
Far and Near Contrast Sensitivity and Quality of Vision with Six Presbyopia Correcting Intraocular Lenses


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Intraocular Lenses
2.3. Surgical Technique
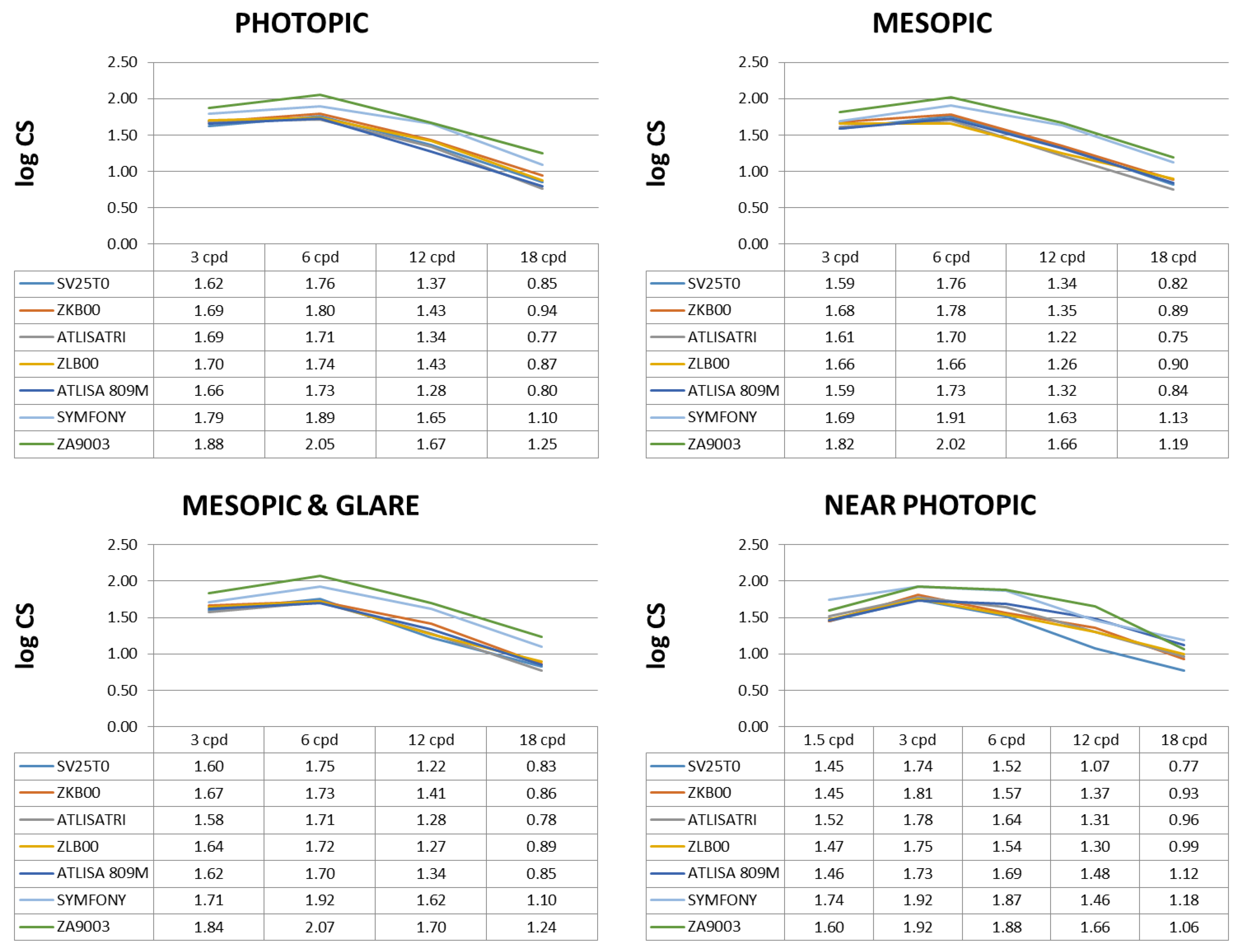
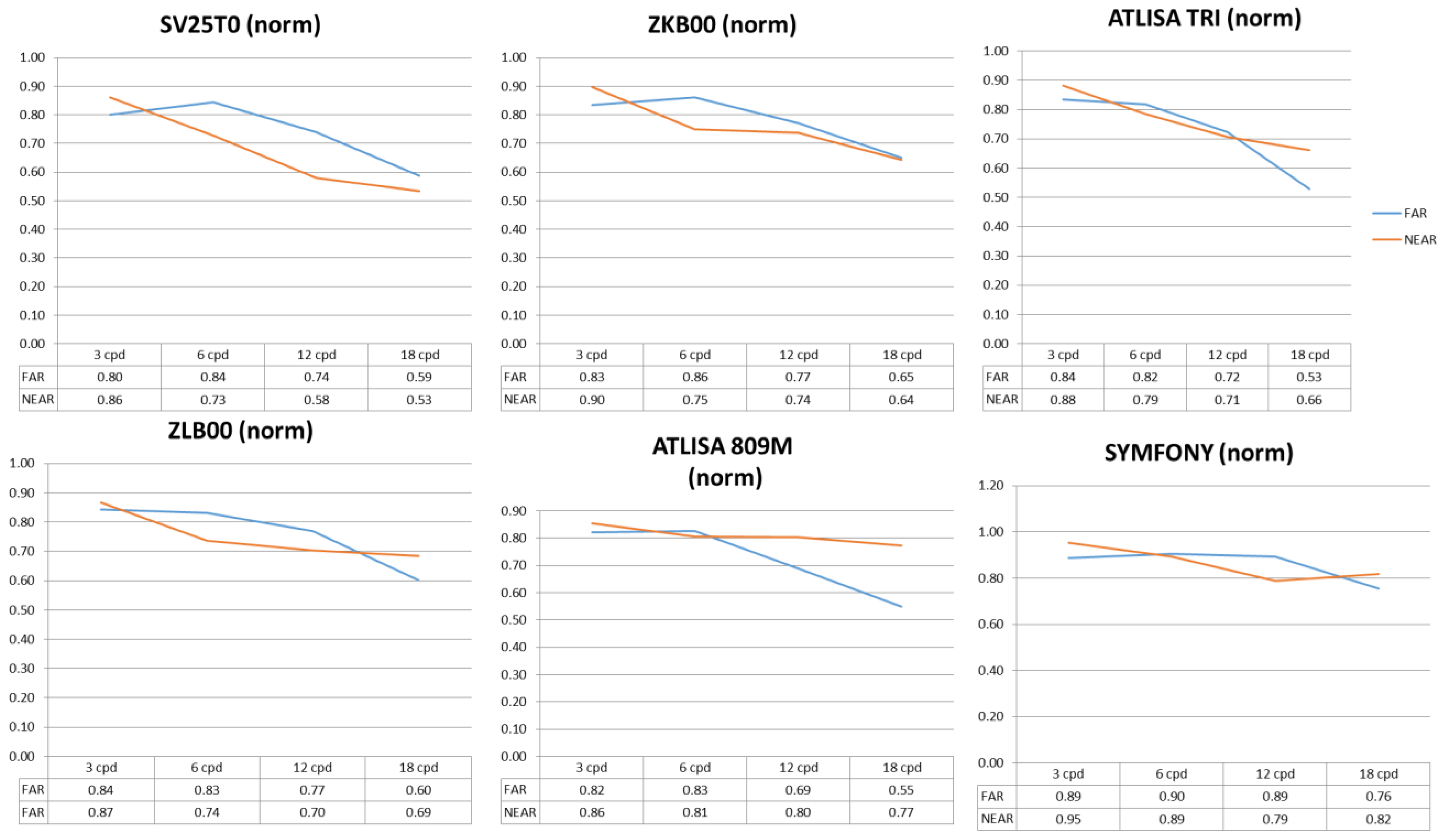
2.4. Contrast Sensitivity
2.5. Quality of Vision
2.6. Data Analysis
3. Results
3.1. Sample Demographics
3.2. Contrast Sensitivity
3.3. Quality of Vision
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ryan, C.; Lewis, J.M. Computer and Internet Use in the United States: 2015; U.S. Census Bureau: Suitland-Silver Hill, MD, USA, 2017. Available online: https://www.census.gov/content/dam/Census/library/publications/2017/acs/acs-37.pdf (accessed on 24 May 2022).
