
Extracorporeal Membrane Oxygenation for Fulminant Myocarditis: Increase of Cardiac Enzyme and SOFA Score Is Associated with High Mortality

 ,
,
Abstract
1. Introduction
2. Materials and Methods
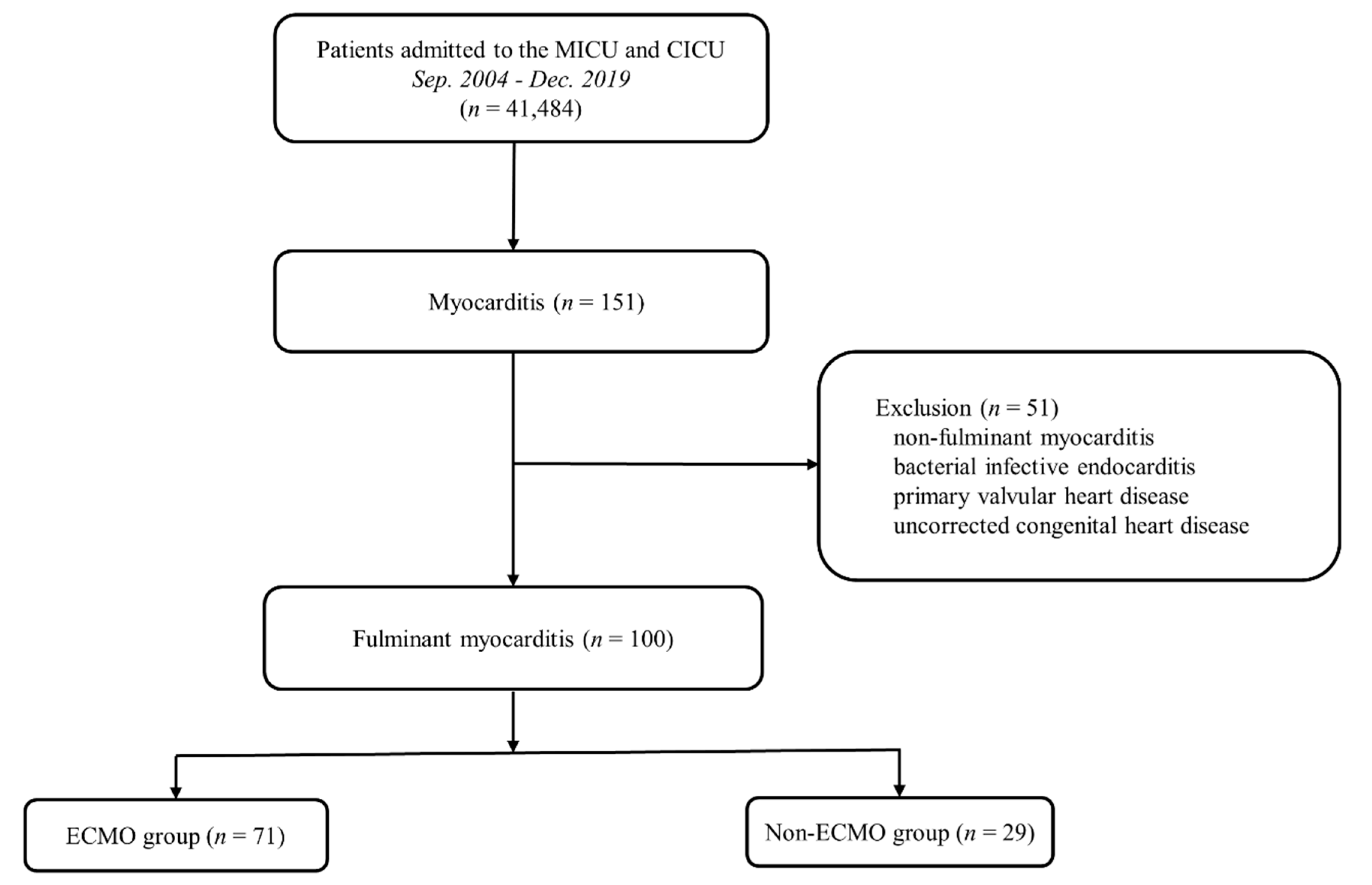
2.1. Study Population
2.2. Definitions and Outcomes
2.3. Statistical Analyses
3. Results
3.1. Baseline Characteristics
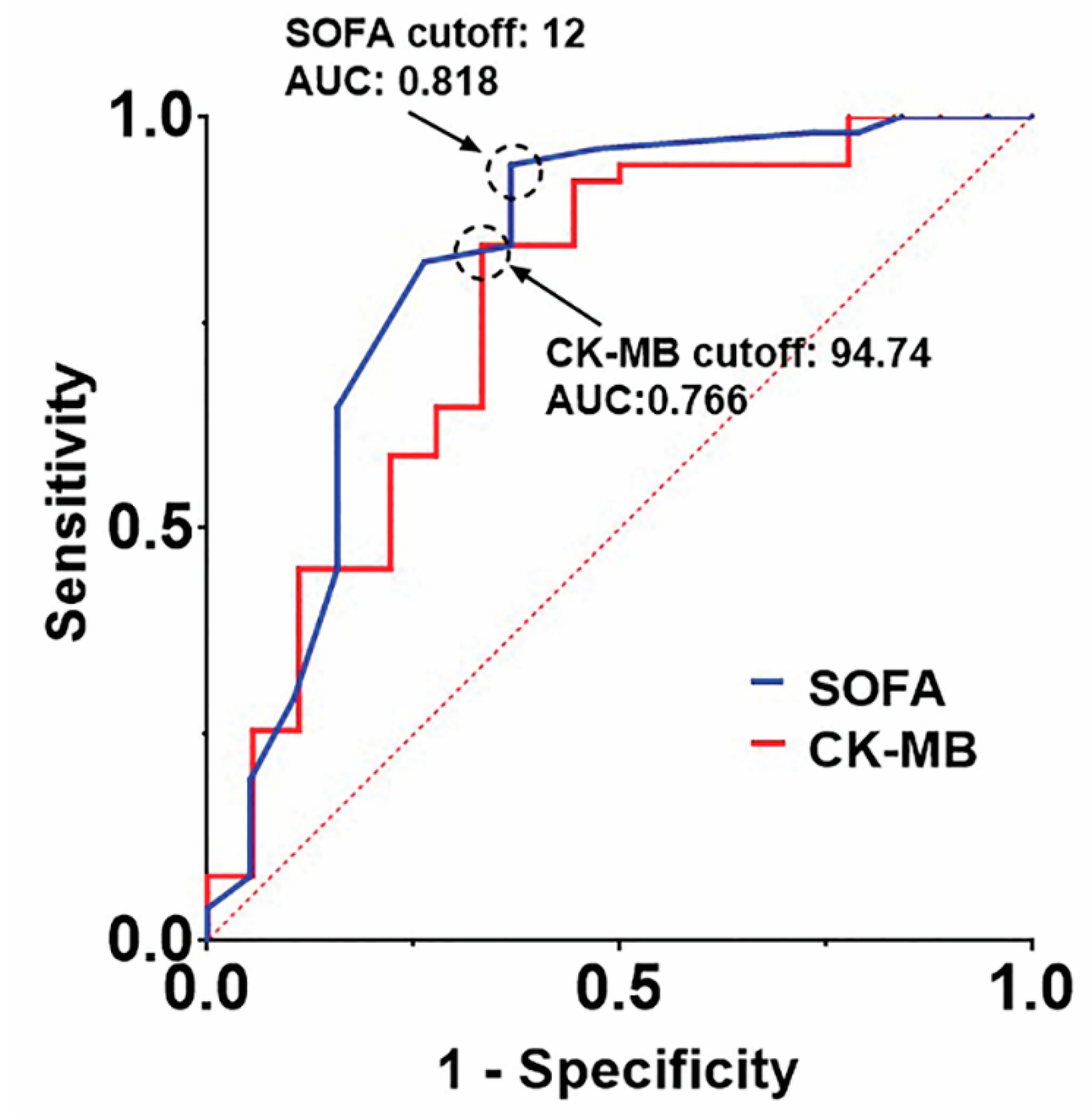
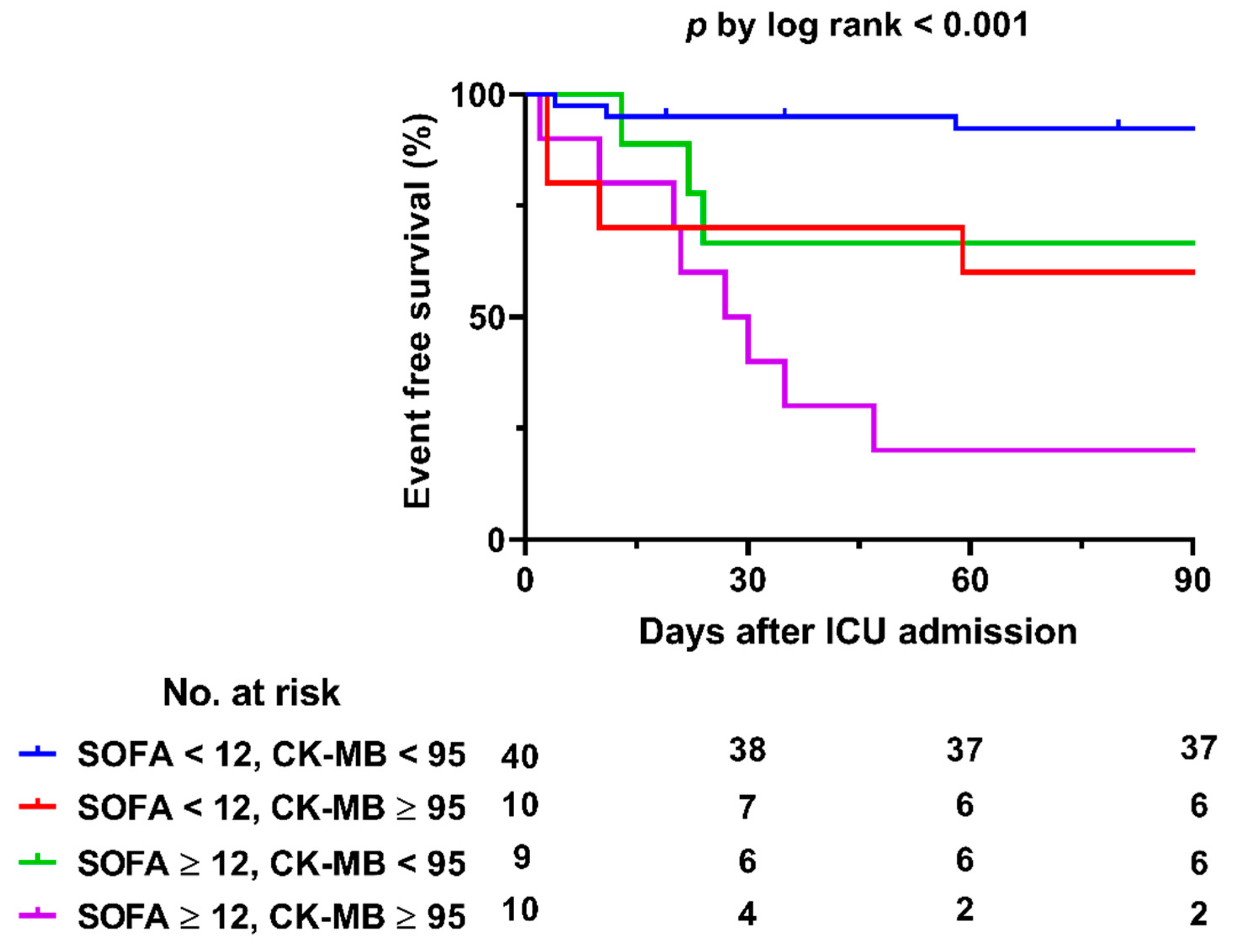
3.2. Clinical Outcomes and Predictors of In-Hospital Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Thiagarajan, R.R.; Barbaro, R.P.; Rycus, P.T.; McMullan, D.M.; Conrad, S.A.; Fortenberry, J.D.; Paden, M.L.; ELSO member centers. Extracorporeal Life Support Organization Registry International Report 2016. ASAIO J. 2017, 63, 60–67. [Google Scholar] [CrossRef]
- Paden, M.L.; Conrad, S.A.; Rycus, P.T.; Thiagarajan, R.R.; ELSO Registry. Extracorporeal Life Support Organization Registry Report 2012. ASAIO J. 2013, 59, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Miyake, C.Y.; Teele, S.A.; Chen, L.; Motonaga, K.S.; Dubin, A.M.; Balasubramanian, S.; Balise, R.R.; Rosenthal, D.N.; Alexander, M.E.; Walsh, E.P.; et al. In-hospital arrhythmia development and outcomes in pediatric patients with acute myocarditis. Am. J. Cardiol. 2014, 113, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Sawamura, A.; Okumura, T.; Ito, M.; Ozaki, Y.; Ohte, N.; Amano, T.; Murohara, T.; CHANGE PUMP Investigators. Prognostic Value of Electrocardiography in Patients with Fulminant Myocarditis Supported by Percutaneous Venoarterial Extracorporeal Membrane Oxygenation- Analysis from the CHANGE PUMP Study. Circ. J. 2018, 82, 2089–2095. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Tsuda, E.; Miyazaki, A.; Ishibashi-Ueda, H.; Yamada, O. Clinical characteristics and long-term outcome of acute myocarditis in children. Heart Vessels. 