
“It Should Have Been Given Sooner, and We Should Not Have to Fight for It”: A Mixed-Methods Study of the Experience of Diagnosis and Early Management of Cerebral Palsy

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instrument
2.3. Data Analysis
3. Results
3.1. Participant Demographics
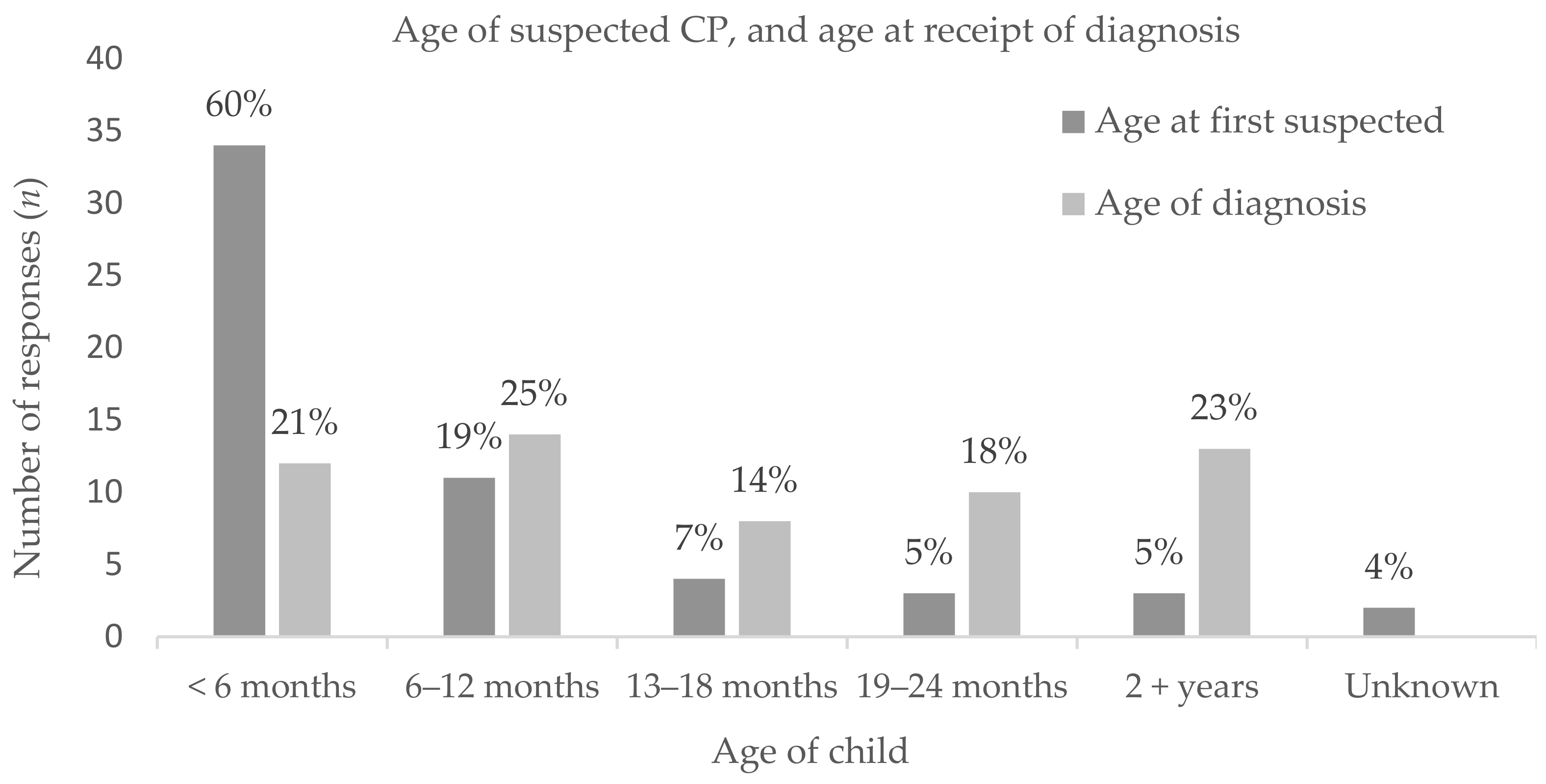
3.2. Family Experience of the Diagnosis
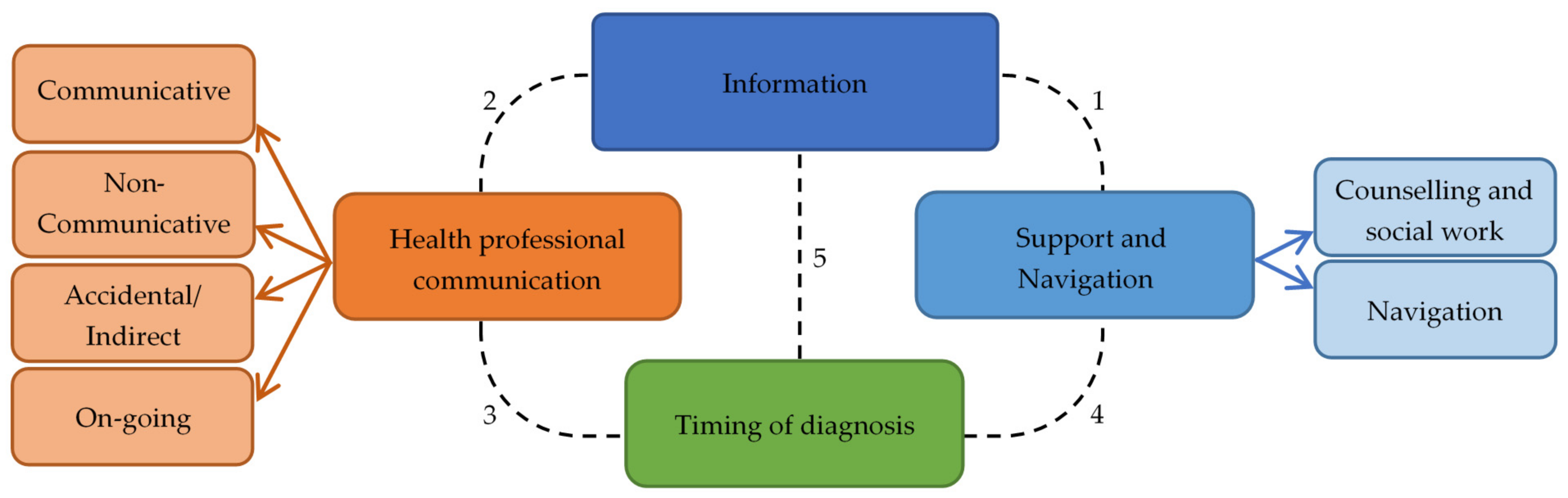
3.3. Themes of Expereinces
3.3.1. Theme: Information Provided about Diagnosis and Outcomes
3.3.2. Theme: Health Professional Communication
Sub Theme: Communicative
“The paediatrician […] met with us in her office 2 days later and we talked for 2.5 h. She has a very holistic view of children’s development. She did NOT sugar-coat anything—she admitted, honestly, the potential problems we may face in the future.”Participant 29
“We described the milestones that our child wasn’t hitting. The paediatrician was lovely, she didn’t interrupt or anything. Once we had finished speaking, she calmly explained she knew why that was, and explained that our child had cerebral palsy. She was very considerate of how we might react and took her time to explain to us in full what this will entail.”Participant 68
Sub Theme: Non-Communicative
“We were referred to a Neuro-developmental therapist who came to our house to meet with us. She walked through our door and within the first minute stated, “ Oh yes she is a typical CP Baby”. That was how we were diagnosed basically! We did not get all the information about CP and what it meant at the time of diagnosis.”Participant 30
“When we were told at birth about the brain damage on the MRI scan, the Doctor didn’t tell us clearly enough (she was too soft about it) and we both came away thinking it was possible our daughter would be OK. Someone had to re-explain to us a couple of days later that she would have lifelong disability and that the brain damage was not reversible.”Participant 52
Sub Theme: Accidental or Indirect Communication
“Had raised concerns with nurses who visited as son was premature…. Was informed nothing to be concerned about. Raised concerns again with paediatrician at regular review. She noted our concerns but never told us what she was suspecting. We received a LETTER in the post which stated she suspected hemiplegia. To be informed about this is a letter was horrendous. I will never forget that day and not having a medical practitioner to talk to and would never wish receiving a diagnosis in the mail on anyone.”Participant 53
