
Mandibular Molar Uprighting Using Skeletal Anchorage: A Novel Approach

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
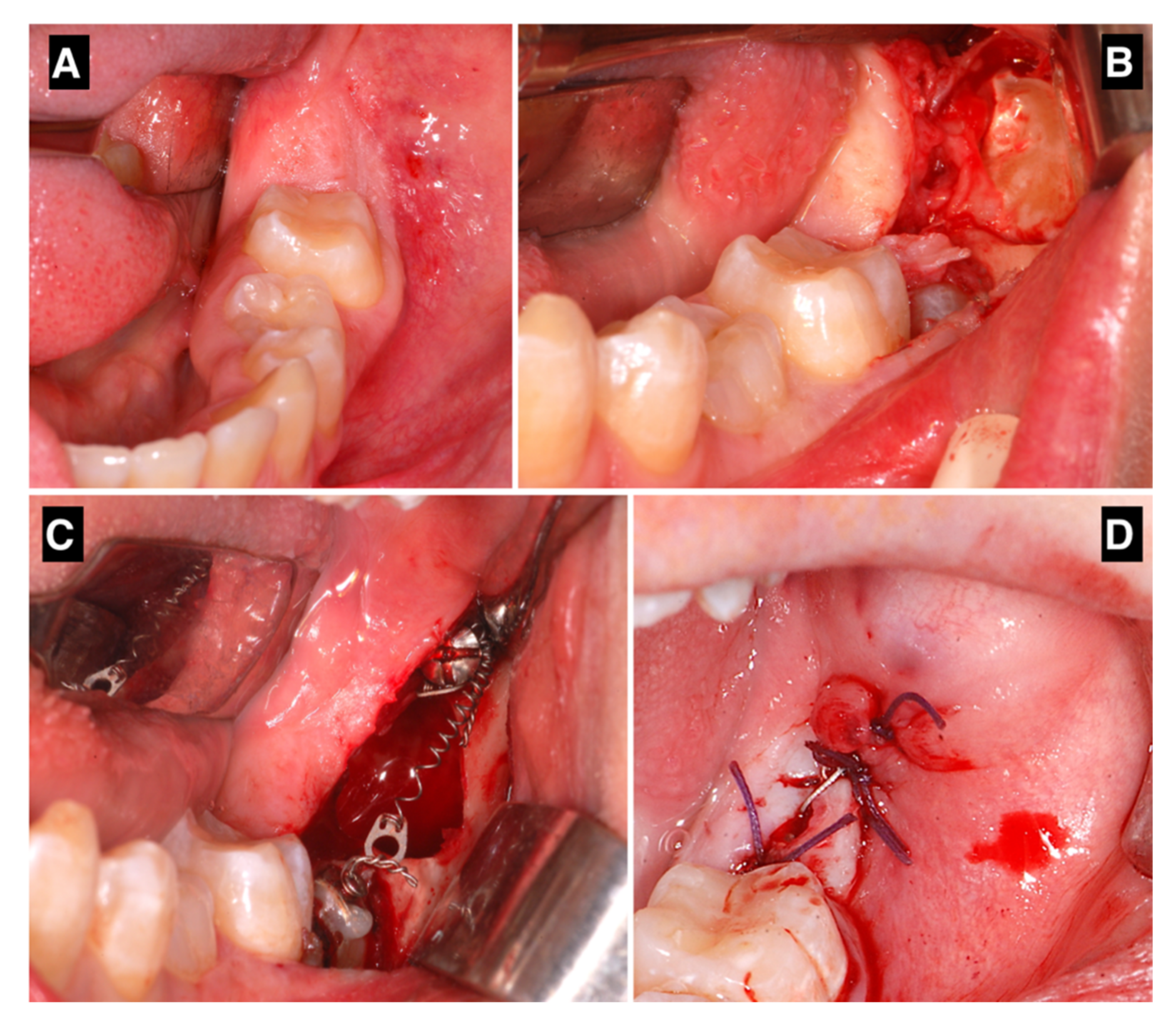
2.2. Surgical and Orthodontic Procedures
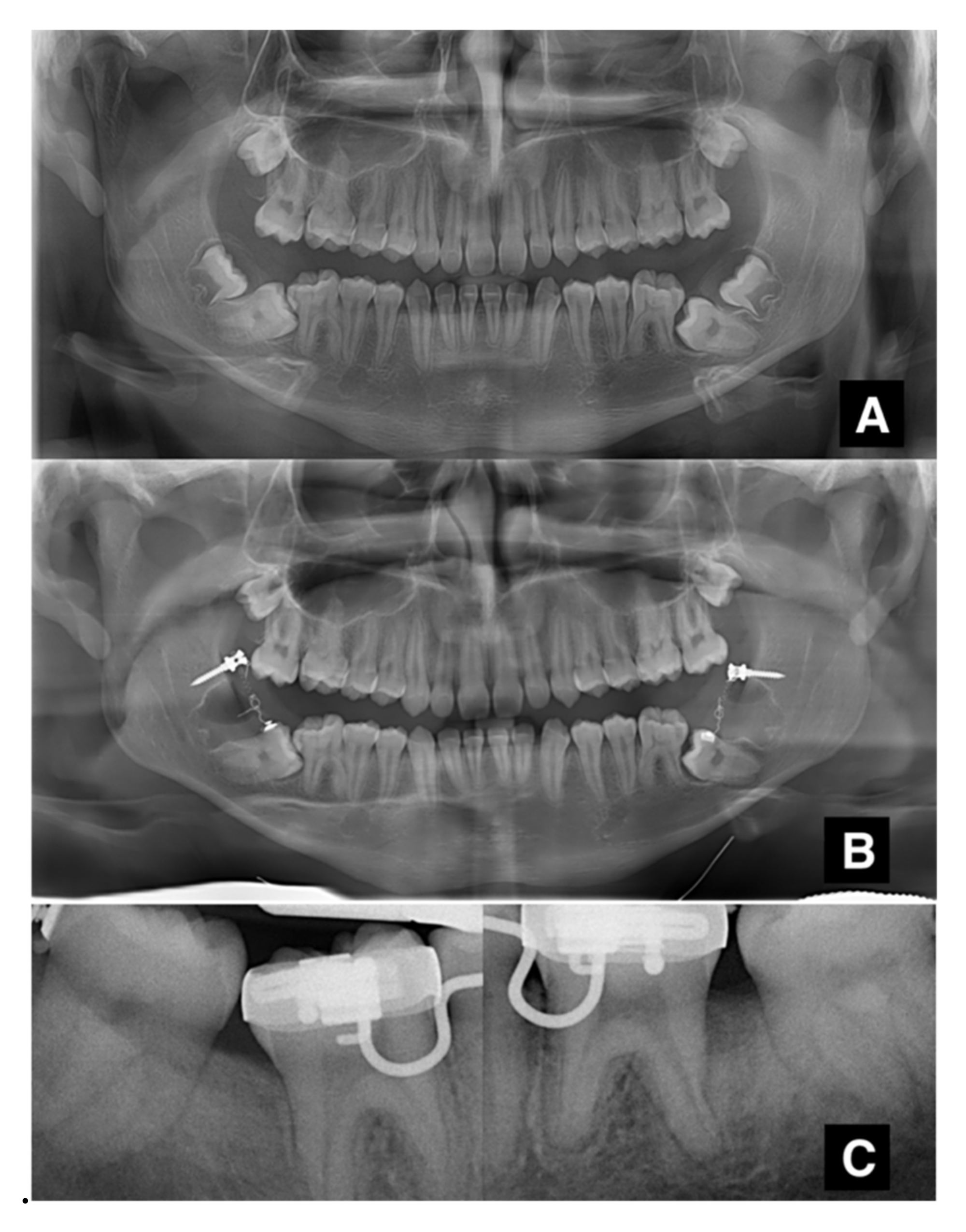
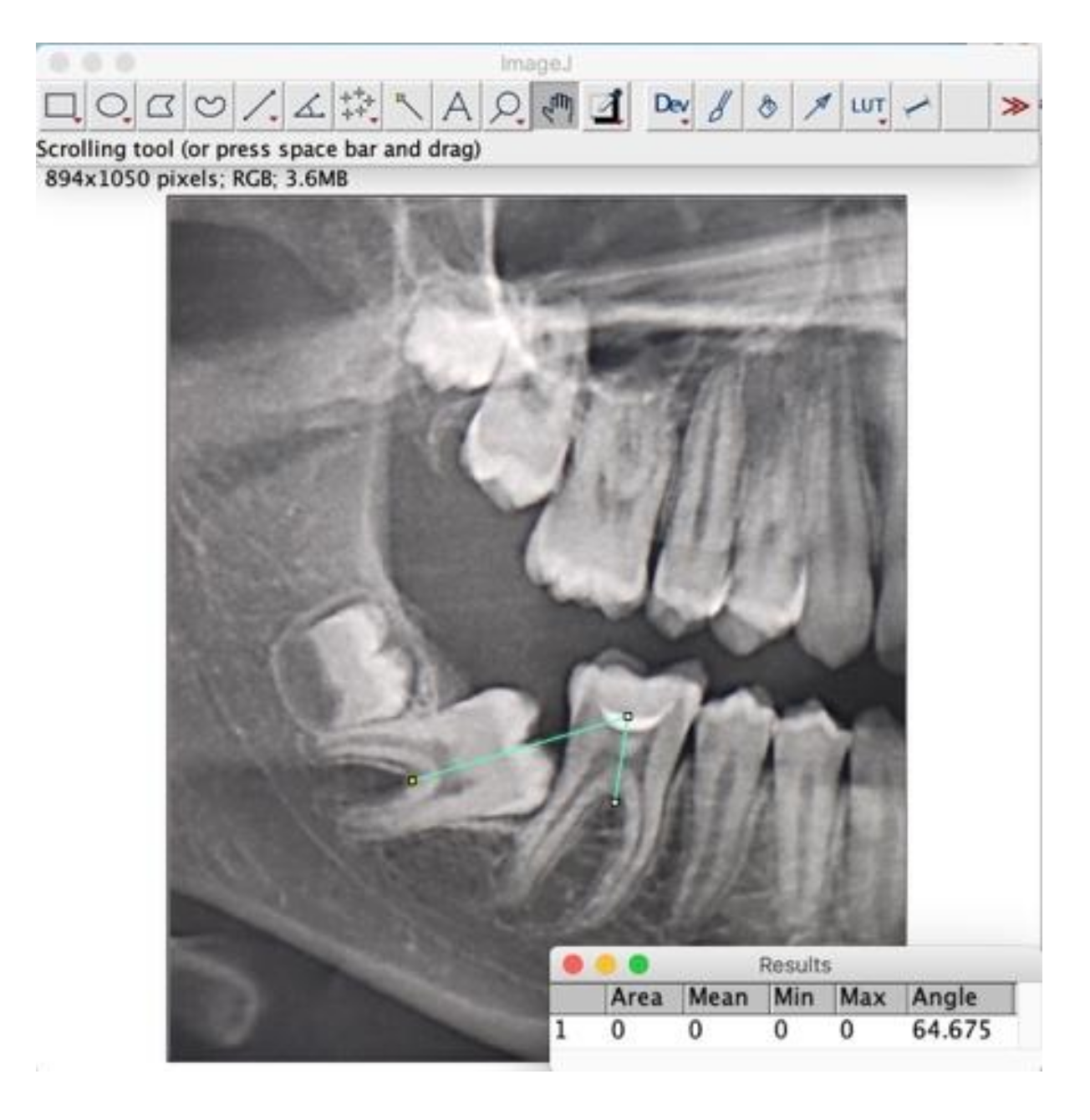
2.3. Measurements
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neville, B.W.; Damm, D.D.; Allen, C.M.; Chi, A.C. Oral and Maxillofacial Pathology; Elsevier: Amsterdam, The Netherlands, 2015; ISBN 978-0-323-34142-4. [Google Scholar]
- Soxman, J.A.; Wunsch, P.B. Anomalies of Tooth Eruption. Clin. Dent. Rev. 2019, 3, 7. [Google Scholar] [CrossRef]
- Grover, P.S.; Lorton, L. The Incidence of Unerupted Permanent Teeth and Related Clinical Cases. Oral Surg. Oral Med. Oral Pathol. 1985, 59, 420–425. [Google Scholar] [CrossRef]
- Varpio, M.; Wellfelt, B. Disturbed Eruption of the Lower Second Molar: Clinical Appearance, Prevalence, and Etiology. ASDC J. Dent. Child. 1988, 55, 114–118. [Google Scholar] [PubMed]
- Cho, S.; Ki, Y.; Chu, V.; Chan, J. Impaction of Permanent Mandibular Second Molars in Ethnic Chinese Schoolchildren. J. Can. Dent. Assoc. 2008, 74, 521. [Google Scholar] [PubMed]
- Bondemark, L.; Tsiopa, J. Prevalence of Ectopic Eruption, Impaction, Retention and Agenesis of the Permanent Second Molar. Angle Orthod. 2007, 77, 773–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baccetti, T. Tooth Anomalies Associated with Failure of Eruption of First and Second Permanent Molars. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 608–610. [Google Scholar] [CrossRef] [PubMed]