- Shieh, K.K.; Chen, M.T. Effects of screen color combination, work-break schedule, and workplace on VDT viewing distance. Int. J. Ind. Ergonom. 1997, 20, 11–18. [Google Scholar] [CrossRef]
- Hayashi, K.; Manabe, S.; Hayashi, H. Visual acuity from far to near and contrast sensitivity in eyes with a diffractive multifocal intraocular lens with low addition power. J. Cataract Refract. Surg. 2009, 35, 2070–2076. [Google Scholar] [CrossRef] [PubMed]
- Montés-Micó, R.; España, E.; Bueno, I.; Charman, W.N.; Menezo, J.L. Visual performance with multifocal intraocular lenses. Mesopic contrast sensitivity under distance and near conditions. Ophthalmology 2004, 111, 85–96. [Google Scholar] [CrossRef]
- Montés-Micó, R.; Alió, J.L. Distance and near contrast sensitivity function after multifocal intraocular lens implantation. J. Cataract Refract. Surg. 2003, 29, 703–711. [Google Scholar] [CrossRef]
- Martínez Palmer, A.; Gómez Faiña, P.; España Albelda, A.; Comas Serrano, M.; Nahra Saad, D.; Castilla Céspedes, M. Visual function with bilateral implantation of monofocal and multifocal intraocular lenses, a prospective, randomized, controlled trial. J. Refract. Surg. 2008, 24, 257–264. [Google Scholar]
- Alfonso, J.F.; Fernández-Vega, L.; Baamonde, M.B.; Montés–Micó, R. Correlation of pupil size with visual acuity and contrast sensitivity after implantation of an apodized diffractive intraocular lens. J. Cataract Refract. Surg. 2007, 33, 430–438. [Google Scholar] [CrossRef]
- Gil, M.A.; Varon, C.; Rosello, N.; Cardona, G.; Buil, J.A. Visual acuity, contrast sensitivity, subjective quality of vision, and quality of life with 4 different multifocal IOLs. Eur. J. Ophthalmol. 2012, 22, 175–187. [Google Scholar] [CrossRef]
- Alfonso, J.F.; Fernández-Vega, L.; Blázquez, J.I.; Montés–Micó, R. Visual function comparison of 2 aspheric multifocal intraocular lenses. J. Cataract Refract. Surg. 2012, 38, 242–248. [Google Scholar] [CrossRef]
- Mesci, C.; Erbil, H.; Ozdoker, L.; Karakurt, Y.; Bilge, A.D. Visual acuity and contrast sensitivity function after accommodative and multifocal intraocular lens implantation. Eur. J. Ophthalmol. 2010, 20, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Rocha, K.M. Extended depth of focus IOLs, The next chapter in refractive technology? J. Refract. Surg. 2017, 33, 146–149. [Google Scholar] [CrossRef] [Green Version]
- Savini, G.; Schiano-Lomoriello, D.; Balducci, N.; Barboni, P. Visual performance of a new extended depth-of-focus intraocular lens compared to a distance-dominant diffractive multifocal intraocular lens. J. Refract. Surg. 2018, 34, 228–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Mesa, R.; Abengózar-Vela, A.; Arumburu, A.; Ruiz-Santos, M. Comparison of visual outcomes after bilateral implantation of extended range of vision and trifocal intraocular lenses. Eur. J. Ophthalmol. 2017, 27, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Savini, G.; Balducci, N.; Carbonara, C.; Rossi, S.; Altieri, M.; Frugis, N.; Zappulla, E.; Bellucci, R.; Alessio, G. Functional assessment of a new extended depth-of-focus intraocular lens. Eye 2019, 33, 404–410. [Google Scholar] [CrossRef] [PubMed]
