
Surgery and Catheter Ablation for Atrial Fibrillation: History, Current Practice, and Future Directions

 , ,
, ,
Abstract
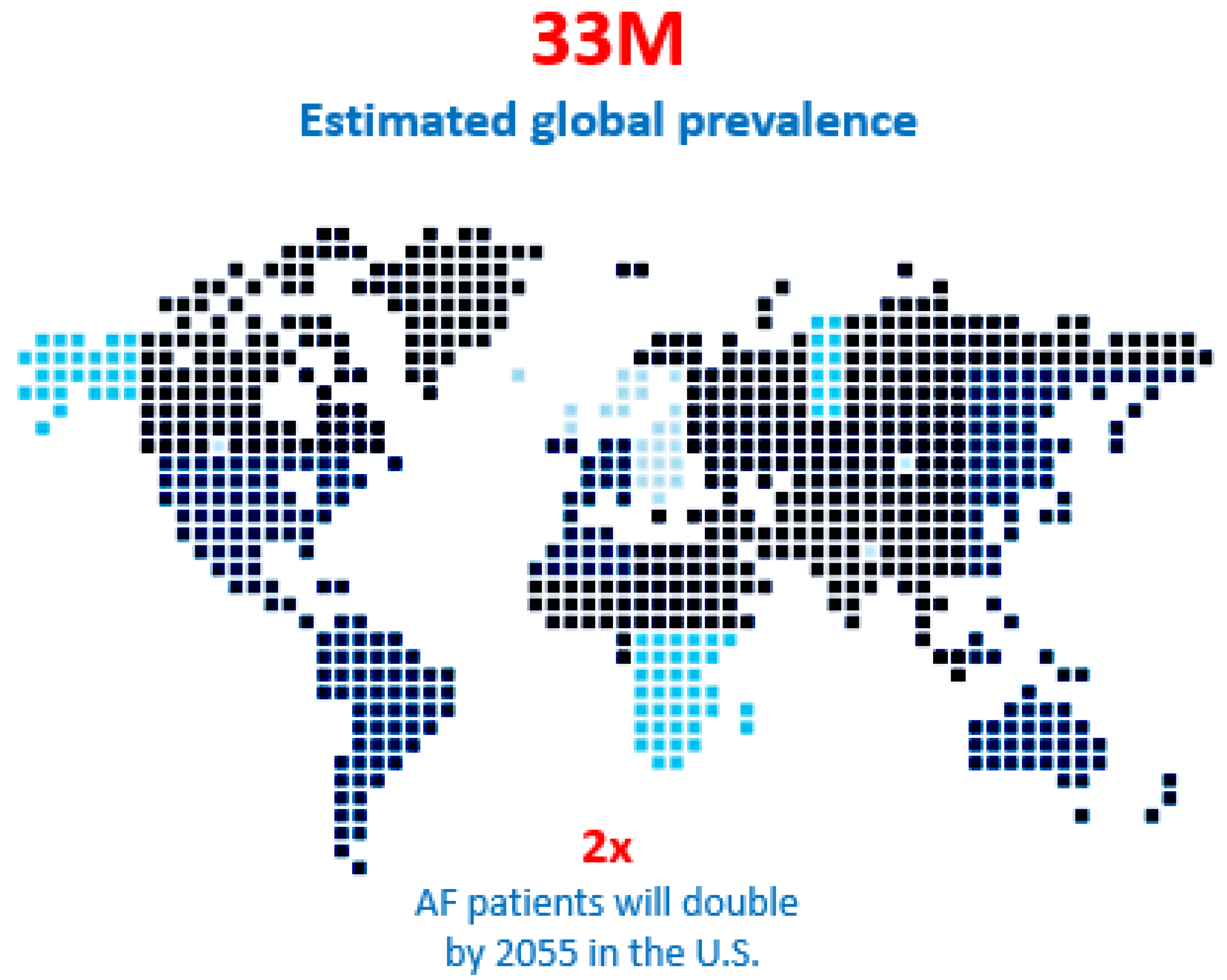
:1. Introduction
2. Surgical Intervention for Atrial Fibrillation
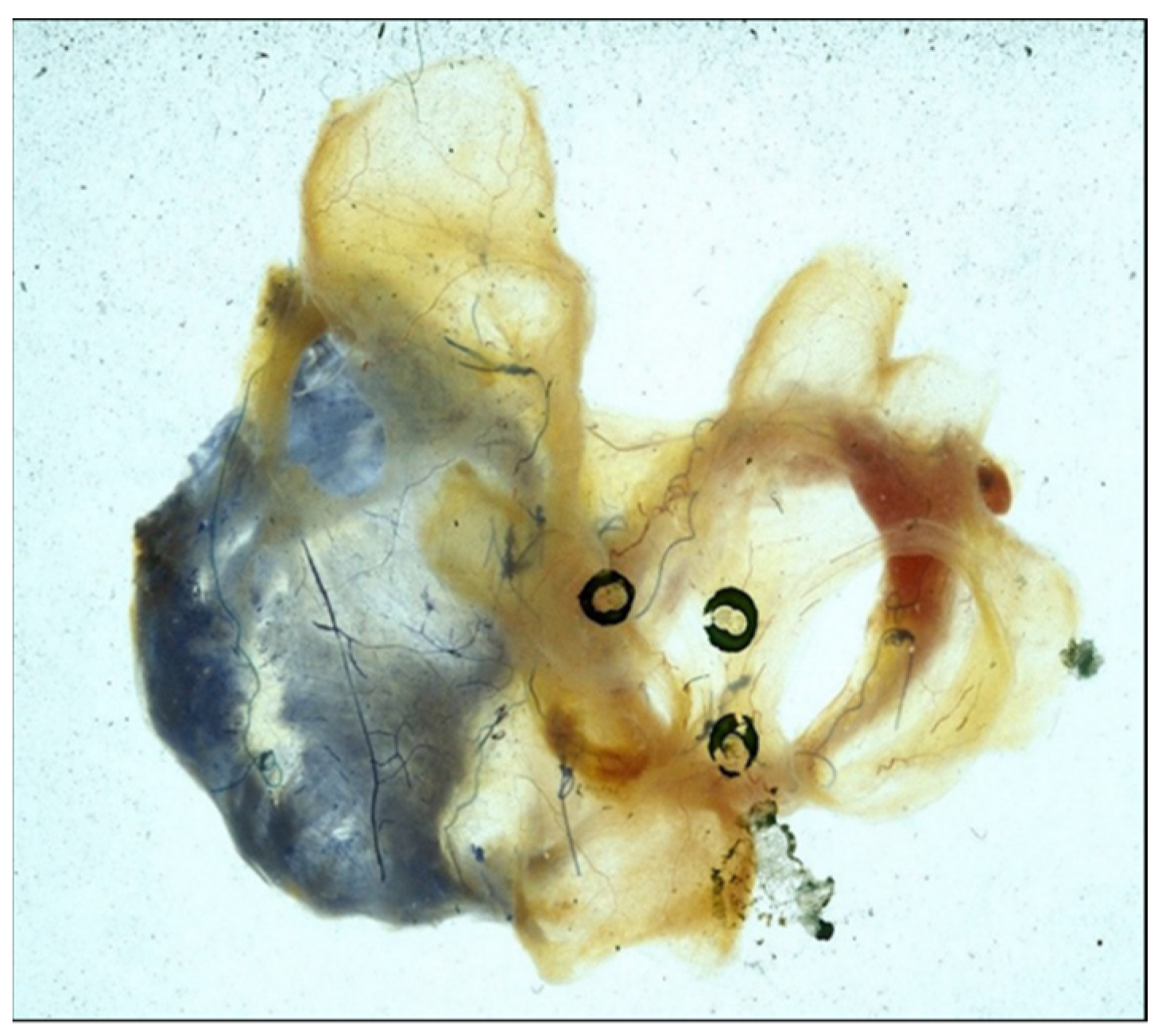
2.1. Electrophysiologic Mapping of Atrial Fibrillation
2.2. Development of the Maze Procedure for Atrial Fibrillation
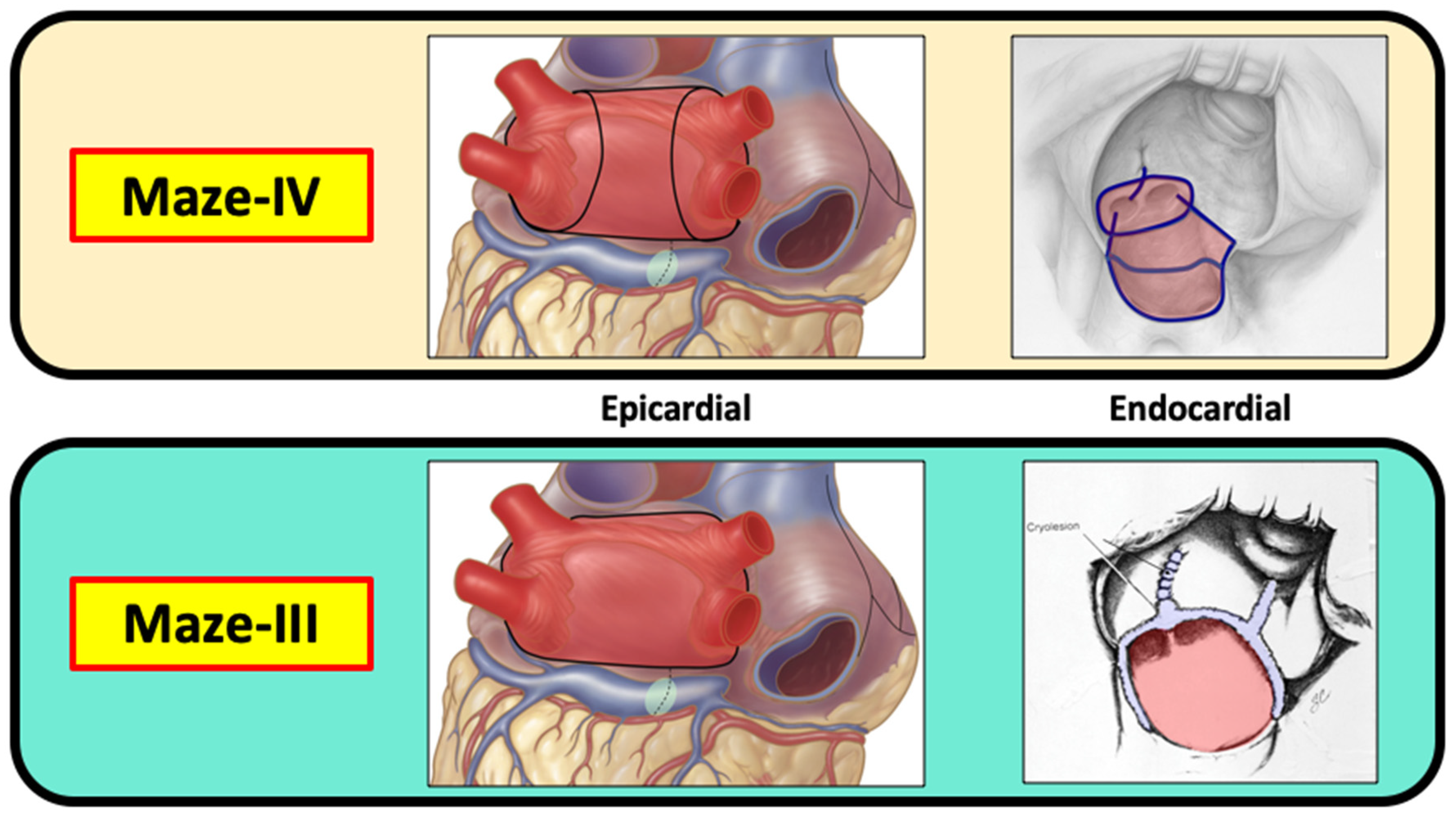
2.3. Chronology from the Maze-I to Maze-IV Procedures for Atrial Fibrillation
3. Catheter Ablation for Atrial Fibrillation
