
Poorly Differentiated Neuroendocrine Larynx Carcinoma: Clinical Features and miRNAs Signature—A New Goal for Early Diagnosis and Therapy?

 , ,
, ,  , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Tissues and Patients
2.2. RNA Extraction
2.3. RT-qPCR for miRNA and mRNA Expression
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Patients
3.2. Patient Management
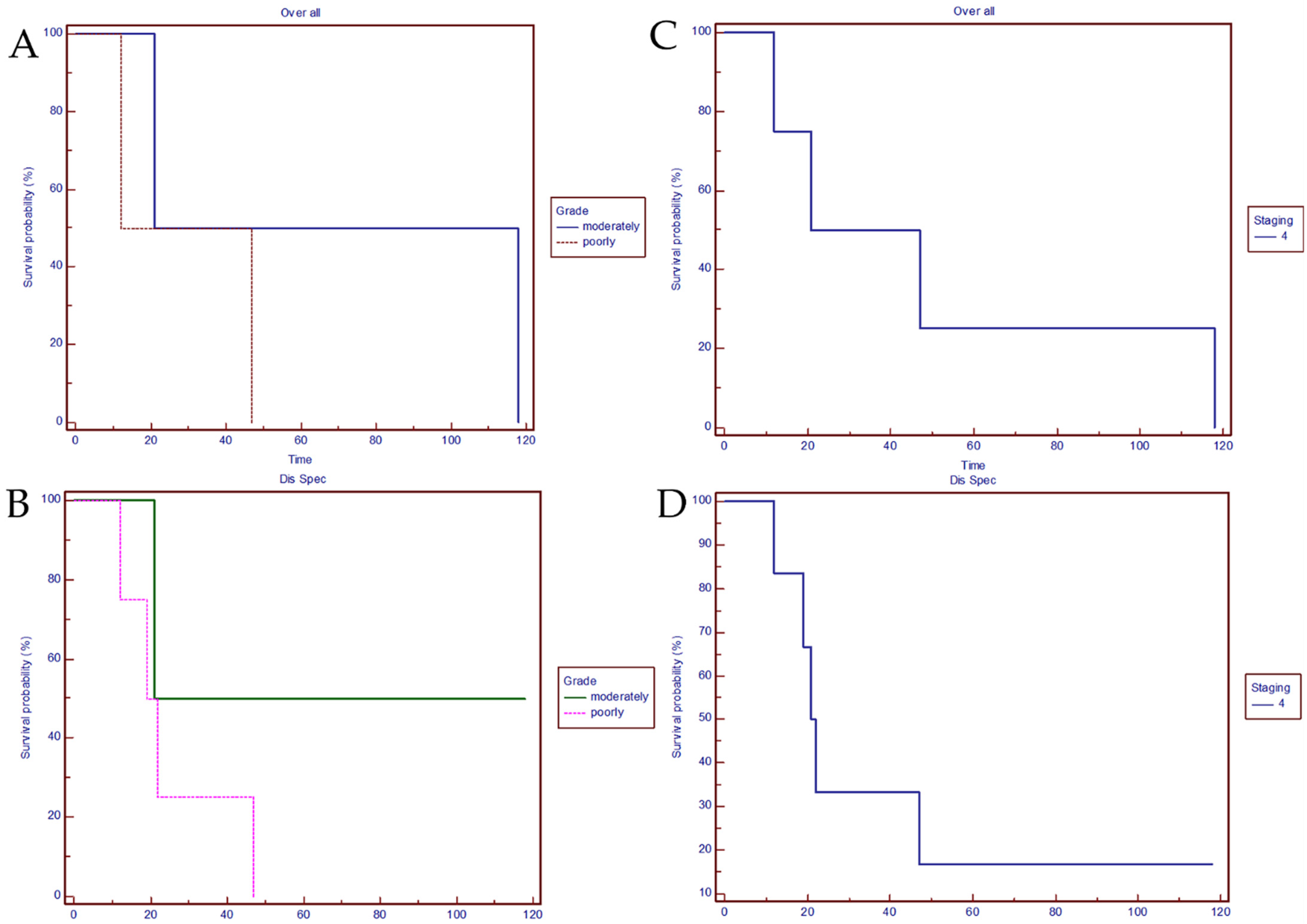
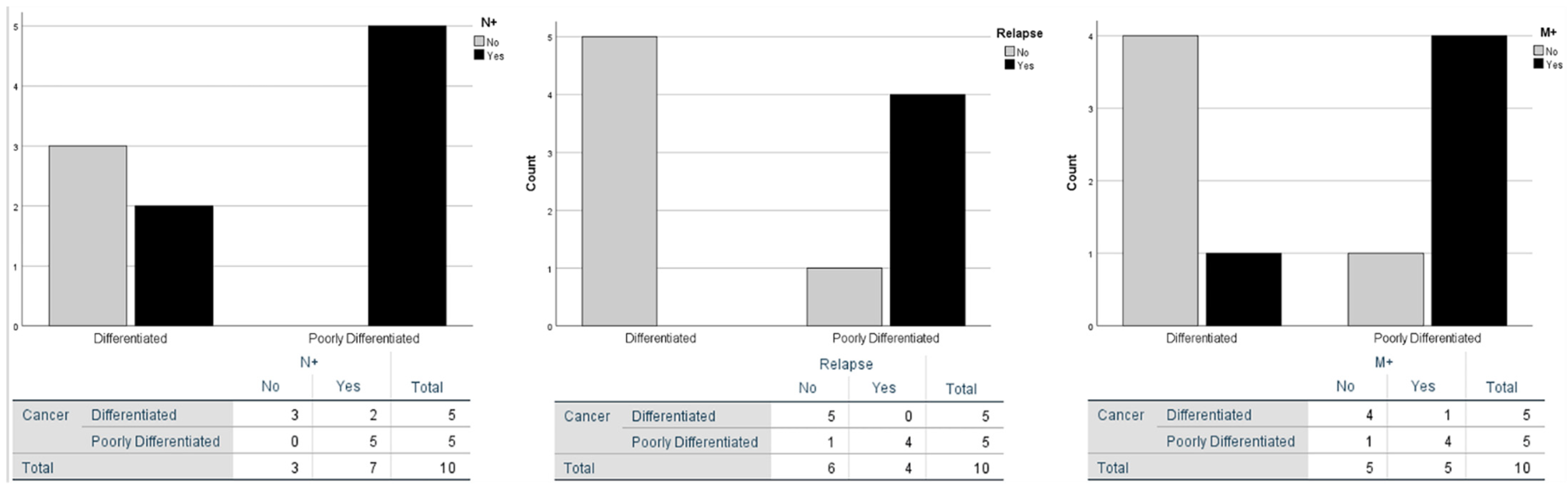
3.3. Clinical Statistical Analysis
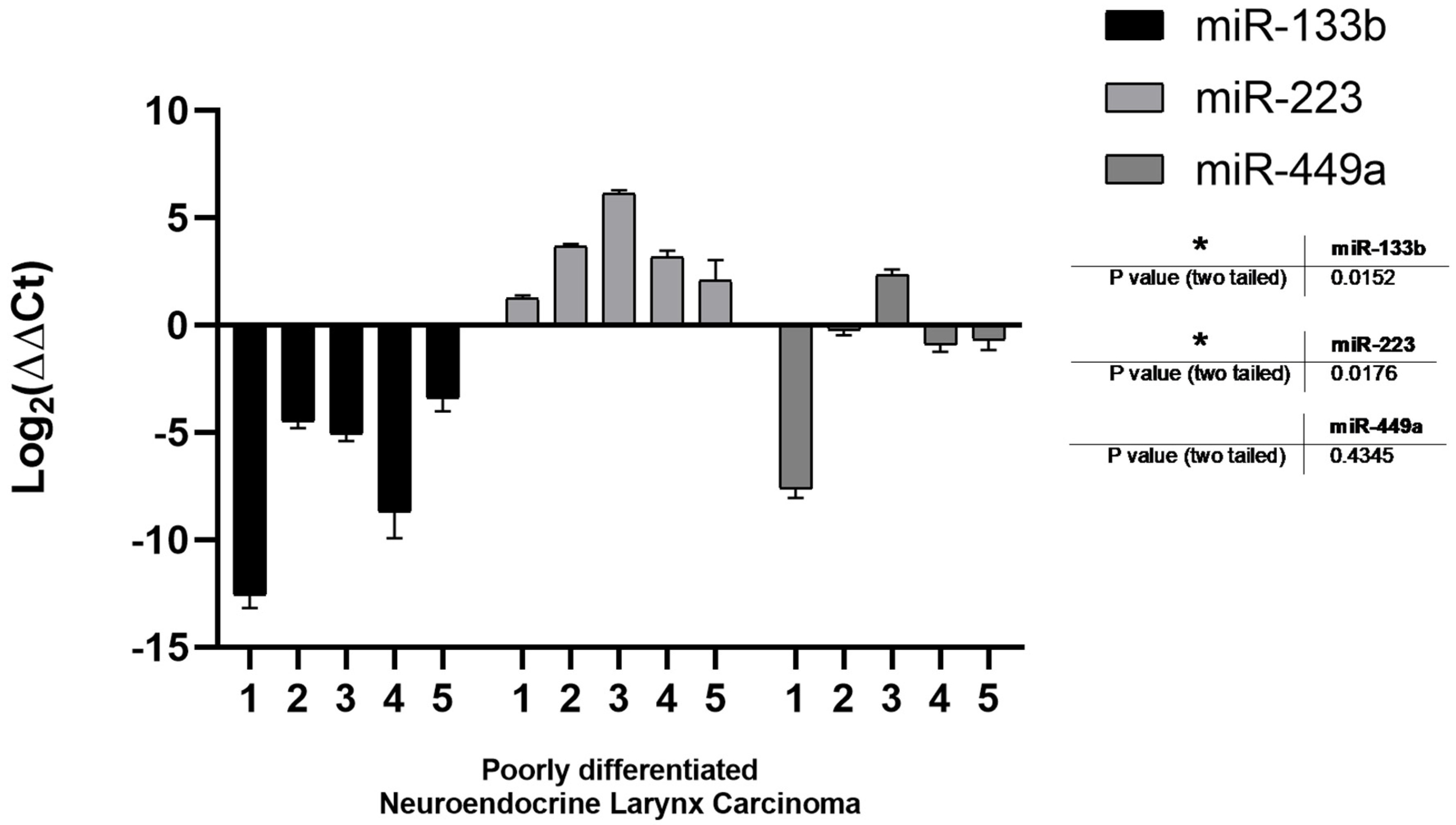
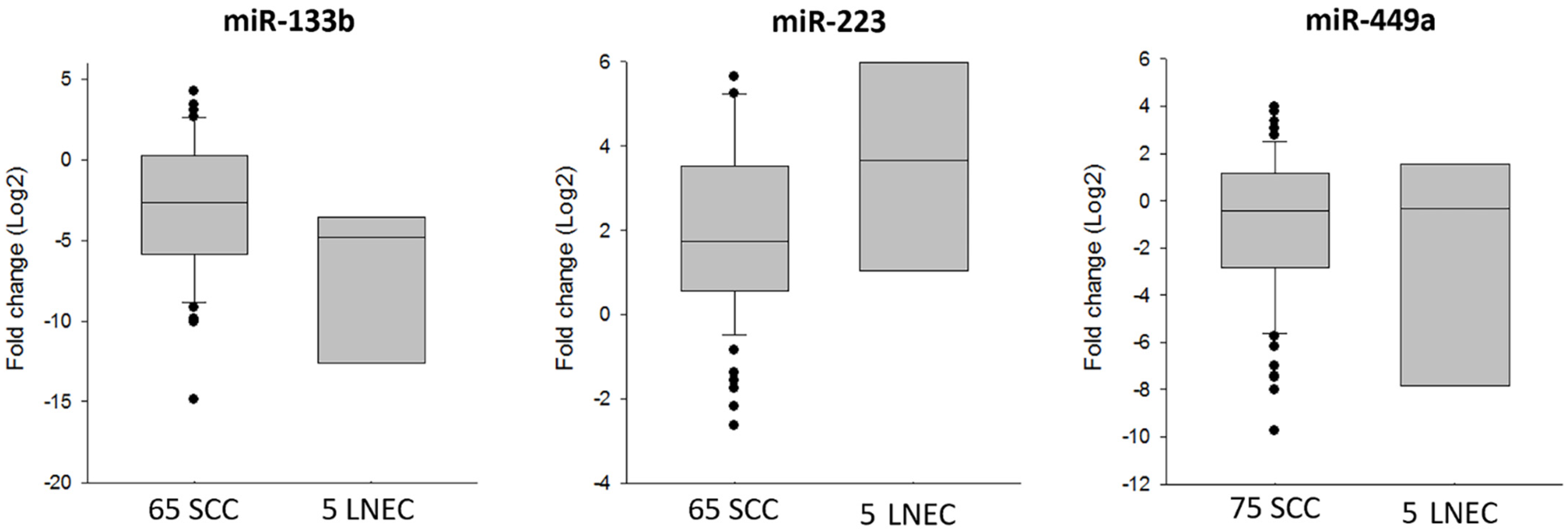
3.4. MicroRNA Analysis
4. Discussion
4.1. Clinical Evidence
- fibroscopy of the upper respiratory tract every month for three months, every three months for two years, and then every six months for three years;
- total body TAC-PET six months after the end of the treatment and then every six months for two years.
4.2. miRNAs Clinical Value
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, H.W.; Bhattacharyya, N. Staging and Survival Analysis for Nonsquamous Cell Carcinomas of the Larynx. Laryngoscope 2008, 118, 1003–1013. [Google Scholar] [CrossRef]
- Ferlito, A.; Silver, C.E.; Bradford, C.R.; Rinaldo, A. Neuroendocrine neoplasms of the larynx: An overview. Head Neck 2009, 31, 1634–1646. [Google Scholar] [CrossRef]
- Strosberg, C.; Ferlito, A.; Triantafyllou, A.; Gnepp, D.R.; Bishop, J.A.; Hellquist, H.; Strojan, P.; Willems, S.M.; Stenman, G.; Rinaldo, A.; et al. Update on Neuroendocrine Carcinomas of the Larynx. Am. J. Clin. Pathol. 2019, 152, 686–700. [Google Scholar] [CrossRef]
