
Levosimendan as a “Bridge to Optimization” in Patients with Advanced Heart Failure with Reduced Ejection—A Single-Center Study

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
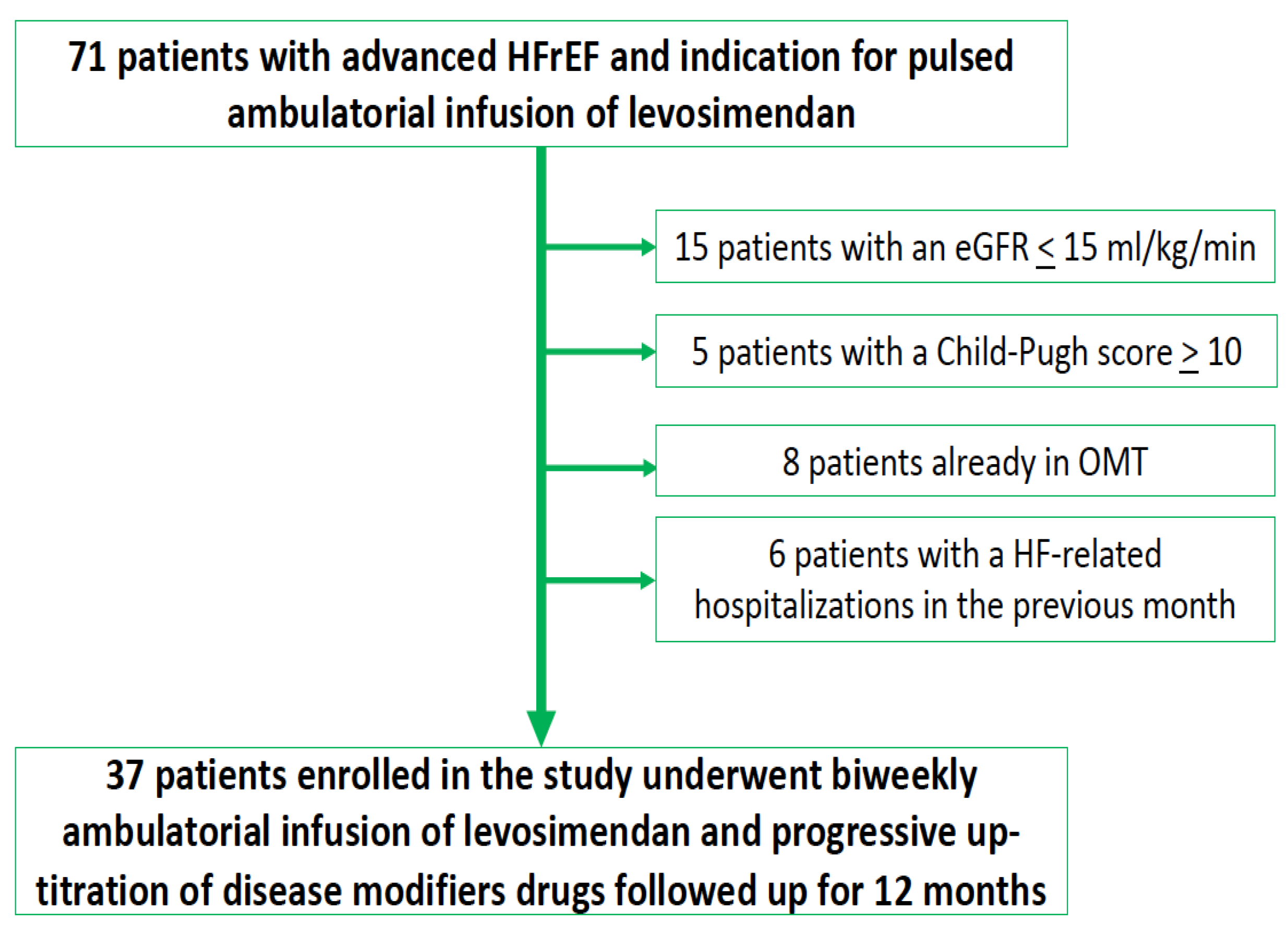
2.1. Study Population
- (1)
- HFrEF with a left ventricular ejection fraction <35%,
- (2)
- NYHA class III-IV,
- (3)
- NT-proBNP >2500 pg/mL,
- (4)
- walking distance at 6-min walking test <300 m,
- (5)
- indication for intermittent ambulatory levosimendan infusion due to episodes of pulmonary or systemic congestion requiring a high dose i.v. diuretics or episodes of low output requiring inotropes or causing >2 unplanned visits or hospitalisations in the last 12 months, and
- (6)
- (1)
- End-stage renal disease (i.e., estimated glomerular filtration rate <15 mL/kg/min according to the CKD-EPI equation),
- (2)
- severe liver impairment (i.e., Child–Pugh score >10).
