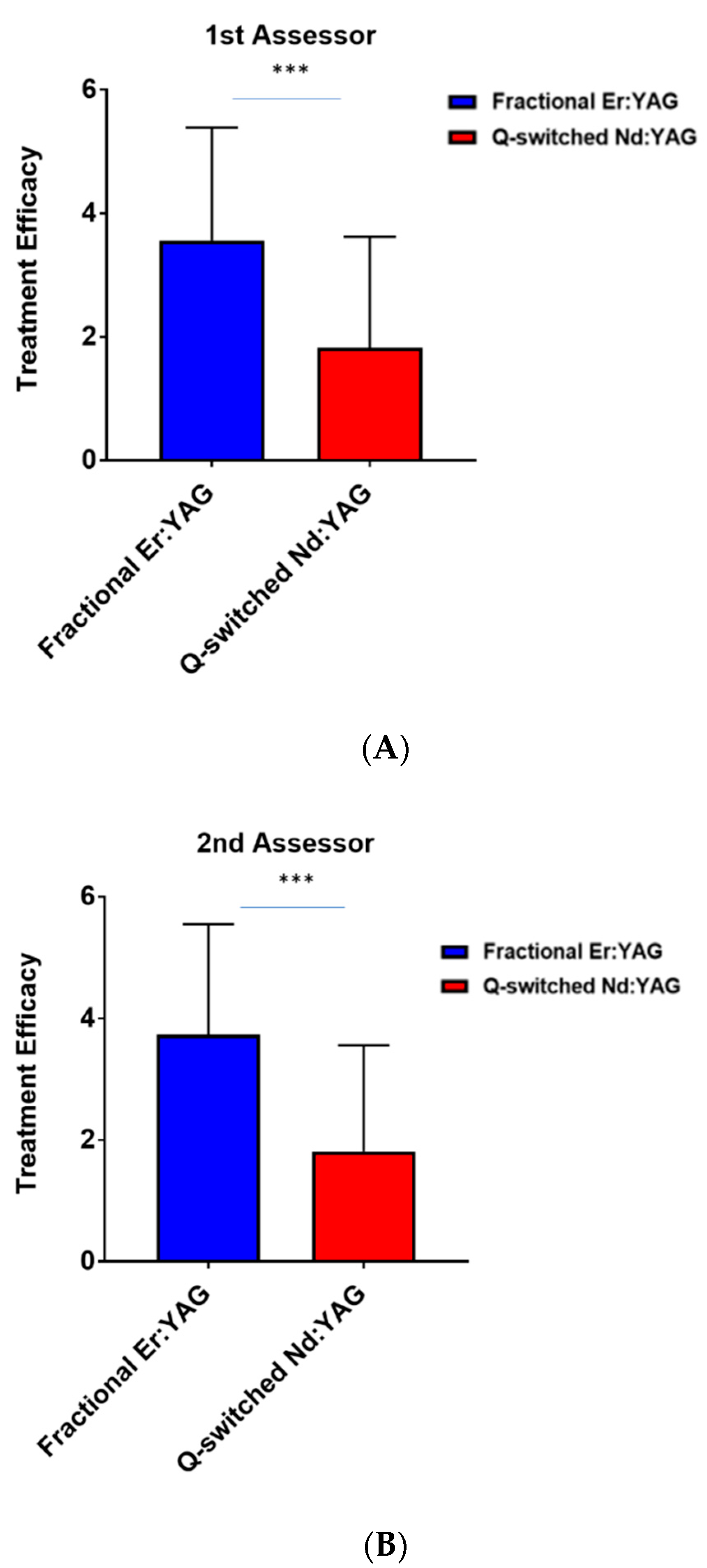
3.3. Efficacy of Treatment
3.4. Patient Satisfaction
3.5. Side Effects
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barnhill, R.L.; Vernon, S.; Rabinovitz, H.S. Benign Melanocytic Neoplasms. In Color Atlas of Dermatopathology; Informa Healthcare USA, Inc.: New York, NY, USA, 2007; pp. 247–278. [Google Scholar]
- Elder, D. Benign Pigmented Lesions and Malignant Melanoma. Lever’s Histopathology of the Skin; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1997; pp. 625–684. [Google Scholar]
- Rasi, A.; Berenji Ardestani, H.; Tabaie, S.M. Hypertrichosis is not so prevalent in Becker’s nevus: Analysis of 47 cases. Int. Sch. Res. Not. 2014, 2014, 953747. [Google Scholar] [CrossRef] [PubMed]
- Kinsler, V.A.; Sebire, N.J. Congenital Naevi and Other Developmental Abnormalities Affecting the Skin. Rook’s Textbook of Dermatology, 9th ed.; Wiley: Hoboken, NJ, USA, 2016; pp. 1–28. [Google Scholar]
- Book, S.; Glass, A.; Laude, T. Congenital Becker’s nevus with a familial association. Pediatric Dermatol. 1997, 14, 373–375. [Google Scholar] [CrossRef] [PubMed]
- Danarti, R.; König, A.; Salhi, A.; Bittar, M.; Happle, R. Becker’s nevus syndrome revisited. J. Am. Acad. Dermatol. 2004, 51, 965–969. [Google Scholar] [CrossRef] [PubMed]
- Happle, R.; Koopman, R.J. Becker nevus syndrome. Am. J. Med. Genet. 1997, 68, 357–361. [Google Scholar] [CrossRef]
- Patrizi, A.; Medri, M.; Raone, B.; Bianchi, F.; Aprile, S.; Neri, I. Clinical Characteristics of Becker’s Nevus in Children: Report of 118 Cases from Italy. Pediatr. Dermatol. 2012, 29, 571–574. [Google Scholar] [CrossRef]
- Becker, S.W. Concurrent melanosis and hypertrichosis in Distribution of Nevus Unius Lateris. Arch. Dermatol. 1949, 60, 155–160. [Google Scholar] [CrossRef]
- Nanni, C.A.; Alster, T.S. Case Report: Treatment of a Becker’s Nevus Using a 694-ntn Long-pulsed Ruby Laser. Dermatol. Surg. 1998, 24, 1032–1034. [Google Scholar] [CrossRef]
- Kim, H.W.; Seo, Y.J.; Lee, J.H.; Park, J.K.; Nam, I.H. Treatment of a Becker’s Nevus Using a Q-Switched ND: YAG Laser. Korean J. Dermatol. 2004, 392–397. [Google Scholar]
- Zachary, C.; Kelly, K. Lasers and Other Energy-Based Therapies. In Dermatology, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2018; p. 2364. [Google Scholar]