“I thought it was a general paediatrician appointment. He said sorry that the results from MRI 8 months ago were incorrect and that PVL is the cause of her CP. Then he realized that I had no idea she even had CP.”Participant 39
“Our daughter experienced a hypoxic event at birth, was diagnosed with HIE. We knew the CP diagnosis was coming but it was never formalized verbally to us—just added to appointment notes.”Participant 28
“I think being expected to understand the diagnosis though reading a letter from the outpatient clinic saying, “may be developing diplegia” and then having a physiotherapist a few months later explain that this means highly likely CP was not very good. Also, we [then] had to wait months before we saw the developmental paediatrician which caused anxiety as we wanted to be doing all we could for our son so he could have the best outcome.”Participant 5
Sub Theme: On-Going Communication
“At 15 days old we were told he had 80-90% chance of having CP and that it would likely be severe based on an MRI. This was not a diagnosis as we were left with a wait and see. He was 2 years before the diagnosis was officially given but by then it was not a shock more an inevitability.”Participant 40
“We knew we were likely dealing with cerebral palsy and the paediatrician had highlighted to us she was under observation for it. We officially recovered our diagnosis when we communicated to the Dr that we thought she had it and he agreed. It was a gentle approach enabling us to accept it when we were ready.”Participant 1
3.3.3. Theme: Time to Diagnosis
“Paediatricians need to risk being wrong and give a diagnosis. The not knowing and wondering what else could be wrong is horrible.”Participant 26
“There we so many opportunities for medical professionals to inform us that our son was high risk of having CP however this information was never passed on to us. […] I know doctors can’t look into the future, but giving a parent an idea in what to expect would be helpful. Your whole world turns upside down at diagnosis stage. […] He was in NICU [Neonatal Intensive Care Unit] 6 weeks and this was never mentioned.”Participant 53
“If I could change one thing it would be earlier diagnosis. She was blue at birth! Delayed from the start, had we had CP explained from beginning and therapy with appropriate therapist she may have progressed faster. […] [The diagnosis] should have been given sooner and we shouldn’t have had to fight for it.”Participant 36
