
Effect of Growth Factor-Loaded Acellular Dermal Matrix/MSCs on Regeneration of Chronic Tympanic Membrane Perforations in Rats

 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. In Vitro Study
2.1.1. Cell Culture and Treatment
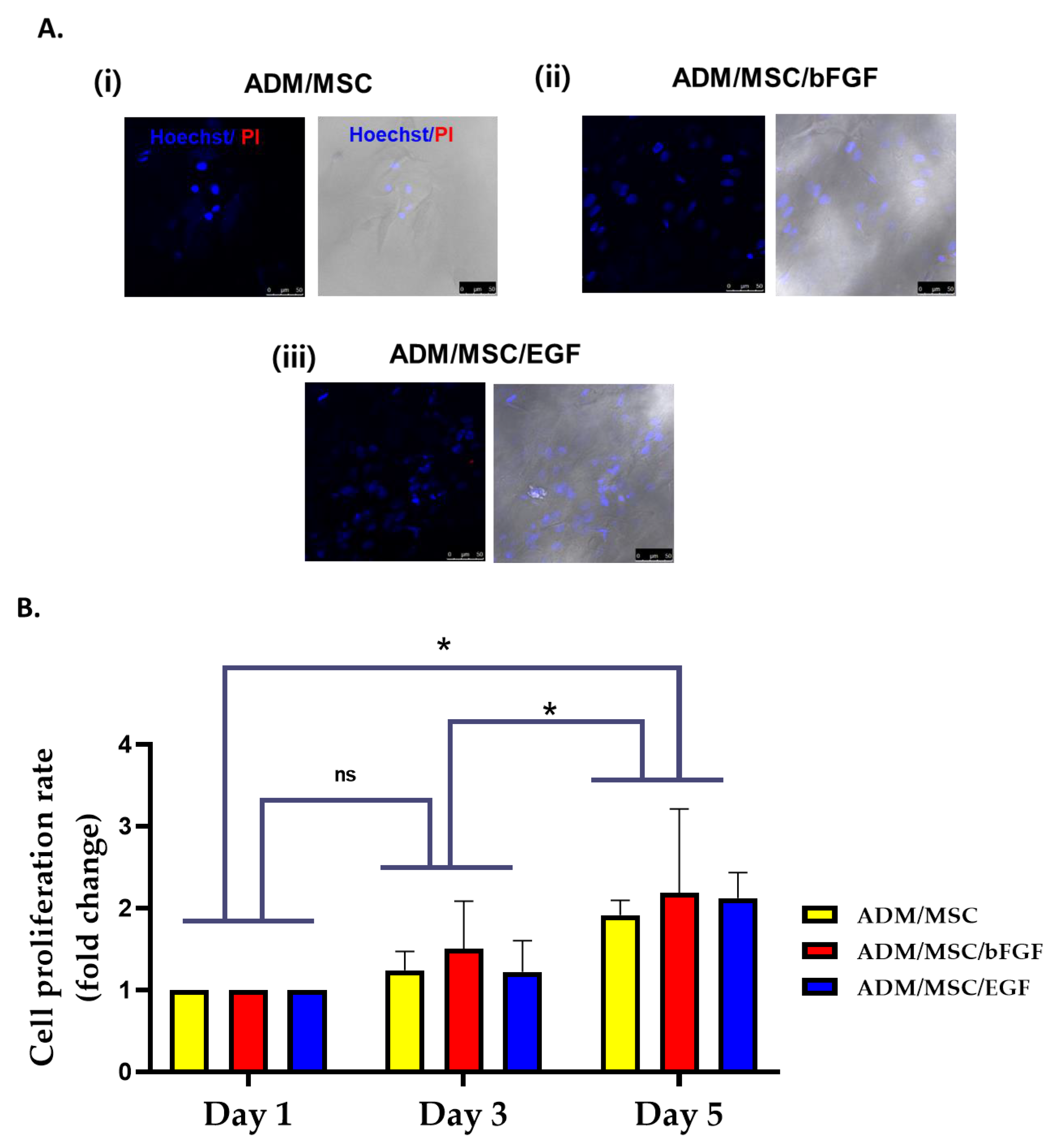
2.1.2. Live and Dead Cell Staining
2.1.3. Cell Viability Assay
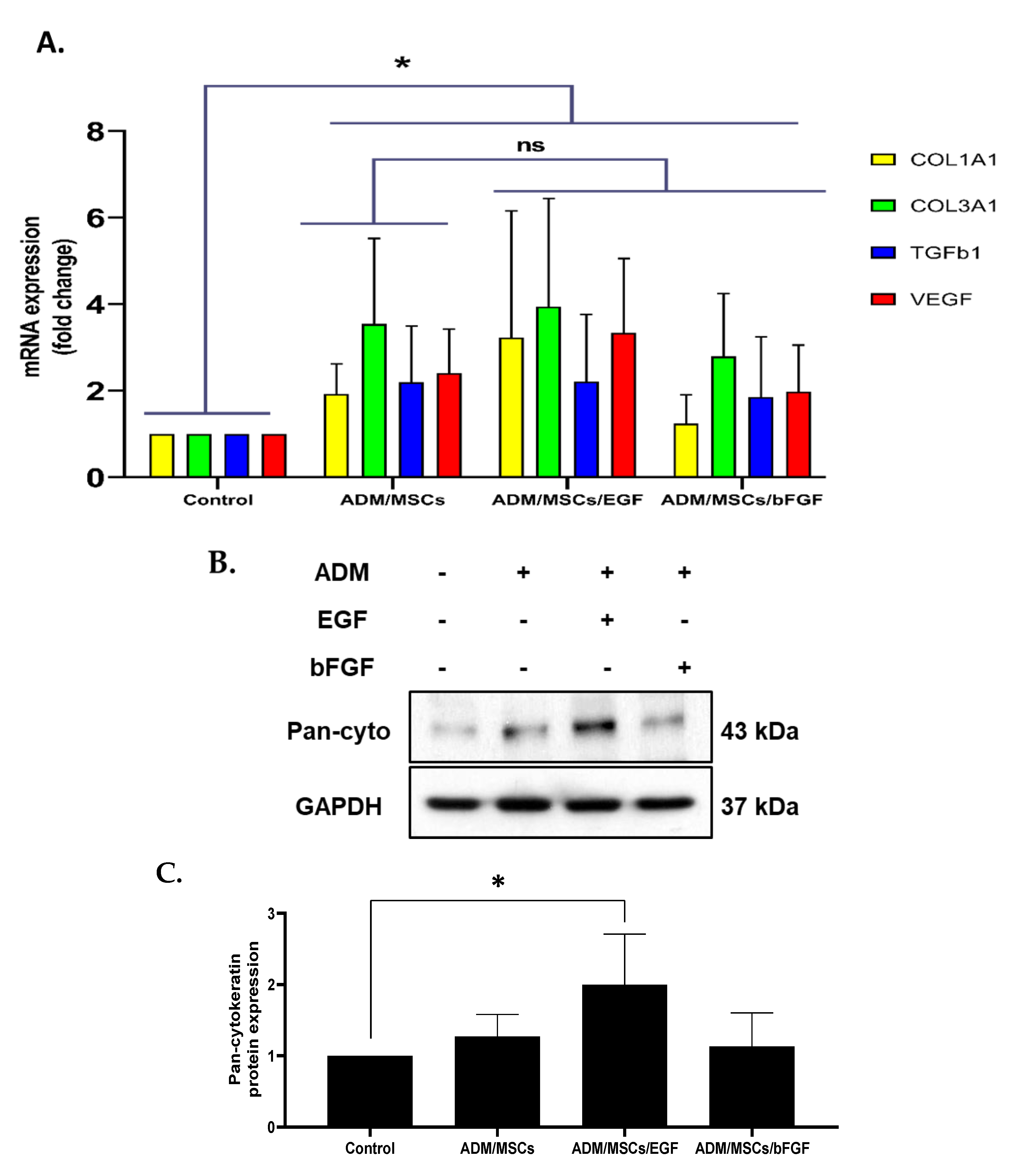
2.1.4. Real-Time PCR (Quantitative PCR)
2.1.5. Immunoblot Analysis
2.2. In Vivo Study
2.2.1. Creation of Chronic TMP
2.2.2. Scaffold Preparation
2.2.3. Application of Scaffold
2.2.4. Otoendoscopic Examination
2.2.5. Histopathological Examination
2.2.6. Immunohistochemistry of Ki-67 in the Rat Tympanic Membrane
2.3. Statistical Analysis
3. Results
3.1. In Vitro Study
3.2. In Vivo Study
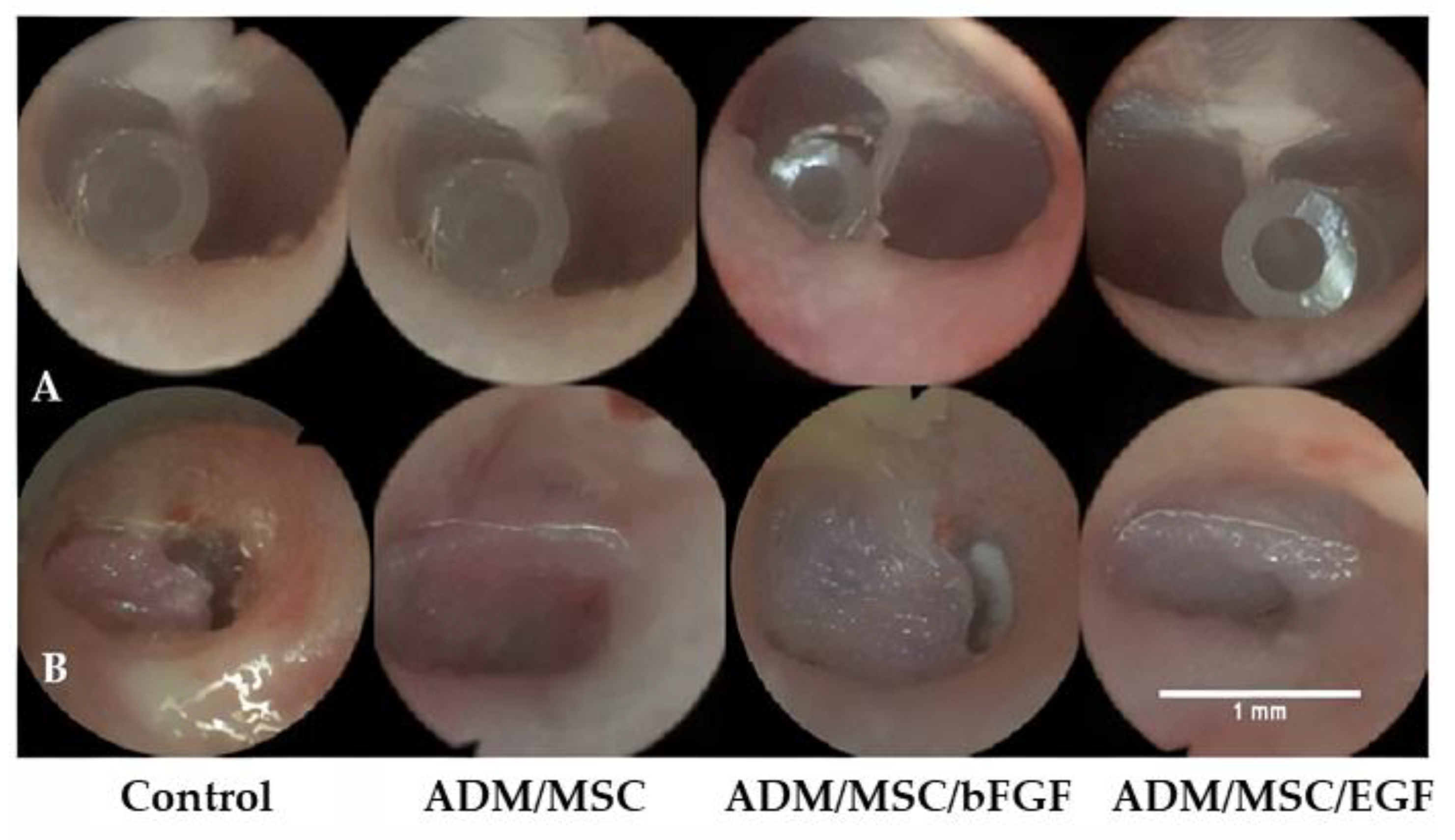
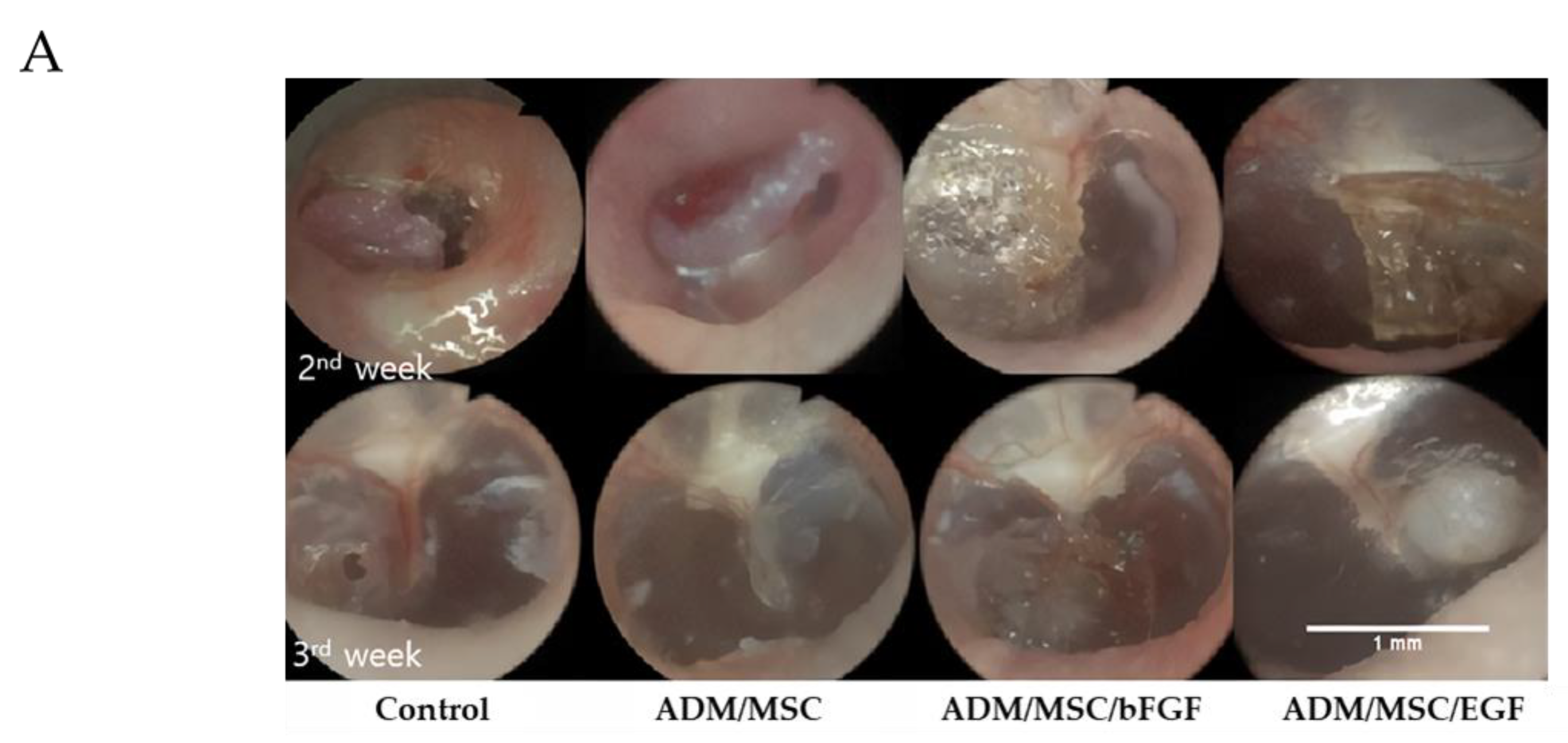
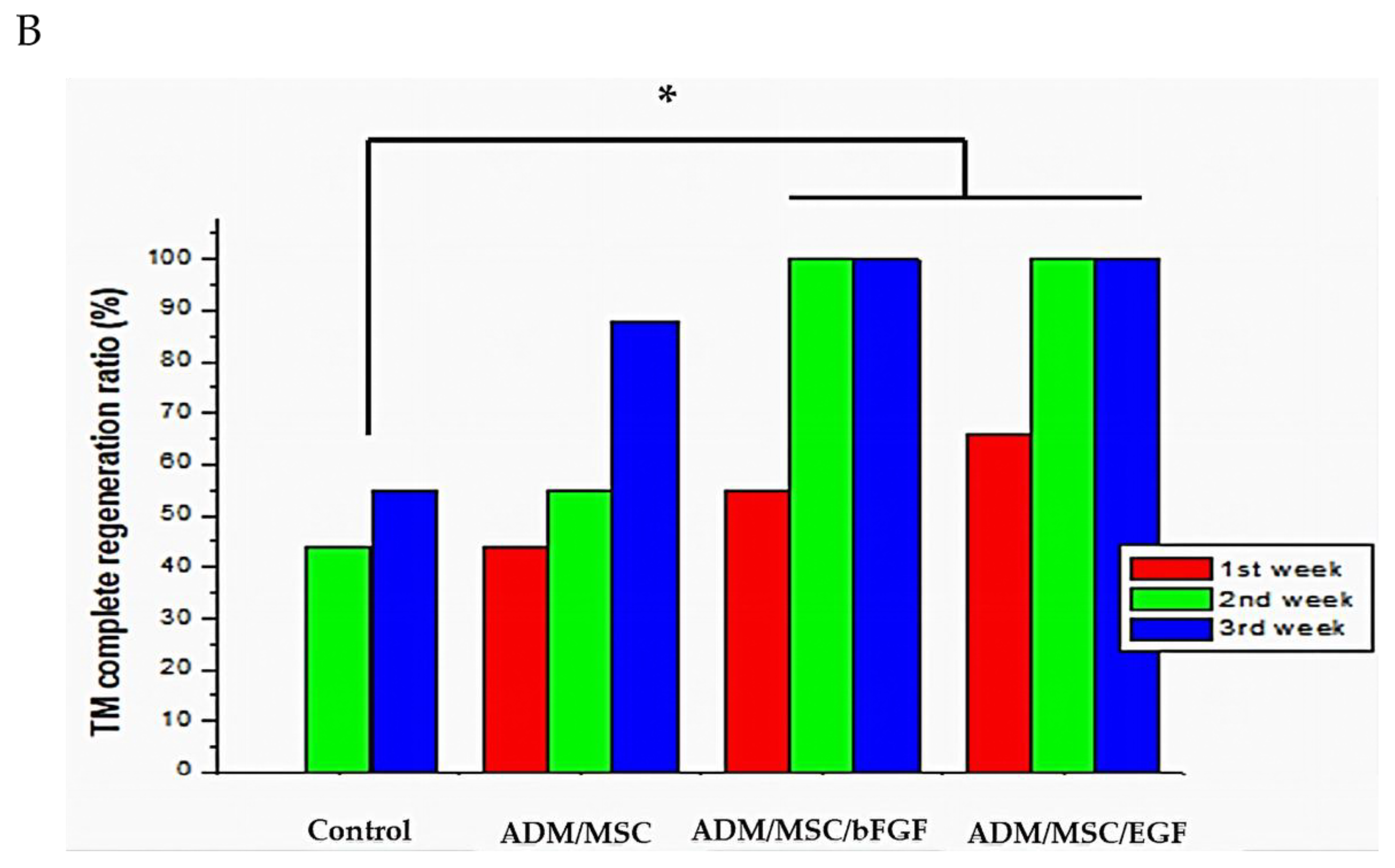
3.2.1. Otoendoscopic Examination
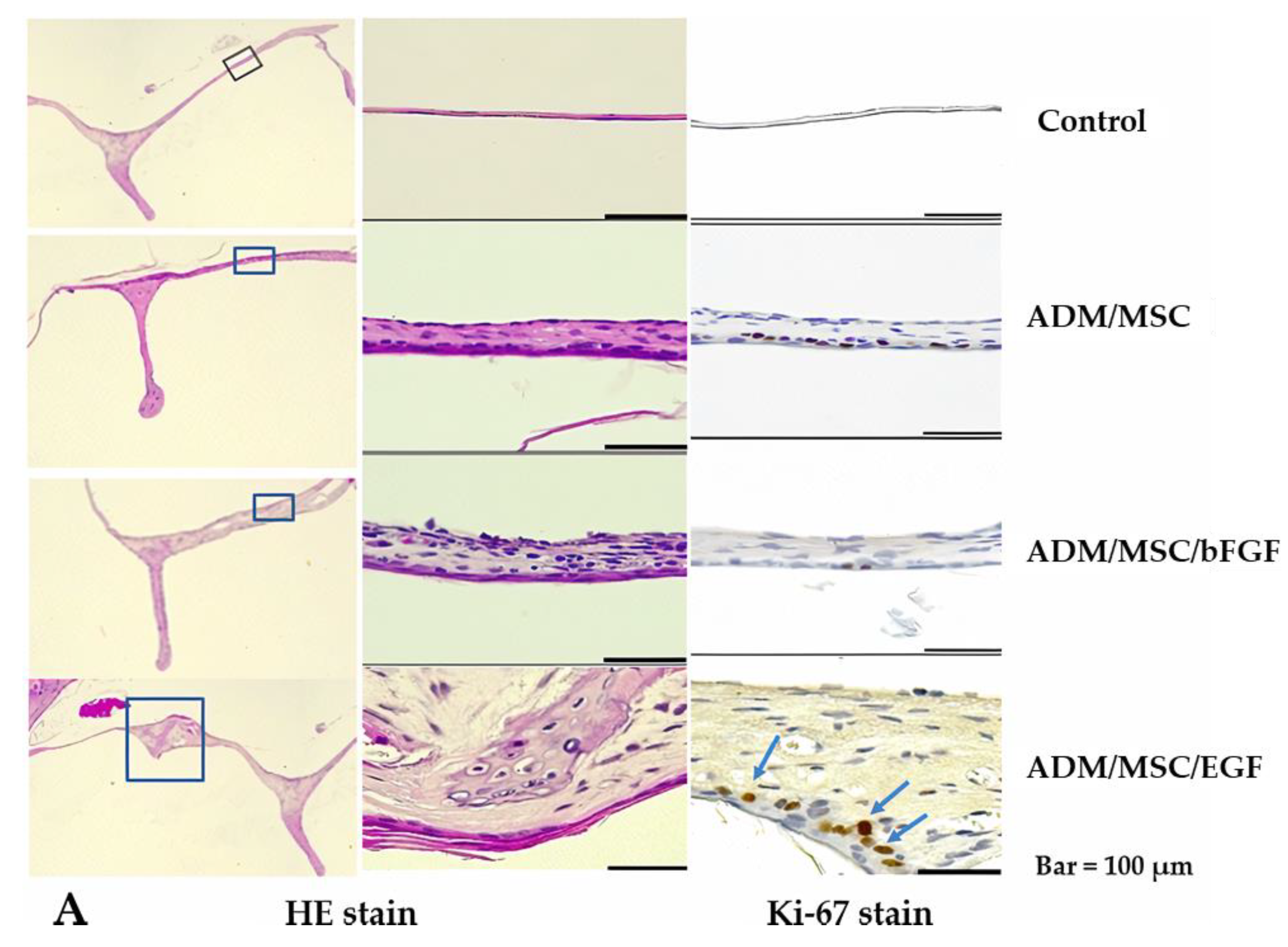
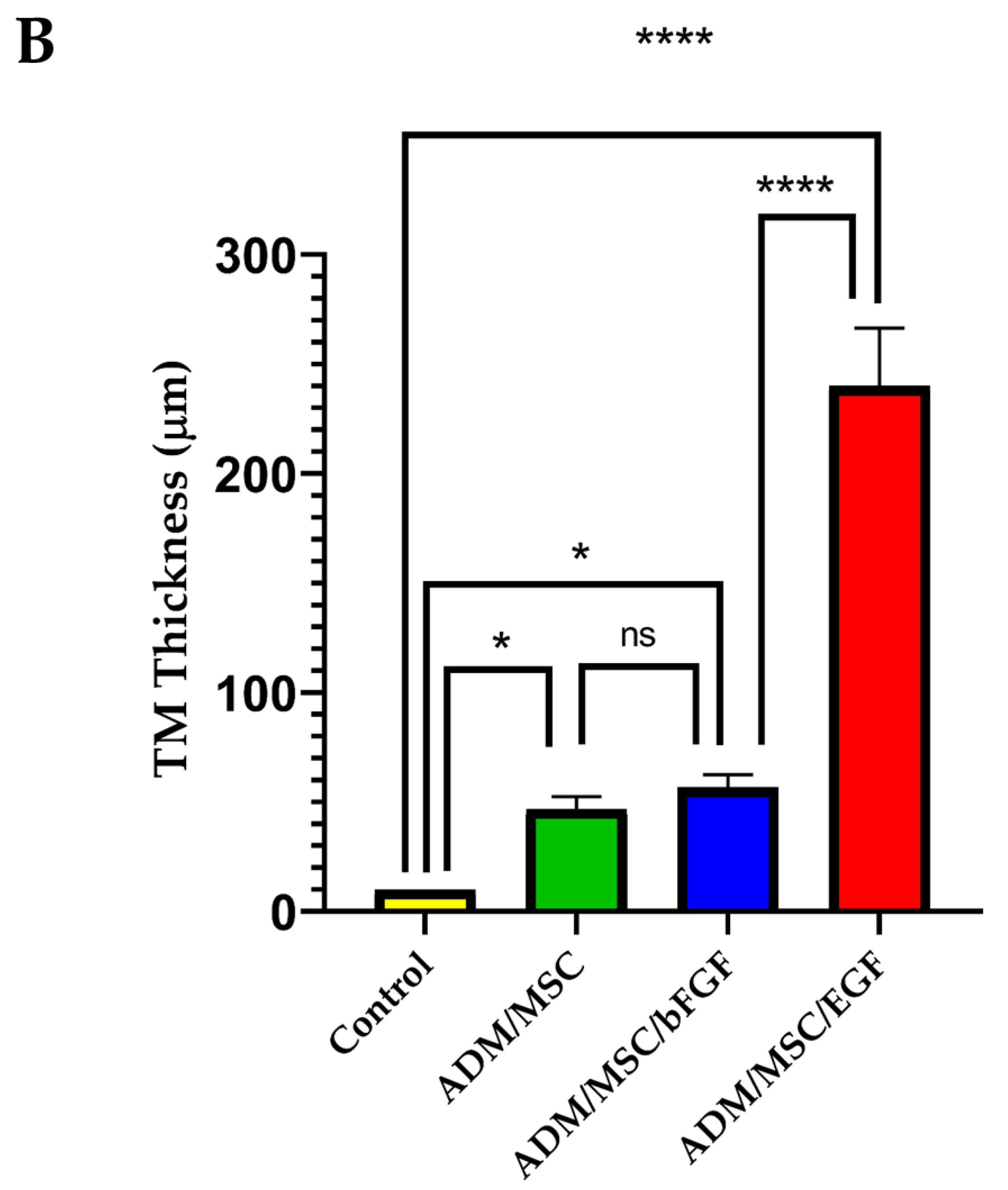
3.2.2. Histological Results
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shiomi, Y.; Shiomi, Y. Surgical outcomes of myringoplasty using platelet-rich plasma and evaluation of the outcome-associated factors. Auris Nasus Larynx 2020, 47, 191–197. [Google Scholar] [CrossRef]
- Lou, Z. Comparison of bilateral same-day and sequential endoscopic cartilage myringoplasty for bilateral chronic tympanic membrane perforation. Acta Oto Laryngol. 2020, 140, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Bhat, V.K.; Ajur, S.; Bongale, K.R.; Sachidananda, R. Prevention of Craniofacial Pain Secondary to Harvesting of Temporalis Fascia—A Novel Technique. J. Int. Adv. Otol. 2019, 15, 405–408. [Google Scholar] [CrossRef]