3.1. Evolution of the Therapeutic Goals of Catheter Ablation for AF
3.2. The Importance, or Lack Thereof, of Real-Time AF Mapping
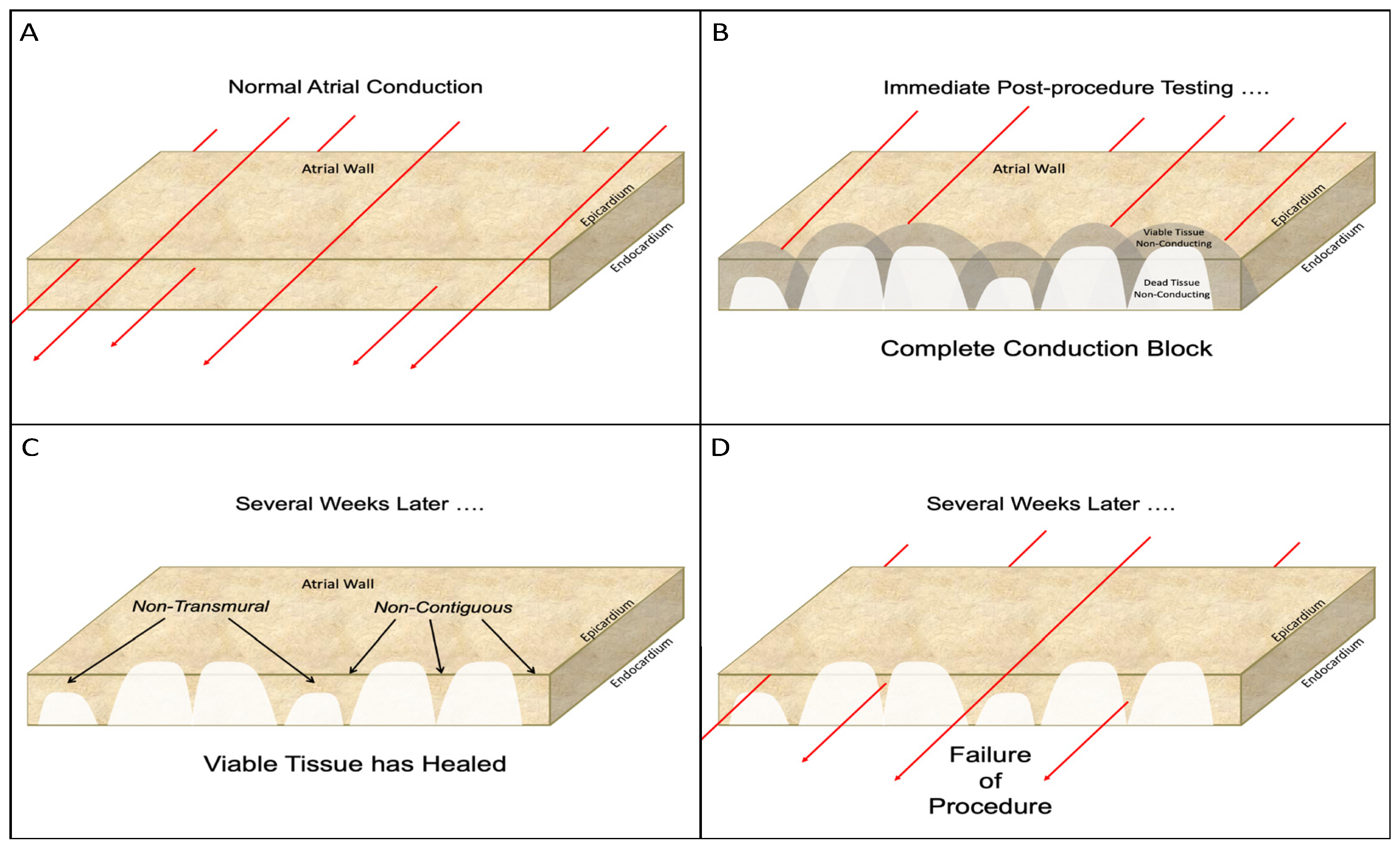
3.3. Fundamental Problems with Catheter Ablation for AF
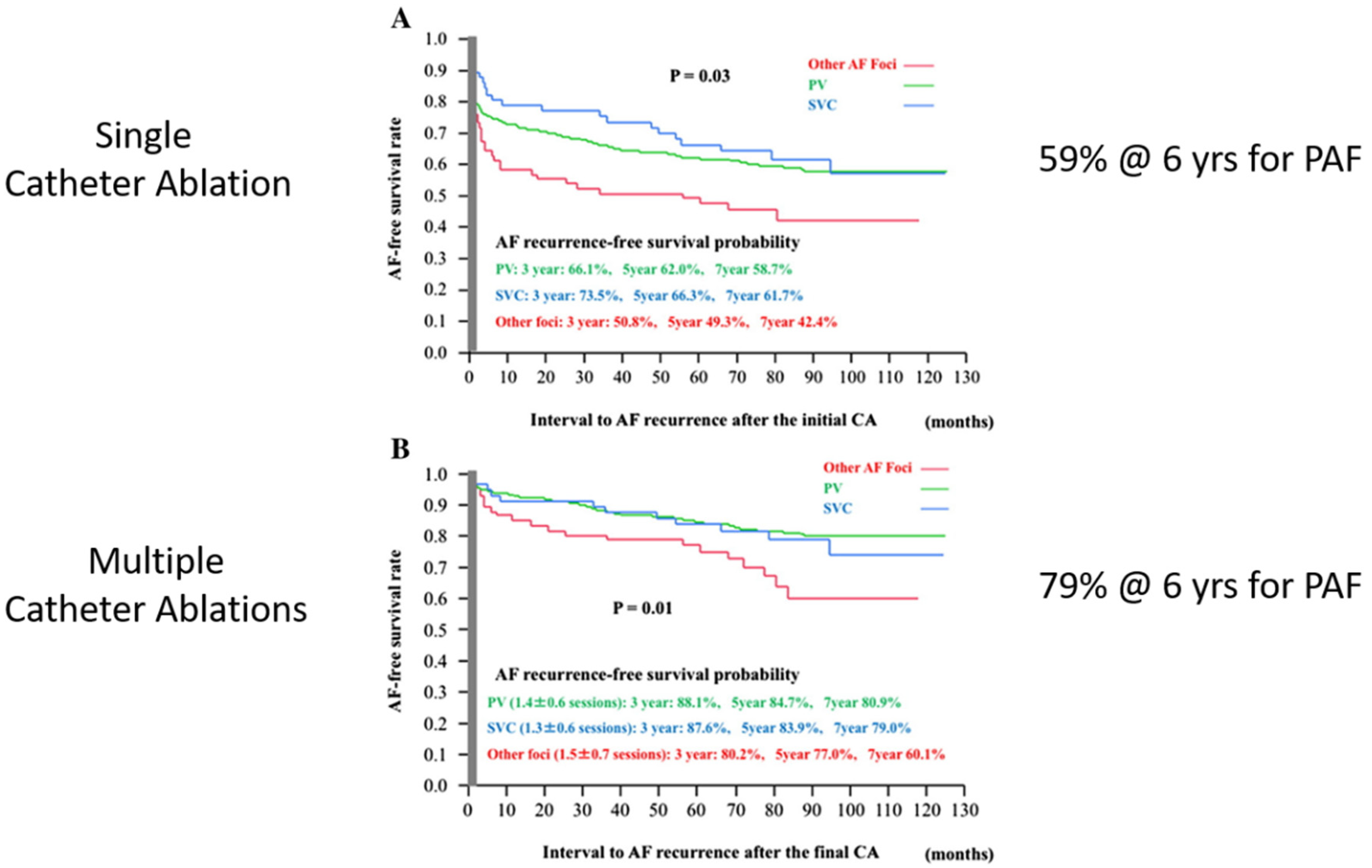
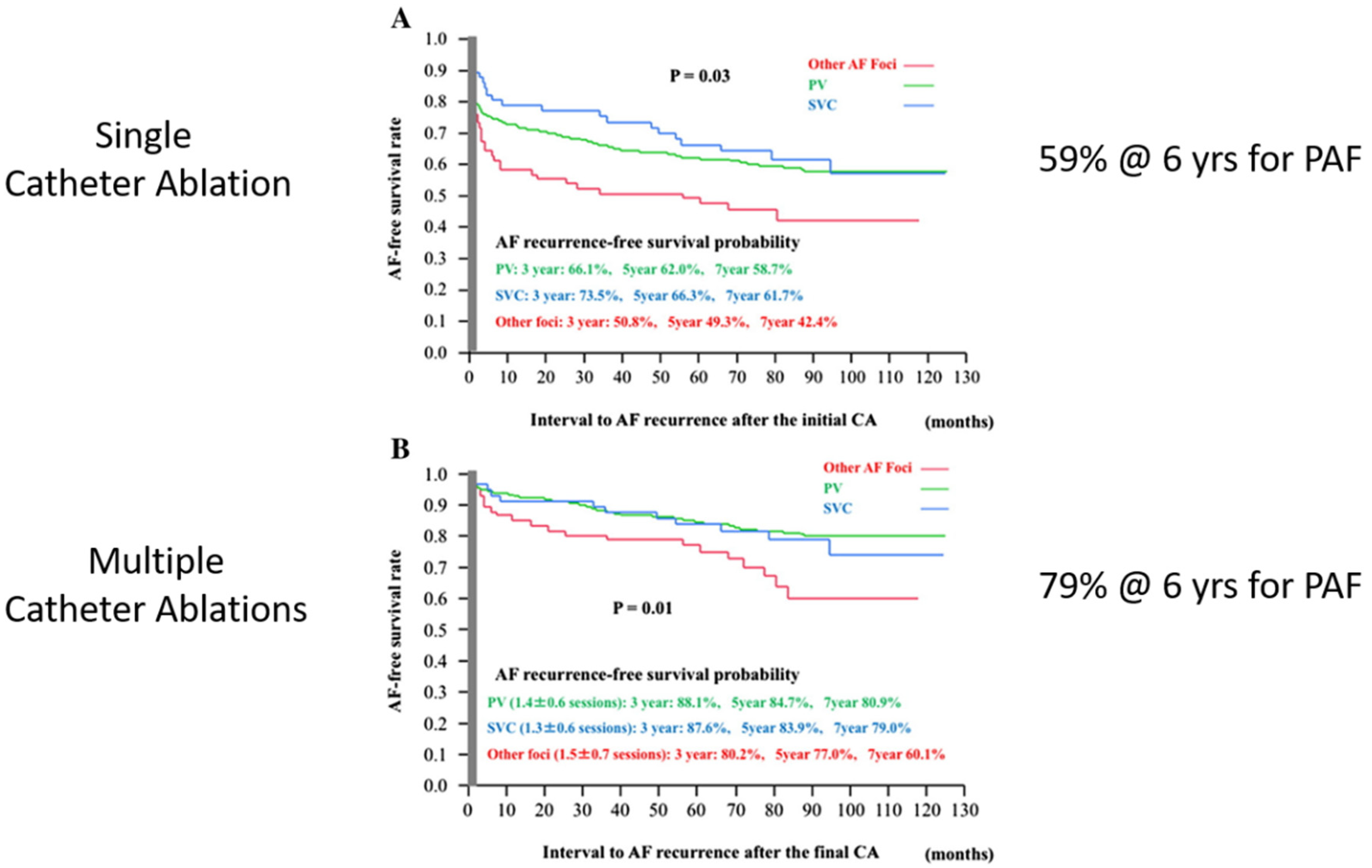
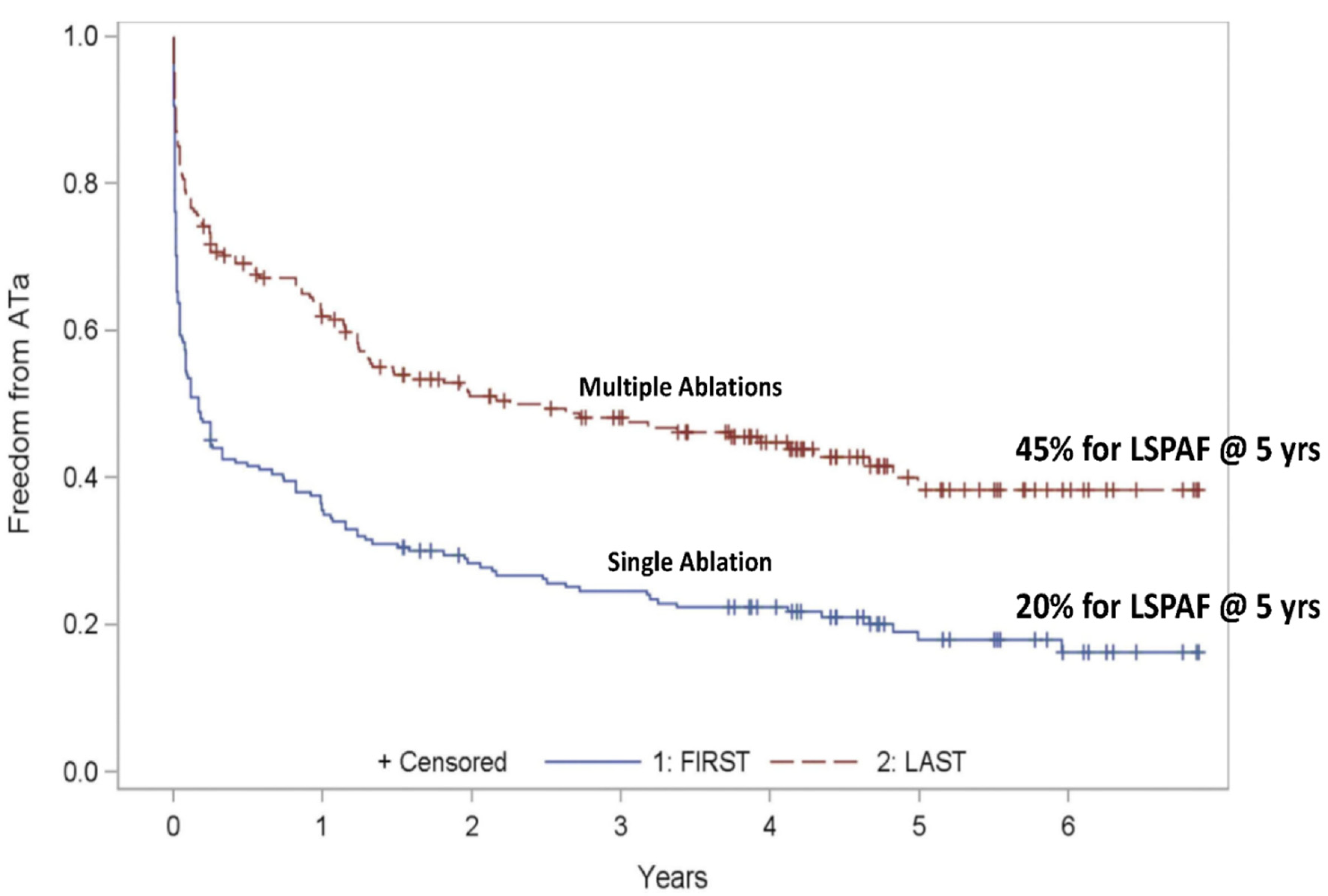
3.4. Results of Catheter Ablation for Atrial Fibrillation
4. Current Status of Surgical Ablation for Concomitant AF
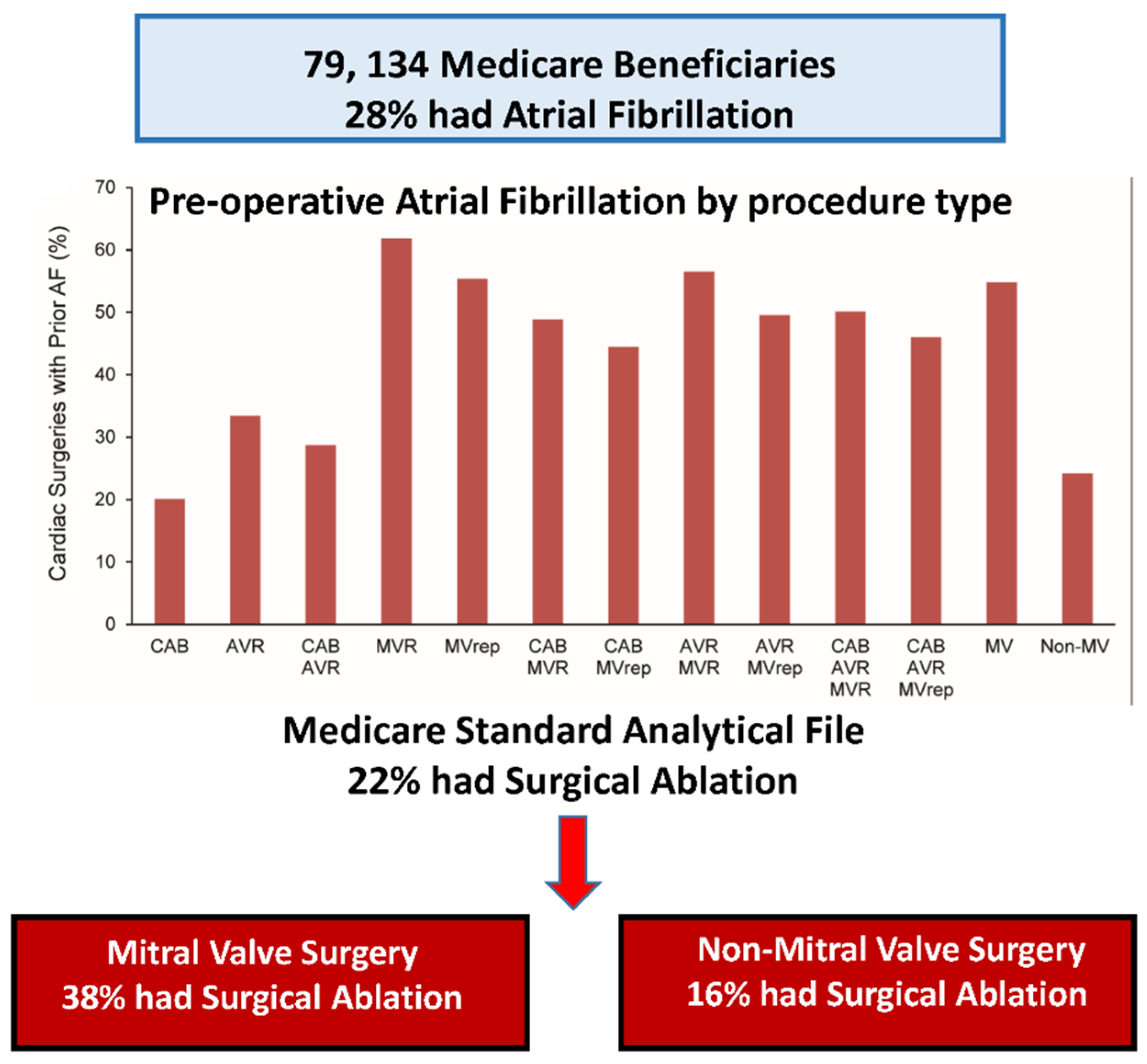
