
Evidence-Based Aerobic Exercise Training in Metabolic-Associated Fatty Liver Disease: Systematic Review with Meta-Analysis

 ,
,  , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Types of Participants
2.1.2. Types of Interventions
2.1.3. Types of Comparisons
2.1.4. Types of Outcomes
2.1.5. Types of Studies
2.2. Search Strategy and Study Selection
2.3. Quality and Risk of Bias Assessment
2.4. Statistical Analysis
3. Results
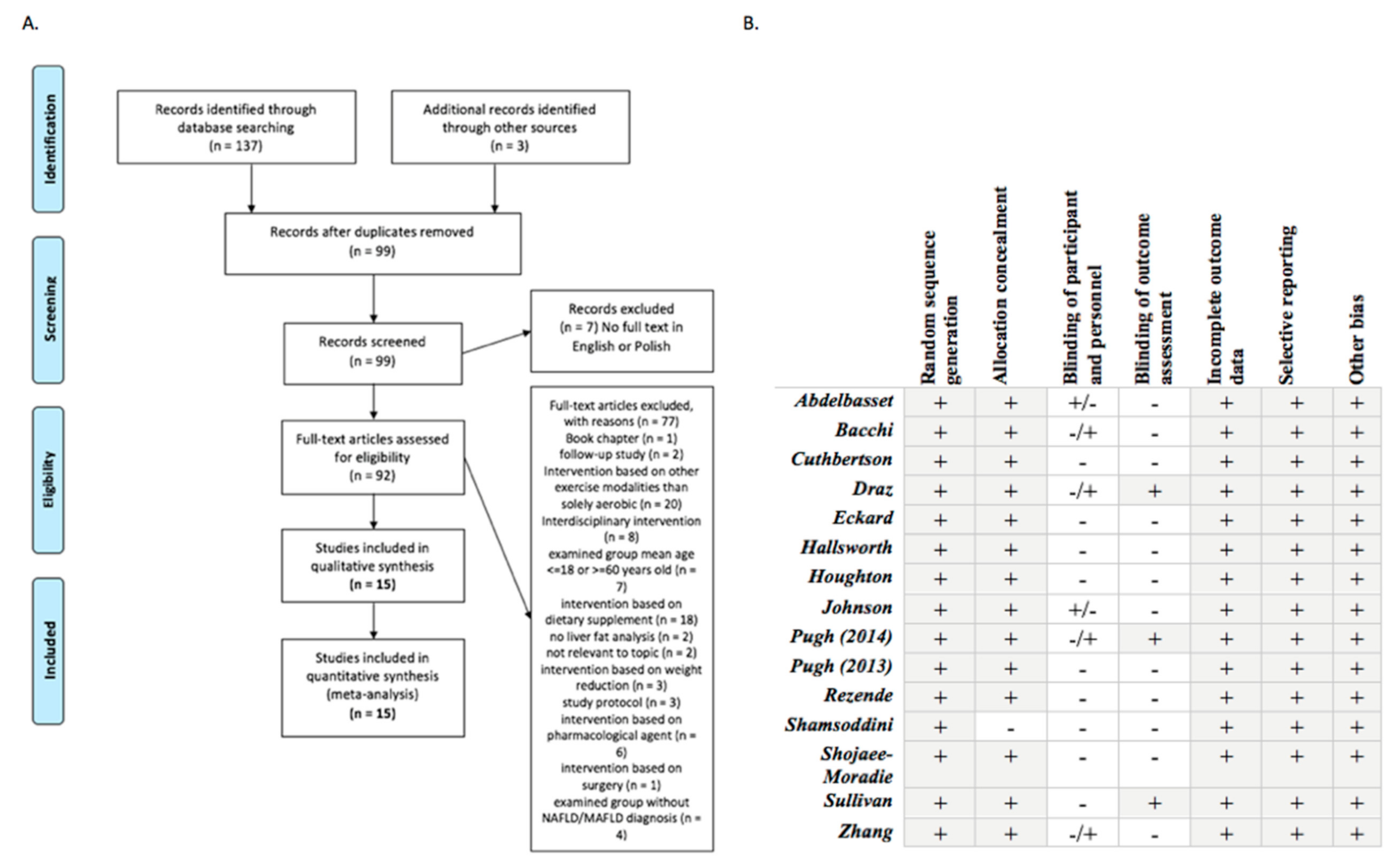
3.1. Study Selection
3.2. Participant Characteristics
3.3. Intervention; Comparison to ACSM Guidelines Characteristics
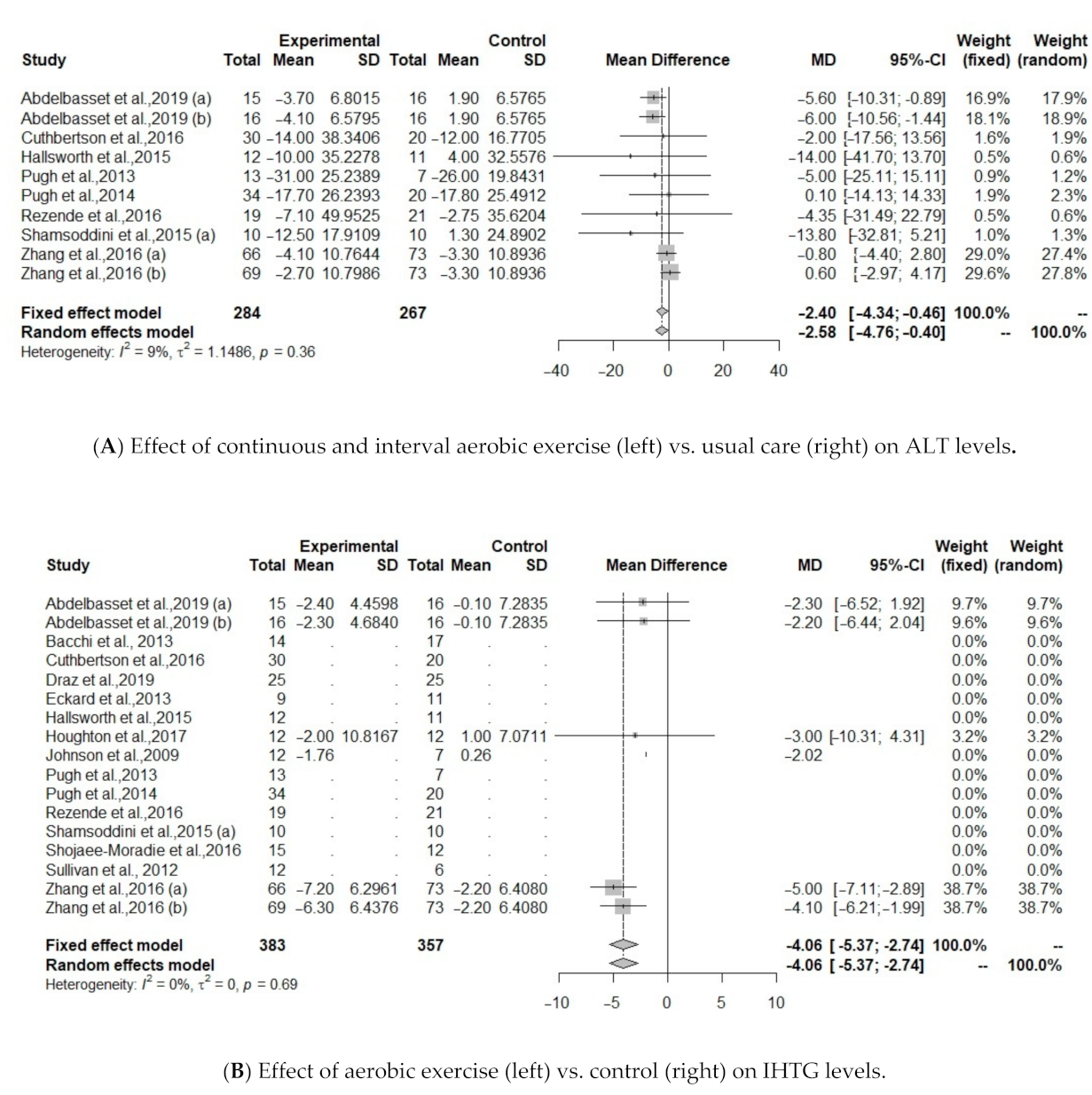
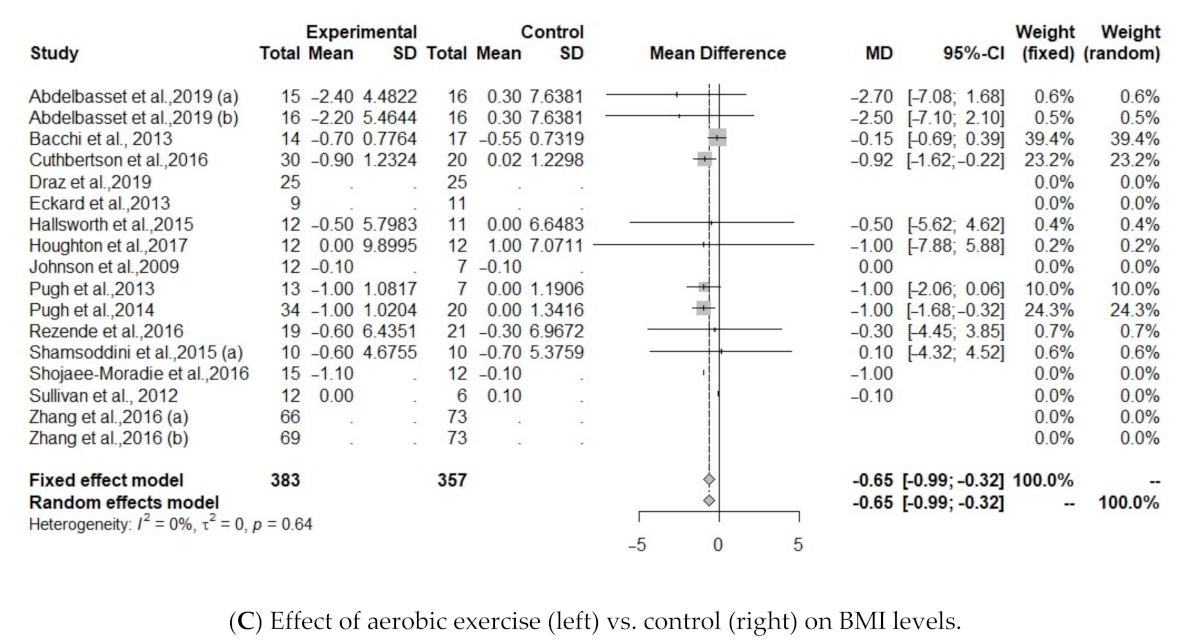
3.4. Effect of Aerobic Exercise on Changes in Serum Levels of Liver, Intrahepatic Triglycerides, Glucose Metabolism and Body Mass Index
3.5. Meta-Regression Analysis Result
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jarvis, H.; Craig, D.; Barker, R.; Spiers, G.; Stow, D.; Anstee, Q.A.; Hanratty, B. Metabolic risk factors and incident advanced liver disease in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of population-based observational studies. PLoS Med. 2020, 17, e1003100. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Shira Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Younossi, Y.Z.; Tacke, F.; Arrese, M.; Sharma, B.C.; Mostafa, I.; Bugianesi, E.; Wong, V.W.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis. Hepatology 2019, 69, 6. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Blissett, D.; Blissett, R.; Henry, L.; Stepanova, M.; Younossi, Y. The economic and clinical burden of non-alcoholic fatty liver disease in the United States and Europe. Hepatology 2016, 64, 1577–1586. [Google Scholar] [CrossRef] [PubMed]
- Qing, Y.; Biyao, Z.; Yee Hui, Y.; Jie, L.; Daniel, Q.H.; Yuankai, W.; Hongli, Y.; Chuanli, L.; Leslie, Y.K.; Xiang, X.; et al. Global prevalence, incidence, and outcomes of non-obese or lean non-alcoholic fatty liver disease: A systematic review and meta-analysis. Lancet Gastroenerol. Hepatol. 2020, 5, 739–752. [Google Scholar]
- Carneros, D.; Lopez-Lluch, G.; Bustos, M. Physiopathology of lifestyle interventions in non-alcoholic fatty liver disease. Nutriens 2020, 12, 3472. [Google Scholar] [CrossRef]
- EASL. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- O’Gorman, P.; Naimimohasses, S.; Monaghan, A.; Kennedy, M.; Melo, A.M.; Ní Fhloinn, D.; Doherty, D.G.; Beddy, P.; Finn, S.P.; Moore, J.B.; et al. Improvement in histological endpoints of MAFLD following a 12-week aerobic exercise intervention. Aliment. Pharmacol. Ther. 2020, 52, 1387–1398. [Google Scholar] [CrossRef] [PubMed]
