
Introducing the Postpartum Toolkit: An Examination of the Feasibility, Acceptability and Pilot Efficacy of an Online Clinical Tool to Enhance Postpartum Functioning and Emotional Wellbeing

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Postpartum Toolkit
- Whether the checklist of items produced from the qualitative data appear theoretically complete. If it does not appear complete, what items should be added?
- Whether there are additional resources that should be incorporated into the feedback to address checklist items?
- What if anything about the way the checklist and feedback is presented (phrasing of information, means of delivering the feedback, etc.) could be improved upon to increase the inclusivity of this tool and/or generally improve the tool?
2.2. Participants
2.3. Data Collection and Procedure
- The degree to which the resources that they were given matched their needs (rated 1–10 with a higher rating indicating a better match).
- The degree to which the resources that they were given were found to be useful (rated 1–10 with a higher rating indicating a higher level of usefulness).
- Whether they used the resources (dichotomous yes/no options for response; if participants responded “yes” a checklist of the resources they were given in their feedback appeared and they were asked to select which resources were used).
- Whether there are resources which they have not yet used but intend to use (dichotomous yes/no options for response; if participants responded “yes” a checklist of the resources they were given in their feedback appeared and they were asked to select which resources have not yet been used but they intend to use).
- How often they referenced their feedback (there were multiple choice options for response).
- If they did not use the resources, what got in the way (there were multiple choice options for response and participants could select all that applied).
- Whether there are other factors which should be included in the checklist (items were listed for participant reference and participants were given a dichotomous yes/no option for response; if they responded “yes” a textbox appeared in which they could specify suggested additions).
- Whether there is anything else that could be included in the feedback/resources (dichotomous yes/no options for response; if they responded “yes” a textbox appeared in which they could specify suggested additions).
- Whether there were other resources which the participant used which were not featured in the feedback list (if they responded “yes” a textbox appeared in which they could specify the resource(s) used).
- Whether participants would have been more likely to use these resources if they had a person introducing them to the resources rather than guiding themselves through feedback that was provided automatically (dichotomous yes/no options for response).
- Other suggestions to improve the tool (dichotomous yes/no options for response; if they responded “yes” indicating they had suggestions, a textbox appeared in which they could specify suggested additions).
2.4. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.1.1. Less-Privileged Subgroup Analysis of Baseline Characteristics
3.1.2. Male-Identifying Subgroup Analysis
3.2. Feasibility of The Postpartum Toolkit
Less-Privileged Subgroup Analysis of the Feasibility of The Postpartum Toolkit
3.3. Acceptability of the Postpartum Toolkit
Less-Privileged Subgroup Analysis of Acceptability of The Postpartum Toolkit
3.4. Pilot Efficacy of The Postpartum Toolkit
Additional Exploratory Efficacy Analysis
3.5. Participant Suggestions for Improving the Postpartum Toolkit
4. Discussion
Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. The Postpartum Toolkit Checklist
| 1. When things don’t go well, I don’t blame myself. | This is not an issue for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 2. When trying new things, I do all of the following: I am patient with myself and don’t expect myself to get things right away I feel comfortable pushing myself beyond my comfort zone I can be flexible with my plans and expectations. | This is a strength for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 3. My baby and I are bonding. | This is going well for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 4. Most of the time my baby’s crying doesn’t overwhelm me. | This is a strength for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 5. Most of the time I am able to calm myself down when I have strong emotions (such as stress, worries, anger) or distressing thoughts. | This is a strength for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 6. I have people in my life that help to make sure I’m taking care of myself. For example, people in my life check-in with me about taking care of myself, or they help me to take care of myself by doing things like watching the baby. | This is going well for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 7. I am able to get the materials I need to take care of the baby and myself (such as diapers and food). | This is not an issue for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 8. I am getting more experienced with taking care of my baby. | This is going well for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 9. When I do things well, I am able to give myself credit for it. | This is a strength for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 10. If you have people in your life who help and support you: when I am talking to people in my life who help or support me, I do all of the following: I can be open and honest I can trust people to help me I can ask for help and take help when it is offered | This is a strength for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 11. I have been able to get my baby into a routine. | This is going well for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 12. When I have a question about parenting or early motherhood, I know how to get an answer that I trust. | This is going well for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 13. I am involved in activities outside of the house (such as friendships, hobbies, professional or volunteer work). | This is going well for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 14. I know myself (when I need to ask for help, what I need, what makes me feel better when I feel down, worried, or stressed). | This is a strength for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 15. My home environment is safe and stable. | This is not an issue for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 16. I know that taking care of myself is important, and guilt does not get in the way of taking care of my own needs. | This is a strength for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 17. I am able to sleep at night when my baby is sleeping. | This is going well for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 18. When thinking about social pressures, I don’t do any of the following: feel like I have to reach the expectations of others worry about other people’s judgments of me compare myself to others. | This is a strength for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 19. I plan and manage time well. | This is a strength for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 20. I have people in my life that I can talk to openly and honestly about my feelings and experiences. | This is not an issue for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 21. I have people to help me with childcare and household management (cooking, cleaning, shopping, etc.). | This is not an issue for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 22. I understand what my baby is trying to tell me (through their cries, body language, etc.). | This is a strength for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 23. If you or your co-parent are currently working: my workplace/my partner’s workplace has been understanding and flexible since I have had my baby. | This is not an issue for me. | This is going ok for me, but could be better. | I’d like help with this. |
| 24. I am not experiencing physical pain or discomfort. | This is not an issue for me. | This is going ok for me, but could be better. | I’d like help with this. |
Appendix B. Alphabetized List of Resources (as Presented to Participants with the Exception of the Removal of Embedded Videos; There is Text to Indicate where the Videos Would Appear)
| A | Question self-blame Parents have a tendency to blame themselves, even when they know things are outside of their control. As one mom said, “Everything that happens is something that you could have affected. And so if things are going poorly you must be doing poorly. To some extent, it’s like some of us get lucky to have things go well at certain points in time and some of us don’t, and that affects how well we can feel like things are getting better.” When you feel yourself taking on blame for something that has gone wrong, ask yourself if your view is accurate. Was what happened really something you could have controlled? This takes practice, but there are exercises you can perform which can get you into the habit of questioning the blame you may be putting on yourself. One exercise is called “Retelling your own story” from Getting Our of Your Mind and Into Your Life by Dr. Steven Hayes. This exercise involves writing down a paragraph to describe a recent event that brought about thoughts of self-blame. After you finish, underline the facts of the story (the aspects of the story that everyone would agree are true regardless of their point of view). Then, write a different story including the same facts. This is a great way of showing you that facts become relevant because of the story that you tell around them, and you have more control over this story than you may think. Here is another exercise: in a paper journal or a notepad app in your phone, write down the “evidence” that you are to blame for a recent event that brought about thoughts of self-blame. Then, write down the “evidence” against blaming yourself. Remember, you want to use fact, not guesses, interpretations, or opinions. This may be hard to do at first, but over time you will become better at seeing the evidence from both sides, and you will see that your responses are not driven by events alone, but also your thoughts and emotions in response to events. |
| B. | Increase self-compassion Work to foster self-compassion, which helps you to see yourself (both strengths and weaknesses) without judgment, and to accept yourself as you are. In short, it is learning to treat yourself like a good friend. As one mother told us: “I think it’s important to not put in too much from yourself. So give yourself some grace and knowing by yourself that you’re doing a good job, even if you don’t feel it at the time.” There is research to show that when we are more self-compassionate, and less self-critical, we are better off. Self-compassion is linked to positive emotions and better overall outcomes, while self-criticism is linked to negative emotions and worse overall outcomes. While we might think being more critical of ourselves will make us more successful, that is not what the research on self-compassion suggests. To give yourself a taste of what this feels like, try the following few steps taught by self-compassion expert Dr. Kristin Neff when you are feeling low, sad, or stressed: Validate your own feelings. Tell yourself “this is hard right now.” Acknowledge that feeling badly, and even suffering, is part of the human experience. You are not alone in this. Bring some words of kindness to yourself. You might say to yourself the things you would say to a good friend such as “I’m sorry this is hard, what can I do to help? I am here for you.” If you want to learn more, there is a free course about self-compassion available at the following link: https://product.soundstrue.com/power-of-self-compassion/free-video-series/?ck_subscriber_id=597375296 The University of California at Los Angeles also has a free meditation that works to foster a sense of loving kindness, give it a try at the following link: https://www.uclahealth.org/marc/mpeg/05_Loving_Kindness_Meditation.mp3 |
| C | Consider seeking professional mental health support It can be helpful to have the support of a psychotherapist or counselor to sort through everything that you are experiencing. The transition to parenting a new baby is tough, and a psychotherapist or counselor can help to support you through all the changes (in your body, relationships, identity) that are happening, and teach you tools to help manage stressors you may be experiencing. Also, as someone outside of your circle of family and circle of friends, you can feel comfortable speaking openly about your relationships. You don’t have to fear that you are putting your thoughts and emotions onto someone else, because it is a psychotherapist or counselor’s job to listen and support you. As one mother described what helped her to adjust after having a new baby: “ I’m going to therapy. I’m talking, I’m communicating, I’m asking for help, I’m asking for support, and I’m getting past day by day.” Here are some places to start when trying to find a psychotherapist or counselor: Postpartum Support International (https://www.postpartum.net/get-help/help-for-moms/) is a good place to look for help in your area because they have information about psychotherapists, counselors, and programs that specifically work with people who have recently had a baby. You can call or text their toll-free helpline at 1-800-944-4773(4PPD) for basic information, support, and resources in your area. If you have health insurance, you can call your insurance company to ask for psychotherapists or counselors in your area. Go to the website Psychology Today (https://www.psychologytoday.com/us) and use their “find a therapist” search bar. You can enter your zip code to find providers near you. Once you have entered your zip code and press the enter key, results will appear. A column will also appear on the left-hand side of the screen and will allow you to select even more specific information about the psychotherapist or counselor you are looking for (your insurance, the issues you would like to focus on, etc.). Here is a specific directory you can use to look for psychotherapists with expertise treating Black women: https://providers.therapyforblackgirls.com/ If you do not have health insurance, you can consider searching local training clinics that offer a sliding fee scale they do not have one set price but set a price based upon how much you can pay. To do this, search on the internet “psychology training clinics near me”. Or, you can try to find a Volunteers in Medicine clinic near you and see if they offer mental health services: https://vimamerica.org/clinics/ There are also several websites organized by professional associations that have searchable directories of mental health providers: The Substance Abuse and Mental Health Services Administration: https://findtreatment.samhsa.gov/ The American Psychological Association: https://locator.apa.org/ The Association for Behavioral and Cognitive Therapies: https://www.findcbt.org/FAT/ Some people benefit from an intensive outpatient program (IOP), which usually involves receiving care from multiple providers and attending more frequent appointments (usually multiple appointments a week) as part of one program. If you are feeling that it is hard to get through the day due to low mood, lots of worries, or other concerns related to your mental health, one of these programs may be helpful for you. See the list below for the locations of intensive programs in the United States: https://www.postpartum.net/get-help/intensive-perinatal-psych-treatment-in-the-us/ |