- Frank, C.A. Treatment options for impacted teeth. J. Am. Dent. Assoc. 2000, 131, 623–632. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Kølsen Petersen, J.; Laskin, D.M. (Eds.) Textbook and Color Atlas of Tooth Impactions: Diagnosis, Treatment, Prevention, 1st ed.; 1st Print; Munksgaard: Copenhagen, Denmark, 1997; ISBN 978-87-16-10693-3. [Google Scholar]
- Magnusson, C.; Kjellberg, H. Impaction and Retention of Second Molars: Diagnosis, Treatment and Outcome. Angle Orthod. 2009, 79, 422–427. [Google Scholar] [CrossRef]
- Eckhart, J.E. Orthodontic Uprighting of Horizontally Impacted Mandibular Second Molars. J. Clin. Orthod. 1998, 32, 621–624. [Google Scholar]
- Shapira, Y.; Borell, G.; Nahlieli, O.; Kuftinec, M.M. Uprighting Mesially Impacted Mandibular Permanent Second Molars. Angle Orthod. 1998, 68, 173–178. [Google Scholar] [CrossRef]
- Suri, L.; Gagari, E.; Vastardis, H. Delayed Tooth Eruption: Pathogenesis, Diagnosis, and Treatment. A Literature Review. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 432–445. [Google Scholar] [CrossRef] [PubMed]
- Freeman, R.S. Mandibular Second Molar Problems. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 19–21. [Google Scholar] [CrossRef]
- Johnson, J.V.; Quirk, G.P. Surgical Repositioning of Impacted Mandibular Second Molar Teeth. Am. J. Orthod. Dentofac. Orthop. 1987, 91, 242–251. [Google Scholar] [CrossRef]