4.1. Prevalence of AF in Cardiac Surgery Patients and Barriers to Its Treatment
- No barriers (40.3%);
- Adds additional aortic cross-clamp time (22.7%);
- “My patients are too high risk” (12.9%);
- No additional payment for AF ablation (4.6%);
- Not comfortable with AF ablation (3.0%);
- Inadequate equipment (3.0%);
- Inadequate staff and support (3.0%);
- Belief that AF ablation worsens AF (3.0%);
- Belief that AF ablation does not work (1.5%).
4.2. Safety of Concomitant AF Ablation in Cardiac Surgery Patients
4.3. Efficacy of Concomitant AF Ablation in Cardiac Surgery Patients
4.4. Beneficial Effects of Concomitant AF Ablation in Cardiac Surgery Patients
4.5. Comfort Level with AF Ablation Surgery
5. Current Status of Surgical Ablation for Stand-Alone AF
5.1. Minimally Invasive CryoMaze-III Procedure
5.2. Off-Pump Minimally Invasive Procedures
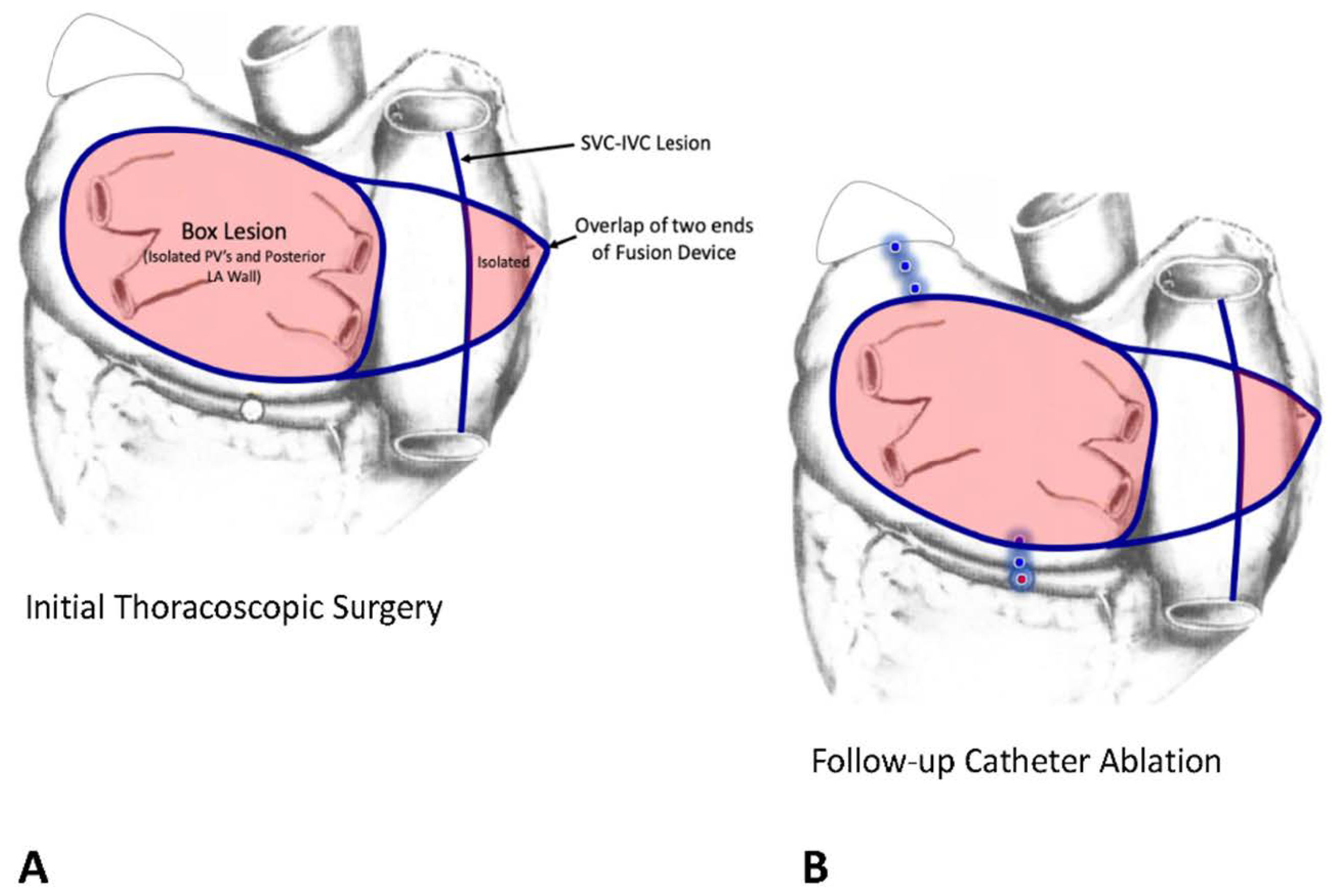
5.3. Off-Pump Hybrid Procedures
- (1)
- Muneretto/Bisleri thoracoscopic (TT) maze procedure;
- (2)
- van Putte TT modified maze procedure;
- (3)
- LaMeir TT maze procedure based on intraoperative mapping;
- (4)
- Convergent procedure.