| D | Use positive affirmations Use positive affirmations when you are feeling anxious and distressed about trying something new. Research shows that this can help to increase your self-worth and improve your mindset. Positive affirmations are positive phrases or statements that you can use to encourage yourself. You can post them around your house or car or you can simply repeat them. Some examples are below. If you don’t connect with any of these, you are welcome to write your own! I am allowing myself space to grow and learn I am letting myself just “be”, without judgment I am accepting my emotions and letting them serve their purpose For more information, visit the following link: https://theblissfulmind.com/positive-affirmations-list/ |
| E | Get some distance from your thoughts Sometimes you may have thoughts that feel much bigger than just thoughts. For example, you may have a thought that you are not meeting your expectations, you may think that you should feel guilty for taking time for yourself, or you may have a thought that others are judging you to be a bad parent. As one mom told us: “Expectations get in your way a lot because you think it’s going to be one way and then…it can feel like a letdown. You can feel like you are failing one after the other, when really it’s just because your expectation is not being met, which is not the same as failing. Bottle-feeding your baby is not the same as failing at breastfeeding. And it probably took me until a month ago to realize.” When you think these things, you have an emotional response, and it may change the way you see yourself. This can be distressing. While these thoughts will be a part of life, you can work to gain a little bit of distance from the thoughts, which will in turn lessen their effect on our emotions and understanding of yourself. There are several techniques for making your distressing thoughts less powerful. Listed below are a few discussed by Dr. Steven Hayes, You can “thank your brain” for having the thoughts. You even just say to yourself “I notice myself having the thought that…” Or you can engage in a meditation, taking a few moments to visualize your thoughts like leaves on a stream. Place each thought that enters your mind on a leaf on the stream and letting it float past. For guidance through this exercise check out the video below, created by Inner Melbourne Clinical Psychology. It is also available at this link: https://www.youtube.com/watch?v=00AbNXNLUUs While these may seem silly, doing things like this will remind you that your thoughts are just thoughts, and allowing yourself to observe them rather than have them “take over” can have a powerful influence on the distress you feel when these thoughts arise. [EMBEDDED LEAVES ON A STREAM VIDEO] |
| F | Learn about bonding with your baby Remind yourself that there is no one “right” way to feel about your relationship with your baby, even if others expect you to feel a certain way. Give yourself time to get to know your baby and trust that you will become closer to the baby over time. In the meantime, the tips below might help you to find new, fun ways to grow closer to your baby. Use the links below to learn about how your baby is developing, and what you can do to encourage growth in your baby while also bonding with them. https://talkingisteaching.org/resources https://www.zerotothree.org/resources/161-development-from-birth-to-12-months-old-forming-a-trusting-bond-to-nurture-learning#downloads https://www.babycenter.com/2_creating-an-attachment-with-your-baby_10350318.bc You may also want to try the free app Vroom, which offers a set of tools and resources to turn everyday moments into “brain building” moments that you and your infant can share together. They also have documents that you can print if you would prefer to not use the app! Learn more at this link: https://www.vroom.org/ You may also like the apps BabySparks (https://babysparks.com/) or Kinedu (https://www.kinedu.com/) help parents support healthy development through play. Use the links below to learn about activities that experts suggest can be helpful for bonding with your baby: https://www.zerotothree.org/resources/1077-activities-for-bonding-and-learning-from-birth-to-12-months https://www.zerotothree.org/resources/2924-6-ways-to-bond-while-you-re-on-the-move The video below was created by YMC Motherhood Unfiltered and is also available at the following link: https://www.youtube.com/watch?v=4VuEIeDrwAM [EMBEDDED YMC MOTHERHOOD UNFILTERED VIDEO] If you have the time, build infant massage into your daily routine. Evidence shows it has lots of benefits for you and baby, including helping you to bond with one another. The video below, created by Cincinnati Children’s, shows you how to get started and is also available at this link: https://www.youtube.com/watch?v=CJPu_bDus3Q [EMBEDDED INFANT MASSAGE VIDEO] Try to be present with your baby. As best you can, avoid activities like scrolling on your phone during time with your baby. Also, keep in mind that these opportunities for bonding may not always be at the times you planned. When your baby is in a playful mood, take advantage of this time. Lean in and let yourself enjoy it. |
| G | Calm your baby and yourself through crying spells Infant crying is very distressing for parents. One mom described how upsetting crying can be by saying: “[My baby] cried for like 45 min straight and I mean it’s so wearing…It’s the worst thing.” It can be helpful to learn from experts about infant crying and how to soothe your baby so that you feel prepared to calm your baby the next time they cry. Helpful links are listed below: https://www.zerotothree.org/resources/272-coping-with-crying-in-babies-and-toddlers The video below was created by Eugene Pediatrics Associates and is also available at this link: https://www.youtube.com/watch?v=Y6TVv85NPlw [EMBEDDED VIDEO] The video below, created by Real Happy Endings, talks about the Book Happiest Baby on the Block by Dr. Harvey Karp. It gives information about calming very young babies (first few months of life). It is also available at this link: https://www.youtube.com/watch?v=crdQy8zliZw. [EMBEDDED VIDEO] If you suspect that your baby is experiencing discomfort, some ways to relieve this are: sucking (either to feed or on a pacifier), security (swaddling the baby, being wrapped up reminds them of being in their mother’s belly which calms them down), shushing (making a shhhh sound or playing white noise) One note, if your baby is in the hospital or experiencing a medical condition, check with their doctor first before trying new things. The video below, created by FirstCry Parenting, is about crying at night. It is also available at this link: https://www.youtube.com/watch?v=3ckmDR7oNbQ [EMBEDDED VIDEO] However, even when you have information about why babies cry and how to soothe them, sometimes you still won’t be able to stop them from crying. If it is safe to do so (you can leave baby in a safe place or can have someone else take over care) during those times, allow yourself to take a break and do something calming for yourself. You might consider taking “shifts” with a co-parent, friend, or other support person. Allowing yourself some time away from the baby can reduce your stress and help you feel more able to tackle the problem of soothing your infant. Also, your baby can sense your energy, if you are calmer, it is likely this will help your baby to become calmer. One way to calm yourself in the moment is through your breathing. Take breaths in through your nose and out through your mouth. Try your best to make the outbreath last longer than the inbreath, as the outbreath has a strong impact on slowing down your heart rate and calming your body down. Also make sure you are “belly breathing” (your belly rises with your inhale; you might imagine wearing pants that are too big and breathing out to hold the pants up). Belly breathing prevents you from shallow “chest breathing” which can increase your anxiety. The video below, created by The Somerville Foundation, shows you how to breathe in a calming way. It is also available at this link: https://www.youtube.com/watch?v=4e3Csho8CBw [EMBEDDED VIDEO] For other calming breathing techniques check out this article: https://greatist.com/happiness/breathing-exercises-relax#Why-controlled-breathing? |
| H | Gain some tools to help you manage strong emotions Especially with all of the changes you are going through (in your body, in your relationships, to your sleeping routine), it is normal to have strong emotions like frustration, stress, or anxiety. One way to calm yourself when you are feeling strong emotions is to use mindfulness. Mindfulness is a technique that teaches you to focus on the present moment, acknowledging the thoughts, emotions, and sensations you are experiencing, without judgment. Mindfulness has been shown to decrease sadness and stress and increase happiness and focus. As one mother described using mindfulness: “In preparation for parenthood, I got into mindfulness and meditation, and so that really helped me sort of find space and calmness and ways to just breathe through any stressors or tension, and sort of reassure myself that all the moments are manageable.” But, like any skill, it takes practice to “build up the mindfulness muscle” so that we can put it into play during distressing moments in life when we need it most. The good news is that there are a number of free online resources that you can use to learn about and practice mindfulness. We have collected some here: Mindfulness Coach Smartphone Application, free self-guided training in Mindfulness https://mobile.va.gov/app/mindfulness-coach Headspace Smartphone Application https://www.headspace.com/headspace-meditation-app UCLA Mindfulness meditations https://www.uclahealth.org/marc/mindful-meditations When you feel very strong emotions, like anger or feeling like you can’t stop thinking about and focusing on your worries (this is called “rumination”), there are also several techniques, discussed by Dr. Marsha Linehan, which can help you to calm yourself down and get through difficult moments. Self-soothing Use your five senses to focus on and savor something that is enjoyable to you. See below for some examples for each sense: Vision: look at the sunset, sunrise, or night sky Hearing: listen to music or a podcast that you like Smell: light a scented candle, smell a kitchen item like coffee beans or vanilla extract, or scented soap (like lavender) Taste: drink your favorite soothing drink like tea or hot chocolate Touch: take a hot shower or bath Improve the current moment. If distracting or self-soothing is not working, try to find the meaning in the current moment. If you are religious, pray. As one mom said, “ I literally just pray, definitely pray…That calms me down. Even if it’s outside the kids, praying calms me down.” Perform a body scan, an exercise in which you focus on your experience of sensations in your body. The video below, created by Vanderbilt University, walks you through how to perform a body scan. It is also available at this link: https://www.youtube.com/watch?v=Xo3PetVUcIc [EMBEDDED VIDEO] When other things don’t work, you can do certain things with your body that can help to calm your emotions. Here are some examples: Put cold water or ice packs to your face while holding your breath. This will initiate the human “dive reflex” which will reduce your emotional arousal very quickly. Do intense aerobic exercise (jumping jacks, jogging) of any kind for 20 min. This has been shown to decrease negative mood and give you a positive mood boost. Be careful with this if you are still recovering from birth. You can consult your doctor about what exercise may be appropriate for you. Use slow, paced breathing. The video below, created by The Somerville Foundation, shows you how to breathe in a calming way. It is also available at this link: https://www.youtube.com/watch?v=4e3Csho8CBw [EMBEDDED VIDEO] Use paired muscle relaxation, which involves relaxing your muscles while breathing out. The video below, created by Therapist Aid, shows you how to do a similar exercise called progressive muscle relaxation. It is also available at this link: https://www.youtube.com/watch?v=1nZEdqcGVzo [EMBEDDED VIDEO] If you are experiencing a lot of anxiety, there is a free application that you can download to your smartphone that will teach you research-backed techniques for taking active steps to manage your anxiety: https://www.anxietycanada.com/resources/mindshift-cbt/ |