- Abate, A.; Cavagnetto, D.; Fama, A.; Matarese, M.; Bellincioni, F.; Assandri, F. Efficacy of Operculectomy in the Treatment of 145 Cases with Unerupted Second Molars: A Retrospective Case–Control Study. Dent. J. 2020, 8, 65. [Google Scholar] [CrossRef]
- Lee, K.-J.; Park, Y.-C.; Hwang, W.-S.; Seong, E.-H. Uprighting Mandibular Second Molars with Direct Miniscrew Anchorage. J. Clin. Orthod. 2007, 41, 627–635. [Google Scholar]
- Giancotti, A.; Muzzi, F.; Santini, F.; Arcuri, C. Miniscrew Treatment of Ectopic Mandibular Molars. J. Clin. Orthod. 2003, 37, 380–383. [Google Scholar]
- Bourzgui, F. (Ed.) Orthodontics—Basic Aspects and Clinical Considerations; IntechOpen: London, UK, 2012; ISBN 978-953-51-0143-7. [Google Scholar]
- Finotti, M.; Del Torre, M.; Roberto, M.; Miotti, F.A. La Distalisation Des Molaires Mandibulaires Peut-Elle Être Facilitée? Une Nouvelle Méthode Thérapeutique. Orthod. Française 2009, 80, 371–378. [Google Scholar] [CrossRef]
- Kravitz, N.D.; Yanosky, M.; Cope, J.B.; Silloway, K.; Favagehi, M. Surgical Uprighting of Lower Second Molars. J. Clin. Orthod. 2016, 50, 33–40. [Google Scholar]
- Derton, N.; Perini, A.; Mutinelli, S.; Gracco, A. Mandibular Molar Uprighting Using Mini-Implants: Different Approaches for Different Clinical Cases—Two Case Reports. Orthodontics 2012, 13, 138–145. [Google Scholar]