- Aleemardani, M.; Bagher, Z.; Farhadi, M.; Chahsetareh, H.; Najafi, R.; Eftekhari, B.; Seifalian, A.M. Can tissue engineering bring hope in the development of human tympanic membrane? Tissue Eng. 2020. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Teh, B.M.; Li, H.; Hu, Y.; Huang, J.; Lv, C.; Bu, S.; Zheng, M.; Shen, Y. Acellular Collagen Scaffold With Basic Fibroblast Growth Factor for Repair of Traumatic Tympanic Membrane Perforation in a Rat Model. Otolaryngol. Head Neck Surg. 2020, 164, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Santa Maria, P.L. A design-thinking approach to therapeutic translation: Tympanic regeneration. Curr. Opin. Otolaryngol. Head Neck Surg. 2020, 28, 274–280. [Google Scholar] [CrossRef]
- Ilhan, E.; Ulag, S.; Sahin, A.; Yilmaz, B.K.; Ekren, N.; Kilic, O.; Sengor, M.; Kalaskar, D.M.; Oktar, F.N.; Gunduz, O. Fabrication of tissue-engineered tympanic membrane patches using 3D-Printing technology. J. Mech. Behav. Biomed. Mater. 2021, 114, 104219. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Huo, Z.; Zhang, H.; Hu, Q.; Ramalingam, M. 3D printing-assisted combinatorial approach for designing mechanically-tunable and vascular supportive nanofibrous membranes to repair perforated eardrum. J. Appl. Polym. Sci. 2021, 138, 50132. [Google Scholar] [CrossRef]
- Hussain, Z.; Pei, R. Necessities, opportunities, and challenges for tympanic membrane perforation scaffolding-based bioengineering. Biomed. Mater. 2021, 16, 032004. [Google Scholar] [CrossRef]
- Mandour, Y.M.H.; Mohammed, S.; Menem, M.A. Bacterial cellulose graft versus fat graft in closure of tympanic membrane perforation. Am. J. Otolaryngol. 2019, 40, 168–172. [Google Scholar] [CrossRef]