- MacRae, S.; Holladay, J.T.; Glasser, A.; Calogero, D.; Hilmantel, G.; Masket, S.; Stark, W.; Tarver, M.E.; Nguyen, T.; Eydelman, M. Special Report, American Academy of Ophthalmology Task Force Consensus Statement for Extended Depth of Focus Intraocular Lenses. Ophthalmology 2017, 124, 139–141. [Google Scholar] [CrossRef] [Green Version]
- Boxer Wachler, B.S.; Krueger, R.R. Normalized contrast sensitivity values. J. Refract. Surg. 1998, 14, 463–466. [Google Scholar] [CrossRef]
- Ginsburg, A.P. Contrast sensitivity and functional vision. Int. Ophthalmol. Clin. 2003, 43, 5–16. [Google Scholar] [CrossRef]
- De Vries, N.E.; Nuijts, R.M. Multifocal intraocular lenses in cataract surgery, literature review of benefits and side effects. J. Cataract Refract. Surg. 2013, 39, 268–278. [Google Scholar] [CrossRef]
- Garcia-Bella, J.; Ventura-Abreu, N.; Morales-Fernandez, L.; Talavero-González, P.; Carballo-Álvarez, J.; Sanz-Fernández, J.C.; Vázquez-Moliní, J.M.; Martínez-de-la-Casa, J.M. Visual outcomes after progressive apodized diffractive intraocular lens implantation. Eur. J. Ophthalmol. 2018, 28, 282–286. [Google Scholar] [CrossRef]
- Pedrotti, E.; Carones, F.; Aiello, F.; Mastropasqua, R.; Bruni, E.; Bonacci, E.; Talli, P.; Nucci, C.; Mariotti, C.; Marchini, G. Comparative analysis of visual outcomes with 4 intraocular lenses, monofocal, multifocal, and extended range of vision. J. Cataract Refract. Surg. 2018, 44, 156–167. [Google Scholar] [CrossRef]
- Escandon-Garcia, S.; Ribeiro, F.J.; McAlinden, C.; Queirós, A.; González-Méijome, J.M. Through-focus vision performance and light disturbances of 3 new intraocular lenses for presbyopia correction. J. Ophthalmol. 2018, 2018, 6165493. [Google Scholar] [CrossRef]
- Cillino, S.; Casuccio, A.; Di Pace, F.; Morreale, R.; Pillitteri, F.; Cillino, G.; Lodato, G. One-year outcomes with new-generation multifocal intraocular lenses. Ophthalmology 2008, 115, 1508–1516. [Google Scholar] [CrossRef]
- Maurino, V.; Allan, B.D.; Rubin, G.S.; Bunce, C.; Xing, W.; Findl, O. Quality of vision after bilateral multifocal intraocular lens implantation, a randomized trial––AT LISA 809M versus AcrySof ReSTOR SN6AD1. Ophthalmology 2015, 122, 700–710. [Google Scholar] [CrossRef] [PubMed]
- Kamlesh, S.; Dadeya, S.; Kaushik, S. Contrast sensitivity and depth of focus with aspheric multifocal versus conventional monofocal intraocular lens. Can. J. Ophthalmol. 2001, 36, 197–201. [Google Scholar] [CrossRef]