- Ferlito, A.; Rinaldo, A.; Bishop, J.A.; Hunt, J.L.; Vander Poorten, V.; Williams, M.D.; Triantafyllou, A.; Devaney, K.O.; Gnepp, D.R.; Kusafuka, K.; et al. Paraneoplastic syndromes in patients with laryngeal neuroendocrine carcinomas: Clinical manifestations and prognostic significance. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 533–536. [Google Scholar] [CrossRef]
- El-Naggar, A.K. Editor’s perspective on the 4th edition of the WHO head and neck tumor classification. J. Egypt. Natl. Cancer Inst. 2017, 29, 65–66. [Google Scholar] [CrossRef]
- Leung, S.C.Y.; Nielsen, T.O.; Zabaglo, L.; Arun, I.; Badve, S.S.; Bane, A.L.; Bartlett, J.M.S.; Borgquist, S.; Chang, M.C.; Dodson, A.; et al. Analytical validation of a standardized scoring protocol for Ki67: Phase 3 of an international multicenter collaboration. NPJ Breast Cancer 2016, 2, 16014. [Google Scholar] [CrossRef]
- Bellizzi, A.M. Immunohistochemistry in the diagnosis and classification of neuroendocrine neoplasms: What can brown do for you? Hum. Pathol. 2020, 96, 8–33. [Google Scholar] [CrossRef]
- Takeuchi, T.; Kawasaki, H.; Luce, A.; Cossu, A.M.; Misso, G.; Scrima, M.; Bocchetti, M.; Ricciardiello, F.; Caraglia, M.; Zappavigna, S. Insight toward the MicroRNA Profiling of Laryngeal Cancers: Biological Role and Clinical Impact. Int. J. Mol. Sci. 2020, 21, 3693. [Google Scholar] [CrossRef]
- Ricciardiello, F.; Capasso, R.; Kawasaki, H.; Abate, T.; Oliva, F.; Lombardi, A.; Misso, G.; Ingrosso, D.; Leone, C.A.; Iengo, M.; et al. A miRNA signature suggestive of nodal metastases from laryngeal carcinoma. Acta Otorhinolaryngol. Ital. 2017, 37, 467–474. [Google Scholar] [CrossRef]