| I | Consider a postpartum doula Consider seeking support from a postpartum doula. A postpartum doula is a trained professional with knowledge of emotional and physical recovery from childbirth, infant soothing and newborn care, and mother-infant bonding. Having a strong support system is key to a healthy transition after having a baby, and a doula can play a major role in that support. You can think of a doula as someone who can “mother” you while you are adjusting to caring for your baby. For example, a doula can help to answer your questions and provide an extra pair of hands with infant care. For more information, check out this article: https://www.nytimes.com/2018/10/02/style/postpartum-doula.html If you are interested in finding a postpartum doula, here is some advice on how to start your search: Look online, the following websites have searchable directories of doulas, make sure you are searching for/selecting postpartum doulas: https://www.dona.org/what-is-a-doula/find-a-doula/ https://cappa.net/directory/ https://doulatrainingsinternational.com/find-a-doula/ A reproductive justice organization led by Black women, can help match Black parents with a doula https://www.roottrj.org/find-a-doula You can also ask about postpartum doulas from childbirth educators, or parenting support groups in your area. If you are concerned with the cost of a doula, here is some information about paying for postpartum doula services: Look for an organization that trains doulas in your community, you may be able to get a discount if a doula is newly trained. You may be able to pay for a doula from a flexible spending or health savings account. Many doulas operate on a sliding fee scale (they adjust their price based upon what you can pay). Look into Community Doula Programs, which pair women with doula support for low or no cost. Contact your local birth centers, hospitals, or state health department to find out whether there is a community doula program near you. For more information https://www.postpartum.net/get-help/birth-and-postpartum-doulas/ |
| J | Learn about the resources around you Taking care of a baby is expensive. It can be stressful and upsetting to be in the struggle to afford baby supplies. However, below are some organizations that may help get you what you need. Baby Supplies Baby2Baby National Network Distributing Childcare Essentials: https://baby2baby.org/national-network/ Breast pump Contact your insurance provider and ask if they are able to provide you with a breast pump. Under the Affordable Care Act insurance plans must provide breastfeeding support, counseling, and equipment for the duration of breastfeeding Car seat Call your local United Way by dialing 211 on your phone Cribs The following organization provides education on the importance of practicing safe sleep for babies and provide portable cribs to families who, otherwise, cannot afford a safe place for their babies to sleep: https://cribsforkids.org/request-a-crib/ Diapers: The National Diaper Bank Network: https://nationaldiaperbanknetwork.org/get-help-now/ General Supplies Local churches and religious charities can provide support regardless of your personal faith. You can contact your local place of worship to learn about what is available in your area. Below are some religious programs and churches that offer support to low-income families. Catholic Charities USA: https://www.catholiccharitiesusa.org/find-help/ Jewish Federation of North America: https://www.jewishfederations.org/ Lutheran Services: https://www.lutheranservices.org/ United Methodist Church: https://www.umc.org/en/find-a-church Baby Box University Available in select states, provides free sleeping boxes (used like a crib) and samples of products like wipes and diapers. You can register for a free education program and get free baby supplies: https://www.babyboxco.com/classes/login Food: Women Infants and Children (WIC) Special Supplemental Nutrition Program: https://www.fns.usda.gov/wic Gives access to healthy food, nutrition education, breastfeeding guidance Caregivers with a low to medium income and those who are part of other programs such as foster care, medical assistance, or SNAP are eligible Feeding America, national network of food banks: http://www.feedingamerica.org/find-your-local-foodbank/ Supplemental Nutrition Assistance Program (SNAP): https://www.fns.usda.gov/snap/recipient/eligibility Medical Care: Find a Volunteers in Medicine affiliated clinic near you which provides free health care services to the uninsured and medically underserved: https://volunteersinmedicine.org/volunteers-in-medicine-clinic-directory/ Free or reduced cost services (food, medical care), search by zip code to see organizations near you: https://www.auntbertha.com/ |
| K | Learn about baby care It takes time to gain experience in taking care of your baby. Each baby is unique. It is important to keep the learning curve in mind, and to be patient with yourself. However, there are also free and low cost educational materials available online that can help you feel more prepared for the challenges of taking care of a baby. These are organized below by topic. Keep in mind that you can also look for classes at hospitals, preschools, pediatrician offices, or social service facilities in your area General infant care classes and trainings: Low cost online parenting classes covering breastfeeding, sleep, infant CPR, baby care and more: https://www.tinyhood.com/online-parenting-classes Baby Box University has a number of free online classes on topics including breastfeeding, infant brain development, and newborn sleep behavior. You can also get rewards for completing the classes: https://www.babyboxco.com/classes/login Breastfeeding Stanford University short course on breastfeeding: https://www.classcentral.com/course/breastfeeding-10633 Lactation Link’s online breastfeeding course: https://lactationlink.com/free-6-day-course/ Women’s health.gov breastfeeding resources: https://www.womenshealth.gov/patient-materials/resource/guides Breastfeeding Class with Lactation Consultant: https://www.milkandlove.com.au/breastfeeding-online-classes-with-katie-james-ibclc/ The video below, created by The Yellow Nursery, has information on getting a good latch in breastfeeding. It is also available at this link: https://www.youtube.com/watch?v=OUqRVSeBpY8 [EMBEDDED VIDEO] Sleep Expert written resources on sleep: https://www.babysleep.com/ Baby Sleep Made Simple Program: https://www.youtube.com/playlist?list=PLTOm7KLBBnKph5OubZ9pO0EeHcw1jO9W- CPR Online CPR course from RedCross (approximately $35): https://www.redcross.org/take-a-class/classes/child-and-baby-first-aid%2Fcpr%2Faed-online/a6R0V0000015FV5.html |
| L | Increase the power of positive emotions The field of positive psychology, led by Dr. Martin Seligman, focuses on building positive qualities and involves techniques that increase how often and how deeply we experience positive emotions. One aspect of positive psychology that may be particularly helpful to you is increasing your awareness of your successes, and learning to appreciate them. This may be especially helpful because it can be hard to give yourself credit for all the good things you are doing as a parent. As one mom said “It’s hard for people to give themselves positive feedback. So when I do have a meeting or hangout, with one or two moms, you don’t hear as many positive statements about, “Oh, I’m doing a great job.” The good news is that you can teach yourself to notice your successes through practice. One way to practice is described below: Take 10–15 min a week to think about things you did well. There is nothing too small! Give the event a name or title, and write down exactly what happened [what you said or did; what others around you said or did]. It is particularly important that you note what you did that made it happen. Our successes don’t just happen randomly, we played a role in them. It can also be helpful to “capitalize” on this event, or purposefully “boost” the positive emotions that come from these events. Below are some suggested ways to do this: Sometimes just writing it down can be effective because it can help us to “relive” the positive event and also remember it better. Share what happened (on social media, to a friend on the phone) Celebrate what happened (do something nice for yourself, big or small, to make the event more memorable) |
| M | Learn about asking for help Folks who have recently given birth often face high expectations and a fear of judgment and shame. This can make it very difficult to ask for help. As one mom said “Sometimes I don’t reach out when I should…And then, I start to get frustrated and not being able to take care of myself. And then, the emotions start to come…sometimes I feel like I can do everything on my own and then I can’t.” But, you need to be aware of your limitations. Shouldering too much and putting your mind and body through lots of stress can be unhealthy for you. This “stress overload” looks different for different people. But here are some signs to look out for: Emotional signs: Your mood may change more than normal (becoming frustrated or agitated more easily) You may feel like you are “losing control” Difficulty calming your thoughts Feeling badly about yourself Starting to avoid other people Physical signs: Headaches Upset stomach If you are experiencing these things, you should consider asking for help. Going through stress for a prolonged period of time can lead to a number of negative health issues. It can be helpful to remind yourself that humans are social creatures, and we all need help sometimes. For a full expert-written article on this, see the following: https://www.psychologytoday.com/us/blog/emotional-mastery/201904/what-makes-it-so-hard-ask-help A key part of asking for help is being emotionally vulnerable, and expressing that you need others. This can be scary, but research suggests that this allows for closer relationships and a number of other positive things. See the following video, featuring Dr. Brené Brown speaking at TEDxHouston for more information on the power of vulnerability. This video is owned by TED, has not been modified, and is available at the following link: https://www.ted.com/talks/brene_brown_the_power_of_vulnerability?utm_campaign=tedspread&utm_medium=referral&utm_source=tedcomshare The licensing agreement for TED materials is also available here: https://creativecommons.org/licenses/by-nc-nd/3.0/legalcode EMBEDDED VIDEO Here are some suggestions that can increase comfort with being vulnerable (for more information, see the following article which these suggestions were drawn from this https://www.huffpost.com/entry/how-to-be-more-vulnerable-relationships_l_5daf65b0e4b0f34e3a7e0abd): Find people in your life who display vulnerability. Having an example to follow can help to build comfort with vulnerability Take it slow. Many people struggle to be vulnerable because they have had experiences earlier in life that have taught them it is dangerous to be vulnerable. Practicing opening up in small ways first can pave the way for opening up in larger ways later. Keep in mind that people generally respond well to displays of vulnerability in others. Think back to a time when someone opened up to you, you likely thought they were brave and were honored that they chose to open up to you. One last thing to keep in mind is that it is important to set boundaries with the “helpers” in our lives. Sometimes they may have strong opinions about how you should be parenting, and you may disagree with their opinions. Here is an expert-written article that has some tips about setting boundaries: https://www.psychologytoday.com/us/blog/the-couch/201903/everybody-needs-boundaries-6-ways-make-them-work-you |
| N | Consider joining a support group It may be helpful to spend some time around other people who are going through a similar stage of life. You might consider joining a parent support group (either in person or online). As one mom described her experience in a mom group: “ [My baby] wouldn’t nap, I was losing my mind and I just remember crying and I was so embarrassed and I opened my eyes and half the room was crying with me. They got it. It wasn’t even like they pitied me, it was just like they knew what I was talking about and they couldn’t give me anything to fix it. But just knowing that they felt it and were with me was enough to make me breathe again.” Below are some places to start: Online support groups from Postpartum Support international: https://www.postpartum.net/get-help/psi-online-support-meetings/ Look for parent meet-ups: https://www.meetup.com/ Mocha Moms, specifically for moms of color: https://www.mochamoms.org/i4a/pages/index.cfm?pageid=1 Group Peer Support (search specifically for parenting groups): https://grouppeersupport.org/ Search Facebook for local mom groups For parents who have had a baby in the Neonatal Intensive Care Unit (NICU) check out the organization HandtoHold: https://handtohold.org/ |
| O | Learn about setting a routine for baby It can be helpful to set up routines for your baby, though it is important to also remember to be flexible and pay attention to your instinct for what your baby needs at any given time. As one mom described the helpfulness of a routine: “Knowing that both of my children are content, and we’re prepared for the next day, and knowing that they’re feeling well, and I’m not anticipating disrupted sleep or those sort of things which, I think, I have been able to really establish through a really good routine with them. So I’m able to sort of feel that calm at the end of the day.” Here is some information about getting your baby started on routines: https://www.babycenter.com/0_the-basics-of-baby-schedules-why-when-and-how-to-start-a-rou_3658352.bc The video below, created by Hello Doctor SA, discusses getting baby into a routine and is also available at this link: https://www.youtube.com/watch?v=yau8wEAjZgM EMBEDDED VIDEO Research suggests that sleep routines may be especially important for your baby. Below are some resources that can help with this: The videos below discuss sleeping routines for very young babies. The first was created by Centura Health and is also available at the following link: https://www.youtube.com/watch?v=mOJ4GlVNvRU. The second was created by the Mount Sinai Parenting Center and is available at the following link: https://www.youtube.com/watch?v=oU4OvpqXcJU EMBEDDED VIDEO EMBEDDED VIDEO One helpful step for establishing routines is tracking activity, or writing down your baby’s behaviors so that you can see patterns. This free app allows you to track sleep and also allows you to ask questions of experts (search in the Apple App Store or Google Play): https://www.johnsonsbaby.com/bedtime-baby-sleep-app The app Huckleberry can also help with tracking your baby’s sleep and connecting you with expert advice: https://huckleberrycare.com/ For tracking multiple behaviors try searching for the “Baby Tracker” app in the Apple Store or Google Play |