- Alfonso, J.F.; Puchades, C.; Fernandez–Vega, L.; Montés–Micó, R.; Valcárcel, B.; Ferrer–Blasco, T. Visual acuity comparison of 2 models of bifocal aspheric intraocular lenses. J. Cataract Refract. Surg. 2009, 35, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Vilar, C.; Hida, W.T.; de Medeiros, A.L.; Magalhaes, K.R.P.; de Moraes Tzelikis, P.F.; Chaves, M.A.P.D.; Motta, A.F.P.; Carricondo, P.C.; Alves, M.R.; Nosé, W. Comparison between bilateral implantation of a trifocal intraocular lens and blended implantation of two bifocal intraocular lenses. Clin. Ophthalmol. 2017, 11, 1393–1397. [Google Scholar] [CrossRef]
- Denoyer, A.; Le Lez, M.L.; Majzoub, S.; Pisella, P.J. Quality of vision after cataract surgery after Tecnis Z9000 intraocular lens implantation, effect of contrast sensitivity and wavefront aberration improvements on the quality of daily vision. J. Cataract Refract. Surg. 2007, 33, 210–216. [Google Scholar] [CrossRef]
- Tzelikis, P.F.; Akaishi, L.; Trindade, F.C.; Boteon, J.E. Spherical aberration and contrast sensitivity in eyes implanted with aspheric and spherical intraocular lenses, a comparative study. Am. J. Ophthalmol. 2008, 145, 827–833. [Google Scholar] [CrossRef]
- Sasaki, A. Initial experience with a refractive multifocal intraocular lens in a Japanese population. J. Cataract Refract. Surg. 2000, 26, 1001–1007. [Google Scholar] [CrossRef]
- Pomerance, G.N.; Evans, D.W. Test-retest reliability of the CSV-1000 contrast test and its relationship to glaucoma therapy. Investig. Ophthalmol. Vis. Sci. 1994, 35, 3357–3361. [Google Scholar]
- Mester, U.; Hunold, W.; Wesendahl, T.; Kaymak, H. Functional outcomes after implantation of Tecnis ZM900 and Array SA40 multifocal intraocular lenses. J. Cataract Refract. Surg. 2007, 33, 1033–1040. [Google Scholar] [CrossRef]
- Monaco, G.; Gari, M.; Di Censo, F.; Poscia, A.; Ruggi, G.; Scialdone, A. Visual performance after bilateral implantation of 2 new presbyopia-correcting intraocular lenses, Trifocal versus extended range of vision. J. Cataract Refract. Surg. 2017, 43, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Mendicute, J.; Kapp, A.; Lévy, P.; Krommes, G.; Arias–Puente, A.; Tomalla, M.; Barraquer, E.; Rozot, P.; Bouchut, P. Evaluation of visual outcomes and patient satisfaction after implantation of a diffractive trifocal intraocular lens. J. Cataract Refract. Surg. 2016, 42, 203–210. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| LENS | MANUFACTURER | ADD POWER (D) | SA (µm) | OPTICAL DESIGN |
|---|---|---|---|---|
| AcrySof ReSTOR SV25T0 | Alcon Laboratories, Fort Worth, TX, USA | +2.5 (n) | −0.20 | Bifocal, anterior aspheric apodized diffractive (3.4 mm) and refractive surface |
| Tecnis ZKB00 | Johnson and Johnson Surgical Vision, Santa Ana, CA | +2.75 (n) | −0.27 | Bifocal, anterior aspheric and posterior diffractive surface |
| Tecnis ZLB00 | +3.25 (n) | |||
| ATLISA 809M | Carl Zeiss Meditec AG, Jena, Germany | +3.75 (n) | −0.18 | Bifocal, aspheric diffractive |
| ATLISATri 839MP | +3.33 (n) +1.66 (i) | Trifocal, anterior surface with an aspheric diffractive profile | ||