“For 9 odd months my wife kept saying something was wrong, then when finally confirmed, the response was ‘we sometimes get it wrong, oh well’”Participant 37
“Would like to have been referred earlier, very stressful feeling like you can’t do anything for your child, but you know something just isn’t right with them.”Participant 49
“We asked for a label for our son’s conditions to given so we could access support services. It was clearly explained to us that it was given with caution as once given the medical professionals tend to stop looking for an answer.”Participant 33
“It took almost 2years for a Dr to diagnosis, they just keep saying “why do you want that diagnosed she already has lots of diagnosis.” It wasn’t till a visiting paediatrician came to town and saw my daughter that they agreed my daughter has CP and put it down as a diagnosis.”Participant 22
“Having an initially warning of about 5 months that that might be what was going on. I felt like the idea was slowly broken in on us.”Participant 8
“Luckily the Paediatrician understood the need early on for our daughter to have a confirmed diagnosis (even though she was very young) so we had certainty and could access services. He was also very direct and clear which I appreciated.”Participant 52
3.3.4. Theme: Support and Information about the Navigation of the Health Service Journey
Sub Theme: Family Support—Counselling and Social Supports
“After that we were left to sort it out ourselves once the referral to the [hospital] went through. We weren’t put in touch with a counsellor or social service to help us which in hindsight was very poor.”Participant 34
“Support, counselling, where to go and talk to someone with experience. The other things we were offered at the time felt quite offensive. Instead of feeling like an advocate for my child I was seen as being defensive or demanding and hard to deal with.”Participant 2
“Recognizing that it is not only the child with the diagnosis that is affected. The whole family is and every decision impacts ALL of those involved.”Participant 33
3.4. Early Management
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. Suppl. 2007, 109, 8–14. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health; WHO: Geneva, Switzerland, 2001; Available online: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (accessed on 30 July 2020).