- Fritz, K.; Salavastru, C. Laser treatment of pigmentation disorders. Z. Dermatol. Venerol. Verwandte Geb. 2020, 71, 920–925. [Google Scholar]
- Maloney, M. Management of Surgical Complications and Suboptimal Results. In Cutaneous Surgery; WB Saunders Co.: Philadelphia, PA, USA, 1994; pp. 921–934. [Google Scholar]
- Tedeschi, A.; Dall’Oglio, F.; Micali, G.; Schwartz, R.A.; Janniger, C. Corrective camouflage in pediatric dermatology. Cutis 2007, 79, 110–112. [Google Scholar]
- Momen, S.; Mallipeddi, R.; Al-Niaimi, F. The use of lasers in Becker’s naevus: An evidence-based review. J. Cosmet. Laser Ther. 2016, 18, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Roh, M.R.; Lee, J.H.; Na, J.I.; Ko, J.Y.; Jung, J.M.; Lee, J.H.; Chang, S.E. Clinicopathologic characteristics of early-onset Becker’s nevus in Korean children and adolescents. Int. J. Dermatol. 2018, 57, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Asilian, A.; Hafezi, H.; Shahmoradi, Z.; Faghihi, G.; Siadat, A.H.; Mozafarpoor, S.; Mohaghegh, F.; Nasimi, M.; Talakoub, M. Q-switched Ruby laser alone or in combination with topical flutamide for the treatment of Becker nevus syndrome; a randomized clinical trial. Iran. J. Dermatol. 2021, 24, 11–17. [Google Scholar] [CrossRef]
- Carroll, L.; Humphreys, T.R. LASER-tissue interactions. Clin. Dermatol. 2006, 24, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, I.; Aoki, A.; Takasaki, A.A. Clinical application of erbium: YAG laser in periodontology. J. Int. Acad. Periodontol. 2008, 10, 22–30. [Google Scholar]
- Manstein, D.; Herron, G.S.; Sink, R.K.; Tanner, H.; Anderson, R.R. Fractional Photothermolysis: A New Concept for Cutaneous Remodeling Using Microscopic Patterns of Thermal Injury. Lasers Surg. Med. 2004, 34, 426–438. [Google Scholar] [CrossRef]
- Nanni, C.A.; Alster, T.S. A practical review of laser-assisted hair removal using the Q-switched Nd: YAG, long-pulsed ruby, and long-pulsed alexandrite lasers. Dermatol. Surg. 1998, 24, 1399–1405. [Google Scholar] [CrossRef]
- Nanni, C.A.; Alster, T.S. Laser-assisted hair removal: Side effects of Q-switched Nd: YAG, long-pulsed ruby, and alexandrite lasers. J. Am. Acad. Dermatol. 1999, 41, 165–171. [Google Scholar] [CrossRef]
