
Xpert MTB/RIF Assay for the Diagnosis of Lymph Node Tuberculosis in Children: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Search Strategy and Sources
2.3. Inclusion and Exclusion Criteria
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment of Studies
2.6. Statistics and Analysis
3. Results
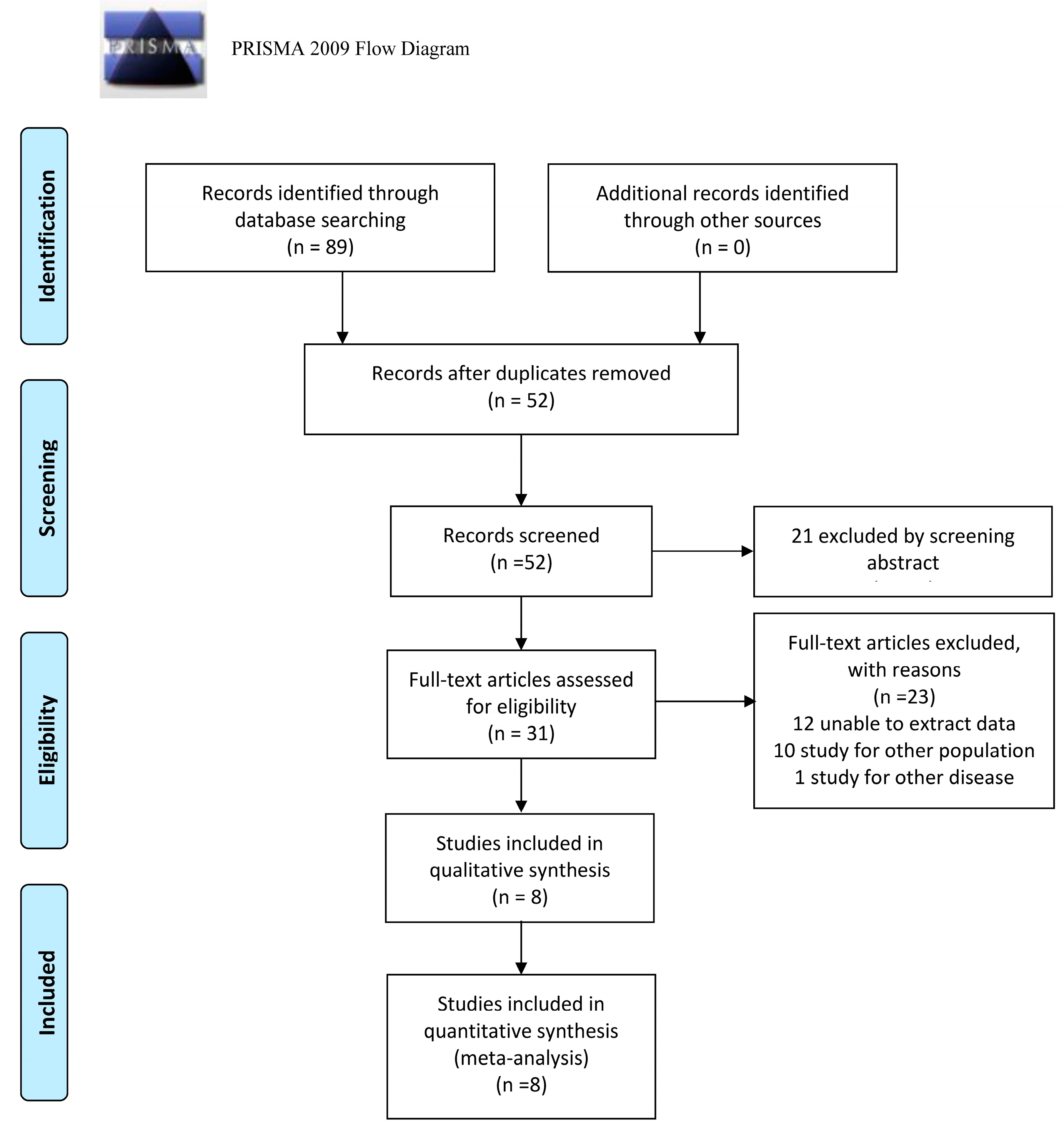
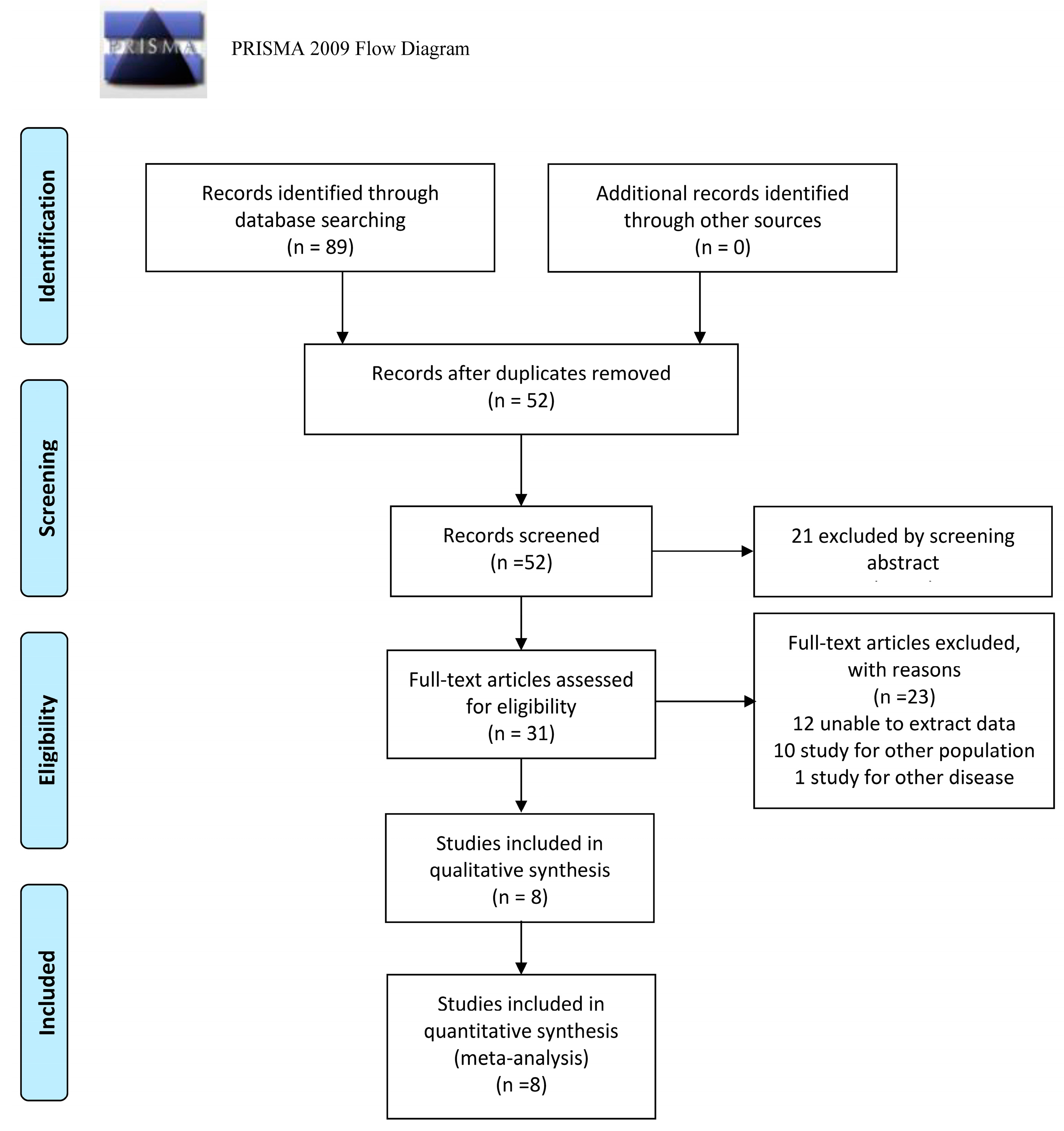
3.1. Results of Included Studies
3.2. Literature Characteristics
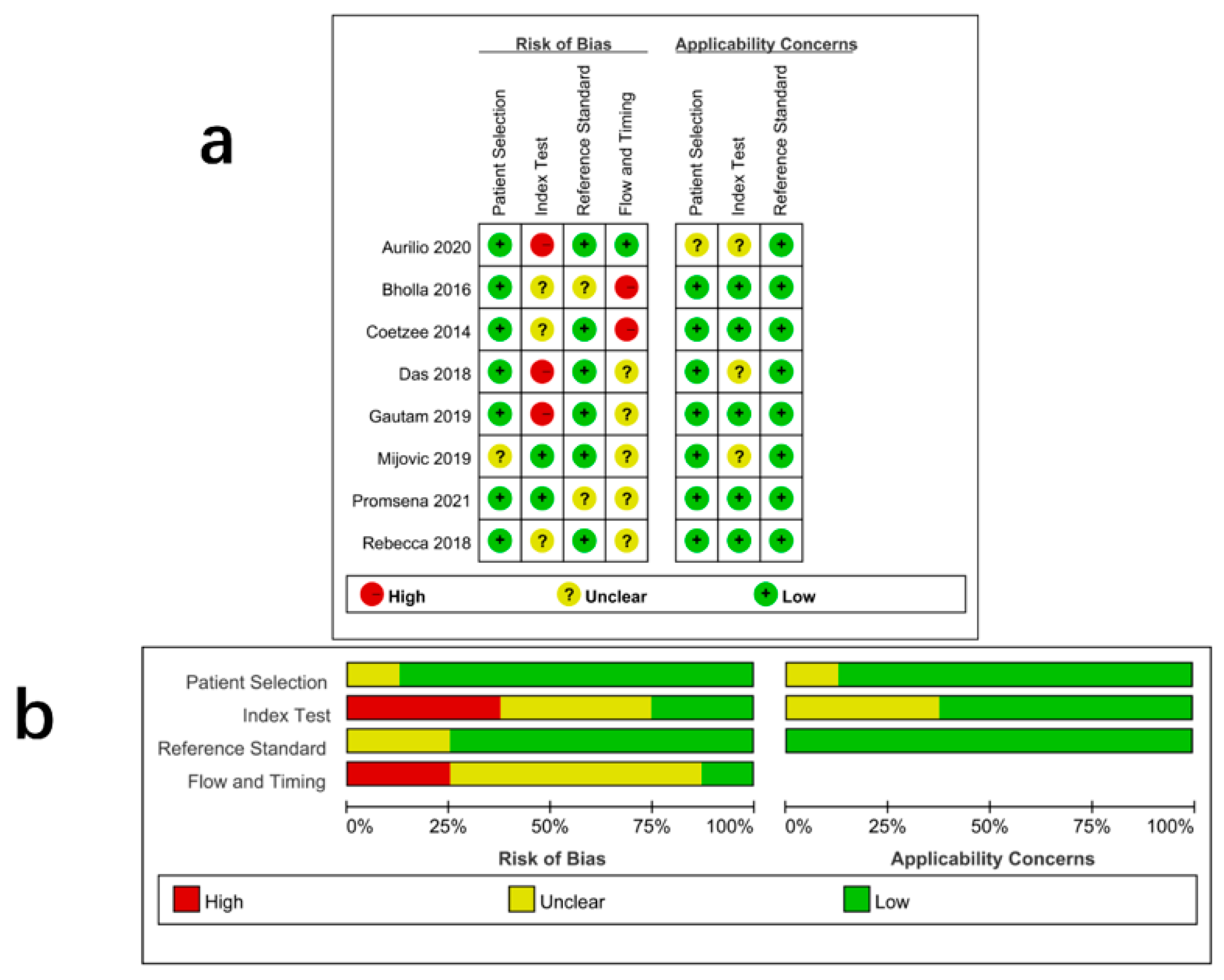
3.3. Quality Assessment
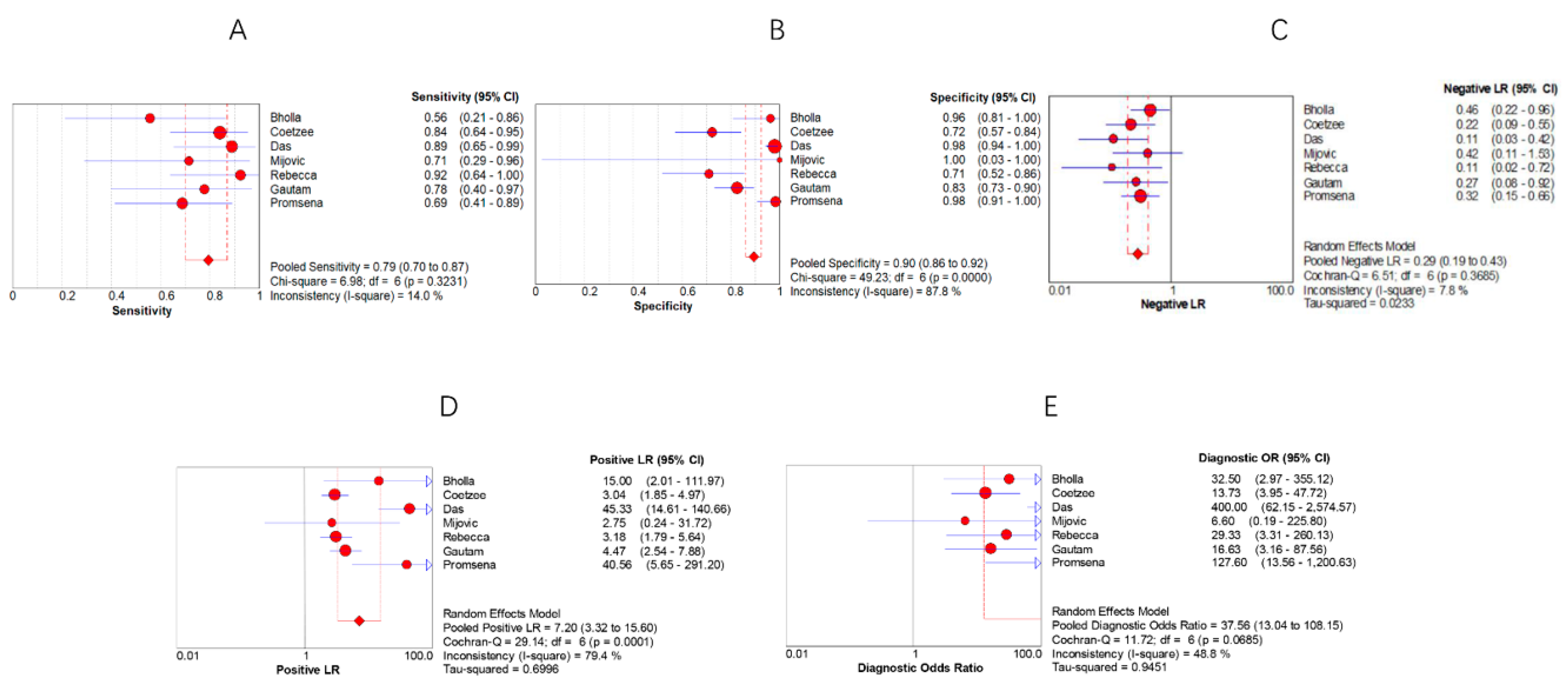
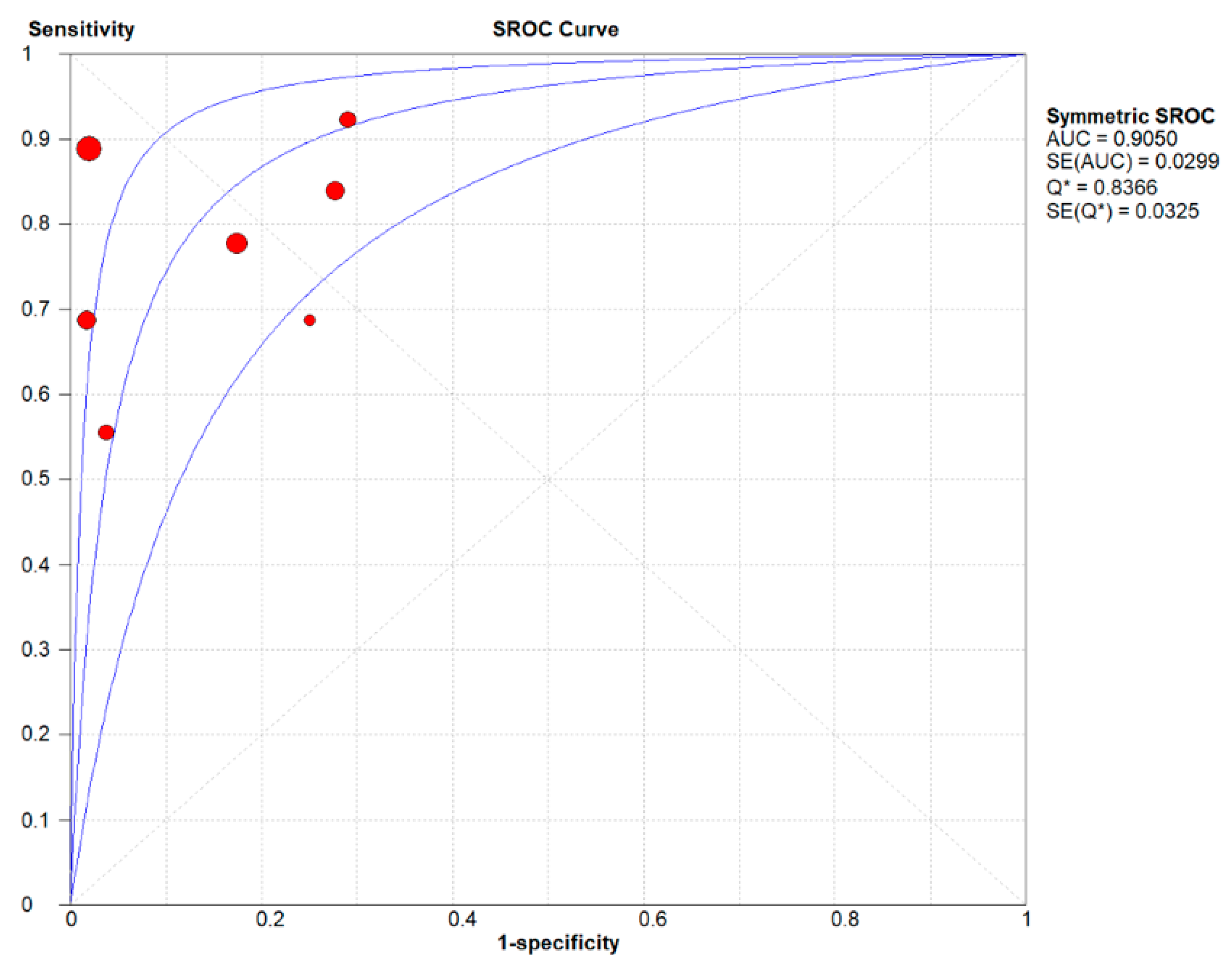
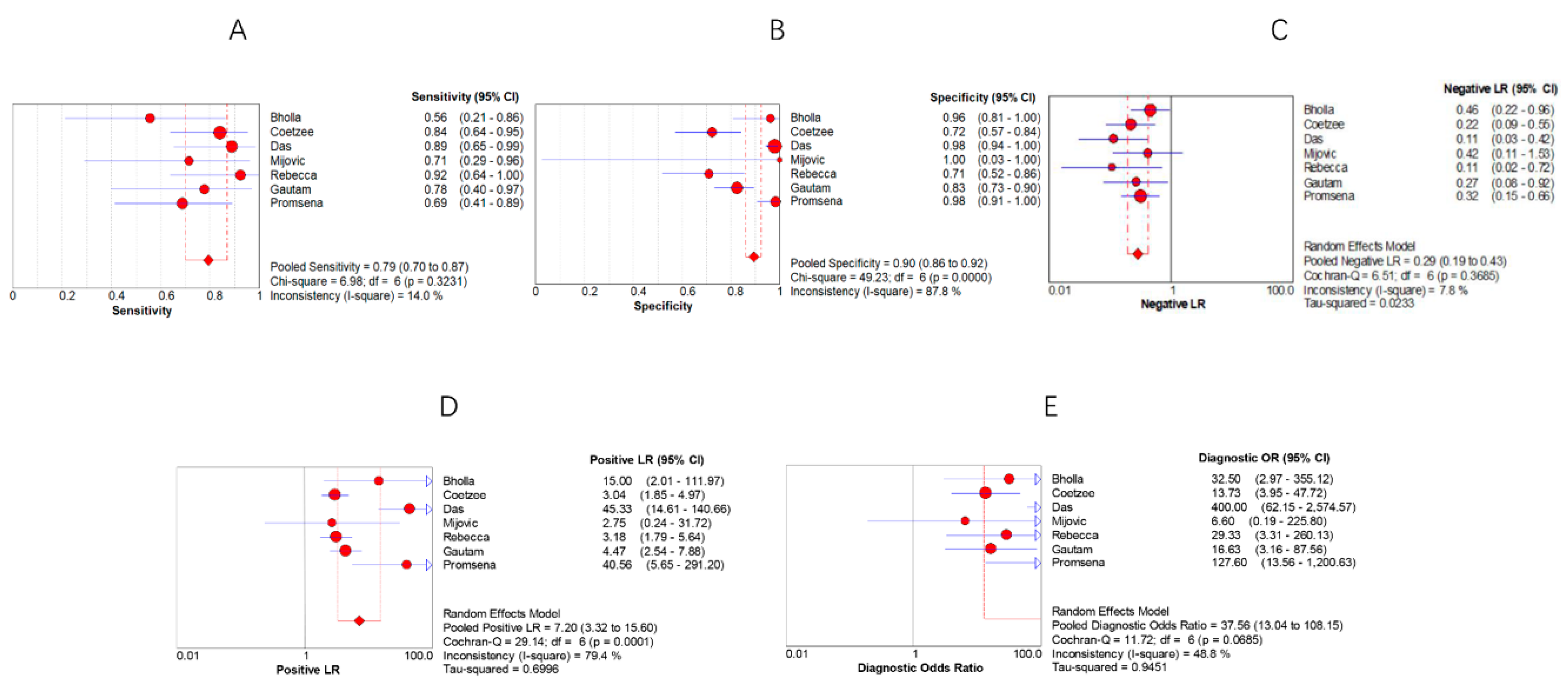
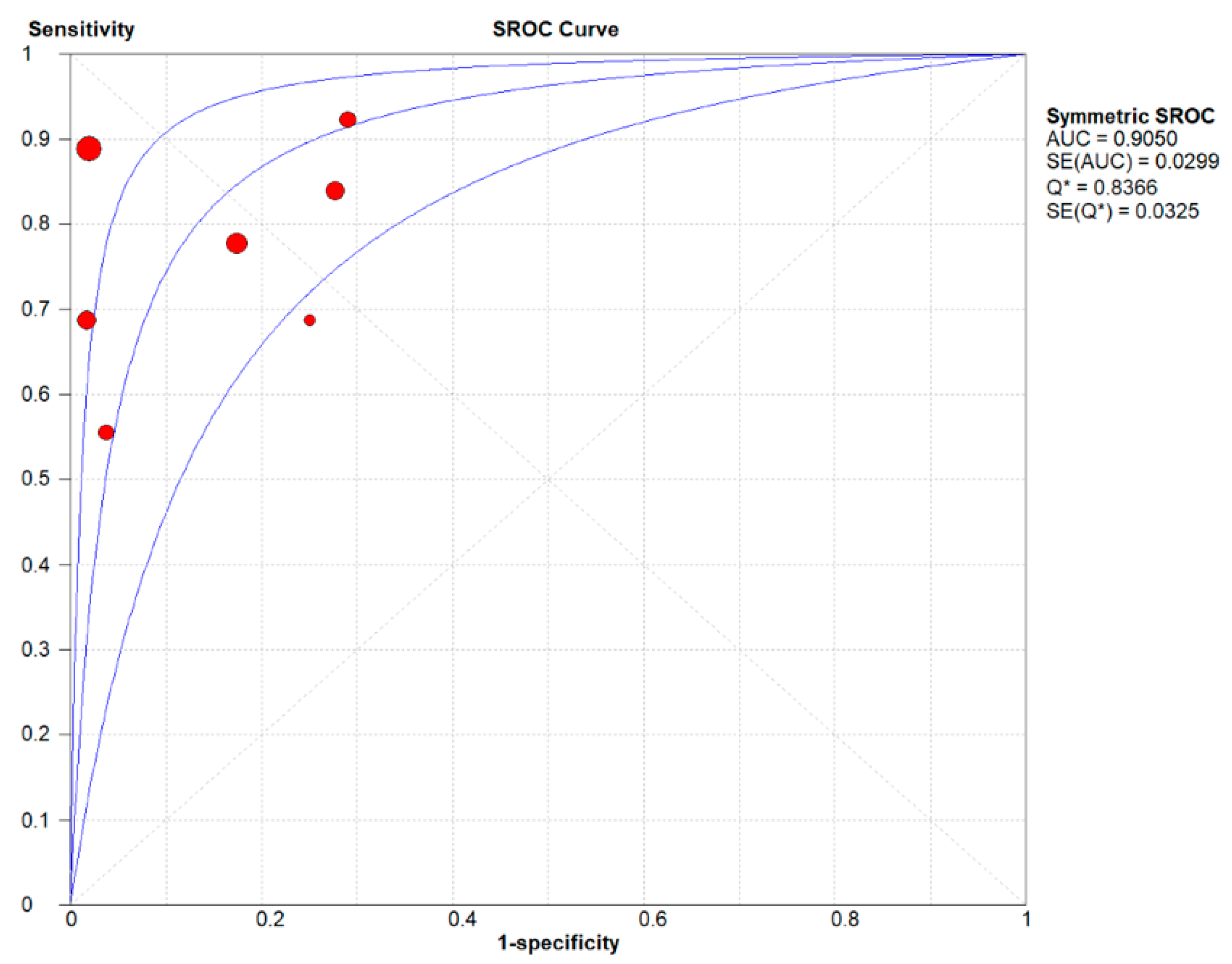
3.4. Summary Results
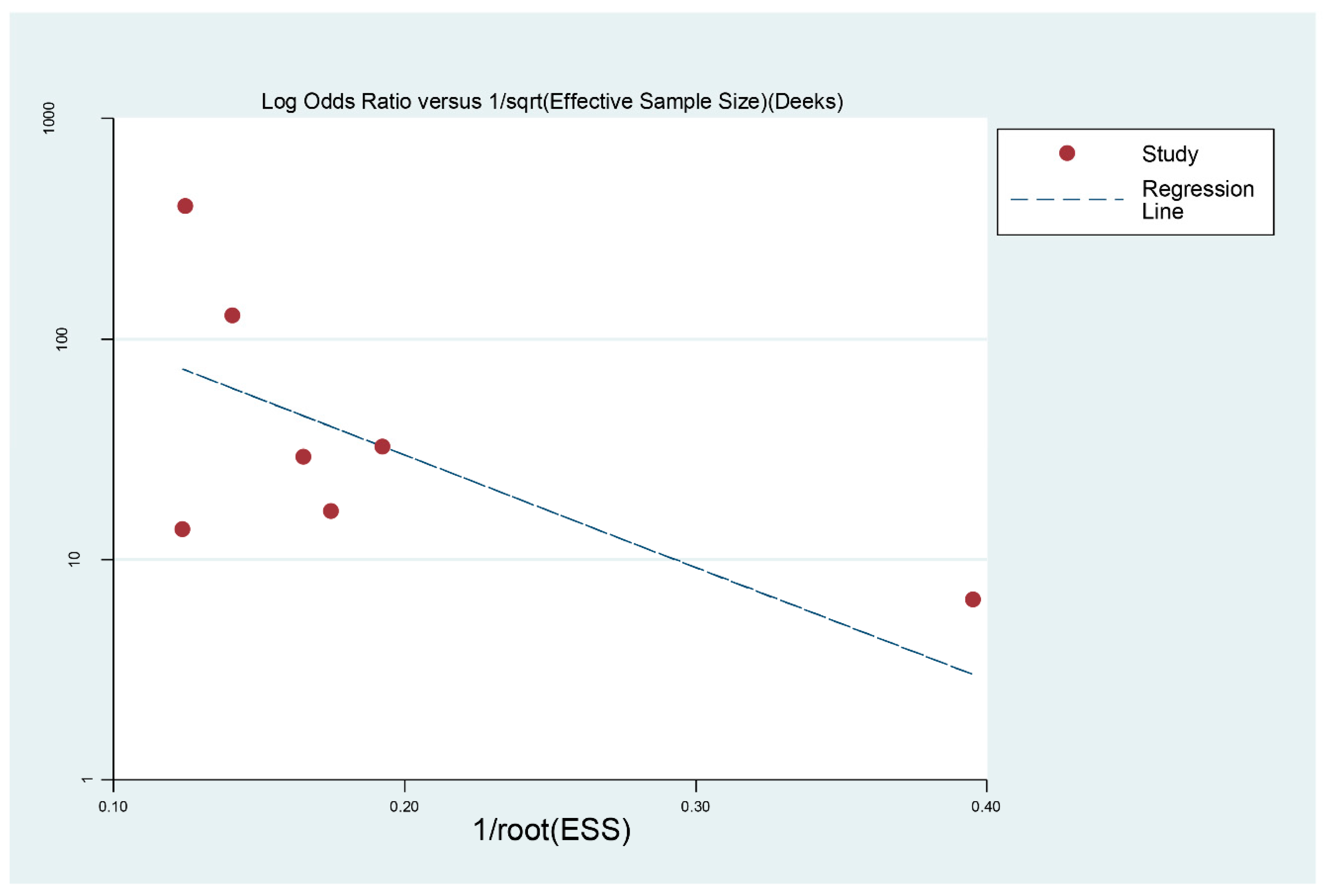
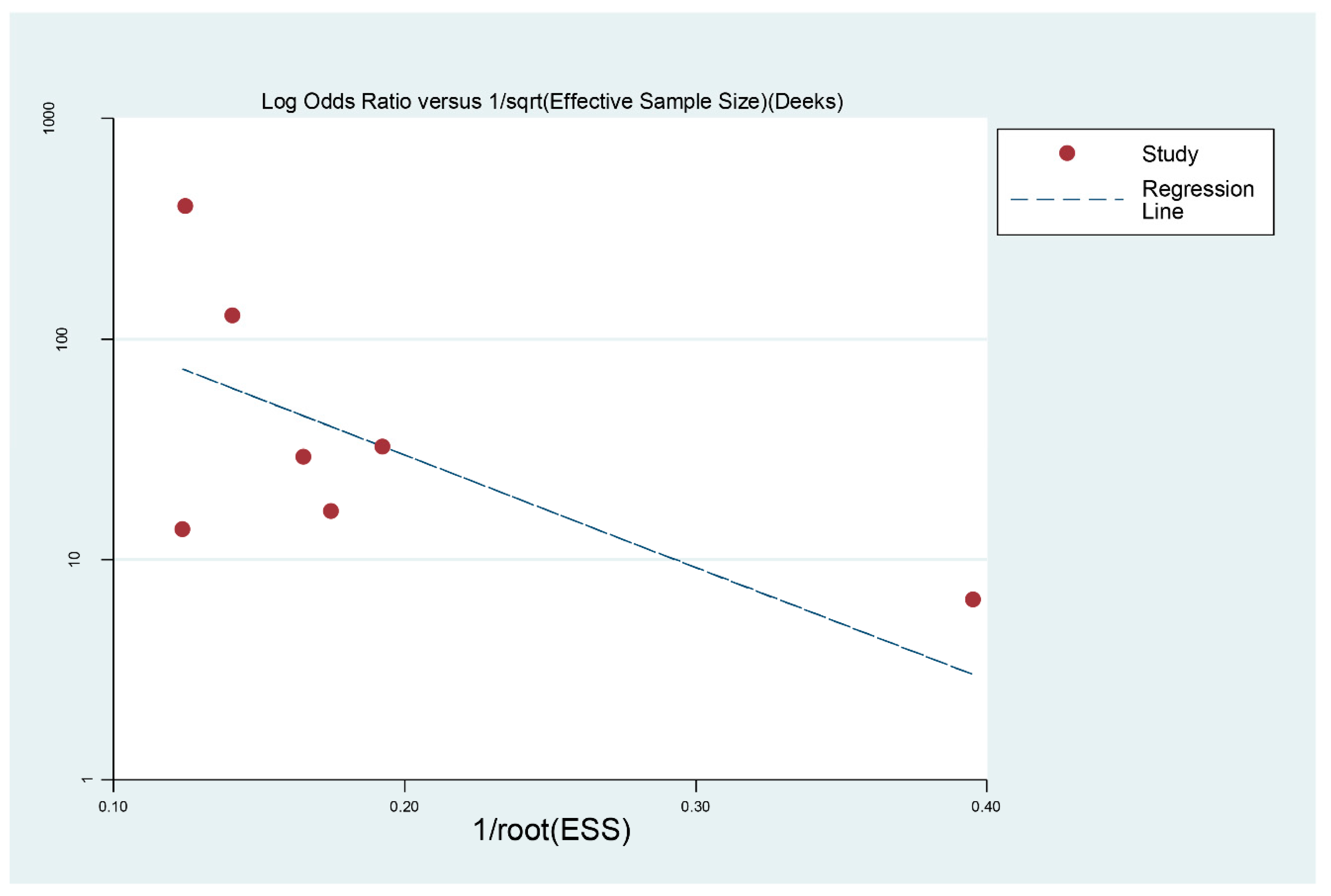
3.5. Publication Bias
4. Discussion
5. Summary
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Nelson, L.J.; Wells, C.D. Global epidemiology of childhood tuberculosis. Int. J. Tuberc. Lung Dis. 2004, 8, 636–647. [Google Scholar]
- Carvalho, I.; Goletti, D.; Manga, S.; Silva, D.R.; Manissero, D.; Migliori, G. Managing latent tuberculosis infection and tuberculosis in children. Pulmonology 2018, 24, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.E.; Young, S.M.; Antoniskis, D.; Davidson, P.T.; Kramer, F.; Barnes, P.F. Relationship of the manifestations of tuberculosis to CD4 cell counts in patients with human immunodeficiency virus infection. Am. Rev. Respir Dis. 1993, 148, 1292–1297. [Google Scholar] [CrossRef] [PubMed]