2.2. Levosimendan Infusion
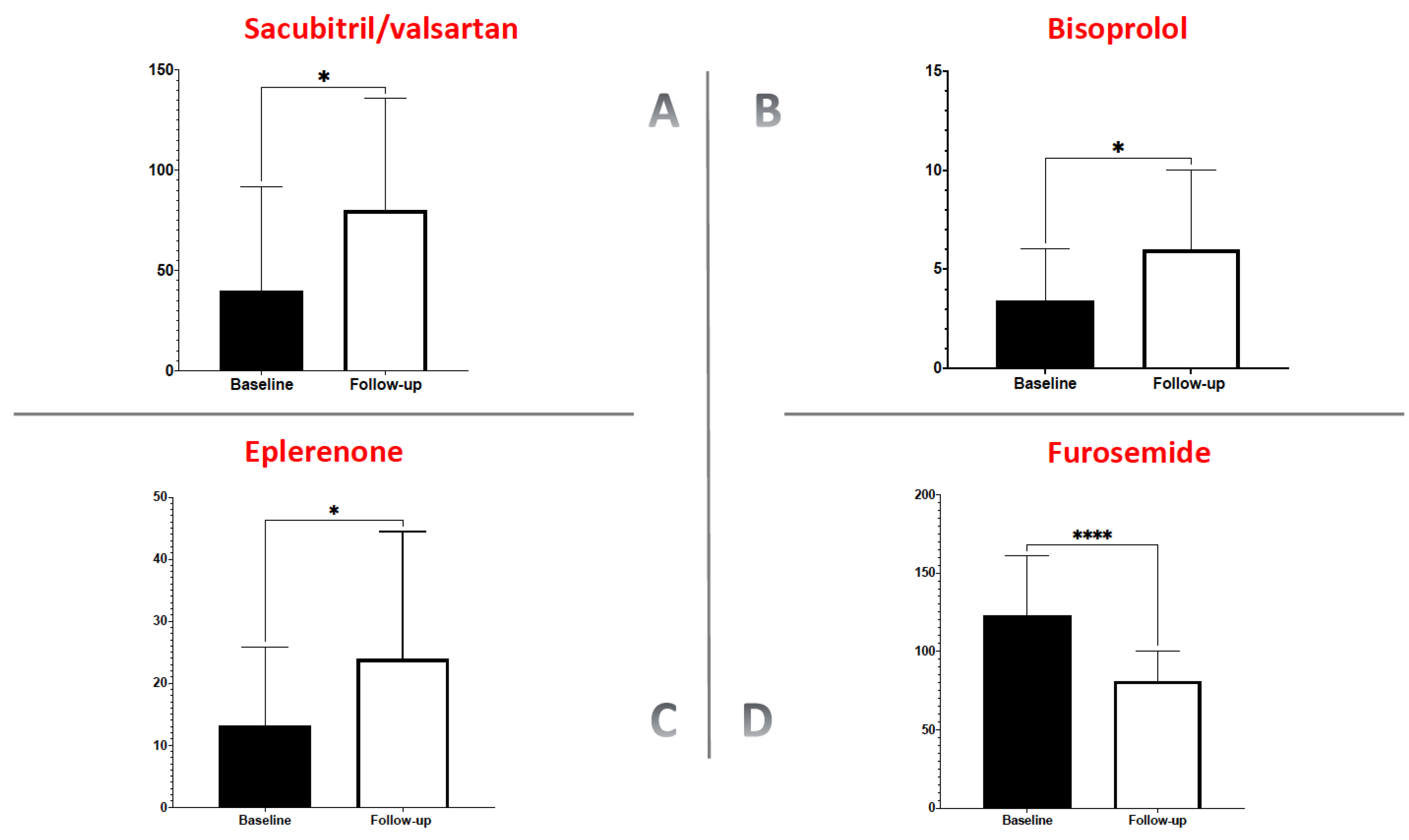
2.3. Evaluation of Disease Modifiers Drug Dose
2.4. Statistical Analysis
3. Results
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Truby, L.K.; Rogers, J.G. Advanced Heart Failure: Epidemiology, Diagnosis, and Therapeutic Approaches. JACC Heart Fail. 2020, 8, 523–536. [Google Scholar] [CrossRef]
- Masarone, D.; Kittleson, M.; Petraio, A.; Pacileo, G. Advanced heart failure: State of the art and future directions. Rev. Cardiovasc. Med. 2022, 23, 48. [Google Scholar] [CrossRef]
- Iacoviello, M.; Vitale, E.; Corbo, M.D.; Correale, M.; Brunetti, N.D. Disease-modifier Drugs in Patients with Advanced Heart Failure: How to Optimize Their Use? Heart Fail. Clin. 2021, 17, 561–573. [Google Scholar] [CrossRef]
- Masarone, D.; Melillo, E.; Gravino, R.; Errigo, V.; Martucci, M.L.; Caiazzo, A.; Petraio, A.; Pölzl, G.; Pacileo, G. Inotropes in Patients with Advanced Heart Failure: Not Only Palliative Care. Heart Fail. Clin. 2021, 17, 587–598. [Google Scholar] [CrossRef]
- Long, Y.X.; Cui, D.Y.; Kuang, X.; Hu, S.; Hu, Y.; Liu, Z.Z. Effect of Levosimendan on Ventricular Systolic and Diastolic Functions in Heart Failure Patients: A Meta-Analysis of Randomized Controlled Trials. J. Cardiovasc. Pharmacol. 2021, 77, 805–813. [Google Scholar] [CrossRef]
- Mavrogeni, S.; Giamouzis, G.; Papadopoulou, E.; Thomopoulou, S.; Dritsas, A.; Athanasopoulos, G.; Adreanides, E.; Vassiliadis, I.; Spargias, K.; Panagiotakos, D.; et al. A 6-month follow-up of intermittent levosimendan administration effect on systolic function, specific activity questionnaire, and arrhythmia in advanced heart failure. J. Card. Fail. 2007, 13, 556–559. [Google Scholar] [CrossRef]
- Parissis, J.T.; Adamopoulos, S.; Farmakis, D.; Filippatos, G.; Paraskevaidis, I.; Panou, F.; Iliodromitis, E.; Kremastinos, D.T. Effects of serial levosimendan infusions on left ventricular performance and plasma biomarkers of myocardial injury and neurohormonal and immune activation in patients with advanced heart failure. Heart 2006, 92, 1768–1772. [Google Scholar] [CrossRef][Green Version]
- Comín-Colet, J.; Manito, N.; Segovia-Cubero, J.; Delgado, J.; Pinilla, J.M.G.; Almenar, L.; Crespo-Leiro, M.G.; Sionis, A.; Blasco, T.; Pascual-Figal, D.; et al. Efficacy and safety of intermittent intravenous outpatient administration of levosimendan in patients with advanced heart failure: The LION-HEART multicentre randomised trial. Eur. J. Heart Fail. 2018, 20, 1128–1136. [Google Scholar] [CrossRef]