- Avieli, H.; Band-Winterstein, T. “What Didn’t I Do for this Child?”: Parents’ Retrospective Construction of their Child’s CP Diagnostic Process. J. Dev. Phys. Disabil. 2017, 29, 385–405. [Google Scholar] [CrossRef]
- Boychuck, Z.; Bussières, A.; Goldschleger, J.; Majnemer, A.; The Prompt Group. Age at referral for diagnosis and rehabilitation services for cerebral palsy: A scoping review. Dev. Med. Child Neurol. 2019, 61, 908–914. [Google Scholar] [CrossRef]
- Novak, I.; Morgan, C.; Adde, L.; Blackman, J.; Boyd, R.N.; Brunstrom-Hernandez, J.; Cioni, G.; Damiano, D.; Darrah, J.; Eliasson, A.-C.; et al. Early, accurate diagnosis and early intervention in cerebral palsy: Advances in diagnosis and treatment. JAMA Pediatr. 2017, 171, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Ashwal, S.; Russman, B.S.; Blasco, P.A.; Miller, G.; Sandler, A.; Shevell, M.; Stevenson, R. Practice Parameter: Diagnostic assessment of the child with cerebral palsy: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2004, 62, 851–863. [Google Scholar] [CrossRef] [PubMed]
- Bosanquet, M.; Copeland, L.; Ware, R.; Boyd, R. A systematic review of tests to predict cerebral palsy in young children. Dev. Med. Child Neurol. 2013, 55, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Romeo, D.M.; Ricci, D.; Brogna, C.; Mercuri, E. Use of the Hammersmith Infant Neurological Examination in infants with cerebral palsy: A critical review of the literature. Dev. Med. Child Neurol. 2016, 58, 240–245. [Google Scholar] [CrossRef]
- Morgan, C.; Romeo, D.M.; Chorna, O.; Novak, I.; Galea, C.; Del Secco, S.; Guzzetta, A. The Pooled Diagnostic Accuracy of Neuroimaging, General Movements, and Neurological Examination for Diagnosing Cerebral Palsy Early in High-Risk Infants: A Case Control Study. J. Clin. Med. 2019, 8, 1879. [Google Scholar] [CrossRef]
- Morgan, C.; Darrah, J.; Gordon, A.M.; Harbourne, R.; Spittle, A.; Johnson, R.; Fetters, L. Effectiveness of motor interventions in infants with cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2016, 58, 900–909. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.; Novak, I.; Dale, R.C.; Guzzetta, A.; Badawi, N. Single blind randomised controlled trial of Goals- Activity- Motor- Enrichment in infants at high risk of cerebral palsy. Res. Dev. Disabil. 2016, 55, 256–267. [Google Scholar] [CrossRef]
- Eliasson, A.C.; Holmefur, M. The influence of early modified constraint-induced movement therapy training on the longitudinal development of hand function in children with unilateral cerebral palsy. Dev. Med. Child Neurol. 2015, 57, 89–94. [Google Scholar] [CrossRef]
- King, S.; Teplicky, R.; King, G.; Rosenbaum, P. Family-Centered Service for Children with Cerebral Palsy and Their Families: A Review of the Literature. Semin. Pediatric Neurol. 2004, 11, 78–86. [Google Scholar] [CrossRef]
- Mckay, M.; Hensey, O. From the other side: Parents’ views of their early contacts with health professionals. Child Care Health Dev. 1990, 16, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Baird, G.; McConachie, H.; Scrutton, D. Parents’ perceptions of disclosure of the diagnosis of cerebral palsy. Arch. Dis. Child. 2000, 83, 475. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.P.; Kellett, U.M.; St John, W. Cerebral palsy: Experiences of mothers after learning their child’s diagnosis. J. Adv. Nurs. 2010, 66, 1213–1221. [Google Scholar] [CrossRef] [PubMed]
