
Acute Kidney Injury Post-Percutaneous Nephrolithotomy (PNL): Prospective Outcomes from a University Teaching Hospital

 , , and
, , and
Abstract
1. Introduction
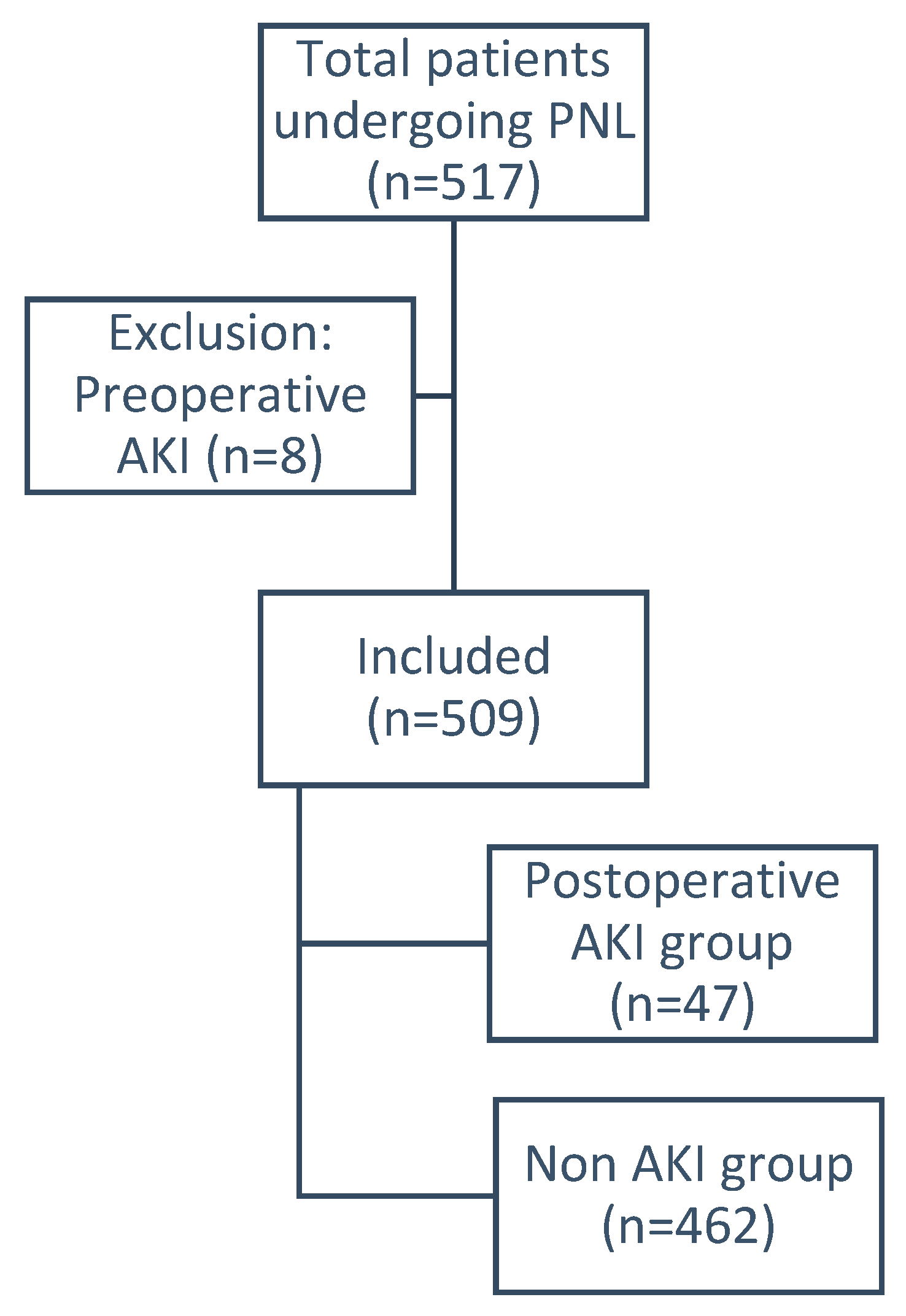
2. Patients and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Türk, C.; Petřík, A.; Sarica, K.; Seitz, C.; Skolarikos, A.; Straub, M.; Knoll, T. EAU guidelines on interventional treatment for urolithiasis. Eur. Urol. 2016, 69, 475–482. [Google Scholar] [CrossRef]
- Reeves, T.; Pietropaolo, A.; Gadzhiev, N.; Seitz, C.; Somani, B.K. Role of Endourological Procedures (PCNL and URS) on Renal Function: A Systematic Review. Curr. Urol. Rep. 2020, 21, 21. [Google Scholar] [CrossRef]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J. Am. Soc. Nephrol. 2005, 16, 3365–3370. [Google Scholar] [CrossRef] [PubMed]
- Hobson, C.; Ozrazgat-Baslanti, T.; Kuxhausen, A.; Thottakkara, P.; Efron, P.A.; Moore, F.A.; Moldawer, L.L.; Segal, M.S.; Bihorac, A. Cost and mortality associated with postoperative acute kidney injury. Ann. Surg. 2015, 261, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Okusa, M.D.; Davenport, A. Reading between the (guide) lines: The KD IGO practice guideline on acute kidney injury in the individual patient. Kidney Int. 2014, 85, 39–48. [Google Scholar] [CrossRef]
- Caddeo, G.; Williams, S.T.; McIntyre, C.W.; Selby, N.M. Acute kidney injury in urology patients: Incidence, causes and outcomes. Nephrourol. Mon. 2013, 5, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Cheungpasitporn, W.; Akhoundi, A.; Ahmed, A.H.; Kashani, K.B. Actual versus ideal body weight for acute kidney injury diagnosis and classification in critically Ill patients. BMC Nephrol. 2014, 15, 176. [Google Scholar] [CrossRef]
- De La Rosette, J.J.; Opondo, D.; Daels, F.P.; Giusti, G.; Serrano, A.; Kandasami, S.V.; Wolf, J.S., Jr.; Grabe, M.; Gravas, S.; Croes Pcnl Study Group. Categorisation of complications and validation of the Clavien score for percutaneous nephrolithotomy. Eur. Urol. 2012, 62, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Michel, M.S.; Trojan, L.; Rassweiler, J.J. Complications in percutaneous nephrolithotomy. Eur. Urol. 2007, 51, 899–906, discussion 906. [Google Scholar] [CrossRef]
- Yu, J.; Park, H.K.; Kwon, H.J.; Lee, J.; Hwang, J.H.; Kim, H.Y. Risk factors for acute kidney injury after percutaneous nephrolithotomy: Implications of intraoperative hypotension. Medicine 2018, 97, e11580. [Google Scholar] [CrossRef]
- Fulla, J.; Calle, J.; Elia, M.; Wright, H.; Li, I. MP22-03 Acute kidney injury and percutaneous nephrolithotomy: Frequency and predictive factors. J. Urol. 2020, 203 (Suppl. 4), e328. [Google Scholar] [CrossRef]