- Ersözlü, T.; Gultekin, E. A comparison of the autologous platelet-rich plasma gel fat graft myringoplasty and the fat graft myringoplasty for the closure of different sizes of tympanic membrane perforations. Ear Nose Throat J. 2020, 99, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Seo, Y.J.; Shim, D.B.; Lee, H.J.; Kim, S.H. Surgical outcomes of tympanoplasty using a sterile acellular dermal allograft: A prospective randomised controlled study. Acta Otorhinolaryngol. Ital. Organo Uff. Della Soc. Ital. Di Otorinolaringol. E Chir. Cervico Facciale 2018, 38, 554–562. [Google Scholar] [CrossRef]
- Lewis, R.E.; Towery, E.A.; Bhat, S.G.; Ward, A.J.; Heidel, R.E.; Bielak, K.M.; Simpson, H.E.; McLoughlin, J.M.; Lewis, J.M. Human Acellular Dermal Matrix Is a Viable Alternative to Autologous Skin Graft in Patients with Cutaneous Malignancy. Am. Surg. 2019, 85, 1056–1060. [Google Scholar] [CrossRef] [PubMed]
- Laidlaw, D.W.; Costantino, P.D.; Govindaraj, S.; Hiltzik, D.H.; Catalano, P.J. Tympanic membrane repair with a dermal allograft. Laryngoscope 2001, 111, 702–707. [Google Scholar] [CrossRef]
- McFeely Jr, W.J.; Bojrab, D.I.; Kartush, J.M. Tympanic membrane perforation repair using AlloDerm. Otolaryngol. Head Neck Surg. 2000, 123, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Lou, Z.; Fu, Y. Effect of Basic Fibroblast Growth Factor in Tympanic Membrane Perforation. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 920–921. [Google Scholar] [CrossRef]
- Röösli, C.; von Büren, T.; Gassmann, N.B.; Huber, A.M. The impact of platelet-derived growth factor on closure of chronic tympanic membrane perforations: A randomized, double-blind, placebo-controlled study. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2011, 32, 1224–1229. [Google Scholar] [CrossRef]
- Lou, Z.C.; Lou, Z.H.; Xiao, J. Regeneration of the tympanic membrane using fibroblast growth factor-2. J. Laryngol. Otol. 2018, 132, 470–478. [Google Scholar] [CrossRef]