| P | Get trustworthy information Whether or not this is your first baby, you are likely going to have questions and encounter new situations that you haven’t dealt with before. It is important to have ways to get your questions answered and get the information you need. As one mom said, “Because we as new moms, we just feel like we got it, we can handle it. We’re supposed to be able to know what we’re doing, but it’s not true. Sometimes it’s overwhelming…if you need help with something like you don’t know things, ask other people…. Don’t think because you’re asking questions that doesn’t mean you know what you’re doing.” Below are some informational websites that are organized by topic. Questions about the 4th trimester (first three months after having a baby): Newmomhealth.com, Expert-written resources for folks in the postpartum period: https://newmomhealth.com/#village Breastfeeding La Leche League, resources for breastfeeding support https://www.llli.org/resources/ Kelly Mom, information about breastfeeding and other parenting topics: https://kellymom.com/category/about/ Happy Family, provides forum to chat with an expert for help with breastfeeding and nutrition): https://www.happyfamilyorganics.com/#chat-now Safety: Searchable database of expert-written safety tips: https://www.safekids.org/safetytips Sleep: Expert-written information https://www.babysleep.com/ General Information American Academy of Pediatrics Website, can search for information by age and topic: https://www.healthychildren.org/English/Pages/default.aspx For general information about newborn care, you can also reference Mt. Sinai Parenting Center’s Youtube channel which has videos on a range of topics: https://www.youtube.com/channel/UC7aKhPwmkYwBVz61tsBJ4Aw/videos https://newsmomsneed.marchofdimes.org/ The Motherhood Center has webinars (some available for free others for a small fee) on a number of topics: https://www.themotherhoodcenter.com/webinars See this link for educational articles as well as a directory to locate perinatal health specialists: https://wearerobyn.co/learn Concerns about developmental delays: The Center for Disease Control and Prevention has information about early intervention and how to find services near you: https://www.cdc.gov/ncbddd/actearly/parents/states.html Note: if you are concerned about your baby’s development, a good first step is to visit your pediatrician for a checkup. Make sure to tell the doctor what you are noticing with your baby that makes you worry. For Black birth parents, you can look into in-person perinatal safe spots providing access, connections, knowledge, and empowerment in order to “eliminate racial and class disparities in birth outcomes”: https://perinataltaskforce.com/official-perinatal-safe-spot-profiles/ You may also want to check out this website https://motherfigure.com/ which can help you to find perinatal specialists in your area. |
| Q | Take a break It is very easy to put your needs last when you have a new baby. But, taking breaks from infant care and getting out of the house are important for you and your baby. This allows for rest, which is helpful for interacting with your baby with higher energy and a more upbeat mood. Sometimes when you don’t get a break it can be hard to appreciate time with your baby. Also, especially right after giving birth, when it is a lot of work to care for baby, you can feel isolated and feel like you are losing part of your identity (your sense of who you are; this is especially true for moms who are used to working/doing lots of things outside of the house). As one mom said “Don’t cancel out all the things that you were doing before because I know you’re busy, and you have a newborn, and you’re trying to focus on it, but try to remember some of the things that you used to like doing before you had the baby…my husband, he literally told me, “I wish you would go out with your friends [laughter].” …he was like, “No, it’s not good for you. You need to go out and socialize with people.” So try not to close off because when you close off from people, you don’t notice it, but your moods change when you get around people.” Make a SMART goal for one thing you can do outside of the house each week. These goals should be: Specific: goal should be simple, straightforward and have the details clearly outlined (When, where, what). Clearly defining your goal will help you to focus your efforts. Measurable: pick something with measurable progress so that you can observe the change occurring as you attain your goal. Attainable: Pick something that is within reach. Taking one step at a time is a proven way to make progress towards goals. Relevant: Pick something you care about and are willing to work towards, this is important because the more you care, the more likely you will stick with your goal and see it through. Time-based: It is helpful to set a timeframe for your goal (within the next week I will___, within the next month I will___). |
| R | Take some time to reflect Especially when you are going through a challenging transition time, like after having a baby, it is important to know yourself, so that you know what to do to make the transition less stressful. This knowledge involves the answers to questions like: what helps me feel relaxed? What are the signs that I am getting overwhelmed? Which of my habits are helping me and which are hurting me? As one mom said “We just have your moments when you’re down. I think it’s important to know what to do when you’re not feeling well, like to reach out for help, reach out to a friend, reach out to your mom, say, “Can you come down and take her for a little bit?” You have your moments when you’re not feeling well, but it’s having the tools to know how to get yourself out of it.” One way to begin to build your knowledge about yourself is to “collect data.” One way to do this is to make a thought record in which you write down information about experiences that you’ve had. You can do this on a piece of paper, or even in a notepad app on your phone. To do this, take a pause at least once a day (even for five minutes!) to think back about events during that day and note the following: 1) what happened (what time is it, who is there, what are they doing?) 2) what were you thinking when it happened? 3) what were you feeling? 4) what did you do in response? Once you collect a couple weeks of data, you can start to see patterns in your responses, and gain a better understanding of how your emotions, thoughts, and behaviors relate to the events of your life. This gives you valuable information for planning in the future so that you “set yourself up for success” and not for low mood, anxiety, stress, or negative feelings about others in your life. |
| S | Learn about resources to help you have a safe and healthy home The environment surrounding you and your baby is important, and influences the wellbeing of your baby and yourself. Not living in stable housing or having unhealthy relationships in the household can have a major negative impact on your adjustment to having a young baby and your beliefs about yourself as a parent. If you don’t have stable housing, here is a website that can assist you: https://www.voa.org/find-housing If you don’t feel safe at home because of the individuals you live with, there are domestic violence resources available here: https://www.thehotline.org/ |
| T | Take care of yourself With a new baby to care for, your needs (showering, food, rest, time to yourself) might take a back seat. However, it is important to take your own needs seriously. This is important not only for your wellbeing, but also for your baby’s. Taking care of yourself will help you: be a better parent (you can’t pour from an empty cup) make sure you keep a sense of your self-worth set a good example for your kids of the importance of taking care of yourself improve your physical and mental health (caregiver “burn out” has been shown to lead to mental and physical health issues) As one mom described the importance of taking care of yourself: “Because when [you don’t have time for yourself] you sort of sink into yourself as a mom…And so you don’t parent well. You don’t cope well with things that are happening or having to put dinner on the table. It sucks… It’s like running on empty.” While it can seem impossible to have time to yourself, even doing small things for yourself can make a big difference. Below are some ideas that were drawn from this article: https://www.verywellfamily.com/how-to-practice-self-care-as-a-new-mom-4771779 Get into a hydration routine. Fill a big water bottle up in the morning and bring it with you throughout the day. You could also put lemon, lime, or other flavoring in it. Give yourself permission to rest. For at least one of your baby’s naps, let yourself not do anything. There are a lot of expectations on new moms, but we all need time to just breathe. Put some music on while you clean. Adding some extra motion (dancing, picking up your pace) while you clean can raise your heart rate and work in a little extra exercise into your day. Also, exercising can be an important way of taking care of yourself. It can improve mental and physical health, and can provide you with a recharging break away from taking care of the baby. But it can raise some questions: How do I start exercising after childbirth? It’s important to take it slow and ease back into exercise after having a baby. You should ask your doctor about exercising in the first few months after birth. Read this article for some tips about easing back in: https://www.parents.com/pregnancy/my-body/postpartum/postpartum-exercise/ What kind of exercise should I do? Walking is a great, gentle cardiovascular exercise. Plus the benefit of getting outside is also good for your mental health. There are also free online videos that you can do which incorporate your baby into the exercise, see below for some examples: https://www.thebump.com/a/exercises-to-do-with-baby https://www.parents.com/parenting/moms/healthy-mom/mommy-and-me-workout/ The video below, created by BodyFit by Amy, has an 18 min “mommy and me” workout. It is also available at the following link: https://www.youtube.com/watch?v=Ni9MxZpCHbk EMBEDDED VIDEO Fitness blender has free customizable videos, though they are not postpartum-specific, so listen to your body as you ease back in https://www.fitnessblender.com/videos Try Yoga, it’s good to build your body’s strength and also good for gaining mindfulness skills (learning to focus on the present movement) that can help with the health of the full mind-body system Yoga with Adrienne Youtube Channel https://www.youtube.com/user/yogawithadriene SarahBeth Yoga Youtube Channel, has some videos that are postpartum specific! https://www.youtube.com/user/SarahBethShow |
| U | Make sleep a priority You have probably heard the advice to “sleep when the baby sleeps”. This is likely easier said than done, especially during the day when it may not be easy to fall asleep and you may want to get other things done. However, it is important to try to sleep when the baby sleeps at night. In addition to reducing feelings of exhaustion and fatigue, sleep is important for our health in the following ways (taken from this article https://www.nhs.uk/live-well/sleep-and-tiredness/why-lack-of-sleep-is-bad-for-your-health/): Sleep boosts your immune system which helps fight off infections and sickness Sleep helps to regulate your hunger and keep you from overeating Better sleep reduces the risk of mental health conditions like depression and anxiety Sleep is good for heart health If you can take advantage of pockets of time throughout the day to catch up on some sleep, do it! It is a cornerstone of health. If you find yourself struggling to fall asleep at night when the baby is sleeping (you lay in bed for hours, or have issues staying asleep even when you aren’t awoken by baby), you may be experiencing insomnia. The good news is that there are lots of effective ways to tackle this problem! A good first step is talking to your doctor, but the tips below can be helpful as well: Set yourself up for good sleep: Don’t do anything but sleep and have sex in your bed. The more activities you do in bed (read, work, browse on your laptop, watch TV), the more you will associate your bed with activity. Try to keep your bedroom cool and dark. Consider using white noise to block out sounds around you for example you can download the following app onto your smartphone: https://apps.apple.com/us/app/sleep-aid-fan-white-noise/id1125321779 Turn the alarm clock around to avoid “clock watching” Try listening to a relaxing audio recording when you get into bed. For example, you might try listening to one of “The Honest Guys” free Youtube videos, many of which are made to help people relax before bed. https://www.youtube.com/channel/UC4jWo5kiyOCt4PnvF4jbaLg If baby’s sleep is impacting your ability to get rest, here is a resource of expert-written information on baby sleep to give you a place to start working through questions or concerns you may have about baby’s sleep: https://www.babysleep.com/ Even if you can’t fall completely asleep, just taking a few minutes to rest (perhaps reading a book or just sitting in a comfortable chair) can be helpful. |