6. Future of the Interventional Treatment of Atrial Fibrillation
6.1. Future of Catheter Ablation for Atrial Fibrillation
6.2. Future of Surgical Ablation for Atrial Fibrillation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.H.; McAnulty, J.H., Jr.; Zheng, Z.J.; et al. Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naccarelli, G.V.; Varker, H.; Lin, J.; Schulman, K.L. Increasing prevalence of atrial fibrillation and flutter in the United States. Am. J. Cardiol. 2009, 104, 1534–1539. [Google Scholar] [CrossRef]
- Steinberg, B.A.; Holmes, D.N.; Ezekowitz, M.D.; Fonarow, G.C.; Kowey, P.R.; Mahaffey, K.W.; Naccarelli, G.; Reiffel, J.; Chang, P.; Peterson, E.D.; et al. Rate versus rhythm control for management of atrial fibrillation in clinical practice: Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) registry. Am. Heart J. 2013, 165, 622–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calkins, H.; Reynolds, M.R.; Spector, P.; Sondhi, M.; Xu, Y.; Martin, A.; Williams, C.J.; Sledge, I. Treatment of atrial fibrillation with antiarrhythmic drugs or radiofrequency ablation: Two systematic literature reviews and meta-analyses. Circ. Arrhythm. Electrophysiol. 2009, 2, 349–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badhwar, V.; Rankin, J.S.; Ad, N.; Grau-Sepulveda, M.; Damiano, R.J.; Gillinov, A.M.; McCarthy, P.M.; Thourani, V.H.; Suri, R.M.; Jacobs, J.P.; et al. Surgical Ablation of Atrial Fibrillation in the United States: Trends and Propensity Matched Outcomes. Ann. Thorac. Surg. 2017, 104, 493–500. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, S.M.; Rozen, G.; Saleh, A.; Vaid, J.; Biton, Y.; Moazzami, K.; Heist, E.K.; Mansour, M.C.; Kaadan, M.I.; Vangel, M.; et al. Catheter Ablation for Cardiac Arrhythmias: Utilization and In-Hospital Complications, 2000 to 2013. JACC Clin. Electrophysiol. 2017, 3, 1240–1248. [Google Scholar] [CrossRef] [PubMed]
- Piccini, J.P.; Hammill, B.G.; Sinner, M.F.; Hernandez, A.F.; Walkey, A.J.; Benjamin, E.J.; Curtis, L.H.; Heckbert, S.R. Clinical course of atrial fibrillation in older adults: The importance of cardiovascular events beyond stroke. Eur. Heart J. 2014, 35, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Ries, L.A.G.; Harkins, D.; Krapcho, M.; Mariotto, A.; Miller, B.A.; Feuer, E.J.; Clegg, L.; Eisner, M.P.; Horner, M.J.; Howlader, N.; et al. SEER Cancer Statistics Review, 1975–2003. Available online: https://seer.cancer.gov/archive/csr/1975_2003/ (accessed on 28 June 2021).
- National Cancer Institute; Bethesda, M.D. Available online: http://seer.cancer.gov/csr/1975_2010/ (accessed on 28 June 2021).
- Stewart, S.; Hart, C.L.; Hole, D.J.; McMurray, J.J. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am. J. Med. 2002, 113, 359–364. [Google Scholar] [CrossRef]
- Cox, J.L. The first Maze procedure. J. Thorac. Cardiovasc. Surg. 2011, 141, 1093–1097. [Google Scholar] [CrossRef] [Green Version]
- Haissaguerre, M.; Jais, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Metayer, P.; Clementy, J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef] [Green Version]
- D’Agostino, H.J.; Harada, A.; Eisenberg, S.; Schuessler, R.; Boineau, J.; Cox, J. Surgical Ablation of Atrial Fibrillation in a Canine Model of Chronic Mitral Regurgitation. Surgical Forum XXXVII 1986, 339, 302–303. [Google Scholar]
- Laschinger, J.C.; Vannier, M.W.; Gronemeyer, S.; Gutierrez, F.; Rosenbloom, M.; Cox, J.L. Noninvasive three-dimensional reconstruction of the heart and great vessels by ECG-gated magnetic resonance imaging: A new diagnostic modality. Ann. Thorac. Surg. 1988, 45, 505–514. [Google Scholar] [CrossRef]
- Canavan, T.E.; Schuessler, R.B.; Cain, M.E.; Lindsay, B.D.; Boineau, J.P.; Corr, P.B.; Cox, J.L. Computerized global electrophysiological mapping of the atrium in a patient with multiple supraventricular tachyarrhythmias. Ann. Thorac. Surg. 1988, 46, 232–235. [Google Scholar] [CrossRef]
- Cox, J.L.; Canavan, T.E.; Schuessler, R.B.; Cain, M.E.; Lindsay, B.D.; Stone, C.; Smith, P.K.; Corr, P.B.; Boineau, J.P. The surgical treatment of atrial fibrillation. II. Intraoperative electrophysiologic mapping and description of the electrophysiologic basis of atrial flutter and atrial fibrillation. J. Thorac. Cardiovasc. Surg. 1991, 101, 406–426. [Google Scholar] [CrossRef]
- Moe, G.K.; Abildskov, J.A. Atrial fibrillation as a self-sustaining arrhythmia independent of focal discharge. Am. Heart J. 1959, 58, 59–70. [Google Scholar] [CrossRef]
- Cox, J.L. The minimally invasive Maze-III procedure. Oper. Tech. Thorac. Cardiovasc. Surg. 2000, 5, 79–92. [Google Scholar] [CrossRef] [Green Version]
- Damiano, R.J., Jr.; Schwartz, F.H.; Bailey, M.S.; Maniar, H.S.; Munfakh, N.A.; Moon, M.R.; Schuessler, R.B. The Cox maze IV procedure: Predictors of late recurrence. J. Thorac. Cardiovasc. Surg. 2011, 141, 113–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oral, H.; Knight, B.P.; Tada, H.; Ozaydin, M.; Chugh, A.; Hassan, S.; Scharf, C.; Lai, S.W.; Greenstein, R.; Pelosi, F., Jr.; et al. Pulmonary vein isolation for paroxysmal and persistent atrial fibrillation. Circulation 2002, 105, 1077–1081. [Google Scholar] [CrossRef] [Green Version]
- Pappone, C.; Rosanio, S.; Oreto, G.; Tocchi, M.; Gugliotta, F.; Vicedomini, G.; Salvati, A.; Dicandia, C.; Mazzone, P.; Santinelli, V.; et al. Circumferential radiofrequency ablation of pulmonary vein ostia: A new anatomic approach for curing atrial fibrillation. Circulation 2000, 102, 2619–2628. [Google Scholar] [CrossRef]
- Wasserlauf, J.; Verma, N. Atrial-esophageal fistula as a complication of AF ablation: A tough one to swallow. J. Cardiovasc. Electrophysiol. 2020, 31, 1377–1378. [Google Scholar] [CrossRef]
- Koruth, J.S.; Reddy, V.Y.; Miller, M.A.; Patel, K.K.; Coffey, J.O.; Fischer, A.; Gomes, J.A.; Dukkipati, S.; D’Avila, A.; Mittnacht, A. Mechanical esophageal displacement during catheter ablation for atrial fibrillation. J. Cardiovasc. Electrophysiol. 2012, 23, 147–154. [Google Scholar] [CrossRef]
- Leung, L.W.; Gallagher, M.M.; Santangeli, P.; Tschabrunn, C.; Guerra, J.M.; Campos, B.; Hayat, J.; Atem, F.; Mickelsen, S.; Kulstad, E. Esophageal cooling for protection during left atrial ablation: A systematic review and meta-analysis. J. Interv. Card. Electrophysiol. 2020, 59, 347–355. [Google Scholar] [CrossRef] [Green Version]
- Lau, D.H.; Zeemering, S.; Maesen, B.; Kuklik, P.; Verheule, S.; Schotten, U. Catheter Ablation Targeting Complex Fractionated Atrial Electrogram in Atrial Fibrillation. J. Atr. Fibrillation 2013, 6, 907. [Google Scholar] [CrossRef]
- Baykaner, T.; Lalani, G.G.; Schricker, A.; Krummen, D.E.; Narayan, S.M. Mapping and ablating stable sources for atrial fibrillation: Summary of the literature on Focal Impulse and Rotor Modulation (FIRM). J. Interv. Card. Electrophysiol. 2014, 40, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Gillinov, A.M.; Gelijns, A.C.; Parides, M.K.; DeRose, J.J., Jr.; Moskowitz, A.J.; Voisine, P.; Ailawadi, G.; Bouchard, D.; Smith, P.K.; Mack, M.J.; et al. Surgical ablation of atrial fibrillation during mitral-valve surgery. N. Engl. J. Med. 2015, 372, 1399–1409. [Google Scholar] [CrossRef] [Green Version]
- Osorio-Jaramillo, E.; Klenk, S.; Laufer, G.; Ehrlich, M.P. Noninvasive Electrocardiographic Imaging: A Novel Tool for Understanding Atrial Fibrillation in Candidates for Cardiac Surgery? Innovations 2020, 15, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Siontis, K.C.; Noseworthy, P.A. Down but not out-addressing the scourge of late pulmonary vein reconnection. J. Cardiovasc. Electrophysiol. 2019, 30, 824–826. [Google Scholar] [CrossRef]