- Santa Maria, P.L.; Gottlieb, P.; Santa Maria, C.; Kim, S.; Puria, S.; Yang, Y.P. Functional Outcomes of Heparin-Binding Epidermal Growth Factor-Like Growth Factor for Regeneration of Chronic Tympanic Membrane Perforations in Mice. Tissue Eng. Part A 2017, 23, 436–444. [Google Scholar] [CrossRef]
- Santa Maria, P.L.; Weierich, K.; Kim, S.; Yang, Y.P. Heparin Binding Epidermal Growth Factor-Like Growth Factor Heals Chronic Tympanic Membrane Perforations With Advantage Over Fibroblast Growth Factor 2 and Epidermal Growth Factor in an Animal Model. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2015, 36, 1279–1283. [Google Scholar] [CrossRef]
- Amoils, C.P.; Jackler, R.K.; Lustig, L.R. Repair of chronic tympanic membrane perforations using epidermal growth factor. Otolaryngol. Head Neck Surg. Off. J. Am. Acad. Otolaryngol. Head Neck Surg. 1992, 107, 669–683. [Google Scholar] [CrossRef]
- Huang, J.; Teh, B.M.; Eikelboom, R.H.; Han, L.; Xu, G.; Yao, X.; Hu, Y.; Zheng, M.; Shen, Y. The effectiveness of bFGF in the treatment of tympanic membrane perforations: A systematic review and meta-analysis. Otol. Neurotol. 2020, 41, 782. [Google Scholar] [CrossRef]
- Seonwoo, H.; Shin, B.; Jang, K.J.; Lee, M.; Choo, O.S.; Park, S.B.; Kim, Y.C.; Choi, M.J.; Kim, J.; Garg, P. Epidermal growth factor–releasing radially aligned electrospun nanofibrous patches for the regeneration of chronic tympanic membrane perforations. Adv. Healthc. Mater. 2019, 8, 1801160. [Google Scholar] [CrossRef]
- Goncalves, S.; Bas, E.; Langston, M.; Grobman, A.; Goldstein, B.J.; Angeli, S. Histologic changes of mesenchymal stem cell repair of tympanic membrane perforation. Acta Oto Laryngol. 2017, 137, 411–416. [Google Scholar] [CrossRef]