| V | Limit social media scrolling New moms have a lot on their plates, and it is especially hard to be a new mom in our culture. Not only does society blame mothers for any struggles or issues experienced by their children, but we are also surrounded by “perfect” images on moms on TV and the Internet. It can be hard to not feel judged, or to not judge yourself, when you are in a culture like that. As one mom said “I think that on Instagram those moms who are like, “I love my baby so much. They’re beautiful.” And I loved her but in the beginning, I personally, didn’t necessarily feel like—I mean, I loved her. I cried when I saw her. She was beautiful, but I was also exhausted and semi miserable about everything. So seeing other people say that they loved their baby and they loved their husband. That’s a huge one. Saying they loved their partner. I’m like, “You can’t, he’s a disaster. He doesn’t do anything right.” I think that made me feel really bad. Like, I’m the only one who hates my husband right now.” But, we can set ourselves up for less comparison, by limiting social media use, especially when you are using it to look at other people’s profiles. Research suggests that this makes us very focused on comparing ourselves to others and has been linked to low mood and other negative mental health impacts. There are also apps for your smartphone that you can download that can help you track time spent on social media and help limit your usage. |
| W | Learn about some tips for effective time management You have a lot on your plate and have to do a lot of thinking and planning in order to make sure everything on your to-do list gets done. While you can’t control everything, below are some articles with tips that might help you to organize your days: https://www.busybudgeter.com/time-management-tips-for-busy-moms/ https://www.psychologytoday.com/us/blog/understand-other-people/201507/developing-time-management-skills https://www.psychologytoday.com/us/blog/between-you-and-me/201912/need-make-plan-try-starting-the-end |
| X | Find someone to talk to Find individuals in your life that you can talk to about your feelings and experiences. This is important as you go through the postpartum transition. Previous research has shown that moms really benefit from having this kind of support. As one mom said “I think someone to talk to is the biggest one. Because I just—I don’t know. I had so many doubts and whether I was doing the right thing or not or trying to figure out the right thing to do for a lot of different scenarios. So yeah, just helped me to be able to talk about that to somebody.” But, it can be hard if you don’t have folks nearby that you feel comfortable opening up to. However, there are some online, free resources that can provide this kind of support. 7cups is a service where you can chat online for free, https://www.7cups.com/ |
| Y | Learn about community support resources It is an incredible amount of work to have a new baby. Society puts a lot of expectations on parents to manage all the responsibilities of their new baby while also continuing along with all of their other responsibilities. Many would argue that this is too much for one person! But, getting help with childcare and managing the home can also be expensive. However, in many places in the US there are organizations called “Mutual Aid” groups, which provide community support to those around them. This can involve help with shopping and food delivery, childcare, or other services. Check out the links below to see what is available in your community! Mutual Aid Hub listing of community self-supported projects https://www.mutualaidhub.org/ Idealist listing of mutual aid/community self-supported projects https://www.idealist.org/en/groups?q=&searchMode=true If you could specifically benefit from help with childcare, search for free or reduced cost care services near you (enter your Zipcode and then select “care” tab at top): https://www.auntbertha.com/ There are also tools that can help you get the most support from your network of family and friends: https://www.mealtrain.com can help you to organize “meal trains” (when folks in your life offer to bring you a meal) https://lotsahelpinghands.com/ can help you to let family and friends know how to best help you |
| Z | Learn the “language” of your baby Babies can’t tell you what they need in words, but they communicate with you in other ways. Being able to understand the “language” of your baby is key to understanding what they need. It can be very upsetting to not understand what your baby is communicating, especially when they are crying. Below are some educational resources to help you to learn the ‘language’ of your infant. Learn about what things affect your baby’s temperament, so you can better understand how your child ‘ticks’: https://www.zerotothree.org/resources/159-temperament-what-makes-your-child-tick Learn about how your response to your infant works to develop their attachment: https://www.zerotothree.org/resources/230-responsive-care-nurturing-a-strong-attachment-through-everyday-moments Here are some resources to help you to better understand your baby’s cues: The video below was created by Bundoo and discusses six different baby cries and what they mean. It is also available at this link: https://www.youtube.com/watch?v=Oyur-q0gGAs EMBEDDED VIDEO Here is a ‘playlist’ of videos about baby behavior by mn health: https://www.youtube.com/watch?v=lLUJV0QLAiY&list=PLnv1INVkmxmtYaMmowS5oBHnbgmps7Ai1 http://csefel.vanderbilt.edu/documents/reading_cues.pdf https://www.childrensmn.org/educationmaterials/childrensmn/article/15276/infant-behavior-cues/ https://www.fhs.gov.hk/english/health_info/child/30119.pdf https://www.fhs.gov.hk/english/health_info/child/13041.html |
| a | Know your rights as an employee If you or your partner is working, the way you/your partner are treated by your employers will have a big effect on your postpartum adjustment. It is important to know your rights when it comes to working during pregnancy and postpartum. Here are is a website that can help you learn those rights: https://www.familyeducation.com/pregnancy/maternity-leave/maternity-leave-laws-what-are-your-rights Here is a government link in case you have questions or want to learn more: https://www.womenshealth.gov/pregnancy/youre-pregnant-now-what/know-your-pregnancy-rights If you require legal help related to your work, here is some information for getting low cost legal help: https://www.americanbar.org/groups/legal_services/flh-home/flh-free-legal-help/ It may also be helpful to check out http://www.thefifthtrimester.com/for-moms-2, which has information about transitioning back to work (scroll down for resources). |
| B | Address your physical pain and discomfort It is common to experience physical pain and discomfort during the postpartum period. Below are some resources to help address this, but it is also important to discuss your concerns with your medical provider. Some of your pain or discomfort may be due to the physical recovery from pregnancy and birth. Here are some websites that provide information about physical recovery from pregnancy and birth: https://newmomhealth.com/ https://www.mayoclinic.org/healthy-lifestyle/labor-and-delivery/basics/postpartum-care/hlv-20049465 (scroll down for articles covering related topics in more detail) Your pain or discomfort may also be due to the repetitive strain/overuse of body during the postpartum period (also called the “ergonomic demands” of baby care). Here are some websites that may be able to help with this kind of discomfort: Baby wearing: https://www.mother.ly/lifestyle/ergonomics-for-moms-babywearing Breast feeding: https://www.mother.ly/lifestyle/ergonomics-for-moms-breastfeeding-positions Daily life: https://www.babyproductsmom.com/2016/03/ergonomic-nursery-tips-tricks-make-parenting-easieron/ If you are experiencing pain or discomfort surrounding urination or sexual intercourse, it may be helpful to look into some specific information about the pelvic floor (the muscles that support your womb, bladder, and bowel). Here are some places to start: http://functionalpelvis.com/ https://healthcare.utah.edu/womenshealth/gynecology/postpartum-pelvic-floor-disorders.php Specialists, like physical or occupational therapists, may also be helpful in relieving physical pain and discomfort. Here are some directories to help you find specialists near you: https://motherfigure.com/ https://wearerobyn.co/ |
- 1-800-SUICIDE (1-800-784-2433)
- 1-800-273-TALK (1-800-273-8255)
Appendix C. Mapping of Resources to Checklist Items
| Checklist Item | Resource Recommendations |
| 1. When things don’t go well, I don’t blame myself. | A “Question self-blame” B “Increase self-compassion” C “Consider seeking mental health support” |
2. When trying new things, I do all of the following:
| B “Increase self-compassion” C “Consider seeking mental health support” D “Use positive affirmations” E “Get some distance from your thoughts” |
| 3. My baby and I are bonding. | F “Learn about bonding with your baby” |
| 4. Most of the time my baby’s crying doesn’t overwhelm me. | G “Calm your baby and yourself through crying spells” |
| 5. Most of the time I am able to calm myself down when I have strong emotions (such as stress, worries, anger) or distressing thoughts. | C “Consider seeking mental health support” E “Get some distance from your thoughts” H “Gain some tools to help you manage strong emotions” |
| 6. I have people in my life that help to make sure I’m taking care of myself. For example, people in my life check-in with me about taking care of myself, or they help me to take care of myself by doing things like watching the baby. | I “Consider a postpartum doula” |
| 7. I am able to get the materials I need to take care of the baby and myself (such as diapers and food). | J “Learn about the resources around you” |
| 8. I am getting more experienced with taking care of my baby. | K “Learn about baby care” |
| 9. When I do things well, I am able to give myself credit for it. | L “Increase the power of positive emotions” |
10. If you have people in your life who help and support you: when I am talking to people in my life who help or support me, I do all of the following:
| C “Consider seeking mental health support” M “Learn about asking for help” N “Consider joining a support group” |
| 11. I have been able to get my baby into a routine. | O “Learn about setting a routine for baby” |
| 12. When I have a question about parenting or early motherhood, I know how to get an answer that I trust. | I “Consider a postpartum doula” N “Consider joining a support group” P “Get trustworthy information” |
| 13. I am involved in activities outside of the house (such as friendships, hobbies, professional or volunteer work). | Q “Take a break” |
| 14. I know myself (when I need to ask for help, what I need, what makes me feel better when I feel down, worried, or stressed). | C “Consider seeking mental health support” R “Take some time to reflect” |
| 15. My home environment is safe and stable. | S “Learn about resources to help you have a safe and healthy home” |
| 16. I know that taking care of myself is important, and guilt does not get in the way of taking care of my own needs. | E “Get some distance from your thoughts” T “Take care of yourself” |
| 17. I am getting as much sleep as I can. | U “Make sleep a priority” |
18. When thinking about social pressures, I don’t do any of the following:
| E “Get some distance from your thoughts” V “Limit social media scrolling” |
| 19. I plan and manage time well. | W “Learn some tips for effective time management” |
| 20. I have people in my life that I can talk to openly and honestly about my feelings and experiences. | N “Consider joining a support group” X “Find someone to talk to” |
| 21. I have people to help me with childcare and household management (cooking, cleaning, shopping, etc.). | I “Consider a postpartum doula” Y “Learn about community support resources” |
| 22. I understand what my baby is communicating to me (through their cries, body language, etc.). | Z “Learn the ‘language’ of your baby” |
| 23. If you or your co-parent are currently working: my workplace/my partner’s workplace has been understanding and flexible since I have had my baby. | A “Know your rights as an employee” |
| 24. I am not experiencing physical pain or discomfort. | B “Address your physical pain and discomfort” |
Appendix D

{kind=link}
| Total (n = 124) a | |
|---|---|
| Average Percentage of Reported Use Across all Resources | 24.29 |
| Resource 1: Address Physical Pain and Discomfort | n (%) |
| Number of participants to whom the resource was offered | 40 (32.3) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 12 (30) |
| Resource 2: Calm your baby and yourself through crying spells | |
| Number of participants to whom the resource was offered | 72 (58.1) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 25 (34.72) |
| Resource 3: Consider a postpartum doula | |
| Number of participants to whom the resource was offered | 93 (75) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 5 (5.38) |
| Resource 4: Consider joining a support group | |
| Number of participants to whom the resource was offered | 91 (73.4) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 19 (20.9) |
| Resource 5: Consider seeking professional mental health support | |
| Number of participants to whom the resource was offered | 122 (98.4) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 29 (23.77) |
| Resource 6: Find someone to talk to | |
| Number of participants to whom the resource was offered | 39 (31.45) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 6 (15.38) |
| Resource 7: Gain some tools to help you manage strong emotions | |
| Number of participants to whom the resource was offered | 89 (71.8) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 24 (26.3) |
| Resource 8: Get some distance from your thoughts | |
| Number of participants to whom the resource was offered | 122 (98.4) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 25 (20.16) |
| Resource 9: Get trustworthy information | |
| Number of participants to whom the resource was offered | 36 (29) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 5 (13.9) |
| Resource 10: Increase self-compassion | |
| Number of participants to whom the resource was offered | 110 (88.7) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 43 (39.09) |