- Ketata, W.; Rekik, W.K.; Ayadi, H.; Kammoun, S. Extrapulmonary tuberculosis. Rev. Pneumol. Clin. 2015, 71, 83–92. [Google Scholar] [CrossRef]
- Wu, X.R.; Yin, Q.Q.; Jiao, A.X.; Xu, B.P.; Sun, L.; Jiao, W.W.; Xiao, J.; Miao, Q.; Shen, C.; Liu, F.; et al. Pediatric tuberculosis at Beijing Children’s Hospital: 2002–2010. Pediatrics 2012, 130, e1433–e1440. [Google Scholar] [CrossRef] [Green Version]
- Vallejo, J.G.; Ong, L.T.; Starke, J.R. Clinical features, diagnosis, and treatment of tuberculosis in infants. Pediatrics 1994, 94, 1–7. [Google Scholar] [CrossRef]
- Popescu, M.R.; Călin, G.; Strâmbu, I.; Olaru, M.; Bălăşoiu, M.; Huplea, V.; Zdrancotă, C.; Pleşea, R.M.; Enache, S.D.; Pleşea, I.E. Lymph node tuberculosis—An attempt of clinico-morphological study and review of the literature. Rom. J. Morphol. Embryol. Rev. Roum. Morphol. Embryol. 2014, 55, 553–567. [Google Scholar]
- Marais, B.J.; Gie, R.P.; Schaaf, H.S.; Hesseling, A.C.; Obihara, C.C.; Starke, J.J.; Enarson, D.A.; Donald, P.R.; Beyers, N. The natural history of childhood intra-thoracic tuberculosis: A critical review of literature from the pre-chemotherapy era. Int. J. Tuberc. Lung Dis. 2004, 8, 392–402. [Google Scholar] [PubMed]