- Mittal, R.; Jung, H.D.; Mittal, J.; Eshraghi, A.A. A perspective on stem cell therapy for ear disorders. J. Cell. Physiol. 2018, 233, 1823–1824. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Olivius, P.; Dirckx, J.; Von Unge, M.; Hultcrantz, M. Stem cells and enhanced healing of chronic tympanic membrane perforation. Acta Oto Laryngol. 2008, 128, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Ong, H.T.; Redmond, S.L.; Marano, R.J.; Atlas, M.D.; von Unge, M.; Aabel, P.; Dilley, R.J. Paracrine activity from adipose-derived stem cells on in vitro wound healing in human tympanic membrane keratinocytes. Stem Cells Dev. 2017, 26, 405–418. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.M.; Wu, L.A.; Zhang, M.; Zhang, R.; Sun, H.H. Homing of endogenous stem/progenitor cells for in situ tissue regeneration: Promises, strategies, and translational perspectives. Biomaterials 2011, 32, 3189–3209. [Google Scholar] [CrossRef]
- Hakuba, N.; Hato, N.; Okada, M.; Mise, K.; Gyo, K. Preoperative factors affecting tympanic membrane regeneration therapy using an atelocollagen and basic fibroblast growth factor. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 60–66. [Google Scholar] [CrossRef]
- Hakuba, N.; Iwanaga, M.; Tanaka, S.; Hiratsuka, Y.; Kumabe, Y.; Konishi, M.; Okanoue, Y.; Hiwatashi, N.; Wada, T. Basic fibroblast growth factor combined with atelocollagen for closing chronic tympanic membrane perforations in 87 patients. Otol. Neurotol. 2010, 31, 118–121. [Google Scholar] [CrossRef]
- Wang, A.Y.; Liew, L.J.; Shen, Y.; Wang, J.T.; von Unge, M.; Atlas, M.D.; Dilley, R.J. Rat model of chronic tympanic membrane perforation: A longitudinal histological evaluation of underlying mechanisms. Int. J. Pediatr. Otorhinolaryngol. 2017, 93, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.Y.; Shen, Y.; Liew, L.J.; Wang, J.T.; von Unge, M.; Atlas, M.D.; Dilley, R.J. Searching for a rat model of chronic tympanic membrane perforation: Healing delayed by mitomycin C/dexamethasone but not paper implantation or iterative myringotomy. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1240–1247. [Google Scholar] [CrossRef] [PubMed]