- Pappone, C.; Vicedomini, G.; Manguso, F.; Gugliotta, F.; Mazzone, P.; Gulletta, S.; Sora, N.; Sala, S.; Marzi, A.; Augello, G.; et al. Robotic magnetic navigation for atrial fibrillation ablation. J. Am. Coll. Cardiol. 2006, 47, 1390–1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saliba, W.; Reddy, V.Y.; Wazni, O.; Cummings, J.E.; Burkhardt, J.D.; Haissaguerre, M.; Kautzner, J.; Peichl, P.; Neuzil, P.; Schibgilla, V.; et al. Atrial fibrillation ablation using a robotic catheter remote control system: Initial human experience and long-term follow-up results. J. Am. Coll Cardiol. 2008, 51, 2407–2411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmayer, K.S.; Gerstenfeld, E.P. Contact force-sensing catheters. Curr. Opin. Cardiol. 2015, 30, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Black-Maier, E.; Pokorney, S.D.; Barnett, A.S.; Zeitler, E.P.; Sun, A.Y.; Jackson, K.P.; Bahnson, T.D.; Daubert, J.P.; Piccini, J.P. Risk of atrioesophageal fistula formation with contact force-sensing catheters. Heart Rhythm. 2017, 14, 1328–1333. [Google Scholar] [CrossRef]
- Verma, A.; Sanders, P.; Macle, L.; Deisenhofer, I.; Morillo, C.A.; Chen, J.; Jiang, C.Y.; Ernst, S.; Mantovan, R. Substrate and Trigger Ablation for Reduction of Atrial Fibrillation Trial-Part II (STAR AF II): Design and rationale. Am. Heart J. 2012, 164, 1–6.e6. [Google Scholar] [CrossRef]
- Tilz, R.R.; Rillig, A.; Thum, A.M.; Arya, A.; Wohlmuth, P.; Metzner, A.; Mathew, S.; Yoshiga, Y.; Wissner, E.; Kuck, K.H.; et al. Catheter ablation of long-standing persistent atrial fibrillation: 5-year outcomes of the Hamburg Sequential Ablation Strategy. J. Am. Coll. Cardiol. 2012, 60, 1921–1929. [Google Scholar] [CrossRef] [Green Version]
- Yang, B.; Jiang, C.; Lin, Y.; Yang, G.; Chu, H.; Cai, H.; Lu, F.; Zhan, X.; Xu, J.; Wang, X.; et al. STABLE-SR (Electrophysiological Substrate Ablation in the Left Atrium During Sinus Rhythm) for the Treatment of Nonparoxysmal Atrial Fibrillation: A Prospective, Multicenter Randomized Clinical Trial. Circ. Arrhythm. Electrophysiol. 2017, 10, e005405. [Google Scholar] [CrossRef]
- Packer, D.L.; Mark, D.B.; Robb, R.A.; Monahan, K.H.; Bahnson, T.D.; Poole, J.E.; Noseworthy, P.A.; Rosenberg, Y.D.; Jeffries, N.; Mitchell, L.B.; et al. Effect of Catheter Ablation vs Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among Patients with Atrial Fibrillation: The CABANA Randomized Clinical Trial. JAMA 2019, 321, 1261–1274. [Google Scholar] [CrossRef]
- Kuck, K.H.; Brugada, J.; Furnkranz, A.; Metzner, A.; Ouyang, F.; Chun, K.R.; Elvan, A.; Arentz, T.; Bestehorn, K.; Pocock, S.J.; et al. Cryoballoon or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2016, 374, 2235–2245. [Google Scholar] [CrossRef] [PubMed]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Takigawa, M.; Takahashi, A.; Kuwahara, T.; Okubo, K.; Takahashi, Y.; Watari, Y.; Nakashima, E.; Nakajima, J.; Yamao, K.; Takagi, K.; et al. Long-term outcome after catheter ablation of paroxysmal atrial fibrillation: Impact of different atrial fibrillation foci. Int. J. Cardiol. 2017, 227, 407–412. [Google Scholar] [CrossRef]
- Voskoboinik, A.; Moskovitch, J.T.; Harel, N.; Sanders, P.; Kistler, P.M.; Kalman, J.M. Revisiting pulmonary vein isolation alone for persistent atrial fibrillation: A systematic review and meta-analysis. Heart Rhythm. 2017, 14, 661–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akkaya, E.; Berkowitsch, A.; Zaltsberg, S.; Greiss, H.; Hamm, C.W.; Sperzel, J.; Neumann, T.; Kuniss, M. Five-year experience with pulmonary vein isolation using the second-generation cryoballoon for treatment of persistent atrial fibrillation. J. Cardiovasc. Electrophysiol. 2018, 29, 1500–1507. [Google Scholar] [CrossRef] [PubMed]
- Cheema, A.; Vasamreddy, C.R.; Dalal, D.; Marine, J.E.; Dong, J.; Henrikson, C.A.; Spragg, D.; Cheng, A.; Nazarian, S.; Sinha, S.; et al. Long-term single procedure efficacy of catheter ablation of atrial fibrillation. J. Interv. Card. Electrophysiol. 2006, 15, 145–155. [Google Scholar] [CrossRef]
- Weerasooriya, R.; Khairy, P.; Litalien, J.; Macle, L.; Hocini, M.; Sacher, F.; Lellouche, N.; Knecht, S.; Wright, M.; Nault, I.; et al. Catheter ablation for atrial fibrillation: Are results maintained at 5 years of follow-up? J. Am. Coll. Cardiol. 2011, 57, 160–166. [Google Scholar] [CrossRef]
- Tondo, C.; Iacopino, S.; Pieragnoli, P.; Molon, G.; Verlato, R.; Curnis, A.; Landolina, M.; Allocca, G.; Arena, G.; Fassini, G.; et al. Pulmonary vein isolation cryoablation for patients with persistent and long-standing persistent atrial fibrillation: Clinical outcomes from the real-world multicenter observational project. Heart Rhythm. 2018, 15, 363–368. [Google Scholar] [CrossRef]
- Andrade, J.G.; Champagne, J.; Dubuc, M.; Deyell, M.W.; Verma, A.; Macle, L.; Leong-Sit, P.; Novak, P.; Badra-Verdu, M.; Sapp, J.; et al. Cryoballoon or Radiofrequency Ablation for Atrial Fibrillation Assessed by Continuous Monitoring: A Randomized Clinical Trial. Circulation 2019, 140, 1779–1788. [Google Scholar] [CrossRef]
- Cox, J.L.; Jaquiss, R.D.; Schuessler, R.B.; Boineau, J.P. Modification of the maze procedure for atrial flutter and atrial fibrillation. II. Surgical technique of the maze III procedure. J. Thorac. Cardiovasc. Surg. 1995, 110, 485–495. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, P.M.; Davidson, C.J.; Kruse, J.; Lerner, D.J.; Braid-Forbes, M.J.; McCrea, M.M.; Elmouelhi, A.M.; Ferguson, M.A. Prevalence of atrial fibrillation before cardiac surgery and factors associated with concomitant ablation. J. Thorac. Cardiovasc. Surg. 2020, 159, 2245–2253.e2215. [Google Scholar] [CrossRef] [PubMed]
- Mehaffey, J.H.; Charles, E.J.; Berens, M.; Clark, M.J.; Bond, C.; Fonner, C.E.; Kron, I.; Gelijns, A.C.; Miller, M.A.; Sarin, E.; et al. Barriers to atrial fibrillation ablation during mitral valve surgery. J. Thorac. Cardiovasc. Surg. 2021; in press. [Google Scholar] [CrossRef]
- Badhwar, V.; Rankin, J.S.; Damiano, R.J.J.; Gillinov, A.M.; Bakaeen, F.G.; Edgerton, J.R.; Philpott, J.M.; McCarthy, P.M.; Bolling, S.F.; Roberts, H.G.; et al. The Society of Thoracic Surgeons 2017 Clinical Practice Guidelines for the Surgical Treatment of Atrial Fibrillation. Ann. Thorac. Surg. 2017, 103, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Ad, N.; Damiano, R.J.J.; Badhwar, V.; Calkins, H.; La Meir, M.; Nitta, T.; Doll, N.; Holmes, S.D.; Weinstein, A.A.; Gillinov, M. Expert consensus guidelines: Examining surgical ablation for atrial fibrillation. J. Thorac. Cardiovasc. Surg. 2017, 153, 1330–1354.e1331. [Google Scholar] [CrossRef] [Green Version]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration with the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef] [PubMed]
- Ad, N.; Henry, L.; Hunt, S.; Holmes, S.D. Do we increase the operative risk by adding the Cox Maze III procedure to aortic valve replacement and coronary artery bypass surgery? J. Thorac. Cardiovasc. Surg. 2012, 143, 936–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Atassi, T.; Kimmaliardjuk, D.M.; Dagenais, C.; Bourke, M.; Lam, B.K.; Rubens, F.D. Should We Ablate Atrial Fibrillation During Coronary Artery Bypass Grafting and Aortic Valve Replacement? Ann. Thorac. Surg. 2017, 104, 515–522. [Google Scholar] [CrossRef] [Green Version]