- Ganchua, S.K.C.; Cadena, A.M.; Maiello, P.; Gideon, H.P.; Myers, A.J.; Junecko, B.F.; Klein, E.C.; Lin, P.L.; Mattila, J.T.; Flynn, J.L. Lymph nodes are sites of prolonged bacterial persistence during Mycobacterium tuberculosis infection in macaques. PLoS Pathog. 2018, 14, e1007337. [Google Scholar] [CrossRef] [PubMed]
- Kang, W.; Yu, J.; Du, J.; Yang, S.; Chen, H.; Liu, J.; Ma, J.; Li, M.; Qin, J.; Shu, W.; et al. The epidemiology of extrapulmonary tuberculosis in China: A large-scale multi-center observational study. PLoS ONE 2020, 15, e0237753. [Google Scholar] [CrossRef] [PubMed]
- Vonasek, B.; Ness, T.; Takwoingi, Y.; Kay, A.W.; van Wyk, S.S.; Ouellette, L.; Marais, B.J.; Steingart, K.R.; Mandalakas, A.M. Screening tests for active pulmonary tuberculosis in children. Cochrane Database Syst. Rev. 2021, 6, Cd013693. [Google Scholar] [CrossRef] [PubMed]
- Cruz, A.T.; Hwang, K.M.; Birnbaum, G.D.; Starke, J.R. Adolescents with tuberculosis: A review of 145 cases. Pediatr. Infect Dis. J. 2013, 32, 937–941. [Google Scholar] [CrossRef] [PubMed]
- Roya-Pabon, C.L.; Perez-Velez, C.M. Tuberculosis exposure, infection and disease in children: A systematic diagnostic approach. Pneumonia 2016, 8, 23. [Google Scholar] [CrossRef] [Green Version]
- Honoré-Bouakline, S.; Vincensini, J.P.; Giacuzzo, V.; Lagrange, P.H.; Herrmann, J.L. Rapid diagnosis of extrapulmonary tuberculosis by PCR: Impact of sample preparation and DNA extraction. J. Clin. Microbiol. 