2013, 28, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Hang, W.; Chen, C.; Seubert, J.M.; Wang, D.W. Fulminant myocarditis: A comprehensive review from etiology to treatments and outcomes. Signal Transduct. Target Ther. 2020, 5, 287. [Google Scholar] [CrossRef]
- Caforio, A.; Sabine, P.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef]
- McCarthy, R.E., 3rd; Boehmer, J.P.; Hruban, R.H.; Hutchins, G.M.; Kasper, E.K.; Hare, J.M.; Baughman, K.L. Long-term outcome of fulminant myocarditis as compared with acute (nonfulminant) myocarditis. N. Engl. J. Med. 2000, 342, 690–695. [Google Scholar] [CrossRef]
- Matsumoto, M.; Asaumi, Y.; Nakamura, Y.; Nakatani, T.; Nagai, T.; Kanaya, T.; Kawakami, S.; Honda, S.; Kataoka, Y.; Nakajima, S.; et al. Clinical determinants of successful weaning from extracorporeal membrane oxygenation in patients with fulminant myocarditis. ESC Heart Fail. 2018, 5, 675–684. [Google Scholar] [CrossRef]
- Ginsberg, F.; Parrillo, J.E. Fulminant myocarditis. Crit. Care Clin. 2013, 29, 465–483. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Matics, T.J.; Sanchez-Pinto, L.N. Adaptation and Validation of a Pediatric Sequential Organ Failure Assessment Score and Evaluation of the Sepsis-3 Definitions in Critically Ill Children. JAMA Pediatr. 2017, 171, e172352. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Toda, K.; Miyagawa, S.; Yoshikawa, Y.; Hata, H.; Yoshioka, D.; Domae, K.; Tsukamoto, Y.; Sakata, Y.; Sawa, Y. Diagnosis, medical treatment, and stepwise mechanical circulatory support for fulminat myocarditis. J. Artif. Organs 2018, 21, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Diddle, J.W.; Almodovar, M.C.; Rajagopal, S.K.; Rycus, P.T.; Thiagarajan, R.R. Extracorporeal