- Saint, L.L.; Damiano, R.J., Jr.; Cuculich, P.S.; Guthrie, T.J.; Moon, M.R.; Munfakh, N.A.; Maniar, H.S. Incremental risk of the Cox-maze IV procedure for patients with atrial fibrillation undergoing mitral valve surgery. J. Thorac. Cardiovasc. Surg. 2013, 146, 1072–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louagie, Y.; Buche, M.; Eucher, P.; Schoevaerdts, J.C.; Gerard, M.; Jamart, J.; Blommaert, D. Improved patient survival with concomitant Cox Maze III procedure compared with heart surgery alone. Ann. Thorac. Surg. 2009, 87, 440–446. [Google Scholar] [CrossRef]
- Deneke, T.; Khargi, K.; Grewe, P.H.; Laczkovics, A.; von Dryander, S.; Lawo, T.; Muller, K.M.; Lemke, B. Efficacy of an additional MAZE procedure using cooled-tip radiofrequency ablation in patients with chronic atrial fibrillation and mitral valve disease. A randomized, prospective trial. Eur. Heart J. 2002, 23, 558–566. [Google Scholar] [CrossRef] [Green Version]
- Schuetz, A.; Schulze, C.J.; Sarvanakis, K.K.; Mair, H.; Plazer, H.; Kilger, E.; Reichart, B.; Wildhirt, S.M. Surgical treatment of permanent atrial fibrillation using microwave energy ablation: A prospective randomized clinical trial. Eur. J. Cardiothorac. Surg. 2003, 24, 475–480; discussion 480. [Google Scholar] [CrossRef]
- Akpinar, B.; Guden, M.; Sagbas, E.; Sanisoglu, I.; Ozbek, U.; Caynak, B.; Bayindir, O. Combined radiofrequency modified maze and mitral valve procedure through a port access approach: Early and mid-term results. Eur. J. Cardiothorac. Surg. 2003, 24, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Abreu Filho, C.A.; Lisboa, L.A.; Dallan, L.A.; Spina, G.S.; Grinberg, M.; Scanavacca, M.; Sosa, E.A.; Ramires, J.A.; Oliveira, S.A. Effectiveness of the maze procedure using cooled-tip radiofrequency ablation in patients with permanent atrial fibrillation and rheumatic mitral valve disease. Circulation 2005, 112, I20–I25. [Google Scholar] [CrossRef] [PubMed]
- Doukas, G.; Samani, N.J.; Alexiou, C.; Oc, M.; Chin, D.T.; Stafford, P.G.; Ng, L.L.; Spyt, T.J. Left atrial radiofrequency ablation during mitral valve surgery for continuous atrial fibrillation: A randomized controlled trial. JAMA 2005, 294, 2323–2329. [Google Scholar] [CrossRef]
- Blomstrom-Lundqvist, C.; Gizurarson, S.; Schwieler, J.; Jensen, S.M.; Bergfeldt, L.; Kenneback, G.; Rubulis, A.; Malmborg, H.; Raatikainen, P.; Lonnerholm, S.; et al. Effect of Catheter Ablation vs Antiarrhythmic Medication on Quality of Life in Patients with Atrial Fibrillation: The CAPTAF Randomized Clinical Trial. JAMA 2019, 321, 1059–1068. [Google Scholar] [CrossRef]
- Chevalier, P.; Leizorovicz, A.; Maureira, P.; Carteaux, J.P.; Corbineau, H.; Caus, T.; DeBreyne, B.; Mabot, P.; Dechillou, C.; Deharo, J.C.; et al. Left atrial radiofrequency ablation during mitral valve surgery: A prospective randomized multicentre study (SAFIR). Arch. Cardiovasc. Dis. 2009, 102, 769–775. [Google Scholar] [CrossRef]
- Prasad, S.M.; Maniar, H.S.; Camillo, C.J.; Schuessler, R.B.; Boineau, J.P.; Sundt, T.M., 3rd; Cox, J.L.; Damiano, R.J., Jr. The Cox maze III procedure for atrial fibrillation: Long-term efficacy in patients undergoing lone versus concomitant procedures. J. Thorac. Cardiovasc. Surg. 2003, 126, 1822–1828. [Google Scholar] [CrossRef] [Green Version]
- Itoh, A.; Kobayashi, J.; Bando, K.; Niwaya, K.; Tagusari, O.; Nakajima, H.; Komori, S.; Kitamura, S. The impact of mitral valve surgery combined with maze procedure. Eur. J. Cardiothorac. Surg. 2006, 29, 1030–1035. [Google Scholar] [CrossRef] [Green Version]
- Ad, N.; Holmes, S.D.; Rongione, A.J.; Badhwar, V.; Wei, L.; Fornaresio, L.M.; Massimiano, P.S. The long-term safety and efficacy of concomitant Cox maze procedures for atrial fibrillation in patients without mitral valve disease. J. Thorac. Cardiovasc. Surg. 2019, 157, 1505–1514. [Google Scholar] [CrossRef]
- Malaisrie, S.C.; McCarthy, P.M.; Kruse, J.; Matsouaka, R.A.; Churyla, A.; Grau-Sepulveda, M.V.; Friedman, D.J.; Brennan, J.M. Ablation of atrial fibrillation during coronary artery bypass grafting: Late outcomes in a Medicare population. J. Thorac. Cardiovasc. Surg. 2021, 161, 1251–1261.e1251. [Google Scholar] [CrossRef]
- Johnson, W.D.; Ganjoo, A.K.; Stone, C.D.; Srivyas, R.C.; Howard, M. The left atrial appendage: Our most lethal human attachment! Surgical implications. Eur. J. Cardiothorac. Surg. 2000, 17, 718–722. [Google Scholar] [CrossRef] [Green Version]
- Lee, R.; Vassallo, P.; Kruse, J.; Malaisrie, S.C.; Rigolin, V.; Andrei, A.C.; McCarthy, P. A randomized, prospective pilot comparison of 3 atrial appendage elimination techniques: Internal ligation, stapled excision, and surgical excision. J. Thorac. Cardiovasc. Surg. 2016, 152, 1075–1080. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, P.M.; Lee, R.; Foley, J.L.; Phillips, L.; Kanayinkal, T.; Francischelli, D.E. Occlusion of canine atrial appendage using an expandable silicone band. J. Thorac. Cardiovasc. Surg. 2010, 140, 885–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salzberg, S.P.; Plass, A.; Emmert, M.Y.; Desbiolles, L.; Alkadhi, H.; Grunenfelder, J.; Genoni, M. Left atrial appendage clip occlusion: Early clinical results. J. Thorac. Cardiovasc. Surg. 2010, 139, 1269–1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanderian, A.S.; Gillinov, A.M.; Pettersson, G.B.; Blackstone, E.; Klein, A.L. Success of surgical left atrial appendage closure: Assessment by transesophageal echocardiography. J. Am. Coll. Cardiol. 2008, 52, 924–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starck, C.T.; Steffel, J.; Emmert, M.Y.; Plass, A.; Mahapatra, S.; Falk, V.; Salzberg, S.P. Epicardial left atrial appendage clip occlusion also provides the electrical isolation of the left atrial appendage. Interact. Cardiovasc. Thorac. Surg. 2012, 15, 416–418. [Google Scholar] [CrossRef] [Green Version]
- Romero, J.; Gabr, M.; Patel, K.; Briceno, D.; Diaz, J.C.; Alviz, I.; Trivedi, C.; Mohanty, S.; Polanco, D.; Della Rocca, D.G.; et al. Efficacy and safety of left atrial appendage electrical isolation during catheter ablation of atrial fibrillation: An updated meta-analysis. Europace 2021, 23, 226–237. [Google Scholar] [CrossRef]
- Lee, R.; McCarthy, P.M.; Wang, E.C.; Vaduganathan, M.; Kruse, J.; Malaisrie, S.C.; McGee, E.C., Jr. Midterm survival in patients treated for atrial fibrillation: A propensity-matched comparison to patients without a history of atrial fibrillation. J. Thorac. Cardiovasc. Surg. 2012, 143, 1341–1351; discussion 1341–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musharbash, F.N.; Schill, M.R.; Sinn, L.A.; Schuessler, R.B.; Maniar, H.S.; Moon, M.R.; Melby, S.J.; Damiano, R.J., Jr. Performance of the Cox-maze IV procedure is associated with improved long-term survival in patients with atrial fibrillation undergoing cardiac surgery. J. Thorac. Cardiovasc. Surg. 2018, 155, 159–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suwalski, P.; Kowalewski, M.; Jasinski, M.; Staromlynski, J.; Zembala, M.; Widenka, K.; Brykczynski, M.; Skiba, J.; Zembala, M.O.; Bartus, K.; et al. Survival after surgical ablation for atrial fibrillation in mitral valve surgery: Analysis from the Polish National Registry of Cardiac Surgery Procedures (KROK). J. Thorac. Cardiovasc. Surg. 2019, 157, 1007–1018 e1004. [Google Scholar] [CrossRef] [PubMed]
- Iribarne, A.; DiScipio, A.W.; McCullough, J.N.; Quinn, R.; Leavitt, B.J.; Westbrook, B.M.; Robich, M.P.; Sardella, G.L.; Klemperer, J.D.; Kramer, R.S.; et al. Surgical Atrial Fibrillation Ablation Improves Long-Term Survival: A Multicenter Analysis. Ann. Thorac. Surg. 2019, 107, 135–142. [Google Scholar] [CrossRef]