- Sonis, A.; Ackerman, M. E-Space Preservation: Is There a Relationship to Mandibular Second Molar Impaction? Angle Orthod. 2011, 81, 1045–1049. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Ossa, D.M.; Escobar-Correa, N.; Ramírez-Bustamante, M.A.; Agudelo-Suárez, A.A. An Umbrella Review of the Effectiveness of Temporary Anchorage Devices and the Factors That Contribute to Their Success or Failure. J. Evid. Based Dent. Pract. 2020, 20, 101402. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number. | Age at Time of Intervention | Sex | Tooth | Type of Impaction | Presence of Third Molar | Treatment Duration (months) | Side Effects | Additional Orthodontic Treatment | Initial Angle |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 19 | M | 3.7 | intra-osseous | 3.8 | 10 | no | yes | 53.4 |
| 2 | 16 | M | 3.7 | mucous | 3.8 | 10 | no | no | 29.4 |
| 3 | 18 | F | 3.7 | mucous | 3.8 | 9 | no | yes | 43.5 |
| 4 | 22 | M | 4.7 | mucous | no | 10 | Ipertrofy of the mucosa | yes | 36.8 |
| 5 | 18 | M | 4.7 | intra-osseous | 4.8 | 11 | Poor hygiene | no | 61.4 |
| 6 | 15 | M | 3.7 | mucous | 3.8 | 10 | Ipertrofy of the mucosa | no | 76.6 |
| 7 | 20 | M | 4.7 | mucous | 4.8 | 10 | no | no | 12.7 |
| 8 | 16 | M | 4.7 | intra-osseous | 4.8 | 14 | no | no | 64.6 |
| 9 | 13 | M | 3.7 | mucous | 3.8 | 4 | no | no | 46.3 |
| 10 | 20 | M | 4.7 | mucous | 4.8 | 11 | no | no | 61.4 |
| 11 | 16 | F | 4.7 | mucous | 4.8 | 10 | no | yes | 71.0 |
| 12 | 14 | F | 4.7 | intra-osseous | 4.8 | 9 | no | no | 67.8 |
| 13 | 18 | F | 3.7 | mucous | 3.8 | 10 | no | no | 104.8 |