- Kawasaki, H.; Takeuchi, T.; Ricciardiello, F.; Lombardi, A.; Biganzoli, E.; Fornili, M.; De Bortoli, D.; Mesolella, M.; Cossu, A.M.; Scrima, M.; et al. Definition of miRNA Signatures of Nodal Metastasis in LCa: miR-449a Targets Notch Genes and Suppresses Cell Migration and Invasion. Mol. Ther.-Nucleic Acids 2020, 20, 711–724. [Google Scholar] [CrossRef]
- Wei, Z.; Chang, K.; Fan, C. Hsa_circ_0042666 inhibits proliferation and invasion via regulating miR-223/TGFBR3 axis in laryngeal squamous cell carcinoma. Biomed. Pharm. 2019, 119, 109365. [Google Scholar] [CrossRef]
- Doescher, J.; Veit, J.A.; Hoffmann, T.K. The 8th edition of the AJCC Cancer Staging Manual: Updates in otorhinolaryngology, head and neck surgery. Hno 2017, 65, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Gao, L.; Meng, Y.; Diao, W.; Zhu, X.; Li, G.; Gao, Z.; Chen, X. Laryngeal Neuroendocrine Carcinomas: A Retrospective Study of 14 Cases. BioMed Res. Int. 2015, 2015, 832194. [Google Scholar] [CrossRef]
- Gnepp, D.R. Small Cell Neuroendocrine Carcinoma of the Larynx. ORL 1991, 53, 210–219. [Google Scholar] [CrossRef]
- Baugh, R.F.; Wolf, G.T.; Krause, C.J.; Beals, T.F.; Forastiere, A. Small Cell Carcinoma of the Larynx: Results of Therapy. Laryngoscope 1986, 96, 1283–1290. [Google Scholar] [CrossRef]
- Ferlito, A.; Rinaldo, A. Primary and secondary small cell neuroendocrine carcinoma of the larynx: A review. Head Neck 2008, 30, 518–524. [Google Scholar] [CrossRef]
- Zhao, N.; Liu, H.; Zhang, A.; Wang, M. Expression levels and clinical significance of miR-203 and miR-133b in laryngeal carcinoma. Oncol. Lett. 2020, 20, 213. [Google Scholar] [CrossRef]
- Chen, G.Y.; Ruan, L. Downregulation Of microRNA-133b And Its Clinical Value In Non-Small Cell Lung Cancer. OncoTargets Ther. 2019, 12, 9421–9434. [Google Scholar] [CrossRef]