| Resource 11: Increase the power of positive emotions | |
| Number of participants to whom the resource was offered | 52 (41.9) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 8 (15.38) |
| Resource 12: Know your rights as an employee | |
| Number of participants to whom the resource was offered | 49 (39.5) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 6 (12.24) |
| Resource 13: Learn about asking for help | |
| Number of participants to whom the resource was offered | 72 (58.1) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 20 (27.78) |
| Resource 14: Learn about baby care | |
| Number of participants to whom the resource was offered | 6 (4.8) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 0 (0) |
| Resource 15: Learn about bonding with your baby | |
| Number of participants to whom the resource was offered | 21 (16.94) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 4 (19.05) |
| Resource 16: Learn about community support resources | |
| Number of participants to whom the resource was offered | 67 (54.03) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 12 (17.91) |
| Resource 17: Learn about resources to help you have a safe and healthy home | |
| Number of participants to whom the resource was offered | 8 (6.45) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 1 (0.81) |
| Resource 18: Learn about setting a routine for baby | |
| Number of participants to whom the resource was offered | 62 (50) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 21 (33.87) |
| Resource 19: Learn about some tips for effective time management | |
| Number of participants to whom the resource was offered | 68 (54.84) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 20 (29.41) |
| Resource 20: Learn about the resources around you | |
| Number of participants to whom the resource was offered | 5 (4.01) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 0 (0) |
| Resource 21: Learn the ‘language’ of your baby | |
| Number of participants to whom the resource was offered | 46 (37.1) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 19 (41.3) |
| Resource 22: Limit social media scrolling | |
| Number of participants to whom the resource was offered | 78 (62.9) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 29 (37.18) |
| Resource 23: Make sleep a priority | |
| Number of participants to whom the resource was offered | 58 (46.77) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 22 (37.93) |
| Resource 24: Question self-blame | |
| Number of participants to whom the resource was offered | 87 (70.16) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 22 (25.29) |
| Resource 25: Take a break | |
| Number of participants to whom the resource was offered | 92 (74.19) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 40 (43.48) |
| Resource 26: Take care of yourself | |
| Number of participants to whom the resource was offered | 98 (79.03) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 44 (44.9) |
| Resource 27: Take some time to reflect | |
| Number of participants to whom the resource was offered | 81 (65.32) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 18 (22.22) |
| Resource 28: Use positive affirmation | |
| Number of participants to whom the resource was offered | 98 (79.03) |
| Number of participants offered the resource who reported using the resource or the intention to use the resource | 41 (41.84) |
Appendix E
| Total (n = 125) | |
|---|---|
| 1. When things don’t go well, I don’t blame myself. | n (%) |
| This is not an issue for me. | 38 (30.4) |
| This is going ok for me, but could be better. | 66 (52.8) |
| I’d like help with this. | 21 (16.8) |
| 2. When trying new things, I do all of the following: I am patient with myself and don’t expect myself to get things right away I feel comfortable pushing myself beyond my comfort zone I can be flexible with my plans and expectations. | |
| This is a strength for me. | 27 (21.6) |
| This is going ok for me, but could be better. | 77 (61.6) |
| I’d like help with this. | 21 (16.8) |
| 3. My baby and I are bonding. | |
| This is going well for me. | 104 (83.2) |
| This is going ok for me, but could be better. | 19 (15.2) |
| I’d like help with this. | 2 (1.6) |
| 4. Most of the time my baby’s crying doesn’t overwhelm me. | |
| This is a strength for me. | 53 (42.4) |
| This is going ok for me, but could be better. | 60 (48) |
| I’d like help with this. | 12 (9.6) |
| 5. Most of the time I am able to calm myself down when I have strong emotions (such as stress, worries, anger) or distressing thoughts. | |
| This is a strength for me. | 36 (28.8) |
| This is going ok for me, but could be better. | 67 (53.6) |
| I’d like help with this. | 22 (17.6) |
| 6. I have people in my life that help to make sure I’m taking care of myself. For example, people in my life check-in with me about taking care of myself, or they help me to take care of myself by doing things like watching the baby. | |
| This is going well for me. | 65 (52) |
| This is going ok for me, but could be better. | 46 (36.8) |
| I’d like help with this. | 14 (11.2) |
| 7. I am able to get the materials I need to take care of the baby and myself (such as diapers and food). | |
| This is not an issue for me. | 120 (96) |
| This is going ok for me, but could be better. | 4 (3.2) |
| I’d like help with this. | 1 (.8) |
| 8. I am getting more experienced with taking care of my baby. | |
| This is going well for me. | 119 (95.2) |
| This is going ok for me, but could be better. | 6 (4.8) |
| I’d like help with this. | 0 |
| 9. When I do things well, I am able to give myself credit for it. | |
| This is a strength for me. | 73 (58.4) |
| This is going ok for me, but could be better. | 48 (38.4) |
| I’d like help with this. | 4 (3.2) |
| 10. If you have people in your life who help and support you: when I am talking to people in my life who help or support me, I do all of the following: I can be open and honest I can trust people to help me I can ask for help and take help when it is offered | |
| This is a strength for me. | 53 (42.2) |
| This is going ok for me, but could be better. | 61 (48.8) |
| I’d like help with this. | 11 (8.8) |
| 11. I have been able to get my baby into a routine. | |
| This is going well for me. | 63 (50.4) |
| This is going ok for me, but could be better. | 49 (39.2) |
| I’d like help with this. | 13 (10.4) |
| 12. When I have a question about parenting or early motherhood, I know how to get an answer that I trust. | |
| This is going well for me. | 89 (71.2) |
| This is going ok for me, but could be better. | 32 (25.6) |
| I’d like help with this. | 4 (3.2) |
| 13. I am involved in activities outside of the house (such as friendships, hobbies, professional or volunteer work). | |
| This is going well for me. | 33 (26.4) |
| This is going ok for me, but could be better | 69 (55.2) |
| I’d like help with this. | 23 (18.4) |
| 14. I know myself (when I need to ask for help, what I need, what makes me feel better when I feel down, worried, or stressed). | |
| This is a strength for me. | 44 (35.2) |
| This is going ok for me, but could be better. | 64 (51.2) |
| I’d like help with this. | 17 (13.6) |
| 15. My home environment is safe and stable. This is not an issue for me. | 117 (93.6) |
| This is going ok for me, but could be better. | 7 (5.6) |
| I’d like help with this. | 1 (.8) |
| 16. I know that taking care of myself is important, and guilt does not get in the way of taking care of my own needs. | |
| This is a strength for me. | 27 (21.6) |
| This is going ok for me, but could be better. | 71 (56.8) |
| I’d like help with this. | 27 (21.6) |
| 17. I am able to sleep at night when my baby is sleeping. | |
| This is going well for me. | 67 (53.6) |
| This is going ok for me, but could be better. | 45 (36) |
| I’d like help with this. | 13 (10.4) |
| 18. When thinking about social pressures, I don’t do any of the following: feel like I have to reach the expectations of others worry about other people’s judgments of me compare myself to others. | |
| This is a strength for me. | 47 (37.6) |
| This is going ok for me, but could be better. | 64 (51.2) |
| I’d like help with this. | 14 (11.2) |
| 19. I plan and manage time well. | |
| This is a strength for me. | 57 (45.6) |
| This is going ok for me, but could be better. | 51 (40.8) |
| I’d like help with this. | 17 (13.6) |
| 20. I have people in my life that I can talk to openly and honestly about my feelings and experiences. | |
| This is not an issue for me. | 86 (68.8) |
| This is going ok for me, but could be better. | 33 (26.4) |
| I’d like help with this. | 6 (4.8) |
| 21. I have people to help me with childcare and household management (cooking, cleaning, shopping, etc.). | |
| This is not an issue for me. | 58 (46.4) |
| This is going ok for me, but could be better. | 50 (40) |
| I’d like help with this. | 17 (13.6) |
| 22. I understand what my baby is trying to tell me (through their cries, body language, etc.). | |
| This is a strength for me. | 79 (63.2) |
| This is going ok for me, but could be better. | 43 (34.3) |
| I’d like help with this. | 3 (2.4) |
| 23. If you or your co-parent are currently working: my workplace/my partner’s workplace has been understanding and flexible since I have had my baby. | |
| This is not an issue for me. | 76 (60.8) |
| This is going ok for me, but could be better. | 42 (33.6) |
| I’d like help with this. | 7 (5.6) |
| 24. I am not experiencing physical pain or discomfort. | |
| This is not an issue for me. | 85 (68) |
| This is going ok for me, but could be better. | 29 (23.2) |
| I’d like help with this. | 11 (8.8) |
Appendix F. Item Level Average for the BIMF
| Total (n = 124) | |
| 1. I am a good mother. | M ± SD |
| Baseline | 5.06 ± 0.94 |
| Follow up | 5.15 ± 0.91 |
| 2. I feel rested. | |
| Baseline | 2.53 ± 1.6 |
| Follow up | 2.9 ± 1.66 |
| 3. I am comfortable with the way I’ve chosen to feed my baby (either bottle or breast, or both). | |
| Baseline | 5.21 ± 1.12 |
| Follow up | 5.4 ± 1.1 |
| 4. My baby and I understand each other. | |
| Baseline | 4.92 ± 0.98 |
| Follow up | 5.03 ± 0.93 |
| 5. I am able to relax and enjoy time with my baby. | |
| Baseline | 4.41 ± 1.28 |
| Follow up | 4.73 ± 1.04 |
| 6. There are people in my life that I can trust to care for my baby when I need a break. | |
| Baseline | 4.91 ± 1.36 |
| Follow up | 5.91 ± 1.34 |
| 7. I am comfortable allowing a trusted friend or relative to care for my baby (can include baby’s father or partner). | |
| Baseline | 5.25 ± 1.06 |
| Follow up | 5.31 ± 1.08 |
| 8. I am getting enough adult interaction. | |
| Baseline | 3.1 ± 1.85 |
| Follow up | 3.73 ± 1.62 |
| 9. I am getting enough encouragement from other people. | |
| Baseline | 4.05 ± 1.55 |
| Follow up | 4.35 ± 1.28 |
| 10. I trust my own feelings (instincts) when it comes to taking care of my baby. | |
| Baseline | 4.9 ± 1.08 |
| Follow up | 5.06 ± 0.88 |
| 11. I take a little time each week to do something for myself. | |
| Baseline | 2.96 ± 1.81 |
| Follow up | 3.4 ± 1.68 |
| 12. I am taking good care of my baby’s physical needs (feedings, changing diapers, doctor’s appointments). | |
| Baseline | 5.77 ± 0.44 |
| Follow up | 5.76 ± 0.45 |
| 13. I am taking good care of my physical needs (eating, showering, etc.) | |
| Baseline | 3.81 ± 1.56 |
| Follow up | 4.11 ± 1.54 |
| 14. I make good decisions about my baby’s health and well being. | |
| Baseline | 5.5 ± 0.67 |
| Follow up | 5.59 ± 0.59 |
| 15. My baby and I are getting into a routine. | |
| Baseline | 4.91 ± 1.1 |
| Follow up | 5.23 ± 0.89 |
| 16. I worry about how other people judge me (as a mother). | |
| Baseline | 3.21 ± 1.81 |
| Follow up | 3.36 ± 1.84 |
| 17. I am able to take care of my baby and my other responsibilities. | |
| Baseline | 3.81 ± 1.56 |
| Follow up | 4.08 ± 1.31 |
| 18. Anxiety or worry often interferes with my mothering ability. | |
| Baseline | 3.36 ± 1.65 |
| Follow up | 3.69 ± 1.6 |
| 19. As time goes on, I am getting better at taking care of my baby. | |
| Baseline | 5.3 ± 0.8 |
| Follow up | 5.44 ± 0.67 |
| 20. I am satisfied with the job I am doing as a new mother. | |
| Baseline | 4.9 ± 0.93 |
| Follow up | 5.15 ± 0.82 |
References
- The Gender Institute of the Australian National University. Gender Inclusive Handbook Every Voice Project. Available online: https://genderinstitute.anu.edu.au/sites/default/files/docs/2021_docs/Gender_inclusive_handbook.pdf (accessed on 1 November 2021).
- Dinour, L.M. Speaking out on “breastfeeding” terminology: Recommendations for gender-inclusive language in research and reporting. Breastfeed. Med. 2019, 14, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Hoffkling, A.; Obedin-Maliver, J.; Sevelius, J. From erasure to opportunity: A qualitative study of the experiences of transgender men around pregnancy and recommendations for providers. BMC Pregnancy Childbirth 2017, 17, 332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logsdon, M.C.; Wisner, K.L.; Pinto-Foltz, M.D. The impact of postpartum depression on mothering. J. Obstet. Gynecol. Neonatal Nurs. 2006, 35, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Handler, A.; Zimmermann, K.; Dominik, B.; Garland, C.E. Universal Early Home Visiting: A Strategy for Reaching All Postpartum Women. Matern. Child Health J. 2019, 23, 1414–1423. [Google Scholar] [CrossRef]
- Fowles, E.R.; Horowitz, J.A. Clinical assessment of mothering during infancy. J. Obstet. Gynecol. Neonatal Nurs. 2006, 35, 662–670. [Google Scholar] [CrossRef]
- Warren, J.B.; Phillipi, C.A. Care of the well newborn. Pediatr. Rev. 2012, 33, 4–18. [Google Scholar] [CrossRef]
- Albers, L.L. Health problems after childbirth. J. Midwifery Women’s Health 2000, 45, 55–57. [Google Scholar] [CrossRef]
- Newport, D.J.; Hostetter, A.; Arnold, A.; Stowe, Z.N. The treatment of postpartum depression: Minimizing infant exposures. J. Clin. Psychiatry 2002, 63, 31–44. [Google Scholar]
- WHO. Postnatal Care for Mothers and Newborns: Highlights from the World Health Organization 2013 Guidelines. Available online: http://www.who.int/maternal_child_adolescent/publications/WHO-MCA-PNC-2014-Briefer_A4.pdf (accessed on 1 October 2020).