membrane oxygenation for the support of adults with acute myocarditis. Crit. Care Med. 2015, 43, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.J.H.; Southern, D.; Wilton, S.B.; James, M.T.; Har, B.; Schnell, G.; van Diepen, S.; Grant, A.D.M. Comparative Prognostic Accuracy of Risk Prediction Models for Cardiogenic Shock. J. Intensive Care Med. 2020, 35, 1513–1519. [Google Scholar] [CrossRef]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Melot, C.; Vincent, J.L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef] [PubMed]
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V. Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults with Suspected Infection Admitted to the Intensive Care Unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef]
- Garcia-Garcia, H.M.; McFadden, E.P.; von Birgelen, C.; Rademaker-Havinga, T.; Spitzer, E.; Kleiman, N.S.; Cohen, D.J.; Kennedy, K.F.; Camenzind, E.; Mauri, L.; et al. Impact of Periprocedural Myocardial Biomarker Elevation on Mortality Following Elective Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2019, 12, 1954–1962. [Google Scholar] [CrossRef]
- Brener, S.J.; Lytle, B.W.; Schneider, J.P.; Ellis, S.G.; Topol, E.J. Association between CK-MB elevation after percutaneous or surgical revascularization and three-year mortality. J. Am. Coll. Cardiol. 2002, 40, 1961–1967. [Google Scholar] [CrossRef][Green Version]
- Brener, S.J.; Ellis, S.G.; Schneider, J.; Topol, E.J. Frequency and long-term impact of myonecrosis after coronary stenting. Eur. Heart J. 2002, 23, 869–876. [Google Scholar] [CrossRef]
- Hsu, K.H.; Chi, N.H.; Yu, H.Y.; Wang, C.H.; Huang, S.C.; Wang, S.S.; Ko, W.J.; Chen, Y.S. Extracorporeal membranous oxygenation support for acute fulminant myocarditis: Analysis of a single center’s experience. Eur. J. Cardiothorac. Surg. 2011, 40, 682–688. [Google Scholar] [CrossRef]