- El-Nahas, A.R.; Taha, D.E.; Ali, H.M.; Elshal, A.M.; Zahran, M.H.; El-Tabey, N.A.; El-Assmy, A.M.; Harraz, A.M.; Moawad, H.E.; Othman, M.M. Othman Acute kidney injury after percutaneous nephrolithotomy for stones in solitary kidneys. Scand. J. Urol. 2017, 51, 165–169. [Google Scholar] [CrossRef]
- Patel, R.; Agarwal, S.; Sankhwar, S.N.; Goel, A.; Singh, B.P.; Kumar, M. A prospective study assessing feasibility of performing percutaneous nephrolithotomy in chronic kidney disease patients—What factors affect the outcome? Int. Braz J. Urol. 2019, 45, 765–774. [Google Scholar] [CrossRef]
- Emiliani, E.; Talso, M.; Baghdadi, M.; Traxer, O. Renal parenchyma injury after percutaneous nephrolithotomy tract dilatations in pig and cadaveric kidney models. Cent. Eur. J. Urol. 2017, 70, 69–75. [Google Scholar]
- Sairam, K.; Scoffone, C.M.; Alken, P.; Turna, B. Percutaneous nephrolithotomy and chronic kidney disease: Results from the CROES PC NL Global Study. J. Urol. 2012, 188, 1195–1200. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; MacKenzie, C.R.; Gold, J.P.; Ales, K.L.; Topkins, M.; Shires, G.T. Preoperative characteristics predicting intraoperative hypotension and hypertension among hypertensives and diabetics undergoing noncardiac surgery. Ann. Surg. 1990, 212, 66–81. [Google Scholar] [CrossRef]
- Oakley, I.; Emond, L. Diabetic cardiac autonomic neuropathy and anesthetic management: Review of the literature. AANA J. 2011, 79, 473–479. [Google Scholar]
- Comfere, T.; Sprung, J.; Kumar, M.M.; Draper, M.; Wilson, D.P.; Williams, B.A.; Danielson, D.R.; Liedl, L.; Warner, D.O. Angiotensin system inhibitors in a general surgical population. Anesth Analg. 2005, 100, 636–644. [Google Scholar] [CrossRef]
- Cheungpasitporn, W.; Thongprayoon, C.; Harrison, A.M.; Erickson, S.B. Admission hyperuricemia increases the risk of acute kidney injury in hospitalized patients. Clin. Kidney J. 2016, 9, 51–56. [Google Scholar] [CrossRef]
- Ejaz, A.A.; Johnson, R.J.; Shimada, M.; Mohandas, R.; Alquadan, K.F.; Beaver, T.M.; Lapsia, V.; Dass, B. The Role of Uric Acid in Acute Kidney Injury. Nephron 2019, 142, 275–283. [Google Scholar] [CrossRef]
- De la Rosette, J.J.; Zuazu, J.R.; Tsakiris, P.; Elsakka, A.M.; Zudaire, J.J.; Laguna, M.P.; de Reijke, T.M. Prognostic factors and percutaneous nephrolithotomy morbidity: A multivariate analysis of a contemporary series using the Clavien classification. J. Urol. 2008, 180, 2489–2493. [Google Scholar] [CrossRef]
- Muslumanoglu, A.Y.; Tefekli, A.; Karadag, M.A.; Tok, A.; Sari, E.; Berberoglu, Y. Impact of percutaneous access point number and location on complication and success rates in percutaneous nephrolithotomy. Urol. Int. 2006, 77, 340–346. [Google Scholar] [CrossRef]