- Hashida, R.; Kawaguchi, T.; Bekki, M.; Omoto, M.; Matsuse, H.; Nago, T.; Takano, Y.; Ueno, T.; Koga, H.; George, J.; et al. Aerobic vs. resistance exercise in non- alcoholic fatty liver disease: A systematic review. J. Hepatol. 2017, 66, 142–152. [Google Scholar] [CrossRef]
- Hallsworth, K.; Adams, L.A. Lifestyle modification in NAFLD/NASH: Facts and figures. JHEP Rep. 2019, 1, 468–479. [Google Scholar] [CrossRef]
- Fernandes, M.; Silva, L.; Kubrusly, M.S.; Lima, T.; Muller, C.R.; Américo, A.; Fernandes, M.P.; Cogliati, B.; Stefano, J.T.; Lagranha, C.J.; et al. Aerobic Exercise Training Exerts Beneficial Effects Upon Oxidative Metabolism and Non-Enzymatic Antioxidant Defense in the Liver of Leptin Deficiency. Mice. Front. Endocrinol. 2020, 11, 588502. [Google Scholar]
- Diniz, T.A.; Lima Junior, E.A.; Teixeira, A.A.; Biondo, L.A.; Rocha, L.; Valadao, I.C.; Silveira, L.S.; Cabral-Santos, C.; Souza, C.O.; Neto, J.C.R. Aerobic training improves NAFLD markers and insulin resistance through AMPK-PPAR-α signaling in obese mice. Life Sci. 2021, 266, 118868. [Google Scholar] [CrossRef] [PubMed]
- Orci, L.A.; Gariani, K.; Oldani, G.; Delaune, V.; Morel, P.; Toso, C. Exercise-based interventions for nonalcoholic fatty liver disease: A meta-analysis and meta-regression. Clin. Gastroenterol. Hepatol. 2016, 14, 1398–1411. [Google Scholar] [CrossRef] [PubMed]
- Keating, S.E.; Hackett, D.A.; George, J.; Johnson, N. Exercise and non-alcoholic fatty liver disease: A systematic review and meta-analysis. J. Hepatol. 2012, 57, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Smart, N.A.; King, N.; McFarlane, J.R.; Graham, P.L.; Dieberg, G. Effect of exercise training on liver function in adults who are overweight or exhibit fatty liver disease: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 834–843. [Google Scholar] [CrossRef] [PubMed]
- Sargeant, J.A.; Gray, L.J.; Bodicoat, D.H.; Willis, S.A.; Stensel, D.J.; Nimmo, M.A.; Aithal, G.P.; King, J.A. The effect of exercise training on intrahepatic triglyceride and hepatic insulin sensitivity: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 1446–1459. [Google Scholar] [CrossRef] [PubMed]
- Zou, T.T.; Zhang, C.; Zhou, Y.F.; Han, Y.J.; Xiong, J.J.; Wu, X.X.; Chen, Y.P.; Zheng, M.H. Lifestyle interventions for patients with nonalcoholic fatty liver disease: A network meta-analysis. Eur. J. Gastroenterol. Hepatol. 2018, 30, 747–755. [Google Scholar] [CrossRef]
- Katsagoni, C.N.; Georgoulis, M.; Papatheodoridis, G.V.; Panagiotakos, D.B.; Kontogianni, M.D. Effects of lifestyle interventions on clinical characteristics of patients with non-alcoholic fatty liver disease: A meta-analysis. Metabolism 2017, 68, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-J.; Zhang, Z.-G.; Li, H. Time to step-up the fight against NAFLD. Hepatology 2018, 67, 6. [Google Scholar]
