1. Introduction
Tuberculosis affects HIV-positive individuals throughout all phases of HIV infection and is the leading cause of mortality among HIV positive patients [
1]. Tuberculosis and human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) constitute a significant percent of infectious disease in resource-limited countries.
Globally, an estimated 10.0 million (range, 8.9–11.0 million) [
2] people fell ill with tuberculosis in 2019, a number that has been declining very slowly in recent years. There were an estimated 1.2 million (range, 1.1–1.3 million) deaths due to tuberculosis among HIV-negative individuals in 2019 (a reduction from 1.7 million in 2000) and an additional 208,000 deaths (range, 177,000–242,000) [
3] among HIV-positive patients (a reduction from 678,000 in 2000).
Currently, the standard screening procedures include using a four-part symptom screen alone or in conjunction with chest radiography (CXR) for people living with HIV (PLHIV) in high-burden settings [
1]. PLHIV who report any of the symptoms of current cough, fever, weight loss, or night sweats may have active tuberculosis; they should be evaluated for tuberculosis and other diseases and should be offered preventive treatment if active tuberculosis is excluded.
The WHO’s target product profile for a tuberculosis screening test requires that the sensitivity be ≥90% and the specificity be ≥70% [
4]. Current tools to screen people living with HIV for active pulmonary tuberculosis are limited to symptom-based screening, which has an unacceptably low specificity, and chest X-ray, which has a relatively low sensitivity. Chest X-ray-based screening has high infrastructural requirements and relies on trained interpreters, both of which are not routinely available in most health care centers in tuberculosis-endemic areas [
5].
C-reactive protein (CRP) is a non-specific inflammatory marker that has been found to be elevated in both HIV-infected and uninfected people with pyogenic infections including active tuberculosis [
6]. CRP is an acute phase reactant, the levels of which rise in response to IL-6 mediated pyogenic infections such as active tuberculosis [
7]. CRP has been proposed to be a potential biomarker for tuberculosis disease as well as a prognostic indicator of disease and treatment [
8]. CRP testing has the advantage of being quick and inexpensive. Although elevations in CRP (≥10 mg/L) are not specific for active tuberculosis, two studies that evaluated CRP as a screening test among PLHIV initiating antiretroviral therapy (ART) found that CRP has a two- to six-fold higher specificity (58% and 81%) than symptom-based tuberculosis screening [
9,
10]. However, previous studies have only looked at CRP as a screening tool for pulmonary tuberculosis and have failed to assess its utility in the screening of extra pulmonary tuberculosis.
This study was conducted to determine the diagnostic accuracy of CRP for the detection of tuberculosis in people living with HIV who are positive according to the WHO symptom screen. It evaluated the utility of CRP as a screening tool for pulmonary as well as extra-pulmonary tuberculosis.
2. Materials and Methods
2.1. Aim
The aim of this study was to determine the diagnostic accuracy of C-reactive protein for the detection of tuberculosis in people living with HIV who are positive according to the WHO symptom screen.
2.2. Objectives
To estimate the sensitivity and specificity of C-reactive protein as a screening test for tuberculosis in people living with HIV who are positive according to the WHO symptom screen.
To calculate the ideal CRP cut-off value to be used in TB screening in PLHIV who are positive according to the WHO symptom screen.
2.3. Study Design and Setting
This was a cross-sectional, observational study that was conducted in the Anti-Retroviral Therapy (ART) centers of tertiary care hospitals attached to Kasturba Medical College, Mangalore, a city in southern India. Data collection was conducted between January 2020 and May 2021. The study was conducted following approval from the institutional ethics committee of Kasturba Medical College, Mangalore.
2.4. Sampling
The sample size was calculated using the ‘
n Master sample size calculator’ based on a CRP sensitivity of 89% [
11], precision of 5%, and a confidence interval of 95%. The sample size was found to be 150. Samples were collected from January 2020 to May 2021.
Patients diagnosed as HIV positive, who come to the Anti-Retroviral Therapy center for follow up, those of who were positive according to the WHO symptom screen, were considered for the study. All the study participants were over 18 years of age and provided written informed consent for their participation in the study. Sampling was convenience based. All consecutive eligible patients were enrolled until the sample size was met.