2003, 41, 2323–2329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muluye, D.; Biadgo, B.; Woldegerima, E.; Ambachew, A. Prevalence of tuberculous lymphadenitis in Gondar University Hospital, Northwest Ethiopia. BMC Public Health 2013, 13, 435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gouda, K.; Das, U.; Dhangadamajhi, G. Utility of Fine Needle Aspiration Cytology (FNAC) in the diagnosis of tuberculous lymphadenitis compared to GeneXpert in a tertiary health care center in Northern Odisha, India. Indian J. Tuberc. 2021, 68, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Chao, S.S.; Loh, K.S.; Tan, K.K.; Chong, S.M. Tuberculous and nontuberculous cervical lymphadenitis: A clinical review. Otolaryngol. Head Neck Surg. 2002, 126, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Derese, Y.; Hailu, E.; Assefa, T.; Bekele, Y.; Mihret, A.; Aseffa, A.; Hussien, J.; Ali, I.; Abebe, M. Comparison of PCR with standard culture of fine needle aspiration samples in the diagnosis of tuberculosis lymphadenitis. J. Infect. Dev. Ctries. 2012, 6, 53–57. [Google Scholar] [CrossRef]
- Fantahun, M.; Kebede, A.; Yenew, B.; Gemechu, T.; Mamuye, Y.; Tadesse, M.; Brhane, B.; Jibriel, A.; Solomon, D.; Yaregal, Z. Diagnostic accuracy of Xpert MTB/RIF assay and non-molecular methods for the diagnosis of tuberculosis lymphadenitis. PLoS ONE 2019, 14, e0222402. [Google Scholar] [CrossRef] [Green Version]