- Aron, M.; Yadav, R.; Goel, R.; Kolla, S.B.; Gautam, G.; Hemal, A.K.; Gupta, N.P. Multi-tract percutaneous nephrolithotomy for large complete staghorn calculi. Urol. Int. 2005, 75, 327–332. [Google Scholar] [CrossRef]
- Rashid, A.O.; Fakhulddin, S.S. Risk factors for fever and sepsis after percutaneous nephrolithotomy. Asian J. Urol. 2016, 3, 82–87. [Google Scholar] [CrossRef]
- Devarajan, P. Emerging urinary biomarkers in the diagnosis of acute kidney injury. Expert Opin. Med. Diagn. 2008, 2, 387–398. [Google Scholar] [CrossRef] [PubMed]
- Borthwick, E.; Ferguson, A. Perioperative acute kidney injury: Risk factors, recognition, management, and outcomes. BMJ 2010, 341, c3365. [Google Scholar] [CrossRef] [PubMed]
- Venkatachalam, M.A.; Griffin, K.A.; Lan, R.; Geng, H.; Saikumar, P.; Bidani, A.K. Acute kidney injury: A springboard for progression in chronic kidney disease. Am. J. Physiol. Renal. Physiol. 2010, 298, F1078–F1094. [Google Scholar] [CrossRef]
- Bucuras, V.; Gopalakrishnam, G.; Wolf, J.S., Jr.; Sun, Y.; Bianchi, G.; Erdogru, T.; de la Rosette, on behalf of the CROES PCNL Study Group. The Clinical Research Office of the Endourological Society Percutaneous Nephrolithotomy Global Study: Nephrolithotomy in 189 patients with solitary kidneys. J. Endourol. 2012, 26, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Peng, Y.; Li, L.; Li, X.; Wang, Q.; Zhang, W.; Dong, H.; Shen, R.; Lu, C.; Liu, M.; et al. Renal function changes after percutaneous nephrolithotomy in patients with renal calculi with a solitary kidney compared to bilateral kidneys. BJU Int. 2018, 122, 633–638. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Complication | Clavien–Dindo | 15Fr | 22Fr | 24Fr | 26Fr | 28Fr | 30Fr | 32Fr | 34Fr | 36Fr | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fever | 2 | 8 | 0 | 3 | 8 | 18 | 4 | 12 | 1 | 2 | 0.743 |
| Haematuria | 1 | 0 | 0 | 2 | 5 | 3 | 1 | 8 | 0 | 0 | 0.342 |
| Angioembolization | 3B | 0 | 0 | 1 | 3 | 2 | 0 | 0 | 0 | 0 | 0.663 |
| Auxiliary proc. | 0.143 | ||||||||||
| URS | 0 | 0 | 0 | 2 | 3 | 1 | 1 | 0 | 0 | ||
| 2nd PNL | 0 | 0 | 0 | 2 | 0 | 0 | 2 | 0 | 0 | ||
| Bladder wash | 0 | 0 | 1 | 2 | 0 | 0 | 2 | 0 | 0 | ||
| Stent reposition | 3A | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | |
| Visual internal Urethrotomy | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Variables | All Patients (n = 509) | AKI Cohort (n = 47) | Non-AKI (n = 462) | p-Value | |
|---|---|---|---|---|---|
| Patient Characteristics | |||||
| Age (years) (mean ± SD) | 48.13 ± 13.92 | 54.83 ± 13.907 | 47.45 ± 13.75 | 0.001 | |
| Gender (M) | 388 (76.2%) | 39 (83%) | 349 (75.5%) | 0.254 | |
| Gender (F) | 121 (23.8%) | 8 (17%) | 113 (24.5%) | ||
| BMI (kg/m2) | 25.23 ± 2.94 | 25.21 ± 3.12 | 25.23 ± 2.92 | 0.974 | |