- Ad, N.; Holmes, S.D.; Friehling, T. Minimally Invasive Stand-Alone Cox Maze Procedure for Persistent and Long-Standing Persistent Atrial Fibrillation: Perioperative Safety and 5-Year Outcomes. Circ. Arrhythm. Electrophysiol. 2017, 10, e005352. [Google Scholar] [CrossRef]
- Cox, J.L.; Malaisrie, S.C.; Churyla, A.; Mehta, C.; Kruse, J.; Kislitsina, O.N.; McCarthy, P.M. Cryosurgery for Atrial Fibrillation: Physiologic Basis for Creating Optimal Cryolesions. Ann. Thorac. Surg. 2021, 112, 354–362. [Google Scholar] [CrossRef]
- Wolf, R.K.; Schneeberger, E.W.; Osterday, R.; Miller, D.; Merrill, W.; Flege, J.B., Jr.; Gillinov, A.M. Video-assisted bilateral pulmonary vein isolation and left atrial appendage exclusion for atrial fibrillation. J. Thorac. Cardiovasc. Surg. 2005, 130, 797–802. [Google Scholar] [CrossRef] [Green Version]
- Edgerton, J.R.; Jackman, W.M.; Mahoney, C.; Mack, M.J. Totally thorascopic surgical ablation of persistent AF and long-standing persistent atrial fibrillation using the “Dallas” lesion set. Heart Rhythm. 2009, 6, S64–S70. [Google Scholar] [CrossRef]
- Muneretto, C.; Bisleri, G.; Rosati, F.; Krakor, R.; Giroletti, L.; Di Bacco, L.; Repossini, A.; Moltrasio, M.; Curnis, A.; Tondo, C.; et al. European prospective multicentre study of hybrid thoracoscopic and transcatheter ablation of persistent atrial fibrillation: The HISTORIC-AF trial. Eur. J. Cardiothorac. Surg. 2017, 52, 740–745. [Google Scholar] [CrossRef] [Green Version]
- Geuzebroek, G.S.; Bentala, M.; Molhoek, S.G.; Kelder, J.C.; Schaap, J.; Van Putte, B.P. Totally thoracoscopic left atrial Maze: Standardized, effective and safe. Interact. Cardiovasc. Thorac. Surg. 2016, 22, 259–264. [Google Scholar] [CrossRef]
- Vos, L.M.; Bentala, M.; Geuzebroek, G.S.; Molhoek, S.G.; van Putte, B.P. Long-term outcome after totally thoracoscopic ablation for atrial fibrillation. J. Cardiovasc. Electrophysiol. 2020, 31, 40–45. [Google Scholar] [CrossRef]
- Pison, L.; La Meir, M.; van Opstal, J.; Blaauw, Y.; Maessen, J.; Crijns, H.J. Hybrid thoracoscopic surgical and transvenous catheter ablation of atrial fibrillation. J. Am. Coll. Cardiol. 2012, 60, 54–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krul, S.P.; Driessen, A.H.; van Boven, W.J.; Linnenbank, A.C.; Geuzebroek, G.S.; Jackman, W.M.; Wilde, A.A.; de Bakker, J.M.; de Groot, J.R. Thoracoscopic video-assisted pulmonary vein antrum isolation, ganglionated plexus ablation, and periprocedural confirmation of ablation lesions: First results of a hybrid surgical-electrophysiological approach for atrial fibrillation. Circ. Arrhythm. Electrophysiol. 2011, 4, 262–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Asmundis, C.; Varnavas, V.; Sieira, J.; Ströker, E.; Coutiño, H.E.; Terasawa, M.; Abugattas, J.P.; Salghetti, F.; Maj, R.; Guimarães, O.T.; et al. Two-year follow-up of one-stage left unilateral thoracoscopic epicardial and transcatheter endocardial ablation for persistent and long-standing persistent atrial fibrillation. J. Interv. Card. Electrophysiol. 2020, 58, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Majewski, J.; Bartus, K.; Kapelak, B.; Myc, J.; Sadowski, J.; Lelakowski, J. Thoracoscopic Ex-Maze III procedure and radiofrequency catheter ablation—A hybrid therapy for permanent atrial fibrillation. A case report. Kardiol. Pol. 2009, 67, 1044–1047. [Google Scholar] [PubMed]
- Luo, X.; Li, B.; Zhang, D.; Zhu, J.; Qi, L.; Tang, Y. Efficacy and safety of the convergent atrial fibrillation procedure: A meta-analysis of observational studies. Interact. Cardiovasc. Thorac. Surg. 2019, 28, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLurgio, D.B.; Crossen, K.J.; Gill, J.; Blauth, C.; Oza, S.R.; Magnano, A.R.; Mostovych, M.A.; Halkos, M.E.; Tschopp, D.R.; Kerendi, F.; et al. Hybrid Convergent Procedure for the Treatment of Persistent and Long-Standing Persistent Atrial Fibrillation: Results of CONVERGE Clinical Trial. Circ. Arrhythm. Electrophysiol. 2020, 13, e009288. [Google Scholar] [CrossRef]
- van der Heijden, C.A.J.; Vroomen, M.; Luermans, J.G.; Vos, R.; Crijns, H.; Gelsomino, S.; La Meir, M.; Pison, L.; Maesen, B. Hybrid versus catheter ablation in patients with persistent and longstanding persistent atrial fibrillation: A systematic review and meta-analysis. Eur. J. Cardiothorac. Surg. 2019, 56, 433–443. [Google Scholar] [CrossRef]
- Reddy, V.Y.; Neuzil, P.; Koruth, J.S.; Petru, J.; Funosako, M.; Cochet, H.; Sediva, L.; Chovanec, M.; Dukkipati, S.R.; Jais, P. Pulsed Field Ablation for Pulmonary Vein Isolation in Atrial Fibrillation. J. Am. Coll. Cardiol. 2019, 74, 315–326. [Google Scholar] [CrossRef]
- De Potter, T.J.R.; Boersma, L.V.A. Ultra-low temperature cryoablation: The coolest innovation EP has been waiting for? J. Cardiovasc. Electrophysiol. 2021, 32, 578–579. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AF | AFL | VT | SVT | |
|---|---|---|---|---|
| Catheter ablation procedures (unweighted) | 39,562 | 25,723 | 9642 | 33,346 |
| Catheter ablation procedures (weighted) | 190,398 | 123,163 | 46,495 | 159,895 |
| ≥1 complication | 7.21 | 3.91 | 9.90 | 3.29 |
| Mortality | 0.24 | 0.20 | 1.82 | 0.12 |
| Post-procedural stroke or TIA | 0.31 | 0.19 | 0.38 | 0.14 |
| Post-procedural infection | 0.26 | 0.32 | 1.07 | 0.18 |
| Cardiac complications a | 1.15 | 0.53 | 1.24 | 0.68 |
| Pericardial complications | 2.02 | 0.41 | 2.47 | 0.81 |
| Vascular complications | 1.09 | 0.64 | 2.08 | 0.48 |
| Hemorrhage | 3.64 | 2.04 | 3.67 | 1.37 |
| Hemorrhage requiring transfusion | 0.69 | 0.37 | 0.86 | 0.18 |
| Diaphragm paralysis | 0.11 | 0.05 | 0.02 | 0.04 |
| Pneumothorax or hemothorax | 0.14 | 0.09 | 0.04 | 0.15 |
| Length of stay | 2.63 ± 0.06 | 3.18 ± 0.05 | 4.7 ± 0.09 | 2.22 ± 0.04 |
| Trial, Year | Number of Pts | Technology | Control 12 Month NSR | Treated 12 Month NSR |
|---|---|---|---|---|
| Deneke et al., 2002 | 30 | Unipolar Cooled RF | 26.7% | 80% (p < 0.01) |
| Schuetz et al., 2003 | 43 | Microwave | 33.3% | 80% (p = 0.036) |
| Akpinar et al., 2003 | 67 | Unipolar RF | 9.4% | 93.6% (p = 0.0001) |
| Abreu Filho et al., 2005 | 70 | Unipolar Cooled RF | 26.9% | 79.4% (p = 0.001) |
| Doukas et al., 2005 | 101 | Unipolar RF | 4.5% | 44.4% (p = 0.001) |
| Blomström-Lunqvist 2007 | 69 | Cryoablation | 42.9% | 73.3% (p = 0.013) |
| Chevalier 2009 | 43 | Unipolar RF | 4% | 57% (p = 0.004) |
| Gillinov, 2015 | 260 | Cryoablation | 29% | 63.2% (p < 0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McCarthy, P.M.; Cox, J.L.; Kislitsina, O.N.; Kruse, J.; Churyla, A.; Malaisrie, S.C.; Mehta, C.K. Surgery and Catheter Ablation for Atrial Fibrillation: History, Current Practice, and Future Directions. J. Clin. Med. 2022, 11, 210. https://doi.org/10.3390/jcm11010210
McCarthy PM, Cox JL, Kislitsina ON, Kruse J, Churyla A, Malaisrie SC, Mehta CK. Surgery and Catheter Ablation for Atrial Fibrillation: History, Current Practice, and Future Directions. Journal of Clinical Medicine. 2022; 11(1):210. https://doi.org/10.3390/jcm11010210
Chicago/Turabian StyleMcCarthy, Patrick M., James L. Cox, Olga N. Kislitsina, Jane Kruse, Andrei Churyla, S. Chris Malaisrie, and Christopher K. Mehta. 2022. "Surgery and Catheter Ablation for Atrial Fibrillation: History, Current Practice, and Future Directions" Journal of Clinical Medicine 11, no. 1: 210. https://doi.org/10.3390/jcm11010210
APA StyleMcCarthy, P. M., Cox, J. L., Kislitsina, O. N., Kruse, J., Churyla, A., Malaisrie, S. C., & Mehta, C. K. (2022). Surgery and Catheter Ablation for Atrial Fibrillation: History, Current Practice, and Future Directions. Journal of Clinical Medicine, 11(1), 210. https://doi.org/10.3390/jcm11010210