- Ishida, K.; Wada, H.; Sakakura, K.; Kubo, N.; Ikeda, N.; Sugawara, Y.; Ako, J.; Momomura, S. Long-term follow-up on cardiac function following fulminant myocarditis requiring percutaneous extracorporeal cardiopulmonary support. Heart Vessel. 2013, 28, 86–90. [Google Scholar] [CrossRef]
- Mirabel, M.; Luyt, C.E.; Leprince, P.; Trouillet, J.L.; Leger, P.; Pavie, A.; Chastre, J.; Combes, A. Outcomes, long-term quality of life, and psychologic assessment of fulminant myocarditis patients rescued by mechanical circulatory support. Crit. Care Med. 2011, 39, 1029–1035. [Google Scholar] [CrossRef]
- Chong, S.Z.; Fang, C.Y.; Fang, H.Y.; Chen, H.C.; Chen, C.J.; Yang, C.H.; Hang, C.L.; Yip, H.K.; Wu, C.J.; Lee, W.C. Associations with the In-Hospital Survival Following Extracorporeal Membrane Oxygenation in Adult Acute Fulminant Myocarditis. J. Clin. Med. 2018, 7, 452. [Google Scholar] [CrossRef]
- Aoyama, N.; Izumi, T.; Hiramori, K.; Isobe, M.; Kawana, M.; Hiroe, M.; Hishida, H.; Kitaura, Y.; Imaizumi, T.; Japanese Investigators of Fulminant Myocarditis. National survey of fulminant myocarditis in Japan: Therapeutic guidelines and long-term prognosis of using percutaneous cardiopulmonary support for fulminant myocarditis (special report from a scientific committee). Circ. J. 2002, 66, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, R.; Centofanti, P.; Gelsomino, S.; Barili, F.; Di Mauro, M.; Orlando, P.; Botta, L.; Milazzo, F.; Actis Dato, G.; Casabona, R.; et al. Venoarterial Extracorporeal Membrane Oxygenation for Acute Fulminant Myocarditis in Adult Patients: A 5-Year Multi-Institutional Experience. Ann. Thorac. Surg. 2016, 101, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Cipriani, M.; Lilliu, M.; Sormani, P.; Varrenti, M.; Raineri, C.; Petrella, D.; Garascia, A.; Pedrotti, P.; Roghi, A.; et al. Survival and Left Ventricular Function Changes in Fulminant Versus Nonfulminant Acute Myocarditis. Circulation 2017, 136, 529–545. [Google Scholar] [CrossRef]