- Opota, O.; Mazza-Stalder, J.; Greub, G.; Jaton, K. The rapid molecular test Xpert MTB/RIF ultra: Towards improved tuberculosis diagnosis and rifampicin resistance detection. Clin. Microbiol. Infect. 2019, 25, 1370–1376. [Google Scholar] [CrossRef] [Green Version]
- Nataraj, G.; Kurup, S.; Pandit, A.; Mehta, P. Correlation of fine needle aspiration cytology, smear and culture in tuberculous lymphadenitis: A prospective study. J. Postgrad. Med. 2002, 48, 113–116. [Google Scholar]
- Coetzee, L.; Nicol, M.P.; Jacobson, R.; Schubert, P.T.; van Helden, P.D.; Warren, R.M.; Wright, C.A. Rapid diagnosis of pediatric mycobacterial lymphadenitis using fine needle aspiration biopsy. Pediatr. Infect. Dis. J. 2014, 33, 893–896. [Google Scholar] [CrossRef] [PubMed]
- Bholla, M.; Kapalata, N.; Masika, E.; Chande, H.; Jugheli, L.; Sasamalo, M.; Glass, T.R.; Beck, H.-P.; Reither, K. Evaluation of Xpert (R) MTB/RIF and Ustar EasyNAT (TM) TB IAD for diagnosis of tuberculous lymphadenitis of children in Tanzania: A prospective descriptive study. BMC Infect. Dis. 2016, 16, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, A.; Anupurba, S.; Mishra, O.P.; Banerjee, T.; Tripathi, R. Evaluation of Xpert MTB/RIF Assay for Diagnosis of Tuberculosis in Children. J. Trop. Pediatrics 2019, 65, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Rebecca, B.; Chacko, A.; Verghese, V.; Rose, W. Spectrum of Pediatric Tuberculosis in a Tertiary Care Setting in South India. J. Trop. Pediatrics 2018, 