- Dagenais, L.; Hall, N.; Majnemer, A.; Birnbaum, R.; Dumas, F.; Gosselin, J.; Koclas, L.; Shevell, M.I. Communicating a Diagnosis of Cerebral Palsy: Caregiver Satisfaction and Stress. Pediatr. Neurol. 2006, 35, 408–414. [Google Scholar] [CrossRef]
- Guttmann, K.; Flibotte, J.; DeMauro, S.B. Parental Perspectives on Diagnosis and Prognosis of Neonatal Intensive Care Unit Graduates with Cerebral Palsy. J. Pediatr. 2018, 203, 156–162. [Google Scholar] [CrossRef]
- Burns, K.E.; Duffett, M.; Kho, M.E.; Meade, M.O.; Adhikari, N.K.; Sinuff, T.; Cook, D.J.; ACCADEMY Group. A guide for the design and conduct of self-administered surveys of clinicians. Can. Med. Assoc. J. 2008, 179, 245–252. [Google Scholar] [CrossRef]
- Passmore, C.; Dobbie, A.E.; Parchman, M.; Tysinger, J. Guidelines for constructing a survey. Fam. Med. 2002, 34, 281–286. [Google Scholar]
- Shevell, A.H.; Shevell, M. Doing the “talk”: Disclosure of a diagnosis of cerebral palsy. J. Child Neurol. 2013, 28, 230–235. [Google Scholar] [CrossRef]
- McIntyre, S.; Morgan, C.; Walker, K.; Novak, I. Cerebral palsy—Don’t delay. Dev. Disabil. Res. Rev. 2011, 17, 114–129. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.A.; Mackey, A.; Sorhage, A.; Battin, M.; Wilson, N.; Spittle, A.; Stott, N.S. Clinical practice of health professionals working in early detection for infants with or at risk of cerebral palsy across New Zealand. J. Paediatr. Child Health 2020, 7. [Google Scholar] [CrossRef]
- Cottrell, D.J.; Summers, K. Communicating an evolutionary diagnosis of disability to parents. Child Care Health Dev. 1990, 16, 211–218. [Google Scholar] [CrossRef]
- Sices, L.; Egbert, L.; Mercer, M.B. Sugar-coaters and Straight Talkers: Communicating About Developmental Delays in Primary Care. Pediatrics 2009, 124, e705–e713. [Google Scholar] [CrossRef] [PubMed]
- Fallowfield, L.; Jenkins, V. Communicating sad, bad, and difficult news in medicine. Lancet 2004, 363, 312–319. [Google Scholar] [CrossRef]
- Guttmann, K.; Flibotte, J.; DeMauro, S.B.; Seitz, H. A Mixed Methods Analysis of Parental Perspectives on Diagnosis and Prognosis of Neonatal Intensive Care Unit Graduates with Cerebral Palsy. J. Child Neurol. 2020, 35, 336–343. [Google Scholar] [CrossRef]
- Sloper, P.; Turner, S. Determinants of parental satisfaction with disclosure of disability. Dev. Med. Child Neurol. 1993, 35, 816–825. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total n (%) | ||||||
|---|---|---|---|---|---|---|
| Responder (n = 57) | ||||||
| Mother | 50 (88%) | |||||
| Father | 2 (3.5%) | |||||
| Mother and Father | 2 (3.5%) | |||||
| Grandparent | 3 (5%) | |||||
| Number of children in the family (n = 57) | ||||||
| 1 child (with CP) | 15 (26%) | |||||
| 2 children | 29 (51%) | |||||
| 3 children | 9 (16%) | |||||
| 4 children | 4 (7%) | |||||
| Prioritised ethnicity of child with CP (n = 57) | ||||||
| New Zealand European | 42 (74%) | |||||
| Māori | 11 (19%) | |||||
| Pacific | 1 (<2%) | |||||
| Asian | 1 (<2%) | |||||
| Prefer not to answer | 1 (<2%) | |||||
| Childs birthplace | Receipt of health services | |||||
| North Island (NZ) | 44 (77%) | 47 (82.5%) | ||||
| South Island (NZ) | 11 (19.5%) | 10 (17.5%) | ||||
| UK | 2 (3.5%) | |||||
| Topographical classification (n = 57) | ||||||
| Hemiplegic | Diplegic | Quadriplegic | Unknown | |||
| 21 (37%) | 16 (28%) | 16 (28%) | 4 (7%) | |||