- Berzigotti, A.; Saran, U.; Dufour, J. Physical activity and liver diseases. Hepatology 2016, 63, 3. [Google Scholar] [CrossRef]
- DeSimone, G. The Tortoise Factor—Get FITT. ACSM’s Health Fit. J. 2019, 23, 3–4. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomized trials. Br. Med. J. 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Easterbrook, P.J.; Berlin, J.A.; Gnpalan, R.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- Cutherberson, D.J.; Shojaee-Moradie, F.; Sprung, V.S.; Jones, H.; Pugh, C.; Richardson, P.; Kemp, G.J.; Barrett, M.; Jackson, N.C.; Thomas, E.L.; et al. Dissociation between exercise-induced reduction in liver fat and changes in hepatic and peripheral glucose homeostasis in obese patients with non-alcoholic fatty liver disease. Clin. Sci. 2016, 130, 93–104. [Google Scholar] [CrossRef]
- Pugh, C.J.; Spring, V.S.; Kemp, G.J.; Richardson, P.; Shojaee-Moradie, F.; Umpleby, A.M.; Green, D.J.; Cable, N.T.; Jones, H.; Cuthbertson, D.J.; et al. Exercise training reverses endothelial dysfunction in nonalcoholic fatty liver disease. Am. J. Physiol. Heart Circ. Physiol. 2014, 307, H1298–H1306. [Google Scholar] [CrossRef]
- Pugh, C.J.; Cuthbertson, D.J.; Sprung, V.S.; Kemp, G.J.; Richardson, P.; Umpleby, A.M.; Green, D.J.; Cable, N.T.; Jones, H. Exercise training improves cutaneous microvascular function in nonalcoholic fatty liver disease. Am. J. Physiol. Endocrinol. Metab. 2013, 305, E50–E58. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.; Kirk, E.P.; Mittendorfer, B.; Patterson, B.W.; Klein, S. Randomized trial of exercise effect on intrahepatic triglyceride content and lipid kinetics in nonalcoholic fatty liver disease. Hepatology 2012, 55, 1738–1745. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.A.; Sachinwalla, T.; Walton, D.W.; Smith, K.; Armstrong, A.; Thompson, M.W.; George, J. Aerobic exercise training reduces hepatic and visceral lipids in obese individuals without weight loss. Hepatology 2009, 50, 1105–1112. [Google Scholar] [CrossRef]
- Hallsworth, K.; Thoma, C.; Hollingsworth, K.G.; Cassidy, S.; Anstee, Q.M.; Day, C.P.; Trenell, M.I. Modified high-intensity interval training reduces liver fat and improves cardiac function in non-alcoholic fatty liver disease: A randomized controlled trial. Clin. Sci. 2015, 129, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.J.; He, J.; Pan, L.L.; Ma, Z.M.; Han, C.K.; Chen, C.S.; Chen, Z.; Han, H.W.; Chen, S.; Sun, Q.; et al. Effects of Moderate and Vigorous Exercise on Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Shamsoddini, A.; Sobhani, V.; Ghamar Chehreh, M.E.; Alavian, S.M.; Zaree, A. Effect of aerobic and resistance exercise training on liver enzymes and hepatic fat in Iranian men with nonalcoholic fatty liver disease. Hepat. Mon. 2015, 15, e31434. [Google Scholar] [CrossRef]