| Hypertension | 142 (27.9%) | 24 (51.1%) | 118 (25.5%) | 0.0002 | |
| Diabetes mellitus | 94 (18.5%) | 14 (29.8%) | 80 (17.3%) | 0.036 | |
| ACE inhibitors | 22 (4.3%) | 5 (10.6%) | 17 (3.7%) | 0.043 | |
| Beta-blockers | 10 (2%) | 1 (2.1%) | 9 (1.9%) | 1.00 | |
| Preoperative Laboratory Values | |||||
| Hemoglobin (mg/dL) | 13.29 ± 1.91 | 12.63 ± 2.25 | 13.36 ± 1.86 | 0.013 | |
| Platelet(/µL) | 273,669.36 ± 79,821.98 | 276,833.33 ± 103,392.68 | 273,354 ± 77,278.68 | 0.778 | |
| Prothrombin time (s) | 10.58 ± 0.39 | 10.75 ± 0.66 | 10.55 ± 0.32 | 0.006 | |
| Creatinine (mg/dL) | 1.42 ± 4.30 | 1.34 ± 0.76 | 1.43 ± 4.5 | 0.895 | |
| Uric Acid (mg/dL) | 4.13 ± 1.52 | 5.23 ± 1.46 | 3.91 ± 1.44 | 0.00001 | |
| Total leucocyte count (/mm3) | 8.73 ± 3.84 | 9.73 ± 9.54 | 8.63 ± 2.65 | 0.06 | |
| Stone Characteristics | |||||
| Stone Volume (mm3) (median (Q1–Q3)) | 880.95 (524.38–1801.25) | 2117.94 (761–12,452) | 825 (503–1573) | 0.00 | |
| Hounsfield Unit (HU) | 970.59 ± 278.55 | 817.45 ± 439.76 | 985.18 ± 253.98 | 0.0001 | |
| Stone location | Upper Calyx | 26 (5.1%) | 2 (4.3%) | 24 (5.2%) | 1.000 |
| Middle Calyx | 53 (10.4%) | 9 (19.1%) | 44 (9.5%) | 0.074 | |
| Lower Calyx | 138 (27.1%) | 15 (31.9%) | 123 (26.6%) | 0.437 | |
| Pelvic | 190 (37.3%) | 14 (29.8%) | 176 (38.1%) | 0.262 | |
| PUJ | 153 (30.1%) | 12 (25.5%) | 141 (30.5%) | 0.477 | |
| Staghorn | 21 (4.12%) | 6 (12.8%) | 15 (3.24%) | 0.008 | |
| Variables | All Patients (n = 509) | AKI Cohort (n = 47) | Non-AKI (n = 462) | p | |
|---|---|---|---|---|---|
| Puncture site | Supracostal | 75 (14.7%) | 5 (10.6%) | 70 (15.2%) | 0.406 |
| Infracostal | 434 (85.3%) | 42 (89.4%) | 392 (84.8%) | ||
| Tract size (Fr) (median (Q1–Q3)) | 28 (26–32) | 28 (26–28) | 28 (26–32) | 0.032 | |
| Puncture Number | Single Puncture | 497 (97.6%) | 43 (91.5%) | 454 (98.3%) | 0.019 |
| >1 Puncture | 12 (2.35%) | 4 (8.51%) | 8 (1.73%) | ||
| Blood Transfusion | 15 (2.9%) | 3 (6.4%) | 12 (2.6%) | 0.153 | |
| Operative time (minutes) | 55.99 ± 16.71 | 63.51 ± 21.79 | 55.23 ± 15.93 | 0.001 | |
| Variable | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| Unadjusted OR | p-Value | Adjusted OR | p-Value | ||
| Age | 1.041 (1.017–1.066) | 0.001 | 1.050 (0.998–1.105) | 0.060 | |
| Gender | Male | 1.578 (0.717–3.477) | 0.257 | 0.129 (0.021–0.787) | 0.026 |
| Female | 1.0 | 1.0 | |||
| BMI | 0.998 (0.901–1.106) | 0.974 | 0.712 (0.550–0.923) | 0.010 | |
| Hypertension | Yes | 3.042 (1.655–5.593) | 0.0003 | 2.514 (0.699–9.035) | 0.158 |
| No | 1.0 | 1.0 | |||
| Diabetes Mellitus | Yes | 2.026 (1.037–3.959) | 0.039 | 2.423 (0.521–11.260) | 0.259 |
| No | 1.0 | 1.0 | |||
| ACE inhibitors | Yes | 3.116 (1.095–8.871) | 0.033 | 60.404 (1.619–2253.49) | 0.026 |