Patients with HIV who had been initiated on Anti-Tuberculosis Therapy (ATT) for any diagnosis of tuberculosis were excluded. Patients with any other auto-immune disease were also excluded.
2.5. Study Description
From January 2020 to May 2021, patients presenting to the Anti-Retroviral Therapy center for follow-up treatment and who qualified as per the inclusion and exclusion criteria were enrolled in the study. Demographic data and other relevant data with respect to patient’s HIV treatment and immunological status were documented. Blood samples from all the patients who were positive according to the WHO symptom screen were sent for C-reactive protein estimation. A value of ≥10 mg/L (rounding to the nearest whole number) was considered as being positive on the CRP screening test (this value was selected based on previous studies [
5,
7]). All patients were subsequently followed up with for a diagnosis of tuberculosis by a physician. The diagnosis of pulmonary TB was made through a nucleic acid amplification test (GeneXpert) using a sputum specimen or bronchoalveolar lavage fluid. The diagnosis of extra pulmonary TB was made based on the site of tuberculosis. Tubercular pleural effusion was diagnosed when pleural fluid analysis revealed an exudative effusion with ADA > 40 U/L or the presence of a positive GeneXpert for Mycobacterium tuberculosis. A diagnosis of tubercular lymphadenitis was made when either a fine-needle aspiration specimen or a lymph node biopsy specimen showed a histopathological confirmation of tuberculosis or was positive on GeneXpert. A diagnosis of abdominal tuberculosis was made when a tissue biopsy specimen or ultrasound-guided aspirate was positive on GeneXpert or was confirmed to be tuberculosis according to histopathology. The objectives of the study were two-fold. First, the objective was to estimate the sensitivity and specificity of C-reactive protein as a screening test for tuberculosis in people living with HIV. Additionally, the second aim of the study was to calculate the ideal CRP cut-off value to be used in tuberculosis screening in PLHIV.
2.6. Statistical Methods
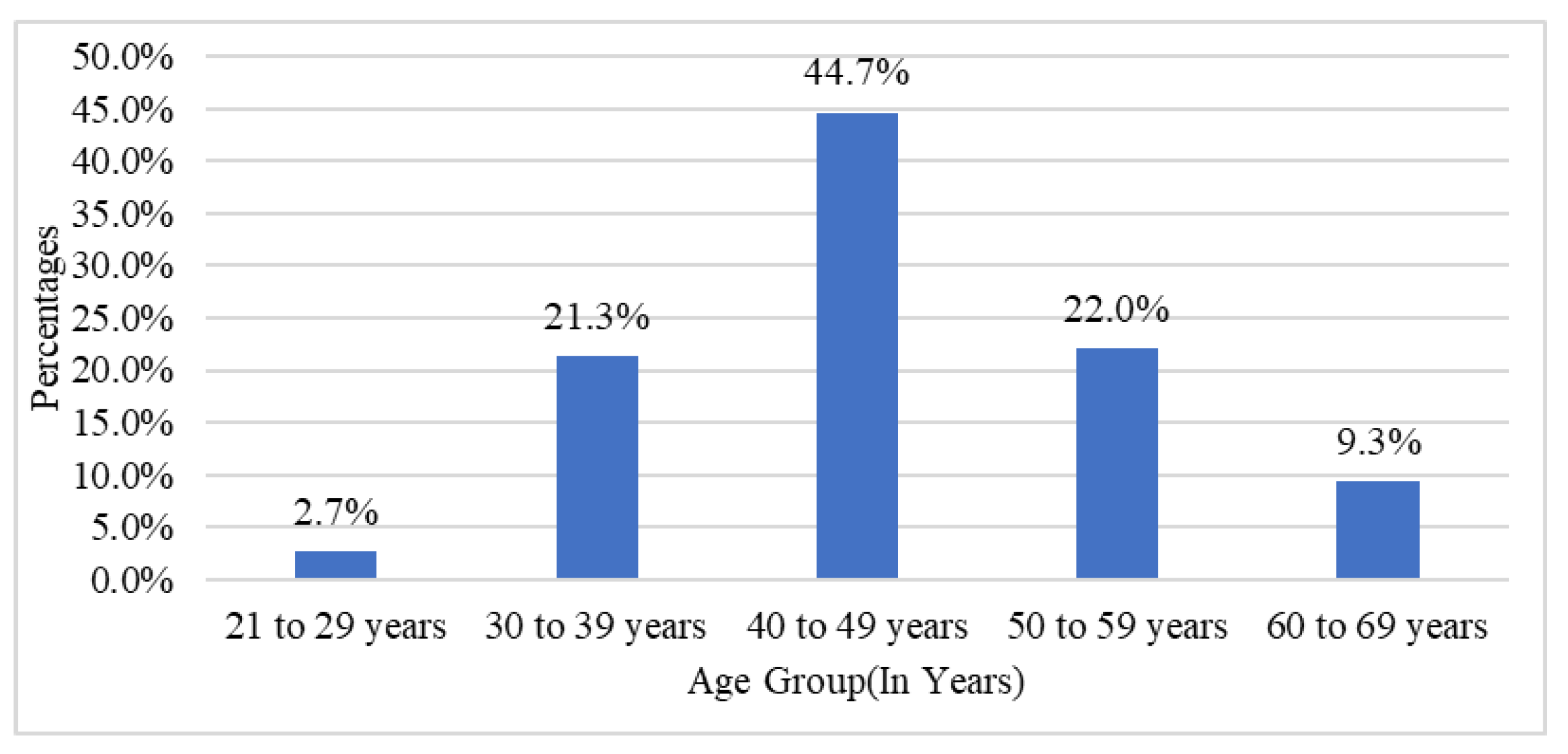
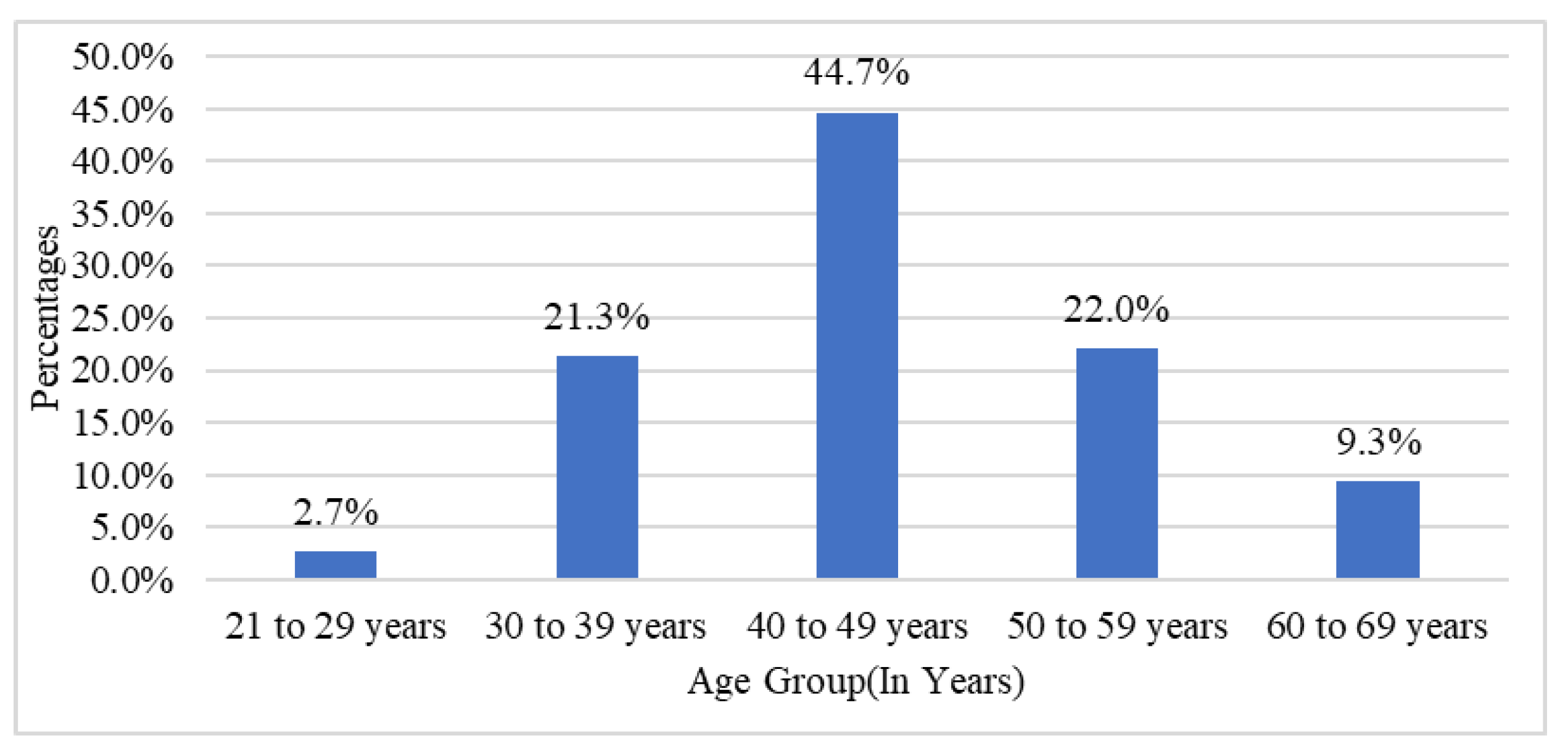
Tuberculosis-positive was considered as the primary outcome variable. The CRP value was considered as the primary explanatory variable. Descriptive analysis was carried out according to the mean, standard deviation, or median for quantitative variables and by frequency and proportion for categorical variables. Data were also represented using appropriate diagrams such as bar graphs, pie charts and stacked bar graphs. The categorical outcomes were compared between study groups using the Chi square test.