- Draz, R.S.; Serry, Z.; Rahmy, A.F.; El Bardesi, M.S.; Tara, M.M. Electroacupuncture versus aerobic interval training on liver functions in patients with nonalcoholic fatty liver. J. Altern. Complement. Med. 2019, 26, 51–57. [Google Scholar] [CrossRef]
- Shojaee-Moradie, F.; Cuthbertson, D.J.; Barrett, M.; Jackson, N.C.; Herring, R.; Thomas, E.L.; Bell, J.; Kemp, G.J.; Wright, J.; Umpleby, A.M. Exercise training reduces liver fat and increases rates of VLDL clearance but not VLDL production in NAFLD. J. Clin. Endocrinol. Metab. 2016, 101, 4219–4228. [Google Scholar] [CrossRef]
- Abdelbasset, W.K.; Tantawy, S.A.; Kamel, D.M.; Alqahtani, B.A.; Elnegamy, T.E.; Soliman, G.S.; Ibrahim, A.A. Effects of high-intensity interval and moderate-intensity continuous aerobic exercise on diabetic obese patients with nonalcoholic fatty liver disease. A comparative randomized controlled trial. Medicine 2020, 99, 10. [Google Scholar] [CrossRef]
- Rezende, R.E.; Duarte, S.M.; Stefano, J.T.; Roschel, H.; Gualano, B.; de Sa Pinto, A.L.; Vezozzo, D.C.; Carrilho, F.J.; Oliveira, C.P. Randomized clinical trial: Benefits of aerobic physical activity for 24 weeks in postmenopausal women with nonalcoholic fatty liver disease. Menopause 2016, 23, 876–883. [Google Scholar] [CrossRef]
- Eckard, C.; Cole, R.; Lockwood, J.; Torres, D.M.; Williams, C.D.; Shaw, J.C.; Harrison, S.A. Prospective histopathologic evaluation of lifestyle modification in nonalcoholic fatty liver disease: A randomized trial. Therap. Adv. Gastroenterol. 2013, 6, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Houghton, D.; Thoma, C.; Hallsworth, K.; Cassidy, S.; Hardy, T.; Burt, A.D.; Tiniakos, D.; Hollingsworth, K.G.; Taylor, R.; Day, C.P.; et al. Exercise reduces liver lipids and visceral adiposity in patients with nonalcoholic steatohepatitis in a randomized controlled trial. Clin. Gastroenterol. Hepatol. 2017, 15, 96–102. [Google Scholar] [CrossRef]
- Bacchi, E.; Negri, C.; Targher, G.; Faccioli, N.; Lanza, M.; Zoppini, G.; Zanolin, E.; Schena, F.; Bonora, E.; Moghetti, P. Both resistance training and aerobic training reduce hepatic fat content in type 2 diabetic subjects with nonalcoholic fatty liver disease (the RAED2 randomized trial). Hepatology 2013, 58, 1287–1295. [Google Scholar] [CrossRef] [PubMed]