64, 544–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mijovic, H.; Al-Nasser, Y.; Al-Rawahi, G.N.; Roberts, A.D. Contribution of Real-Time Xpert MTB/RIF Testing to Establishing Early Diagnosis of Pediatric Extrapulmonary Tuberculosis in a Nonendemic Setting A Case Series. Pediatric Infect. Dis. J. 2019, 38, 1249–1251. [Google Scholar] [CrossRef] [PubMed]
- Gautam, H.; Singla, M.; Jain, R.; Lodha, R.; Kabra, S.K.; Singh, U.B. Point-of-care urine lipoarabinomannan antigen detection for diagnosis of tuberculosis in children. Int. J. Tuberc. Lung Dis. 2019, 23, 714–719. [Google Scholar] [CrossRef]
- Aurilio, R.B.; Marsili, V.V.; Santos Malaquias, T.d.S.; Kritski, A.L.; Sant’Anna, C.C. The use of Gene-Xpert MTB RIF in the diagnosis of extrapulmonary tuberculosis in childhood and adolescence. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200104. [Google Scholar] [CrossRef]
- Promsena, P.; Jantarabenjakul, W.; Suntarattiwong, P.; Sudjaritruk, T.; Anugulruengkitt, S.; Rotcheewaphan, S.; Petsong, S.; Sawangsinth, P.; Sophonphan, J.; Tawan, M.; et al. Diagnostic Accuracy of Loop-Mediated Isothermal Amplification (TB-LAMP) for Tuberculosis in Children. J. Pediatric Infect. Dis. Soc. 2021, 11, 9–15. [Google Scholar] [CrossRef]
- Kay, A.W.; González Fernández, L.; Takwoingi, Y.; Eisenhut, M.; Detjen, A.K.; Steingart, K.R.; Mandalakas, A.M. Xpert MTB/RIF and Xpert MTB/RIF Ultra assays for active tuberculosis and rifampicin resistance in children. Cochrane Database Syst. Rev. 2020, 8, Cd013359. [Google Scholar] [CrossRef]