| No | 1.0 | 1.0 | |||
| Beta-blocker | Yes | 1.094 (0.136–8.830) | 0.933 | 0.770 (0.031–19.033) | 0.873 |
| No | 1.0 | 1.0 | |||
| Creatinine | 0.994 (0.911–1.085) | 0.896 | 1.332 (0.861–2.059) | 0.198 | |
| Uric Acid | 1.758 (1.336–2.315) | 0.00005 | 2.163 (1.459–3.209) | 0.0001 | |
| Total leucocyte count | 1.045 (0.989–1.103) | 0.116 | 0.999 (0.841–1.187) | 0.988 | |
| Operative Time | 1.028 (0.983–1.049) | 0.001 | 1.015 (0.982–1.049) | 0.364 | |
| Blood Transfusion (n) | Yes | 2.557 (0.695–9.405) | 0.158 | 8.408 (0.396–178.42) | 0.172 |
| No | 1.0 | 1.0 | |||
| Stone size | 1.000 | 1.000 | |||
| Stone Location (n) | Upper calyx | 0.811 (0.186–3.545) | 0.781 | 0.223 (0.011–4.509) | 0.328 |
| Middle calyx | 2.250 (1.021–4.959) | 0.044 | 1.822 (0.269–12.370) | 0.539 | |
| Lower calyx | 1.292 (0.676–2.467) | 0.438 | 1.843 (0.336–10.121) | 0.482 | |
| Pelvis | 0.689 (0.359–1.324) | 0.264 | 1.897 (0.333–10.796) | 0.471 | |
| PUJ | 0.478 (0.394–1.548) | 0.781 | 1.582 (0.205–12.207) | 0.660 | |
| Staghorn | 4.361 (1.605–11.846) | 0.004 | 0.594 (0.032–10.944) | 0.726 | |
| Tract number (n) | Single Tract | 1.000 | 1.000 | ||
| >1 Tracts | 5.279 (1.527–18.248) | 0.009 | 89.698 (0.795–10,119.9) | 0.062 | |
| Tract site (n) | Supracostal | 0.667 (0.255–1.744) | 0.408 | 0.054 (0.003–1.121) | 0.05 |
| Infracostal | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pillai, S.; Kriplani, A.; Chawla, A.; Somani, B.; Pandey, A.; Prabhu, R.; Choudhury, A.; Pandit, S.; Taori, R.; Hegde, P. Acute Kidney Injury Post-Percutaneous Nephrolithotomy (PNL): Prospective Outcomes from a University Teaching Hospital. J. Clin. Med. 2021, 10, 1373. https://doi.org/10.3390/jcm10071373
Pillai S, Kriplani A, Chawla A, Somani B, Pandey A, Prabhu R, Choudhury A, Pandit S, Taori R, Hegde P. Acute Kidney Injury Post-Percutaneous Nephrolithotomy (PNL): Prospective Outcomes from a University Teaching Hospital. Journal of Clinical Medicine. 2021; 10(7):1373. https://doi.org/10.3390/jcm10071373
Chicago/Turabian StylePillai, Sunil, Akshay Kriplani, Arun Chawla, Bhaskar Somani, Akhilesh Pandey, Ravindra Prabhu, Anupam Choudhury, Shruti Pandit, Ravi Taori, and Padmaraj Hegde. 2021. "Acute Kidney Injury Post-Percutaneous Nephrolithotomy (PNL): Prospective Outcomes from a University Teaching Hospital" Journal of Clinical Medicine 10, no. 7: 1373. https://doi.org/10.3390/jcm10071373
APA StylePillai, S., Kriplani, A., Chawla, A., Somani, B., Pandey, A., Prabhu, R., Choudhury, A., Pandit, S., Taori, R., & Hegde, P. (2021). Acute Kidney Injury Post-Percutaneous Nephrolithotomy (PNL): Prospective Outcomes from a University Teaching Hospital. Journal of Clinical Medicine, 10(7), 1373. https://doi.org/10.3390/jcm10071373