- Keating, S.E.; Adams, L.A. Exercise in NAFLD: Just do it. J. Hepatol. 2016, 65, 671–673. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Wasfy, M.; Baggish, A.L. Exercise dose in clinical practice. Circulation 2016, 133, 2297–2313. [Google Scholar] [CrossRef]
- Colberg Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, e147–e167. [Google Scholar] [CrossRef]
- Keating, S.E.; Hackett, D.A.; Parker, H.M.; O’Connor, H.T.; Gerofi, J.A.; Sainsbury, A. Effect of aerobic exercise training dose on liver fat and visceral adiposity. J. Hepatol. 2015, 63, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Dirk, J.; van der, W.; Vikas, S.; Hongji, Z.; Allan, T.; Hai, H. The Effects of Physical Exercise on Fatty Liver Disease. Gene Expr. 2018, 18, 89–101. [Google Scholar]
- Krasnoff, J.B.; Painter, P.L.; Wallace, J.P.; Bass, N.M.; Merriman, R.B. Health-related fitness and physical activity in patients with nonalcoholic fatty liver disease. Hepatology 2008, 47, 1158–1166. [Google Scholar] [CrossRef]
- Zelber-sagi, S.; Nitzan-Kaluski, D.; Goldsmith, R.; Webb, M.; Zvibel, I.; Goldiner, I. Role of leisure-time physical activity in nonalcoholic fatty liver disease: A population based study. Hepatology 2008, 48, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Finucane, F.M.; Sharp, S.J.; Purslow, L.R.; Horton, K.; Horton, J.; Savage, D.B.; Brage, S.; Besson, H.; De Lucia Rolfe, E.; Sleigh, A. The effects of aerobic exercise on metabolic risk, insulin sensitivity and intrahepatic lipid in healthy older people from the Hertfordshire Cohort Study: A randomised controlled trial. Diabetologia 2010, 53, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Goodpaster, B.H.; Delany, J.P.; Otto, A.D.; Kuller, L.; Vockley, J.; South-Paul, J.E.; Thomas, S.B.; Brown, J.; McTigue, K.; Hames, K.C. Effects of diet and physical activity inter- ventions on weight loss and cardiometabolic risk fac- tors in severely obese adults: A randomized trial. JAMA 2010, 304, 1795–1802. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, S.; Thoma, C.; Hallsworth, K.; Parikh, J.; Hollingsworth, K.G.; Taylor, R.; Jakovljevic, D.G.; Trenell, M.I. High inten- sity intermittent exercise improves cardiac structure and function and reduces liver fat in patients with type 2 diabetes: A randomised controlled trial. Diabetologia 2016, 59, 56–66. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Defined criteria for the current study |
| P (population) | Adult patients with MAFLD |
| I (intervention) | Aerobic exercise |
| C (comparison) | Usual care or another type of intervention |