- Masarone, D.; Melillo, E.; Errigo, V.; Martucci, M.L.; Pacileo, R.; Pollesello, P.; Petraio, A.; Pacileo, G. Hemodynamic Effects of Levosimendan in Outpatients With Advanced Heart Failure: An Echocardiographic Pilot Study. J. Cardiovasc. Pharmacol. 2021, 79, e36–e40. [Google Scholar] [CrossRef]
- Apostolo, A.; Vignati, C.; Della Rocca, M.; De Martino, F.; Berna, G.; Campodonico, J.; Contini, M.; Muratori, M.; Palermo, P.; Mapelli, M.; et al. Why Levosimendan Improves the Clinical Condition of Patients With Advanced Heart Failure: A Holistic Approach. J. Card. Fail. 2021, 28, 509–514. [Google Scholar] [CrossRef]
- Masarone, D.; Valente, F.; Verrengia, M.; Ammendola, E.; Gravino, R.; D’Alterio, G.; Petraio, A.; Pacileo, G. Efficacy and safety of repeated infusion of levosimendan in outpatients with advanced heart failure: A real-world experience. J. Cardiovasc. Med. 2020, 21, 919–921. [Google Scholar] [CrossRef]
- Oliva, F.; Perna, E.; Marini, M.; Nassiacos, D.; Cirò, A.; Malfatto, G.; Morandi, F.; Caico, I.; Perna, G.; Meloni, S.; et al. Scheduled intermittent inotropes for Ambulatory Advanced Heart Failure. The RELEVANT-HF multicentre collaboration. Int. J. Cardiol. 2018, 272, 255–259. [Google Scholar] [CrossRef]
- Berger, R.; Moertl, D.; Huelsmann, M.; Bojic, A.; Ahmadi, R.; Heissenberger, I.; Pacher, R. Levosimendan and prostaglandin E1 for uptitration of beta-blockade in patients with refractory, advanced chronic heart failure. Eur. J. Heart Fail. 2007, 9, 202–208. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Rosano, G.M.; Moura, B.; Metra, M.; Böhm, M.; Bauersachs, J.; Ben Gal, T.; Adamopoulos, S.; Abdelhamid, M.; Bistola, V.; Čelutkienė, J.; et al. Patient profiling in heart failure for tailoring medical therapy. A consensus document of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2021, 23, 872–881. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef]
- Ameri, P.; Bertero, E.; Maack, C.; Teerlink, J.R.; Rosano, G.; Metra, M. Medical treatment of heart failure with reduced ejection fraction: The dawn of a new era of personalized treatment? Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, 539–546. [Google Scholar] [CrossRef]
- Komajda, M.; Follath, F.; Swedberg, K.; Cleland, J.; Aguilar, J.; Cohen-Solal, A.; Dietz, R.; Gavazzi, A.; van Gilst, W.; Hobbs, R.; et al. The EuroHeart Failure Survey programme--a survey on the quality of care among patients with heart failure in Europe. Part 2: Treatment. Eur. Heart J. 2003, 24, 464–474. [Google Scholar] [CrossRef]