| Functional classification | ||||||
| I | II | III | IV | V | Unknown | |
| GMFCS (n = 53) | 12 (23%) | 16 (30%) | 4 (7.5%) | 7 (13%) | 6 (11.5%) | 8 (15%) |
| MACS (n = 48) | 4 (8.5%) | 14 (29%) | 3 (6%) | 5 (10.5%) | 5 (10.5%) | 17 (35.5%) |
| Health professional providing the diagnosis (n = 56) | |||||
| General Paediatrician | 23 (41%) | Neonatologist & General Paediatrician | 1 (1%) | ||
| Pediatric Neurologist | 12 (21%) | Neonatal follow-up/Pediatric fellow | 1 (1%) | ||
| Developmental Paediatrician | 9 (16%) | General Practitioner | 1 (1%) | ||
| Neonatologist | 2 (4%) | Physiotherapist | 1 (1%) | ||
| Occupational Therapist | 3 (5%) | PICU Consultant | 1 (1%) | ||
| Pediatric Rehabilitation Consultant | 2 (4%) | ||||
| At the time of diagnosis and the months following, where you given: | Yes | Yes, not enough | No | I do not recall | |
| Clear information about what the diagnostic tests/assessments were for? | 24 (43%) | 13 (23%) | 14 (25%) | 5 (9%) | |
| Clear information about what cerebral palsy is? | 21 (38%) | 12 (21%) | 21 (38%) | 2 (4%) | |
| Clear information about what the future may involve for your child? | 17 (30%) | 17 (30%) | 22 (39%) | 0 (0%) | |
| Time to ask questions and clarify your understanding? | 27 (48%) | 15 (27%) | 11 (20%) | 3 (3%) | |
| Family satisfaction with diagnosis experience (n = 57) | |||||
| Very satisfied | 13 (23%) | ||||
| Satisfied | 16 (28%) | ||||
| Neutral | 10 (18%) | ||||
| Dissatisfied | 11 (19%) | ||||
| Extremely Dissatisfied | 7 (12%) | ||||
| Theme | Extremely/Satisfied (n) | Neutral (n) | Extremely/Dissatisfied (n) | |
|---|---|---|---|---|
| Health Professional Communication | Communicative | 12 | 1 | 1 |
| On-going | 7 | 1 | ||
| Non-communicative | 4 | 8 | ||
| Accidental/Indirect | 3 | 6 | ||
| Time to diagnosis | Early/ongoing | 8 | 3 | 3 |
| Delayed/withheld | 4 | 1 | 8 | |
| Support | Navigation | 8 | 4 | 5 |
| Family & social support | 28 | 10 | 16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williams, S.A.; Alzaher, W.; Mackey, A.; Hogan, A.; Battin, M.; Sorhage, A.; Stott, N.S. “It Should Have Been Given Sooner, and We Should Not Have to Fight for It”: A Mixed-Methods Study of the Experience of Diagnosis and Early Management of Cerebral Palsy. J. Clin. Med. 2021, 10, 1398. https://doi.org/10.3390/jcm10071398
Williams SA, Alzaher W, Mackey A, Hogan A, Battin M, Sorhage A, Stott NS. “It Should Have Been Given Sooner, and We Should Not Have to Fight for It”: A Mixed-Methods Study of the Experience of Diagnosis and Early Management of Cerebral Palsy. Journal of Clinical Medicine. 2021; 10(7):1398. https://doi.org/10.3390/jcm10071398
Chicago/Turabian StyleWilliams, Sîan A, Woroud Alzaher, Anna Mackey, Amy Hogan, Malcolm Battin, Alexandra Sorhage, and N Susan Stott. 2021. "“It Should Have Been Given Sooner, and We Should Not Have to Fight for It”: A Mixed-Methods Study of the Experience of Diagnosis and Early Management of Cerebral Palsy" Journal of Clinical Medicine 10, no. 7: 1398. https://doi.org/10.3390/jcm10071398
APA StyleWilliams, S. A., Alzaher, W., Mackey, A., Hogan, A., Battin, M., Sorhage, A., & Stott, N. S. (2021). “It Should Have Been Given Sooner, and We Should Not Have to Fight for It”: A Mixed-Methods Study of the Experience of Diagnosis and Early Management of Cerebral Palsy. Journal of Clinical Medicine, 10(7), 1398. https://doi.org/10.3390/jcm10071398