| Tecnis Symfony ZXR00 | Johnson and Johnson Surgical Vision, Santa Ana, CA | ≈+1.75 (i) | −0.27 | Extended depth of focus, wavefront-designed anterior surface, posterior achromatic diffractive surface with echelette design |
| Tecnis ZA9003 | Johnson and Johnson Surgical Vision, Santa Ana, CA | - | −0.27 | Monofocal, anterior aspheric |
| SVT250 Bifocal | ZKB00 Bifocal | ZLB00 Bifocal | ATLISA 809M Bifocal | ATLISA Tri 839MP Trifocal | Symfony ZXR00 Extended Depth of Focus | ZA9003 Monofocal | p | |
|---|---|---|---|---|---|---|---|---|
| n (eyes) | 19 | 20 | 20 | 18 | 19 | 20 | 36 | |
| Age (years) | 74.3 ± 7.5 | 68.9 ± 12.9 | 73.3 ± 4.6 | 71.6 ± 7.1 | 68.7 ± 10.3 | 68.2 ± 6.2 | 72.1 ± 5.8 | 0.064 |
| Gender (male/female) | 8/11 | 5/15 | 7/13 | 4/14 | 4/15 | 5/15 | 15/21 | 0.428 |
| IOL power (D) | 21.3 ± 2.4 | 21.6 ± 3.4 | 22.3 ± 1.7 | 22.3 ± 2.4 | 21.9 ± 4.3 | 21.8 ± 5.7 | 21.0 ± 3.6 | 0.832 |
| Pupil diameter (mm) | 3.2 ± 0.6 | 3.4 ± 0.7 | 3.2 ± 0.7 | 3.0 ± 0.6 | 3.3 ± 0.8 | 3.3 ± 0.8 | 3.1 ± 0.7 | 0.768 |
| Spatial Frequency | SVT250 Bifocal | ZKB00 Bifocal | ZLB00 Bifocal | ATLISA 809M Bifocal | ATLISA Tri 839MP Trifocal | Symfony ZXR00 EDOF | ZA9003 Monofocal | p | |
|---|---|---|---|---|---|---|---|---|---|
| DCSP | 3 cpd | 1.63 1.34–1.93 | 1.78 1.17–1.93 | 1.75 1.34–1.93 | 1.78 1.17–1.93 | 1.78 1.17–1.93 | 1.78 1.49–2.08 | 1.93 1.49–2.08 | <0.001 |
| 6 cpd | 1.70 1.38–2.29 | 1.77 1.38–2.29 | 1.70 1.55–1.99 | 1.70 1.21–2.14 | 1.70 1.38–2.14 | 1.84 1.55–2.29 | 2.07 1.70–2.29 | <0.001 | |
| 12 cpd | 1.40 0.91–1.69 | 1.40 0.91–1.99 | 1.40 1.08–1.69 | 1.25 0.31–1.84 | 1.08 0.91–1.84 | 1.69 1.40–1.99 | 1.69 0.91–1.99 | <0.001 | |
| 18 cpd | 0.81 0.47–1.25 | 0.96 0.47–1.55 | 0.81 0.47–1.25 | 0.81 0.13–1.10 | 0.64 0.13–1.25 | 1.10 0.81–1.55 | 1.25 0.47–1.55 | <0.001 | |
| DCSM | 3 cpd | 1.49 1.34–1.93 | 1.71 1.17–2.09 | 1.63 1.34–2.08 | 1.63 1.17–1.93 | 1.63 1.34–1.93 | 1.63 1.34–1.93 | 1.78 1.63–2.08 | 0.001 |
| 6 cpd | 1.70 1.55–2.29 | 1.84 1.38–2.14 | 1.70 0.61–2.14 | 1.84 1.38–2.14 | 1.70 1.21–1.99 | 1.84 1.55–2.29 | 1.99 1.55–2.29 | <0.001 | |
| 12 cpd | 1.40 0.91–1.69 | 1.40 0.31–1.69 | 1.25 0.31–1.69 | 1.25 0.91–1.84 | 1.25 0.31–1.69 | 1.69 1.25–1.99 | 1.69 0.91–1.99 | <0.001 | |
| 18 cpd | 0.81 0.47–1.10 | 0.89 0.47–1.25 | 0.96 0.64–1.25 | 0.81 0.47–1.40 | 0.81 0.13–1.25 | 1.10 0.64–1.55 | 1.25 0.47–1.55 | <0.001 | |
| DCSMG | 3 cpd | 1.56 1.34–1.93 | 1.63 1.34–1.93 | 1.63 1.17–2.08 | 1.63 1.17–1.93 | 1.49 1.00–1.93 | 1.78 1.34–1.93 | 1.78 1.63–2.08 | <0.001 |
| 6 cpd | 1.70 1.55–2.14 | 1.70 1.21–2.14 | 1.84 0.61–2.29 | 1.70 1.38–1.99 | 1.70 1.21–2.14 | 1.99 1.55–2.14 | 1.99 1.70–2.29 | <0.001 | |
| 12 cpd | 1.40 0.31–1.69 | 1.40 0.31–1.99 | 1.25 0.31–1.69 | 1.40 0.31–1.84 | 1.25 0.91–1.69 | 1.54 1.25–1.99 | 1.69 1.08–1.99 | <0.001 | |
| 18 cpd | 0.81 0.47–1.25 | 0.89 0.47–1.55 | 0.96 0.64–1.40 | 0.81 0.64–1.55 | 0.64 0.13–1.25 | 1.10 0.64–1.55 | 1.25 0.81–1.55 | <0.001 | |
| NCSP | 1.5 cpd | 1.54 1.30–1.54 | 1.54 1.30–1.85 | 1.54 1.30–1.85 | 1.54 1.30–1.85 | 1.54 1.30–1.85 | 1.85 1.30–2.23 | 1.54 1.30–2.08 | <0.001 |