- Chen, S.W.; Wang, T.B.; Tian, Y.H.; Zheng, Y.G. Down-regulation of microRNA-126 and microRNA-133b acts as novel predictor biomarkers in progression and metastasis of non small cell lung cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 14983–14988. [Google Scholar]
- Wu, D.; Pan, H.; Zhou, Y.; Zhou, J.; Fan, Y.; Qü, P. microRNA-133b downregulation and inhibition of cell proliferation, migration and invasion by targeting matrix metallopeptidase-9 in renal cell carcinoma. Mol. Med. Rep. 2014, 9, 2491–2498. [Google Scholar] [CrossRef]
- Lin, C.; Xie, L.; Lu, Y.; Hu, Z.; Chang, J. miR-133b reverses cisplatin resistance by targeting GSTP1 in cisplatin-resistant lung cancer cells. Int. J. Mol. Med. 2018, 41, 2050–2058. [Google Scholar] [CrossRef]
- Zhang, K.; Zhou, H.; Yan, B.; Cao, X. TUG1/miR-133b/CXCR4 axis regulates cisplatin resistance in human tongue squamous cell carcinoma. Cancer Cell Int. 2020, 20, 1–13. [Google Scholar] [CrossRef]
- Hou, B.; Ishinaga, H.; Midorikawa, K.; Shah, S.A.; Nakamura, S.; Hiraku, Y.; Oikawa, S.; Murata, M.; Takeuchi, K. Circulating microRNAs as novel prognosis biomarkers for head and neck squamous cell carcinoma. Cancer Biol. Ther. 2015, 16, 1042–1046. [Google Scholar] [CrossRef]
- Pomari, E.; Lovisa, F.; Carraro, E.; Primerano, S.; D’Amore, E.S.G.; Bonvini, P.; Nigro, L.L.; De Vito, R.; Vinti, L.; Farruggia, P.; et al. Clinical impact of miR-223 expression in pediatric T-Cell lymphoblastic lymphoma. Oncotarget 2017, 8, 107886–107898. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, A.; Khorshid, H.R.K.; Mowla, S.J.; Mohebbi, H.A.; Mohammadian, A.; Yaseri, M.; Solaymani-Dodaran, M.; Sherafatian, M.; Tavallaie, M. Altered miR-223 Expression in Sputum for Diagnosis of Non-Small Cell Lung Cancer. Avicenna J. Med. Biotechnol. 2017, 9, 189–195. [Google Scholar] [PubMed]