| O (outcomes) | Primary: changes in serum levels of liver enzymes, intrahepatic triglycerides Secondary: glucose metabolism, anthropometric changes |
| S (study design) | Randomized clinical trials |
| First Author, Year | No of pts | MAFLD Definition | Age Years | BMI kg/m2 | Female/Male | Treatment/ Control | Endpoints | |
|---|---|---|---|---|---|---|---|---|
| TG | CG | |||||||
| Abdelbasset et al., 2019 | 15 | 16 | Ultrasound; Diabetes, Obesity | 54.9 | 36.7 | 7/8 | CAEx/UC | ALT, HOMA2-IR, HOMA-IR, BMI, IHTG |
| Abdelbasset et al., 2019 | 16 | 16 | Ultrasound; Diabetes, Obesity | 54.4 | 36.3 | 6/10 | IEx/UC | ALT, HOMA2-IR, HOMA-IR, BMI, IHTG |
| Bacchi et al., 2013 | 14 | 17 | Diabetes | 55.6 | 30.5 | 56 | CAEx/REx | ALT, AST, GGT, BMI |
| Cuthbertson et al., 2016 | 30 | 20 | 1H MRS (>5.3% IHCL); Obesity | 50.0 | 30.7 | 7/23 | CAEx/UC | ALT, AST, GGT, HOMA2-IR, BMI |
| Draz et al., 2019 | 25 | 25 | Ultrasound; Obesity | 30-55 | 37.8 | 25/0 | IEx/EAc | ALT, AST |
| Eckard et al., 2013 | 9 | 11 | Biopsy; Obesity | 52 | 31.3 | 3/6 | CAEx+REx/UC | ALT, AST |
| Hallsworth et al., 2015 | 12 | 11 | 1H MRS (>5% IHTG); Obesity | 54.0 | 31 | N/R | IEx/UC | ALT, AST, GGT, HOMA2-IR, BMI |
| Houghton et al., 2016 | 12 | 12 | Biopsy; Obesity | 54 | IEx+REx/UC | ALT, AST, GGT, HOMA-IR, BMI, IHTG | ||
| Johnson et al., 2009 | 12 | 7 | 1H MRS; Obesity | 49.1 | N/R | CAEx/St | ALT, HOMA2-IR, HOMA-IR, BMI, IHTG | |
| Pugh et al., 2014 | 34 | 20 | 1H MRS (IHTG >5.5%); Obesity | 48 | 31 | 12/22 | CAEx/UC | ALT, AST, GGT, HOMA2-IR, HOMA-IR, BMI |
| Pugh et al., 2013 | 13 | 7 | 1H MRS (IHTG >5.5%); Obesity | 50 | 31 | 6/7 | CAEx/UC | ALT, AST, GGT, BMI |
| Rezende et al., 2016 | 19 | 21 | Biopsy; Obesity | 56.2 | 34.1 | 19/0 | CAEx/UC | ALT, AST, GGT, HOMA-IR, BMI |
| Shamsoddini et al., 2015 | 10 | 10 | Ultrasound; Overweight | 39.7 | 28.1 | 0/10 | CAEx/UC | ALT, AST, HOMA-IR, BMI |
| Shojaee-Moradie et al., 2016 | 15 | 12 | Ultrasound or liver biopsy; Obesity | 52.4 | 31.6 | 0/15 | CAEx+REx/UC | ALT, AST, GGT, BMI |
| Sullivan et al., 2012 | 12 | 6 | 1H MRS (IHTG >10%); Obesity | 48.6 | 37.1 | 8/4 | CAEx/UC | ALT, BMI |
| Zhang et al., 2016 (a) | 66 | 73 | Ultrasound, 1H MRS (>5% IHTG); Overweight | 53.2 | 27.9 | 52/14 | CAEx/UC | ALT, AST, IHTG |
| Zhang et al., 2016 (b) | 69 | 73 | Ultrasound, 1H MRS (>5% IHTG); Overweight | 54.4 | 28.1 | 51/18 | CAEx/UC | ALT, AST, IHTG |
| Frequency | Intensity | Type | Time | Progression | Duration | Volume | ACSM Criteria Met * ? | |
|---|---|---|---|---|---|---|---|---|
| Abdelbasset et al., 2019 | 3 d per week | 60–70% HRmax | Continuous training, Three phases: warm-up, training and cool down; Cycle ergometer | 8 weeks | None | 40–50 min | 120–150 min/week | No |