- Chang, J.; Lin, M.; Chen, T.; Chen, D.; Chen, S.; Hsu, J.; Wang, P.; Lin, Y. Heart Failure and Mortality of Adult Survivors from Acute Myocarditis Requiring Intensive Care Treatment—A Nationwide Cohort Study. Int. J. Med. Sci. 2017, 14, 1241–1250. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ECMO (n = 71) | Non-ECMO (n = 29) | p -Value | |
|---|---|---|---|
| Patient demographics | |||
| Age (year) | 34 (19–46) | 14 (4–49.5) | 0.14 |
| Adult (≥18 year) | 41 (31–49) (n = 55) | 52 (39–56.50) (n = 13) | 0.069 |
| Pediatric (<18 year) | 4 (0–7.75) (n = 16) | 6 (1.5–10.75) (n = 16) | 0.364 |
| Gender, male | 25 (35.2%) | 19 (65.5%) | 0.006 |
| BSA (m2) | 1.60 (1.40–1.69) | 1.43 (0.68–1.72) | 0.137 |
| Smoking | 14 (20%) | 3 (10.3%) | 0.246 |
| Diabetes mellitus | 14 (19.7%) | 1 (3.4%) | 0.039 |
| Hypertension | 15 (21.1%) | 2 (6.9%) | 0.086 |
| Malignancy | 4 (5.6%) | 2 (6.9%) | 0.809 |
| Dyslipidemia | 3 (4.3%) | 1 (3.4%) | 0.857 |
| Chronic kidney disease a | 3 (4.3%) | 0 (0%) | 0.261 |
| Previous coronary artery diseases b | 4 (5.6%) | 0 (0%) | 0.192 |
| Cardiac arrest | 24 (33.8%) | 6 (20.7%) | 0.194 |
| ECPR c | 15 (21.1%) | 0 (0%) | NA |
| Data at ICU admission | |||
| Cardiac enzymes | |||
| Troponin I (ng/mL) | 16.96 (3.42–41.70) | 4.35 (1.25–21.15) | 0.007 |
| CK-MB (ng/mL) | 55.76 (23.96–107.36) | 24.59 (11.92–68.76) | 0.026 |
| NT-proBNP (pg/mL) * | 15618 (7582–32,400) | 7839 (3223–26,338) | 0.068 |
| WBC (×103/μL) | 12.79 (9.17–16.92) | 9.73 (8.11–13.86) | 0.037 |
| CRP (mg/dL) | 4.27 (1.32–11.34) | 2.71 (0.56–6.51) | 0.087 |