- Crespo-Leiro, M.G.; Barge-Caballero, E. Advanced Heart Failure: Definition, Epidemiology, and Clinical Course. Heart Fail. Clin. 2021, 17, 533–545. [Google Scholar] [CrossRef]
- Caira, C.; Brasolin, B.; Maestrini, V.; Scardala, R.; Orvieto, G.; Mancone, M.; Fedele, F. 475 Effects of Levosimendan on renal function and renal hemodynamic parameters in patients with acute heart failure. Eur. J. Heart Fail. Suppl. 2007, 6, 103. [Google Scholar] [CrossRef]
- Zemljic, G.; Bunc, M.; Yazdanbakhsh, A.P.; Vrtovec, B. Levosimendan Improves Renal Function in Patients With Advanced Chronic Heart Failure Awaiting Cardiac Transplantation. J. Card. Fail. 2007, 13, 417–421. [Google Scholar] [CrossRef]
- Nieminen, M.S.; Akkila, J.; Hasenfuss, G.; Kleber, F.X.; Lehtonen, L.A.; Mitrovic, V.; Nyquist, O.; Remme, W.J. Hemodynamic and neurohumoral effects of continuous infusion of levosimendan in patients with congestive heart failure. J. Am. Coll. Cardiol. 2000, 36, 1903–1912. [Google Scholar] [CrossRef]
- Mcmurray, J.J.V.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure. PARADIGM-HF Investigators and Committees. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef]
- Masarone, D.; Melillo, E.; Errigo, V.; Valente, F.; Pacileo, G. Clinical relevance of transient worsening renal function after initiation of sacubitril/valsartan. Curr. Med. Res. Opin. 2020, 37, 9–12. [Google Scholar] [CrossRef]
- Wang, T.-D.; Tan, R.S.; Lee, H.-Y.; Ihm, S.-H.; Rhee, M.-Y.; Tomlinson, B.; Pal, P.; Yang, F.; Hirschhorn, E.; Prescott, M.F.; et al. Effects of Sacubitril/Valsartan (LCZ696) on Natriuresis, Diuresis, Blood Pressures, and NT-proBNP in Salt-Sensitive Hypertension. Hypertension 2017, 69, 32–41. [Google Scholar] [CrossRef]
- Pontremoli, R.; Borghi, C.; Filardi, P.P. Renal protection in chronic heart failure: Focus on sacubitril/valsartan. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, 445–452. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Total Population (n = 37) |
|---|---|
| Age (mean ± SD) | 55.8 ± 13.2 years |
| Female sex (n, %) | 6 (16%) |
| Ischaemic (n, %) | 20 (54%) |
| Hypertension (n, %) | 18 (48%) |
| Diabetes (n, %) | 17 (45%) |
| COPD (n, %) | 12 (32%) |
| NYHA class III (n, %) | 25 (67%) |
| NYHA class IV (n, %) | 12 (33%) |
| SBP (mean ± SD) | 97 ± 10 mmHg |
| DBP (mean ± SD) | 62 ± 8 mmHg |
| NT-pro BNP (mean ± SD) | 3448 ± 1187 pg/mL |