- Barkin, J.L.; Wisner, K.L.; Bromberger, J.T.; Beach, S.R.; Terry, M.A.; Wisniewski, S.R. Development of the Barkin index of maternal functioning. J. Women’s Health 2010, 19, 2239–2246. [Google Scholar] [CrossRef] [Green Version]
- Barkin, J.L.; Wisner, K.L.; Bromberger, J.T.; Beach, S.R.; Wisniewski, S.R. Assessment of functioning in new mothers. J. Women’s Health 2010, 19, 1493–1499. [Google Scholar] [CrossRef]
- Barkin, J.L.; Wisner, K.L.; Wisniewski, S.R. The psychometric properties of the Barkin index of maternal functioning. J. Obstet. Gynecol. Neonatal Nurs. 2014, 43, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Albanese, A.M.; Geller, P.A.; Steinkamp, J.M.; Barkin, J.L. In Their Own Words: A Qualitative Investigation of the Factors Influencing Maternal Postpartum Functioning in the United States. Int. J. Environ. Res. Public Health 2020, 17, 6021. [Google Scholar] [CrossRef] [PubMed]
- Declercq, E.; Sakala, C.; Corry, M.P.; Applebaum, S. New mothers speak out. In National Survey Results Highlight Women’s Postpartum Experiences; Childbirth Connection: New York, NY, USA, 2008. [Google Scholar]
- Cohen, J.L.; Daw, J.R. Postpartum Cliffs—Missed Opportunities to Promote Maternal Health in the United States. JAMA Health Forum 2021, 2, e214164. [Google Scholar] [CrossRef]
- Hassan, J. Prenatal education and postpartum well-being. J. Pregnancy Child Health 2016, 3, 2–6. [Google Scholar] [CrossRef]
- Serçekuş, P.; Mete, S. Effects of antenatal education on maternal prenatal and postpartum adaptation. J. Adv. Nurs. 2010, 66, 999–1010. [Google Scholar] [CrossRef]
- Guerra-Reyes, L.; Christie, V.M.; Prabhakar, A.; Siek, K.A. Mind the gap: Assessing the disconnect between postpartum health information desired and health information received. Women’s Health Issues 2017, 27, 167–173. [Google Scholar] [CrossRef]
- King, T.L. The Mismatch Between Postpartum Services and Women’s Needs: Supermom Versus Lying-In. J. Midwifery Women’s Health 2013, 58, 607–608. [Google Scholar] [CrossRef] [Green Version]
- Rouhi, M.; Stirling, C.M.; Crisp, E.P. Mothers’ views of health problems in the 12 months after childbirth: A concept mapping study. J. Adv. Nurs. 2019, 75, 3702–3714. [Google Scholar] [CrossRef] [Green Version]
- McCarter, D.; MacLeod, C.E. What do women want? Looking beyond patient satisfaction. Nurs. Women’s Health 2019, 23, 478–484. [Google Scholar] [CrossRef] [Green Version]
- Albanese, A.M.; Geller, P.A.; Sikes, C.A.; Barkin, J.L. The Importance of Patient-Centered Research in the Promotion of Postpartum Mental Health. Front. Psychiatry 2021, 12, 720106. [Google Scholar] [CrossRef]
- Suplee, P.D.; Bloch, J.R.; McKeever, A.; Borucki, L.C.; Dawley, K.; Kaufman, M. Focusing on maternal health beyond breastfeeding and depression during the first year postpartum. J. Obstet. Gynecol. Neonatal Nurs. 2014, 43, 782–791. [Google Scholar] [CrossRef] [PubMed]
- DiBari, J.N.; Yu, S.M.; Chao, S.M.; Lu, M.C. Use of postpartum care: Predictors and barriers. J. Pregnancy 2014, 2014, 530769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fahey, J.O.; Shenassa, E. Understanding and meeting the needs of women in the postpartum period: The perinatal maternal health promotion model. J. Midwifery Women’s Health 2013, 58, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L.E. Identifying predictors of breastfeeding self-efficacy in the immediate postpartum period. Res. Nurs. Health 2006, 29, 256–268. [Google Scholar] [CrossRef]
- Barkin, J.L.; Bloch, J.R.; Hawkins, K.C.; Thomas, T.S. Barriers to optimal social support in the postpartum period. J. Obstet. Gynecol. Neonatal Nurs. 2014, 43, 445–454. [Google Scholar] [CrossRef]
- Evans, M.G.; Phillippi, S.; Gee, R.E. Examining the screening practices of physicians for postpartum depression: Implications for improving health outcomes. Women’s Health Issues 2015, 25, 703–710. [Google Scholar] [CrossRef]
- Accortt, E.E.; Wong, M.S. It is time for routine screening for perinatal mood and anxiety disorders in obstetrics and gynecology settings. Obstet. Gynecol. Surv. 2017, 72, 553–568. [Google Scholar] [CrossRef]
- Barkin, J.L.; Osborne, L.M.; Buoli, M.; Bridges, C.C.; Callands, T.A.; Ezeamama, A.E. Training frontline providers in the detection and management of perinatal mood and anxiety disorders. J. Women’s Health 2020, 29, 889–890. [Google Scholar] [CrossRef]
- Abrams, L.S.; Dornig, K.; Curran, L. Barriers to service use for postpartum depression symptoms among low-income ethnic minority mothers in the United States. Qual. Health Res. 2009, 19, 535–551. [Google Scholar] [CrossRef]
- Woods-Giscombe, C.; Robinson, M.N.; Carthon, D.; Devane-Johnson, S.; Corbie-Smith, G. Superwoman schema, stigma, spirituality, and culturally sensitive providers: Factors influencing African American women’s use of mental health services. J. Best Pract. Health Prof. Divers. 2016, 9, 1124. [Google Scholar]
- Lara-Cinisomo, S.; Clark, C.T.; Wood, J. Increasing diagnosis and treatment of perinatal depression in Latinas and African American women: Addressing stigma is not enough. Women’s Health Issues 2018, 28, 201–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, C.; Fowles, E.; Walker, L. Postpartum maternal health care in the United States: A critical review. J. Perinat. Educ. 2006, 15, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tikkanen, R.; Gunja, M.Z.; FitzGerald, M.; Zephyrin, L. Maternal mortality and maternity care in the United States compared to 10 other developed countries. Issue Briefs Commonw. Fund 2020. [Google Scholar] [CrossRef]
- Murray Horwitz, M.E.; Molina, R.L.; Snowden, J.M. Postpartum Care in the United States—New Policies for a New Paradigm. N. Engl. J. Med. 2018, 379, 1691–1693. [Google Scholar] [CrossRef] [PubMed]
- The Pew Research Center. Internet/Broadband Fact Sheet. Available online: https://www.pewresearch.org/internet/fact-sheet/internet-broadband/ (accessed on 11 November 2020).
- Lau, Y.; Htun, T.P.; Wong, S.N.; Tam, W.S.W.; Klainin-Yobas, P. Therapist-supported internet-based cognitive behavior therapy for stress, anxiety, and depressive symptoms among postpartum women: A systematic review and meta-analysis. J. Med. Internet Res. 2017, 19, e138. [Google Scholar] [CrossRef]
- Chan, K.L.; Chen, M. Effects of social media and mobile health apps on pregnancy care: Meta-analysis. JMIR Mhealth Uhealth 2019, 7, e11836. [Google Scholar] [CrossRef]
- Monteiro, F.; Pereira, M.; Canavarro, M.C.; Fonseca, A. Be a Mom’s Efficacy in Enhancing Positive Mental Health among Postpartum Women Presenting Low Risk for Postpartum Depression: Results from a Pilot Randomized Trial. Int. J. Environ. Res. Public Health 2020, 17, 4679. [Google Scholar] [CrossRef]
- Biviji, R.; Vest, J.R.; Dixon, B.E.; Cullen, T.; Harle, C.A. Content analysis of behavior change techniques in maternal and infant health apps. Transl. Behav. Med. 2020, 11, 504–515. [Google Scholar] [CrossRef]
- Bodnar, D.; Ryan, D.; Smith, J. Patient Guide: Self-Care Program for Women with Postpartum Depression and Anxiety. Available online: https://fhop.ucsf.edu/sites/fhop.ucsf.edu/files/wysiwyg/CanadianWomen%27sHealth_Self-care%20Program.Postpartum%20Depression%20and%20Anxiety.pdf (accessed on 2 July 2020).
- Flesch, R. A new readability yardstick. J. Appl. Psychol. 1948, 32, 221. [Google Scholar] [CrossRef]
- Gustavson, K.; von Soest, T.; Karevold, E.; Røysamb, E. Attrition and generalizability in longitudinal studies: Findings from a 15-year population-based study and a Monte Carlo simulation study. BMC Public Health 2012, 12, 918. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 385–396. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horowitz, J.M.; Ruth, I.; Rakesh, K. Most Americans Say There is Too Much Economic Inequality in the US but Fewer Than Half Call It a Priority. Available online: https://www.pewresearch.org/social-trends/2020/01/09/trends-in-income-and-wealth-inequality/-fnref-27661-5 (accessed on 14 April 2022).
- Averett, K.H. Queer parents, gendered embodiment and the de-essentialisation of motherhood. Fem. Theory 2021, 22, 284–304. [Google Scholar] [CrossRef]
- DuBois, C.M.; Millstein, R.A.; Celano, C.M.; Wexler, D.J.; Huffman, J.C. Feasibility and acceptability of a positive psychological intervention for patients with type 2 diabetes. Prim. Care Companion CNS Disord. 2016, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barkin, J.L.; Wisner, K.L. The role of maternal self-care in new motherhood. Midwifery 2013, 29, 1050–1055. [Google Scholar] [CrossRef]
- Barkin, J.L.; Beals, L.; Bridges, C.C.; Ezeamama, A.; Serati, M.; Buoli, M.; Erickson, A.; Chapman, M.; Bloch, J.R. Maternal Functioning and Depression Scores Improve Significantly With Participation in Visiting Moms® Program. J. Am. Psychiatr. Nurses Assoc. 2019, 27, 54–63. [Google Scholar] [CrossRef]
- The Pew Research Center. Social Media Usage: 2005–2015. Available online: https://www.pewresearch.org/internet/2015/10/08/social-networking-usage-2005-2015/ (accessed on 1 November 2020).