- Aurangabadkar, S. Optimizing Q-switched lasers for melasma and acquired dermal melanoses. Indian J. Dermatol. Venereol. Leprol. 2019, 85, 10–17. [Google Scholar] [CrossRef]
- Mun, J.Y.; Jeong, S.Y.; Kim, J.; Han, S.S.; Kim, I.-H. A low fluence Q-switched Nd:YAG laser modifies the 3D structure of melanocyte and ultrastructure of melanosome by subcellular-selective photothermolysis. QJM Int. J. Med. 2010, 60, 11–18. [Google Scholar] [CrossRef]
- Goldberg, D.J. Laser Treatment of Pigmented Lesions. Dermatol. Clin. 1997, 15, 397–407. [Google Scholar] [CrossRef]
- Hruza, G.J. Q-switched ruby laser irradiation of normal human skin. Histologic and ultrastructural findings. Arch. Dermatol. 1991, 127, 1799–1805. [Google Scholar] [CrossRef] [PubMed]
- Landthaler, M.; Brunner, R.; Haina, D.; Frank, F.; Waidelich, W.; Braun-Falco, O. First Experiences with the Nd: YAG Laser in Dermatology. In Neodymium-YAG Laser in Medicine and Surgery; Elsevier: New York, NY, USA, 1983; pp. 175–183. [Google Scholar]
- Anderson, R.R.; Margolis, R.J.; Watenabe, S.; Flotte, T.; Hruza, G.J.; Dover, J.S. Selective Photothermolysis of Cutaneous Pigmentation by Q-switched Nd: YAG Laser Pulses at 1064, 532. and 355 nm. J. Investig. Dermatol. 1989, 93, 28–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trelles, M.A.; Allones, I.; Moreno-Arias, G.A.; Vélez, M. Becker’s naevus: A comparative study between erbium: YAG and Q-switched neodymium: YAG; clinical and histopathological findings. Br. J. Dermatol. 2005, 152, 308–313. [Google Scholar] [CrossRef]
- Trelles, M.A.; Allones, I.; Vélez, M.; Moreno-Arias, G.A. Becker’s nevus: Erbium: YAG versus Q-switched neodimium: YAG? Lasers Surg. Med. 2004, 34, 295–297. [Google Scholar] [CrossRef] [PubMed]
- Al-Saif, F.; Al-Mekhadab, E.; Al-Saif, H. Efficacy and safety of short-pulse erbium: Yttrium aluminum garnet laser treatment of Becker’s nevus in Saudi patients: A pilot study. Int. J. Health Sci. 2017, 11, 14–17. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Range | Mean | |
|---|---|---|---|
| Age/years | 10–58 | 23.65 ± 10.86 | |
| Age of onset/years | 7–14 | 10.86 ± 2.04 | |
| Number | Percent | ||
| Age group/years | <20 | 9 | 39.13% |
| 20–40 | 12 | 52.17% | |
| >40 | 2 | 8.69% | |
| Gender | Male | 8 | 34.78% |
| Female | 15 | 65.21% | |
| Residency | Urban | 21 | 91.30% |
| Rural | 2 | 8.69% | |