- Fassan, M.; Saraggi, D.; Balsamo, L.; Realdon, S.; Scarpa, M.; Castoro, C.; Coati, I.; Salmaso, R.; Farinati, F.; Guzzardo, V.; et al. Early miR-223 Upregulation in Gastroesophageal Carcinogenesis. Am. J. Clin. Pathol. 2017, 147, 301–308. [Google Scholar] [CrossRef]
- Purwanto, I.; Heriyanto, D.S.; Widodo, I.; Hakimi, M.; Hardianti, M.S.; Aryandono, T.; Haryana, S.M. MicroRNA-223 is Associated with Resistance Towards Platinum-based Chemotherapy and Worse Prognosis in Indonesian Triple-negative Breast Cancer Patients. Breast Cancer Targets Ther. 2021, 13, 1–7. [Google Scholar] [CrossRef]
- Zhou, Y.; Chen, E.; Tang, Y.; Mao, J.; Shen, J.; Zheng, X.; Xie, S.; Zhang, S.; Wu, Y.; Liu, H.; et al. miR-223 overexpression inhibits doxorubicin-induced autophagy by targeting FOXO3a and reverses chemoresistance in hepatocellular carcinoma cells. Cell Death Dis. 2019, 10, 1–13. [Google Scholar] [CrossRef]
- Wu, D.; Liu, J.; Chen, J.; He, H.; Ma, H.; Lv, X. miR-449a Suppresses Tumor Growth, Migration, and Invasion in Non-Small Cell Lung Cancer by Targeting a HMGB1-Mediated NF-κB Signaling Pathway. Oncol. Res. Featur. Preclin. Clin. Cancer 2019, 27, 227–235. [Google Scholar] [CrossRef]
- You, J.; Zhang, Y.; Li, Y.; Fang, N.; Liu, B.; Zu, L.; Zhou, Q. MiR-449a suppresses cell invasion by inhibiting MAP2K1 in non-small cell lung cancer. Am. J. Cancer Res. 2015, 5, 2730–2744. [Google Scholar]