| 14 | 23 | F | 4.7 | intra-osseous | 4.8 | 11 | no | no | 54.6 |
| 15 | 14 | F | 4.7 | intra-osseous | 4.8 | 9 | no | no | 73.6 |
| 16 | 21 | M | 4.7 | intra-osseous | no | 10 | no | no | 41.5 |
| 17 | 16 | F | 3.7 | intra-osseous | 3.8 | 9 | no | no | 13.3 |
| 18 | 21 | F | 4.7 | intra-osseous | 4.8 | 10 | no | yes | 49.3 |
| 19 | 14 | M | 3.7 | intra-osseous | 3.8 | 10 | no | yes | 75.7 |
| 14 | M | 4.7 | intra-osseous | 4.8 | 10 | no | yes | 76.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sbricoli, L.; Ricci, S.; Cattozzo, A.; Favero, R.; Bressan, E.; Sivolella, S. Mandibular Molar Uprighting Using Skeletal Anchorage: A Novel Approach. J. Clin. Med. 2022, 11, 3565. https://doi.org/10.3390/jcm11133565
Sbricoli L, Ricci S, Cattozzo A, Favero R, Bressan E, Sivolella S. Mandibular Molar Uprighting Using Skeletal Anchorage: A Novel Approach. Journal of Clinical Medicine. 2022; 11(13):3565. https://doi.org/10.3390/jcm11133565
Chicago/Turabian StyleSbricoli, Luca, Sara Ricci, Andrea Cattozzo, Riccardo Favero, Eriberto Bressan, and Stefano Sivolella. 2022. "Mandibular Molar Uprighting Using Skeletal Anchorage: A Novel Approach" Journal of Clinical Medicine 11, no. 13: 3565. https://doi.org/10.3390/jcm11133565
APA StyleSbricoli, L., Ricci, S., Cattozzo, A., Favero, R., Bressan, E., & Sivolella, S. (2022). Mandibular Molar Uprighting Using Skeletal Anchorage: A Novel Approach. Journal of Clinical Medicine, 11(13), 3565. https://doi.org/10.3390/jcm11133565