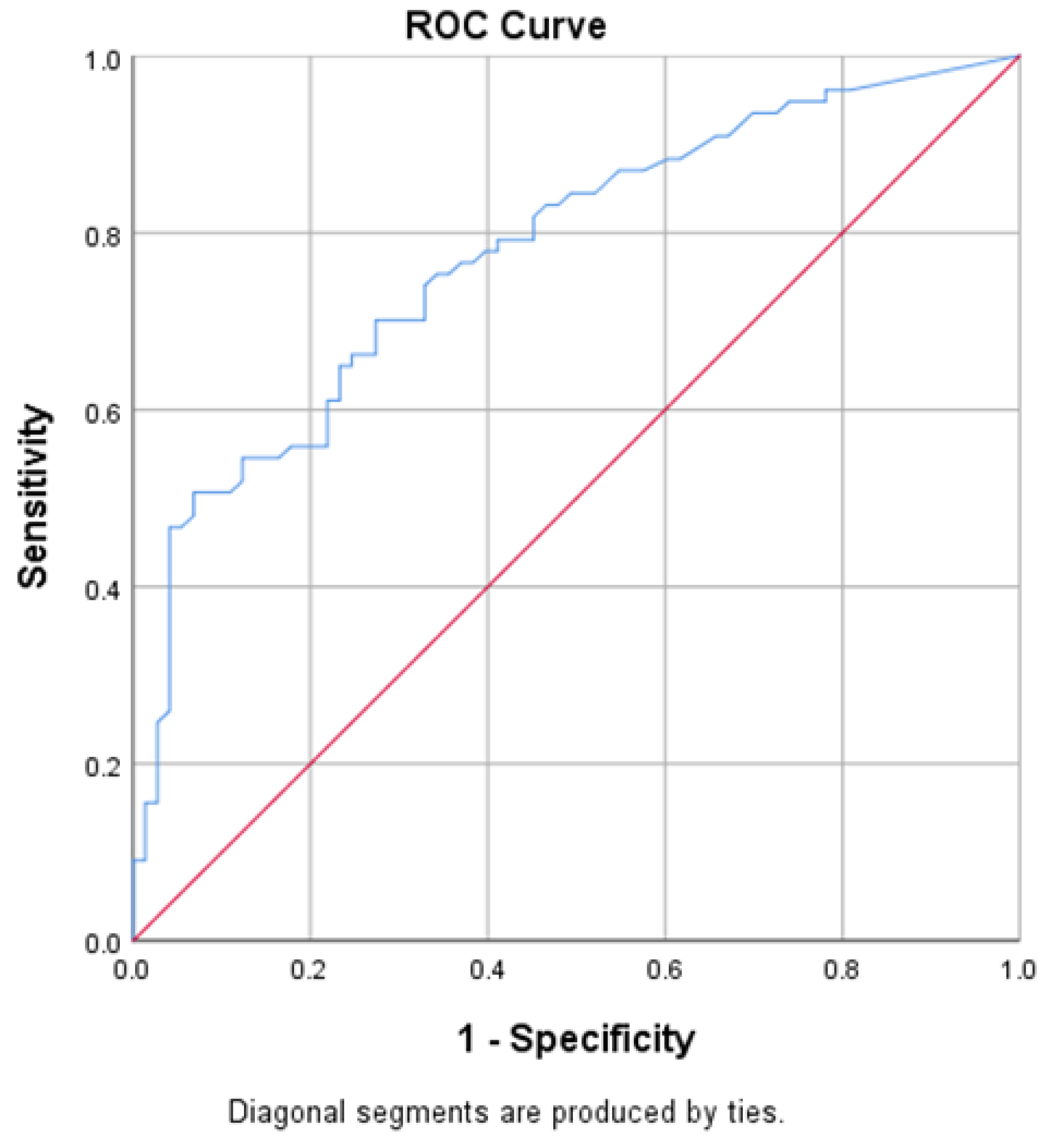
CRP-positive was considered as the screening test, and tuberculosis-positive was considered as the gold standard. The utility of the CRP value in predicting tuberculosis positivity was assessed by means of receiver operative curve (ROC) analysis. The area under the ROC curve, along with its 95% CI and p value, is presented in the results. Based on the ROC analysis, it was decided that 8.25 would be considered the ideal cut-off value. The sensitivity, specificity, predictive values, and diagnostic accuracy of the screening test along with their 95% CI are presented in the results. A p value of < 0.05 was considered statistically significant. Data were analyzed using coGuide software, V.1.03 (producer—coGuide, headquarters—Bengaluru, India).
4. Discussion
Tuberculosis and HIV are public health problems that have a synergistic effect on each other. In people living with HIV (PLHIV), tuberculosis increases HIV replication [
6], while HIV lowers the immune response against tuberculosis, leading to increased active tuberculosis infection, re-infection, or reactivation, thus increasing the risk of progression from latent tuberculosis to active tuberculosis. CRP is a non-specific marker of inflammation. Although CRP values have been found to be elevated in HIV-positive individuals both before and after the initiation of ART without underlying tuberculosis, studies have shown that the CRP value is usually <3 mg/dL, irrespective of their immune status (i.e., CD4 count and viral load) [
12,
13].
In studies by Shapiro AE et al. [
8] and Lawn SD et al. [
9], it was found that CRP values were significantly elevated in those with tuberculosis compared to those without tuberculosis. Previous studies have only looked at CRP as a screening tool for the detection of pulmonary tuberculosis in people living with HIV. Ours is the first to have studied the utility of CRP as a screening tool for both pulmonary as well as extra pulmonary tuberculosis. The four-part WHO symptom screen had a sensitivity of 79%, a specificity of 50%, and a negative predictive value of 97.7% at a tuberculosis prevalence of 5%, as reported in a meta-analysis by the WHO [
14].
In this study, after ROC analysis of the data, we found that a CRP value of 8.25 mg/dL which provided optimum sensitivity and specificity, had fair predictive validity in detecting tuberculosis, as indicated by an area under the curve value of 0.777 (95% CI 0.703 to 0.851, p value < 0.001). CRP (≥8.25 mg/dL) had a sensitivity of 70.13% and a specificity of 69.86% in predicting tuberculosis, and the total diagnostic accuracy was 70% in the present study.