- Ten Cate, W.J.; Curtis, L.; Rarey, K.; Small, G. Localization of glucocorticoid receptors and glucocorticoid receptor mRNAs in the rat cochlea. Laryngoscope 1993, 103, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, A.D.; Ferguson, M.W. Tissue engineering of replacement skin: The crossroads of biomaterials, wound healing, embryonic development, stem cells and regeneration. J. R. Soc. Interface 2007, 4, 413–437. [Google Scholar] [CrossRef] [PubMed]
- Giles, B. Wound healing in spontaneous perforation or myringotomy and middle ear reconstruction. Ear Nose Throat J. 2007, 86, 30–32. [Google Scholar] [CrossRef]
- Masutani, H.; Nakai, Y.; Sugita, M.; Ohashi, K.; Moriguchi, M.; Matsunaga, K. Microvasculature of the tympanic membrane. Acta Oto Laryngol. 1991, 111, 99–104. [Google Scholar] [CrossRef]
- Chen, L.; Tredget, E.E.; Wu, P.Y.; Wu, Y. Paracrine factors of mesenchymal stem cells recruit macrophages and endothelial lineage cells and enhance wound healing. PLoS ONE 2008, 3, e1886. [Google Scholar] [CrossRef]
- Goncalves, S.; Bas, E.; Goldstein, B.J.; Angeli, S. Effects of cell-based therapy for treating tympanic membrane perforations in mice. Otolaryngol. Head Neck Surg. 2016, 154, 1106–1114. [Google Scholar] [CrossRef]
- Duscher, D.; Barrera, J.; Wong, V.W.; Maan, Z.N.; Whittam, A.J.; Januszyk, M.; Gurtner, G.C. Stem cells in wound healing: The future of regenerative medicine? A mini-review. Gerontology 2016, 62, 216–225. [Google Scholar] [CrossRef]
- Ramsay, H.A.; Heikkonen, E.J.; Laurila, P.K. Effect of epidermal growth factor on tympanic membranes with chronic perforations: A clinical trial. Otolaryngol. Head Neck Surg. 1995, 113, 375–379. [Google Scholar] [CrossRef]