| Creatinine (mg/dL) | 1.04 (0.80–1.51) | 0.62 (0.48–1.04) | <0.001 |
| Lactic acid (mmol/L) | 5.09 (2.97–9.08) | 2.33 (1.41–3.81) | <0.001 |
| EF (%) at ICU admission | 20.0 (15.0–34.0) | 40.4 (36.1–58.5) | <0.001 |
| SOFA score d | 9 | 5 | <0.001 |
| Documented arrhythmia | 63 (90%) (n = 70) | 23 (79.3%) | 0.152 |
| Asystole | 5 (7.1%) | 0 (0%) | |
| Brady-arrhythmia e | 12 (17.1%) | 5 (17.2%) | |
| Tachy-arrhythmia f | 36 (51.4%) | 7 (24.1%) | |
| VT/VF g | 30 (42.9%) | 3 (10.3%) | |
| Widened QRS complex h | 3 (4.3%) | 5 (17.2%) | |
| Other arrhythmias i | 7 (10%) | 6 (20.7%) | |
| Mechanical ventilator | 62 (87.3%) | 11 (37.9%) | <0.001 |
| CRRT j | 27 (38.0%) | 1 (3.4%) | <0.001 |
| IABP k | 18 (25.4%) | 2 (6.9%) | 0.036 |
| All (n = 100) | ECMO (n = 71) | Non-ECMO (n = 29) | p-Value | |
|---|---|---|---|---|
| In-hospital mortality | 22 (22%) | 20 (28.2%) | 2 (6.9%) | 0.020 |
| Proportion of heart transplantation/VAD | 8 (8%) | 8 (11.3%) | 0 (0%) | 0.101 |
| Long-term outcomes (n = 78) | ||||
| Death after hospital discharge | 3 (3.8%) | 3 (5.9%) | 0 (0%) | 0.547 |
| Median NYHA class of the survivors | 1 | 1 | 1 | 0.453 |
| EF (%) at last echocardiography during follow-up | 61.7 (56–66.8) | 60 (52.5–65) | 63 (60.1–67.8) | 0.059 |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Overall cohort | ||||
| Age | 1 (0.955–1.048) | 0.985 | ||
| Gender, male | 0.608 (0.094–3.947) | 0.602 | ||
| Deployment of ECMO | 0.563 (0.022–14.386) | 0.729 | ||
| CRRT | 2.889 (0.511–16.332) | 0.230 | ||
| Cardiac arrest | 1.140 (0.163–7.942) | 0.895 | ||
| EF (%) at ICU admission | 0.976 (0.919–1.036) | 0.419 | ||
| CRP | 1.003 (0.871–1.154) | 0.972 | ||
| Lactic acid | 1.106 (0.905–1.352) | 0.323 | ||
| CK-MB | 1.006 (0.997–1.015) | 0.212 | 1.006 (0.998–1.013) | 0.139 |