| Abdelbasset et al., 2019 | 3 d per week | 50–85% VO2max | Interval training, Three phases: warm-up, training and cool down; Cycle ergometer | 8 weeks | None | 40 min | 120 min/week | Progressively yes |
| Bacchi et al., 2013 | 3 d per week | 60–65% HRR | Continuous training, Cycle, treadmill; CG: resistance training | 16 weeks | None | 60 min | 180 min/week | No |
| Cuthbertson et al., 2016 | 3–5 d per week | 3 weeks 30% HRR; 5 week at 60% HRR by week 12 | Continuous training, Treadmill, cross-trainer, cycle ergometer, rower | 16 weeks | Duration, frequency, intensity | 30–45 min | 90–225 min/week | Progressively yes |
| Draz et al., 2019 | 3 d per week | 60–85% HRmax | Interval training, Three phases: warm-up, training and cool down; Cycle ergometer, CG: electroacupuncture | 6 weeks | None | 30 min | 90 min/week | Progressively yes |
| Eckard et al., 2013 | 4–7 d per week | N/A | Combination training, Cycle, Treadmill, resistance training | 24 weeks | Frequency, intensity, time | 20–60 min | 80–420 min/week | No |
| Hallsworth et al., 2015 | 3 d per week | 6–20 point Borg rating of perceived exertion (RPE) | Interval training, Three phases: warm-up, training and cool down; Cycle ergometer | 12 weeks | None | 30–40 min | 90–120 min/week | Yes |
| Houghton et al., 2016 | 3 d per week | 6–20 point Borg rating of perceived exertion (RPE) | Combination training, Cycling intervals, resistance exercise | 12 weeks | None | 45–60 min | 180 min/week | No |
| Johnson et al., 2009 | 3 d per week | 50% VO2peak for week 1, 60% for week 2, and 70% for weeks 3 and 4. | Continuous training, Cycle ergometer; CG: stretching 3 d per wk. | 4 weeks | Intensity | 30–45 min | 120–180 min/week | Yes |
| Pugh et al., 2014 | 3–5 d per week | 3 wks 30% HRR; from 4 wk 45% HRR; from 12 wk 60% HRR. | Continuous training, Treadmill, cycle ergometer | 16 weeks | Duration, frequency, intensity | 30–45 min | 90–225 min/week | Progressively yes |
| Pugh et al., 2013 | 3–5 d per week | From 1 wk 30% HRR to 60% HRR by 12 wk | Continuous training, Treadmill | 16 weeks | Duration, frequency, intensity | 30–45 min | 90–225 min/week | Progressively yes |
| Rezende et al., 2016 | 2 d per week | From VAT up to 10% below RCP | Continuous training, Three phases: warm-up, training and cool down; Treadmill | 24 weeks | Duration | 40–60 min | 80–120 min/week | No |
| Shamsoddini et al., 2015 | 3 d per week | From 1 wk 60% HRmax to 75% HRmax by the final wk. | Continuous training, Three phases: warm-up, training and cool down; treadmill | 8 weeks | Intensity | 45 min | 135 min/week | No |