- Lou, Z.; Yang, J.; Tang, Y.; Fu, Y. Topical application of epidermal growth factor with no scaffold material on the healing of human traumatic tympanic membrane perforations. Clin. Otolaryngol. 2016, 41, 744–749. [Google Scholar] [CrossRef] [PubMed]
- Lou, Z.-C.; Dong, Y.; Lou, Z.-H. Comparative study of epidermal growth factor and observation only on human subacute tympanic membrane perforation. Am. J. Otolaryngol. 2019, 40, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Kanemaru, S.-I.; Umeda, H.; Kitani, Y.; Nakamura, T.; Hirano, S.; Ito, J. Regenerative treatment for tympanic membrane perforation. Otol. Neurotol. 2011, 32, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Santa Maria, P.L.; Redmond, S.L.; Atlas, M.D.; Ghassemifar, R. The role of epidermal growth factor in the healing tympanic membrane following perforation in rats. J. Mol. Histol. 2010, 41, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Dolhi, N.; Weimer, A.D. Tympanic Membrane Perforations. In Statpearls; 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557887/ (accessed on 6 May 2020).
- Makuszewska, M.; Bonda, T.; Cieślińska, M.; Bialuk, I.; Winnicka, M.; Niemczyk, K. Expression of collagen type III in healing tympanic membrane. Int. J. Pediatr. Otorhinolaryngol. 2020, 136, 110196. [Google Scholar] [CrossRef]
- Mozaffari, M.; Jiang, D.; Tucker, A.S. Developmental aspects of the tympanic membrane: Shedding light on function and disease. Genesis 2020, 58, e23348. [Google Scholar] [CrossRef]