| Skin types | Type III | 10 | 43.47% |
| Type IV | 13 | 56.5% | |
| Lesion Characteristics | Number | Percent | |
|---|---|---|---|
| Lesion localization | Face | 3 | 13.04% |
| Neck | 1 | 4.37% | |
| Upper trunk | 6 | 26.08% | |
| Upper extremity | 3 | 13.04% | |
| Lower extremity | 1 | 4.37% | |
| Upper trunk with upper extremity | 9 | 39.13% | |
| Lesion color | Light brown | 3 | 13.04% |
| Moderate brown | 11 | 47.82% | |
| Dark brown | 7 | 30.43% | |
| Extremely dark brown | 2 | 8.69% | |
| Hypertrichosis | Positive | 6 | 26.08% |
| Negative | 17 | 73.91% | |
| Hair density | Mild | 4 | 17.39% |
| Moderate | 1 | 4.37% | |
| Marked | 1 | 4.37% | |
| Associated acneiform lesions | Positive | 2 | 8.69% |
| Negative | 21 | 91.30% | |
| Previous treatment | Laser (before 1 year) | 5 | 21.73% |
| Topical therapy (before 6 months) | 2 | 8.69% | |
| None | 16 | 69.56% | |
| Grade of Improvement | After Treatment | p Value | |
|---|---|---|---|
| Fractional Er:YAG (2940 nm) No. (%) | Q-Switched Nd:YAG (1064 nm) No. (%) | ||
| Failure (0%) | 0 (0%) | 8 (34.78%) | 0.001 |
| Mild (1–25%) | 5 (21.79%) | 4 (17.39%) | |
| Moderate (26–50%) | 3 (13.04%) | 6 (26.08%) | |
| Good (51–75%) | 8 (34.78%) | 2 (8.69%) | |
| Excellent (76–99%) | 3 (13.04%) | 3 (13.04%) | |
| Perfect (100%) | 4 (17.39%) | 0 (0%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Bakaa, M.K.; Al-Dhalimi, M.A.; Dube, P.; Khalaf, F.K. Evaluating the Roles of Different Types of Laser Therapy in Becker’s Nevus Treatment. J. Clin. Med. 2022, 11, 4230. https://doi.org/10.3390/jcm11144230
Al-Bakaa MK, Al-Dhalimi MA, Dube P, Khalaf FK. Evaluating the Roles of Different Types of Laser Therapy in Becker’s Nevus Treatment. Journal of Clinical Medicine. 2022; 11(14):4230. https://doi.org/10.3390/jcm11144230
Chicago/Turabian StyleAl-Bakaa, Muhammad K., Muhsin A. Al-Dhalimi, Prabhatchandra Dube, and Fatimah K. Khalaf. 2022. "Evaluating the Roles of Different Types of Laser Therapy in Becker’s Nevus Treatment" Journal of Clinical Medicine 11, no. 14: 4230. https://doi.org/10.3390/jcm11144230
APA StyleAl-Bakaa, M. K., Al-Dhalimi, M. A., Dube, P., & Khalaf, F. K. (2022). Evaluating the Roles of Different Types of Laser Therapy in Becker’s Nevus Treatment. Journal of Clinical Medicine, 11(14), 4230. https://doi.org/10.3390/jcm11144230