- Ishikawa, D.; Yoshikawa, K.; Takasu, C.; Kashihara, H.; Nishi, M.; Tokunaga, T.; Higashijima, J.; Shimada, M. Expression Level of MicroRNA-449a Predicts the Prognosis of Patients with Gastric Cancer. Anticancer. Res. 2019, 40, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Mao, A.; Zhao, Q.; Zhou, X.; Sun, C.; Si, J.; Zhou, R.; Gan, L.; Zhang, H. MicroRNA-449a enhances radiosensitivity by downregulation of c-Myc in prostate cancer cells. Sci. Rep. 2016, 6, 27346. [Google Scholar] [CrossRef] [PubMed]
- Van Der Laan, T.P.; Plaat, B.E.C.; Van Der Laan, B.F.A.M.; Halmos, G.B. Clinical recommendations on the treatment of neuroendocrine carcinoma of the larynx: A meta-analysis of 436 reported cases. Head Neck 2014, 37, 707–715. [Google Scholar] [CrossRef]
- Moertel, C.G.; Kvols, L.K.; O’Connell, M.J.; Rubin, J. Treatment of neuroendocrine carcinomas with combined etoposide and cisplatin. Evidence of major therapeutic activity in the anaplastic variants of these neoplasms. Cancer 1991, 68, 227–232. [Google Scholar] [CrossRef]
- Mitry, E.; Baudin, E.; Ducreux, M.; Sabourin, J.C.; Rufié, P.; Aparicio, T.; Lasser, P.; Elias, D.; Duvillard, P.; Schlumberger, M.; et al. Treatment of poorly differentiated neuroendocrine tumours with etoposide and cisplatin. Br. J. Cancer 1999, 81, 1351–1355. [Google Scholar] [CrossRef] [PubMed]
- Rinke, A.; Gress, T.M. Neuroendocrine Cancer, Therapeutic Strategies in G3 Cancers. Digestion 2017, 95, 109–114. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Age | 69 | 58 | 55 | 58 | 60 | 70 | 49 | 57 | 81 | 74 |
| Sex | M | F | M | F | F | M | M | M | M | M |
| Voluptuous Habits | Smoke | Smoke Alcohol | Smoke | None | Smoke | None | Smoke Alcohol | Smoke Alcohol | Smoke Alcohol | Smoke Alcohol |