- Seo, Y.S.; Kang, J.M.; Kim, D.S.; Ahn, J.G. Xpert MTB/RIF assay for diagnosis of extrapulmonary tuberculosis in children: A systematic review and meta-analysis. BMC Infect. Dis. 2020, 20, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NO. | Author | Year | Study Design | Country | Source of Specimens | Gold Standard | Type of Apecimens | TP | FP | FN | TN |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Coetzee [22] | 2014 | Prospective | South Africa | 72 clinical specimens | Culture | fine needle aspiration biopsy (FNAB) | 21 | 13 | 4 | 34 |
| 2 | Bholla [23] | 2016 | Prospective | Tanzania | 36 clinical specimens | Culture | fine needle aspirates of lymph nodes | 5 | 1 | 4 | 26 |
| 3 | Das [24] | 2018 | Prospective | India | 171 clinical specimens | Culture | gastric aspirates, cerebrospinal fluids, induced sputum and lymph node aspirates | 16 | 3 | 2 | 150 |
| 4 | Rebecca [25] | 2018 | Retrospective | India | 44 clinical specimens | Culture | extrapulmonary specimens | 12 | 9 | 1 | 22 |
| 5 | Mijovic [26] | 2019 | Prospective | India | 8 clinical specimens | Culture | respiratory and extrapulmonary specimens | 5 | 0 | 2 | 1 |
| 6 | Gautam [27] | 2019 | Prospective | India | 101 clinical specimens | Culture | fine-needle cytological aspirates | 7 | 16 | 2 | 76 |