| Shojaee-Moradie et al., 2016 | 4–5 d per week | 40–60 HRR | Combination training, outdoor aerobic activities, resistance exercise | 16 weeks | Duration | 20–60 min | 80–300 min/week | Progressively yes |
| Sullivan et al., 2012 | 5 d per week | 45–55% VO2peak | Continuous training, Treadmill | 16 weeks | Duration | 30–60 min | 150–300 min/week | Yes |
| Zhang et al., 2016 (a) | 5 d per week | 6 mo 65–80% HRmax; | Continuous training, Treadmill | 24 weeks | Intensity | 30 min | 150 min/week | Yes |
| Zhang et al., 2016 (b) | 5 d per week | 45–55% HRmax | Continuous training, Treadmill | 24 weeks | None | 30 min | 150 min/week | Yes |
| Outcomes | MD | 95% CI | p-Value | I2 |
|---|---|---|---|---|
| ALT (U/L) | −0.87 | −2.57, 0.81 | 0.31 | 33.9 |
| ALT (U/L) * | −2.4 | −4.34, −0.46 | 0.01 | 9.1 |
| AST (U/L) | 0.02 | −1.09, 1.13 | 0.97 | 35.7 |
| GGT (U/L) | −0.73 | −3.82, 2.36 | 0.64 | 0 |
| IHTG (%) | −4.05 | −5.37, −2.74 | <0.0001 | 0 |
| HOMA2-IR | −0.06 | −0.73, 0.61 | 0.85 | 71.7 |
| HOMA-IR | −0.28 | −0.88, 0.31 | 0.35 | 12.7 |
| BMI (kg/m2) | −0.97 | −1.40, −0.55 | <0.0001 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Słomko, J.; Zalewska, M.; Niemiro, W.; Kujawski, S.; Słupski, M.; Januszko-Giergielewicz, B.; Zawadka-Kunikowska, M.; Newton, J.; Hodges, L.; Kubica, J.; et al. Evidence-Based Aerobic Exercise Training in Metabolic-Associated Fatty Liver Disease: Systematic Review with Meta-Analysis. J. Clin. Med. 2021, 10, 1659. https://doi.org/10.3390/jcm10081659
Słomko J, Zalewska M, Niemiro W, Kujawski S, Słupski M, Januszko-Giergielewicz B, Zawadka-Kunikowska M, Newton J, Hodges L, Kubica J, et al. Evidence-Based Aerobic Exercise Training in Metabolic-Associated Fatty Liver Disease: Systematic Review with Meta-Analysis. Journal of Clinical Medicine. 2021; 10(8):1659. https://doi.org/10.3390/jcm10081659
Chicago/Turabian StyleSłomko, Joanna, Marta Zalewska, Wojciech Niemiro, Sławomir Kujawski, Maciej Słupski, Beata Januszko-Giergielewicz, Monika Zawadka-Kunikowska, Julia Newton, Lynette Hodges, Jacek Kubica, and et al. 2021. "Evidence-Based Aerobic Exercise Training in Metabolic-Associated Fatty Liver Disease: Systematic Review with Meta-Analysis" Journal of Clinical Medicine 10, no. 8: 1659. https://doi.org/10.3390/jcm10081659
APA StyleSłomko, J., Zalewska, M., Niemiro, W., Kujawski, S., Słupski, M., Januszko-Giergielewicz, B., Zawadka-Kunikowska, M., Newton, J., Hodges, L., Kubica, J., & Zalewski, P. (2021). Evidence-Based Aerobic Exercise Training in Metabolic-Associated Fatty Liver Disease: Systematic Review with Meta-Analysis. Journal of Clinical Medicine, 10(8), 1659. https://doi.org/10.3390/jcm10081659