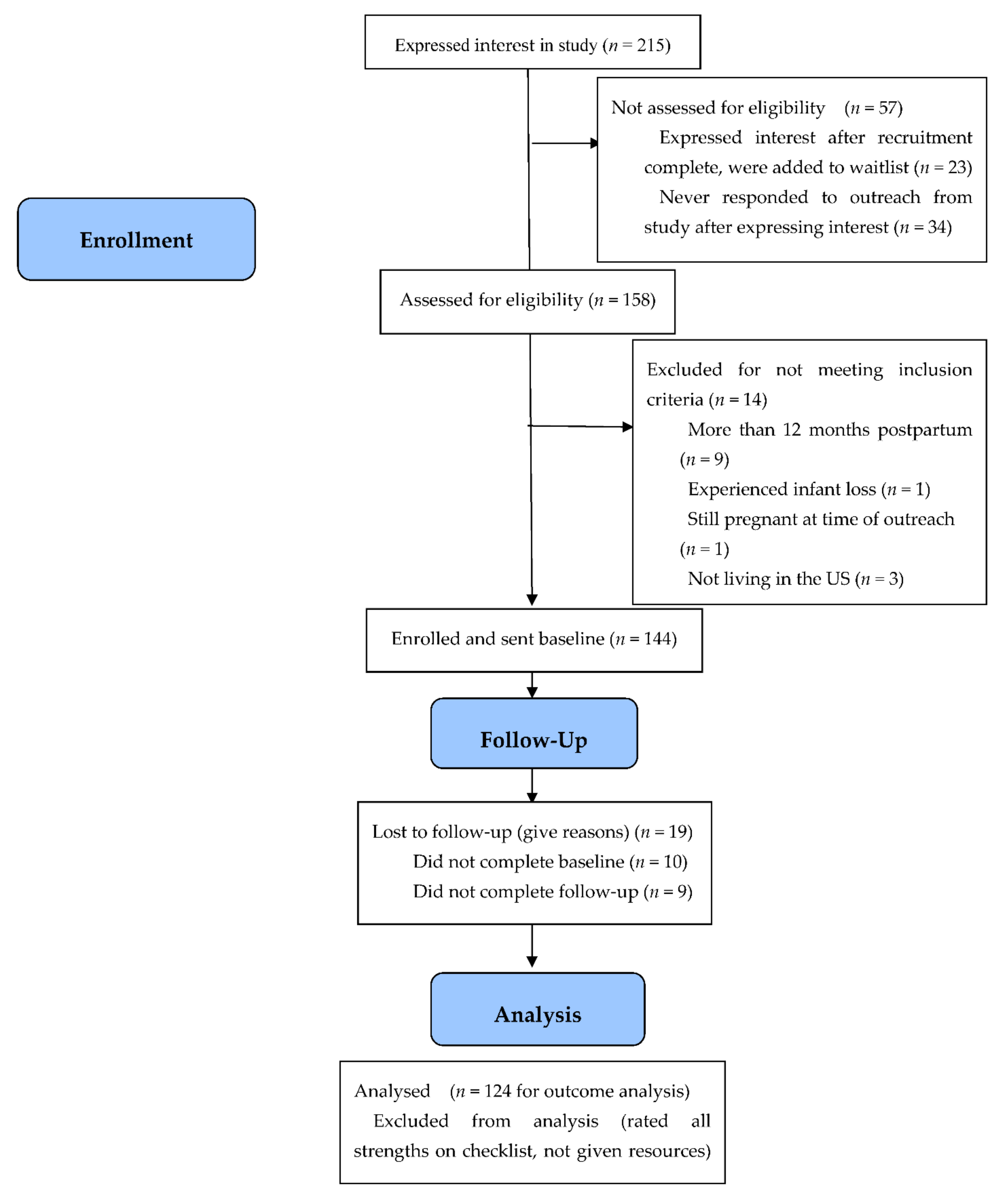
| Total (n = 125) | |
|---|---|
| Race | n (%) |
| Asian | 9 (7.2) |
| Black or African-American | 3 (2.4) |
| Multiracial | 3 (2.4) |
| Other | 3 (2.4) |
| Prefer not to report | 5 (4.0) |
| White | 102 (81.6) |
| Ethnicity | |
| Hispanic or Latinx | 10 (8) |
| Non-Hispanic or Latinx | 115 (92) |
| Gender | |
| Female | 123 (98.4) |
| Male | 2 (1.6) |
| Marital Status | |
| Married | 117 (93.6) |
| Partnered but not married | 7 (5.6) |
| Single | 1 (0.8) |
| Access to support with infant care | |
| No | 10 (8) |
| Yes | 115 (92) |
| Religious Identity | |
| Buddhist | 3 (2.4) |
| Christian | 71 (56.8) |
| Jewish | 10 (8) |
| Not religious | 36 (28.8) |
| Other | 5 (4) |
| Education | |
| College graduate | 47 (37.6) |
| Graduate degree | 70 (56) |
| Did not complete high school | 1 (0.8) |
| High school graduate/GED | 4 (3.2) |
| Other | 3 (2.4) |
| Employment | |
| Employed | 102 (81.6) |
| Homemaker/stay at home | 16 (12.8) |
| Other | 7 (5.6) |
| Income | |
| Less than USD $25,000 | 3 (2.4) |
| USD $25,000–USD $74,999 | 23 (18.4) |
| USD $75,000–USD $124,999 | 37 (29.6) |
| USD $125,000–USD $174,999 | 22 (17.6) |
| More than USD $175,000 | 40 (32) |
| Participant age (years) | |
| 18–25 | 5 (4) |
| 25–35 | 85 (68) |
| 35–45 | 34 (27.2) |
| 46 or older | 1 (0.8) |
| Age of youngest infant at baseline | |
| 0–3 months | 32 (25.6) |
| 3–6 months | 42 (33.6) |
| 6–9 months | 28 (22.4) |
| 9–12 months | 23 (18.4) |
| Mode of delivery | |
| Caesarean section | 36 (28.8) |
| Vaginal | 89 (71.2) |
| Whether mode of delivery proceeded as planned | |
| Yes | 111 (88.8) |
| No | 14 (11.2) |
| Youngest infant singleton or multiple | |
| Singleton | 123 (98.4) |
| Multiple | 2 (1.6) |
| Number of children | |
| 1 | 67 (53.6) |
| 2 | 49 (39.2) |
| 3 | 6 (4.8) |
| 4 | 2 (1.6) |
| More than 4 | 1 (0.8) |
| Whether pregnancy of youngest infant was planned | |
| Yes | 108 (86.4) |
| No | 17 (13.6) |
| Infant born at term | |
| At term | 119 (95.2) |
| Preterm | 6 (4.8) |
| Whether youngest infant was hospitalized in a Neonatal Intensive Care Unit | |
| No | 109 (87.2) |
| Yes | 16 (12.8) |
| Whether participant experienced postpartum re-hospitalization | |
| No | 119 (95.2) |
| Yes | 6 (4.8) |
| Whether participant received treatment for infertility to conceive youngest infant | |
| No | 109 (87.2) |
| Yes | 16 (12.8) |
| Participant history of stillbirth or miscarriage | |
| History of stillbirth or miscarriage | 34 (27.2) |
| No history | 91 (72.8) |
| Participant psychiatric history | |
| Negative history of psychiatric or psychological condition | 87 (69.9) |
| Positive history of psychiatric or psychological condition | 38 (30.4) |
| Experienced a medical condition complicating pregnancy | |
| No | 74 (59.2) |
| Yes | 51 (40.8) |
| Medical conditions experienced during pregnancy | |
| Asthma in pregnancy | 12 (9.6) |
| Diabetes related | 12 (9.6) |
| High blood pressure during pregnancy | 18 (14.4) |
| Obesity in pregnancy | 14 (11.2) |
| Other medical condition a | 12 (9.6) |
| Total (n = 124) a | ||
|---|---|---|
| Did you use any of the resources? | n (%) | |
| Yes | 70 (56.5) | |
| No | 54 (43.5) | |
| How often did you refer to/look at the feedback that was sent to you? | ||
| A few times | 56 (45.2) | |
| I only looked at it once | 54 (43.5) | |
| Often | 2 (1.6) | |
| Several times | 12 (9.7) | |
| If you did not use these resources, what got in the way? b | ||
| Didn’t find the resources appealing | 17 (13.7) | |
| Didn’t have time | 50 (40.32) | |
| Forgot about it | 42 (33.87) | |
| Other | 17 (13.7) | |
| COVID-19 made use difficult | 3 (2.42) | |
| Cost | 4 (3.23) | |
| Resources not useful | 6 (4.8) | |
| Formatting made difficult to access | 6 (4.8) | |
| Would you have been more likely to use these resources if you had a person introducing them to you rather than looking into things yourself? | ||
| Yes | 72 (58.1) | |
| No | 52 (41.9) | |
| M ± SD | Range | |
| On a scale from 1–10 how much did you feel the feedback matched your needs (with 10 being the best match)? | 7.42 ± 2.0 | 1–10 |
| On a scale from 1–10 how helpful did you find your personalized resources (with 10 being the most helpful)?c | 6.96 ± 2.35 | 1–10 |
| Measure | Baseline Score | Follow-Up Score | t (123) | Two-Sided p | Cohen’s d | ||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| Barkin Index of Maternal Functioning (BIMF) a | 87.88 | 12.28 | 92.38 | 12.55 | −5.07 | <0.001 | 0.46 |
| Perceived Stress Scale-10 (PSS-10) c | 18.16 | 6.29 | 16.26 | 5.96 | 4.07 | <0.001 | 0.37 |
| Hospital anxiety and Depression Scale-Anxiety Subscale (HADS-A) b | 7.99 | 4.16 | 7.12 | 3.73 | 3.18 | 0.002 | 0.29 |
| Hospital Anxiety and Depression Scale-Depression Subscale (HADS-D) b | 5.44 | 3.33 | 4.6 | 3.24 | 3.6 | <0.001 | 0.32 |
| Used Resources (n = 70) | Did Not Use Resources (n = 54) | |
|---|---|---|
| BIMF Baseline M ± SD | 86.7 ± 12.61 | 89.41 ± 11.78 |
| BIMF Follow-Up M ± SD | 92.63 ± 12.55 | 92.06 ± 12.66 |
| PSS-10 Baseline M ± SD | 18.46 ± 6.8 | 17.78 ± 5.61 |
| PSS-10 Follow-Up M ± SD | 15.69 ± 5.84 | 17.00 ± 6.09 |
| HADS Anxiety Baseline M ± SD | 8.46 ± 4.59 | 7.39 ± 3.48 |
| HADS Anxiety Follow-Up M ± SD | 7.33 ± 3.85 | 6.85 ± 3.59 |
| HADS Depression Baseline M ± SD | 5.41 ± 3.45 | 5.46 ± 3.20 |
| HADS Depression Follow-Up M ± SD | 4.19 ± 3.01 | 5.15 ± 3.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albanese, A.M.; Geller, P.A.; Steinkamp, J.M.; Bloch, J.R.; Sikes, C.; Barkin, J.L. Introducing the Postpartum Toolkit: An Examination of the Feasibility, Acceptability and Pilot Efficacy of an Online Clinical Tool to Enhance Postpartum Functioning and Emotional Wellbeing. J. Clin. Med. 2022, 11, 2748. https://doi.org/10.3390/jcm11102748
Albanese AM, Geller PA, Steinkamp JM, Bloch JR, Sikes C, Barkin JL. Introducing the Postpartum Toolkit: An Examination of the Feasibility, Acceptability and Pilot Efficacy of an Online Clinical Tool to Enhance Postpartum Functioning and Emotional Wellbeing. Journal of Clinical Medicine. 2022; 11(10):2748. https://doi.org/10.3390/jcm11102748
Chicago/Turabian StyleAlbanese, Ariana M., Pamela A. Geller, Jackson M. Steinkamp, Joan R. Bloch, Chris Sikes, and Jennifer L. Barkin. 2022. "Introducing the Postpartum Toolkit: An Examination of the Feasibility, Acceptability and Pilot Efficacy of an Online Clinical Tool to Enhance Postpartum Functioning and Emotional Wellbeing" Journal of Clinical Medicine 11, no. 10: 2748. https://doi.org/10.3390/jcm11102748
APA StyleAlbanese, A. M., Geller, P. A., Steinkamp, J. M., Bloch, J. R., Sikes, C., & Barkin, J. L. (2022). Introducing the Postpartum Toolkit: An Examination of the Feasibility, Acceptability and Pilot Efficacy of an Online Clinical Tool to Enhance Postpartum Functioning and Emotional Wellbeing. Journal of Clinical Medicine, 11(10), 2748. https://doi.org/10.3390/jcm11102748