| 7 | Aurilio [28] | 2020 | Retrospective | Brazil | 20 clinical specimens | Culture | Cervical LNTB, Supraclavicular LNTB, Axillar LNTB, Inguinal LNTB | 5 | 0 | 4 | 11 |
| 8 | Promsena [29] | 2021 | Prospective | Thailand | 75 clinical specimens | Culture | lymph nodes tissue from fine-needle aspiration or biopsy | 11 | 1 | 5 | 58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.-K.; Liu, R.-S.; Wang, Y.-X.; Quan, E.-X.; Liu, Y.-H.; Guo, X.-G. Xpert MTB/RIF Assay for the Diagnosis of Lymph Node Tuberculosis in Children: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 4616. https://doi.org/10.3390/jcm11154616
Chen H-K, Liu R-S, Wang Y-X, Quan E-X, Liu Y-H, Guo X-G. Xpert MTB/RIF Assay for the Diagnosis of Lymph Node Tuberculosis in Children: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(15):4616. https://doi.org/10.3390/jcm11154616
Chicago/Turabian StyleChen, Hao-Kai, Rui-Si Liu, Yi-Xuan Wang, En-Xiang Quan, Yuan-Hua Liu, and Xu-Guang Guo. 2022. "Xpert MTB/RIF Assay for the Diagnosis of Lymph Node Tuberculosis in Children: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 15: 4616. https://doi.org/10.3390/jcm11154616
APA StyleChen, H.-K., Liu, R.-S., Wang, Y.-X., Quan, E.-X., Liu, Y.-H., & Guo, X.-G. (2022). Xpert MTB/RIF Assay for the Diagnosis of Lymph Node Tuberculosis in Children: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(15), 4616. https://doi.org/10.3390/jcm11154616