- Jang, C.H.; Ahn, S.; Lee, J.W.; Lee, B.H.; Lee, H.; Kim, G. Mesenchymal stem cell-laden hybrid scaffold for regenerating subacute tympanic membrane perforation. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 72, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Jang, C.H.; Cho, Y.B.; Yeo, M.; Lee, H.; Min, E.J.; Lee, B.H.; Kim, G.H. Regeneration of chronic tympanic membrane perforation using 3D collagen with topical umbilical cord serum. Int. J. Biol. Macromol. 2013, 62, 232–240. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Sequence (5′–3′) |
|---|---|
| COL1A1 | CTGGAAGAGTGGAGAGTACTGG GGAATCCATCGGTCATGCTCT |
| COL3A1 | GAAAGAGGATCTGAGGGCTC CTCCATAATACGGGGCAAAACC |
| TGFβ1 | CAAGTGGACATCAACGGGTTC TCCGTGGAGCTGAAGCAATAG |
| VEGF | CTACCTCCACCATGCCAAGTG GCAGTAGCTGCGCTGATAGAC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, G.-W.; Moon, C.; Song, A.; Vijayakumar, K.A.; Ang, M.J.; Jang, C.H. Effect of Growth Factor-Loaded Acellular Dermal Matrix/MSCs on Regeneration of Chronic Tympanic Membrane Perforations in Rats. J. Clin. Med. 2021, 10, 1541. https://doi.org/10.3390/jcm10071541
Cho G-W, Moon C, Song A, Vijayakumar KA, Ang MJ, Jang CH. Effect of Growth Factor-Loaded Acellular Dermal Matrix/MSCs on Regeneration of Chronic Tympanic Membrane Perforations in Rats. Journal of Clinical Medicine. 2021; 10(7):1541. https://doi.org/10.3390/jcm10071541
Chicago/Turabian StyleCho, Gwang-Won, Changjong Moon, Anji Song, Karthikeyan A. Vijayakumar, Mary Jasmin Ang, and Chul Ho Jang. 2021. "Effect of Growth Factor-Loaded Acellular Dermal Matrix/MSCs on Regeneration of Chronic Tympanic Membrane Perforations in Rats" Journal of Clinical Medicine 10, no. 7: 1541. https://doi.org/10.3390/jcm10071541
APA StyleCho, G.-W., Moon, C., Song, A., Vijayakumar, K. A., Ang, M. J., & Jang, C. H. (2021). Effect of Growth Factor-Loaded Acellular Dermal Matrix/MSCs on Regeneration of Chronic Tympanic Membrane Perforations in Rats. Journal of Clinical Medicine, 10(7), 1541. https://doi.org/10.3390/jcm10071541