| Atrial fibrillation | 15 (40%) |
| Hb (mean ± SD) | 11.7 ± 1.8 g/dL |
| Creatinine (mean ± SD) | 1.4 ± 1.3 mg/dL |
| eGFR (mean ± SD) | 36.7 ± 18.1 mL/min/1.73 m2 |
| LVEDV (mean ± SD) | 2321.2 ± 85.9 mL |
| LVESV (mean ± SD) | 192.7 ± 80.2 mL |
| LVEF (mean ± SD) | 26.8 ± 9.4% |
| E wave (mean ± SD) | 128.1 ± 39.5 cm/s |
| e’ average (mean ± SD) | 6.9 ± 3.5 cm/s |
| E/e’ average (mean ± SD) | 21.2 ± 6.3 |
| DecT (mean ± SD) | 165.2 ± 28.3 m/s |
| LAVi (mean ± SD) | 52.5 ± 13.5 mL/m2 |
| PASP (mean ± SD) | 40.8 ± 12.6 mmHg |
| TAPSE (mean ± SD) | 14.1 ± 5.4 mm |
| Peak systolic s wave (mean ± SD) | 8.7 ± 3.2 cm/s |
| Loop diuretic (n, %) | 37 (100%) |
| Furosemide dose (mean ± SD) | 123.2 ± 32.48 mg |
| β-blocker (n, %) | 37 (100 %) |
| Bisoprolol dose (mean ± SD) | 3.2 ± 2.8 mg |
| ARNI (n, %) | 37 (100%) |
| ARNI dose (mean ± SD) | 41.67 ± 32.48 mg |
| MRA (n, %) | 37 (100%) |
| Eplerenone dose | 9.7 ± 8.8 mg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masarone, D.; Kittleson, M.M.; Martucci, M.L.; Valente, F.; Gravino, R.; Verrengia, M.; Ammendola, E.; Contaldi, C.; Di Palma, V.; Caiazzo, A.; et al. Levosimendan as a “Bridge to Optimization” in Patients with Advanced Heart Failure with Reduced Ejection—A Single-Center Study. J. Clin. Med. 2022, 11, 4227. https://doi.org/10.3390/jcm11144227
Masarone D, Kittleson MM, Martucci ML, Valente F, Gravino R, Verrengia M, Ammendola E, Contaldi C, Di Palma V, Caiazzo A, et al. Levosimendan as a “Bridge to Optimization” in Patients with Advanced Heart Failure with Reduced Ejection—A Single-Center Study. Journal of Clinical Medicine. 2022; 11(14):4227. https://doi.org/10.3390/jcm11144227
Chicago/Turabian StyleMasarone, Daniele, Michelle M. Kittleson, Maria L. Martucci, Fabio Valente, Rita Gravino, Marina Verrengia, Ernesto Ammendola, Carla Contaldi, Vito Di Palma, Angelo Caiazzo, and et al. 2022. "Levosimendan as a “Bridge to Optimization” in Patients with Advanced Heart Failure with Reduced Ejection—A Single-Center Study" Journal of Clinical Medicine 11, no. 14: 4227. https://doi.org/10.3390/jcm11144227
APA StyleMasarone, D., Kittleson, M. M., Martucci, M. L., Valente, F., Gravino, R., Verrengia, M., Ammendola, E., Contaldi, C., Di Palma, V., Caiazzo, A., Petraio, A., Pollesello, P., & Pacileo, G. (2022). Levosimendan as a “Bridge to Optimization” in Patients with Advanced Heart Failure with Reduced Ejection—A Single-Center Study. Journal of Clinical Medicine, 11(14), 4227. https://doi.org/10.3390/jcm11144227