| 3 cpd | 1.64 1.38–1.93 | 1.93 1.38–1.93 | 1.64 1.38–2.23 | 1.64 1.38–2.23 | 1.64 1.38–2.23 | 1.93 1.64–2.34 | 1.93 1.38–2.23 | 0.001 | |
| 6 cpd | 1.49 1.32–2.10 | 1.65 1.04–1.85 | 1.65 1.04–1.85 | 1.65 1.32–2.27 | 1.65 1.32–2.10 | 1.85 1.32–2.27 | 1.85 1.32–2.27 | <0.001 | |
| 12 cpd | 1.18 0.90–1.51 | 1.51 0.70–1.94 | 1.18 0.70–1.74 | 1.51 0.90–1.94 | 1.51 0.90–1.94 | 1.51 0.90–1.94 | 1.74 0.90–2.10 | <0.001 | |
| 18 cpd | 0.85 0.60–1.18 | 0.85 0.60–1.60 | 1.00 0.60–1.41 | 1.00 0.60–1.41 | 1.00 0.60–1.41 | 1.18 0.60–1.60 | 1.18 0.30–1.81 | <0.001 |
| SVT250 Bifocal | ZKB00 Bifocal | ZLB00 Bifocal | ATLISA 809M Bifocal | ATLISA Tri 839MP Trifocal | Symfony ZXR00 EDOF | ZA9003 Monofocal | p | ||
|---|---|---|---|---|---|---|---|---|---|
| Spectacle use at far | Always | 0 | 0 | 0 | 0 | 0 | 5.6 | 11.1 | 0.002 |
| Sometimes | 0 | 0 | 5.0 | 0 | 0 | 5.6 | 13.9 | ||
| Never | 100.0 | 100.0 | 95.0 | 100.0 | 100.0 | 88.9 | 75.0 | ||
| Spectacle use at intermediate | Always | 0 | 0 | 0 | 0 | 0 | 5.6 | 11.1 | 0.033 |
| Sometimes | 10.5 | 5.3 | 10.0 | 0 | 0 | 0 | 13.9 | ||
| Never | 89.5 | 94.7 | 90.0 | 100.0 | 100.0 | 94.4 | 75.0 | ||
| Spectacle use at near | Always | 15.8 | 5.3 | 5.0 | 0 | 0 | 16.7 | 75 | <0.001 |
| Sometimes | 52.6 | 52.6 | 30.0 | 23.5 | 22.2 | 22.2 | 25.0 | ||
| Never | 31.6 | 42.1 | 65.0 | 76.5 | 77.8 | 61.1 | 0 | ||
| Halos occurrence and intensity | None | 84.2 | 42.1 | 50.0 | 35.3 | 50.0 | 38.9 | 94.4 | <0.001 |
| 1 | 5.3 | 26.3 | 15.0 | 11.8 | 5.6 | 16.7 | 5.6 | ||
| 2 | 5.3 | 21.1 | 0 | 17.6 | 27.8 | 44.4 | 0 | ||
| 3 | 5.3 | 10.5 | 35.0 | 35.3 | 16.7 | 0 | 0 | ||
| Glare occurrence and intensity | None | 0 | 0 | 0 | 0 | 5.6 | 0 | 0 | 0.016 |
| 1 | 47.4 | 52.6 | 47.4 | 35.3 | 16.7 | 38.9 | 77.8 | ||
| 2 | 15.8 | 5.3 | 31.6 | 17.6 | 27.8 | 22.2 | 16.7 | ||
| 3 | 21.1 | 21.1 | 5.3 | 29.4 | 11.1 | 5.6 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil, M.Á.; Varón, C.; Cardona, G.; Buil, J.A. Far and Near Contrast Sensitivity and Quality of Vision with Six Presbyopia Correcting Intraocular Lenses. J. Clin. Med. 2022, 11, 4150. https://doi.org/10.3390/jcm11144150
Gil MÁ, Varón C, Cardona G, Buil JA. Far and Near Contrast Sensitivity and Quality of Vision with Six Presbyopia Correcting Intraocular Lenses. Journal of Clinical Medicine. 2022; 11(14):4150. https://doi.org/10.3390/jcm11144150
Chicago/Turabian StyleGil, Miguel Á., Consuelo Varón, Genis Cardona, and José A. Buil. 2022. "Far and Near Contrast Sensitivity and Quality of Vision with Six Presbyopia Correcting Intraocular Lenses" Journal of Clinical Medicine 11, no. 14: 4150. https://doi.org/10.3390/jcm11144150
APA StyleGil, M. Á., Varón, C., Cardona, G., & Buil, J. A. (2022). Far and Near Contrast Sensitivity and Quality of Vision with Six Presbyopia Correcting Intraocular Lenses. Journal of Clinical Medicine, 11(14), 4150. https://doi.org/10.3390/jcm11144150