| Tumor site | Supraglottic/Glottic | Supraglottic | Glottic/Supraglottic | Supraglottic | Supraglottic | Supraglottic | Hypopharyngolaryngeal | Glottic/Supraglottic | Glottic/Supraglottic | Supraglottic |
| Histological Differentiation | Poorly Large Cells | Poorly Small Cells | Poorly Large Cells | Poorly Small Cells | Moderately G2 | Well G1 | Moderately G2 | Well G1 | Poorly Large Cells | Moderately G2 |
| Diagnosis | Nov 15 | Sep 17 | Jan 18 | Feb 18 | Jan 18 | Feb 17 | Feb 18 | Feb 17 | Dec 14 | Dec 09 |
| Initial Treatment | TL | TL | TL | OPHLI | OPHLI | Laser Cordectomy | Hypopharyngolaryngectomy | TL | TL | OPHL I |
| pTNM | PT4aN3M0 | PT4aN2aM0 | PT3N3AM0 | PT3N2AM0 | PT3N2BM0 | PT1N0M0 | PT4ANOM0 | PT3N0M1 | PT4aN3M0 | PT4aN2aM0 |
| Neck Dissection | LLND | LLND | LLND | LLND | LLND | NO | LLND | LLND | LLND | LLND |
| Adjuvant Therapy | ChRT | RT | ChRT | ChRT | RT | NONE | RT | Ch | NONE | NONE |
| Follow Up (months) | 47 | 25 | 22 | 19 | 22 | 30 | 21 | 30 | 12 | 118 |
| Vital Status | † M | Follow Up | M | M | Follow Up | Follow Up | † M | Follow Up | † N Recurrence And M | † Other Cause |
| Poorly Differentiated LNEC | M+ | N+ | Relapse | ||
|---|---|---|---|---|---|
| Poorly differentiated LNEC | Pearson Correlation | 1 | 0.600 | 0.655 * | 0.816 ** |
| Sig. (2-tailed) | 0.067 | 0.040 | 0.004 | ||
| N | 10 | 10 | 10 | 10 | |
| M+ | Pearson Correlation | 0.600 | 1 | 0.218 | 0.816 ** |
| Sig. (2-tailed) | 0.067 | 0.545 | 0.004 | ||
| N | 10 | 10 | 10 | 10 | |
| N+ | Pearson Correlation | 0.655 * | 0.218 | 1 | 0.535 |
| Sig. (2-tailed) | 0.040 | 0.545 | 0.111 | ||
| N | 10 | 10 | 10 | 10 | |
| Relapse | Pearson Correlation | 0.816 ** | 0.816 ** | 0.535 | 1 |
| Sig. (2-tailed) | 0.004 | 0.004 | 0.111 | ||