| SOFA score | 1.480 (1.044–2.098) | 0.028 | 1.715 (1.304–2.256) | <0.001 |
| ECMO group | ||||
| Age | 0.991 (0.950–1.034) | 0.678 | ||
| Gender, male | 0.334 (0.055–2.021) | 0.233 | ||
| CRRT | 2.543 (0.555–11.661) | 0.230 | ||
| Cardiac arrest | 1.028 (0.169–6.235) | 0.976 | ||
| CK-MB | 1.013 (1.003–1.023) | 0.011 | 1.014 (1.003–1.024) | 0.009 |
| SOFA score | 1.492 (1.089–2.046) | 0.013 | 1.499 (1.180–1.903) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.I.; Chung, S.; Yang, J.-H.; Sung, K.; Kim, D.; Choi, J.-O.; Jeon, E.-S.; Yang, J.H.; Cho, Y.H. Extracorporeal Membrane Oxygenation for Fulminant Myocarditis: Increase of Cardiac Enzyme and SOFA Score Is Associated with High Mortality. J. Clin. Med. 2021, 10, 1526. https://doi.org/10.3390/jcm10071526
Lee YI, Chung S, Yang J-H, Sung K, Kim D, Choi J-O, Jeon E-S, Yang JH, Cho YH. Extracorporeal Membrane Oxygenation for Fulminant Myocarditis: Increase of Cardiac Enzyme and SOFA Score Is Associated with High Mortality. Journal of Clinical Medicine. 2021; 10(7):1526. https://doi.org/10.3390/jcm10071526
Chicago/Turabian StyleLee, Yun Im, Suryeun Chung, Ji-Hyuk Yang, Kiick Sung, Darae Kim, Jin-Oh Choi, Eun-Seok Jeon, Jeong Hoon Yang, and Yang Hyun Cho. 2021. "Extracorporeal Membrane Oxygenation for Fulminant Myocarditis: Increase of Cardiac Enzyme and SOFA Score Is Associated with High Mortality" Journal of Clinical Medicine 10, no. 7: 1526. https://doi.org/10.3390/jcm10071526
APA StyleLee, Y. I., Chung, S., Yang, J.-H., Sung, K., Kim, D., Choi, J.-O., Jeon, E.-S., Yang, J. H., & Cho, Y. H. (2021). Extracorporeal Membrane Oxygenation for Fulminant Myocarditis: Increase of Cardiac Enzyme and SOFA Score Is Associated with High Mortality. Journal of Clinical Medicine, 10(7), 1526. https://doi.org/10.3390/jcm10071526