The results of this study were comparable with the diagnostic accuracy reported by other studies. There was variation in reporting the diagnostic accuracy of CRP with regard to the gold standard used (Culture/ Gene Xpert MTB-CB NAAT/ Sputum positive) because other studies included pulmonary tuberculosis only, in which it is easier to obtain the microbiological evidence of tuberculosis that is necessary for its diagnosis. Because our study included extra pulmonary tuberculosis, it also accepted other modalities to reach a diagnosis of tuberculosis, such as obtaining microbiological evidence in some situations, for example in cases of tubercular pleural effusion, abdominal tuberculosis, etc., may not have been practical.
In the study by Shapiro AE et al. [
8], using CRP to discriminate between the presence of tuberculosis (positive culture) and the absence of tuberculosis (negative culture) resulted in an area under the ROC curve of 0.80. Using a CRP threshold >5 mg/L resulted in a sensitivity of 90.5% and a specificity of 58.5%. Using a CRP threshold >10 mg/L, the sensitivity decreased to 78.6%, and the specificity increased to 72.3%. Lawn SD et al. [
9] observed that very low (<1.5 mg/L) CRP concentrations excluded tuberculosis (100% negative predictive value), whereas very high concentrations (>400 mg/L) were strongly predictive of tuberculosis (100% positive predictive value). The area under the curve (AUC) was 0.81 when all patients were included and was similar when the analysis was restricted to patients with a positive WHO symptom screen. Yoon C et al. [
5] observed that compared to POC CRP, the WHO symptom screen had higher sensitivity (89% vs. 96%) but substantially lower specificity (72% vs. 14%,
p < 0·0001). They observed that POC CRP met the minimum TB screening test sensitivity (≥90%) and specificity (≥70%) targets when the cut-point was lowered to 8 mg/L (AUROC 0·80, 95% CI: 0·77 to 0·83) or 9 mg/L (AUROC 0·81, 95% CI: 0·78 to 0·83.
From this study, it was concluded that the relationship between CRP-positive (with a cut-off value of 10 mg/L) and tuberculosis was found to be statistically significant. CRP was found to have to a sensitivity of 64.94% and a specificity of 76.71%. After ROC analysis, the ideal cut-off for CRP was found to be 8.25 (with a sensitivity of 70.13% and a specificity of 69.86%).
The current WHO-consolidated guidelines on tuberculosis include CRP as a screening tool for tuberculosis in treatment-naïve individuals with HIV as a conditional recommendation. The cut-off value recommended by the WHO is >5 mg/L [
15]. Our study helps to reiterate the value of CRP as a screening tool for TB in PLHIV and shows its validity in patients who are on anti-retroviral therapy as well as its utility in extra-pulmonary tuberculosis. The ideal cut-off value as per our study was chosen to optimize the sensitivity and specificity. Our data suggest that a cut-off value of >5 mg/L would result in a sensitivity and specificity of 81% and 54%, respectively.
The limitations of this study were that the sample size was small, thus reducing the power of the study. The study did not use TB cultures as the gold standard, which may have resulted in missed cases. Previous studies have shown that the sensitivity and specificity of GeneXpert was found to be 88.5% and 96.7% for the detection of pulmonary TB and 85.1% and 95.7% for the detection of extra-pulmonary TB [
16]. The diagnostic gold standard used to detect extra-pulmonary TB has its challenges. It does not provide microbiological evidence of tuberculosis and involves invasive procedure which may not be feasible in all patients. Although in some cases of tuberculosis, obtaining tissue/microbiological evidence of TB maybe challenging, and in practice, patients maybe be treated based on a clinical diagnosis of TB, we avoided using this as a criterion for diagnosis to maintain objectivity. This study used lab CRP values for screening and not-point-of care-CRP, which may be more appropriate for screening.





{kind=link}
{kind=link}