| N | 10 | 10 | 10 | 10 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricciardiello, F.; Falco, M.; Tortoriello, G.; Riccardi, F.; Pellini, R.; Iorio, B.; Russo, G.; Longo, G.; Coppola, C.; Takeuchi, T.; et al. Poorly Differentiated Neuroendocrine Larynx Carcinoma: Clinical Features and miRNAs Signature—A New Goal for Early Diagnosis and Therapy? J. Clin. Med. 2021, 10, 2019. https://doi.org/10.3390/jcm10092019
Ricciardiello F, Falco M, Tortoriello G, Riccardi F, Pellini R, Iorio B, Russo G, Longo G, Coppola C, Takeuchi T, et al. Poorly Differentiated Neuroendocrine Larynx Carcinoma: Clinical Features and miRNAs Signature—A New Goal for Early Diagnosis and Therapy? Journal of Clinical Medicine. 2021; 10(9):2019. https://doi.org/10.3390/jcm10092019
Chicago/Turabian StyleRicciardiello, Filippo, Michela Falco, Giuseppe Tortoriello, Ferdinando Riccardi, Raul Pellini, Brigida Iorio, Giuseppe Russo, Giuseppe Longo, Ciro Coppola, Takashi Takeuchi, and et al. 2021. "Poorly Differentiated Neuroendocrine Larynx Carcinoma: Clinical Features and miRNAs Signature—A New Goal for Early Diagnosis and Therapy?" Journal of Clinical Medicine 10, no. 9: 2019. https://doi.org/10.3390/jcm10092019
APA StyleRicciardiello, F., Falco, M., Tortoriello, G., Riccardi, F., Pellini, R., Iorio, B., Russo, G., Longo, G., Coppola, C., Takeuchi, T., Grimaldi, A., Abate, M., Scrima, M., Cossu, A. M., Addeo, R., Ottaiano, A., Scarpa, A., Boscaino, A., Motta, G., ... Misso, G. (2021). Poorly Differentiated Neuroendocrine Larynx Carcinoma: Clinical Features and miRNAs Signature—A New Goal for Early Diagnosis and Therapy? Journal of Clinical Medicine, 10(9), 2019. https://doi.org/10.3390/jcm10092019