
Impact of Antibiotic Therapy and Metabolic Parameters in Non-Small Cell Lung Cancer Patients Receiving Checkpoint Inhibitors



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Endpoints
2.3. 18F-Fluorodeoxyglucose Positron Emission Tomography Computed Tomography (18F-FDG PET/CT) Imaging Protocol
2.4. Statistical Analysis
3. Results
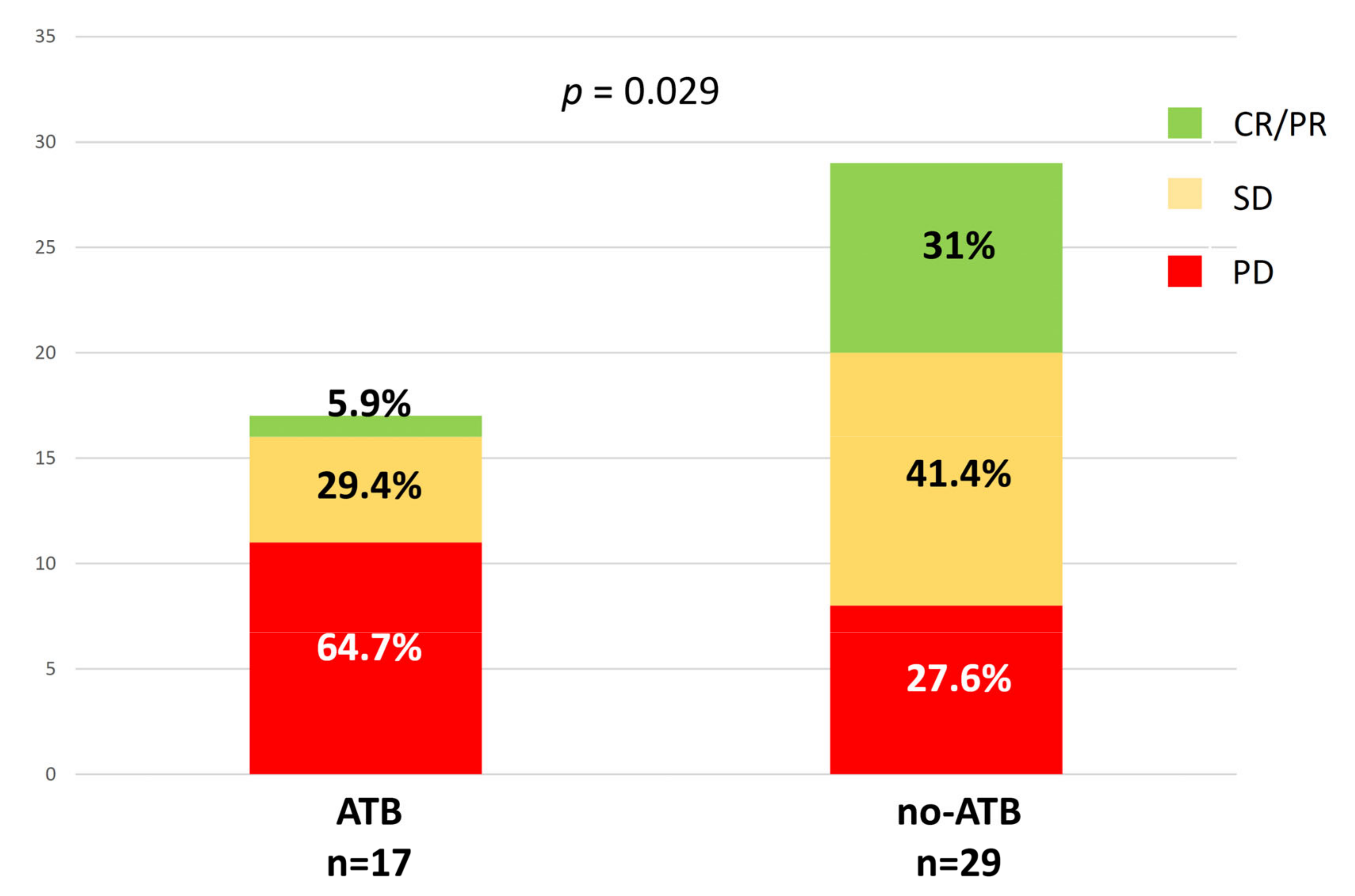
3.1. Antibiotics (ATB) Therapy and Response Evaluation
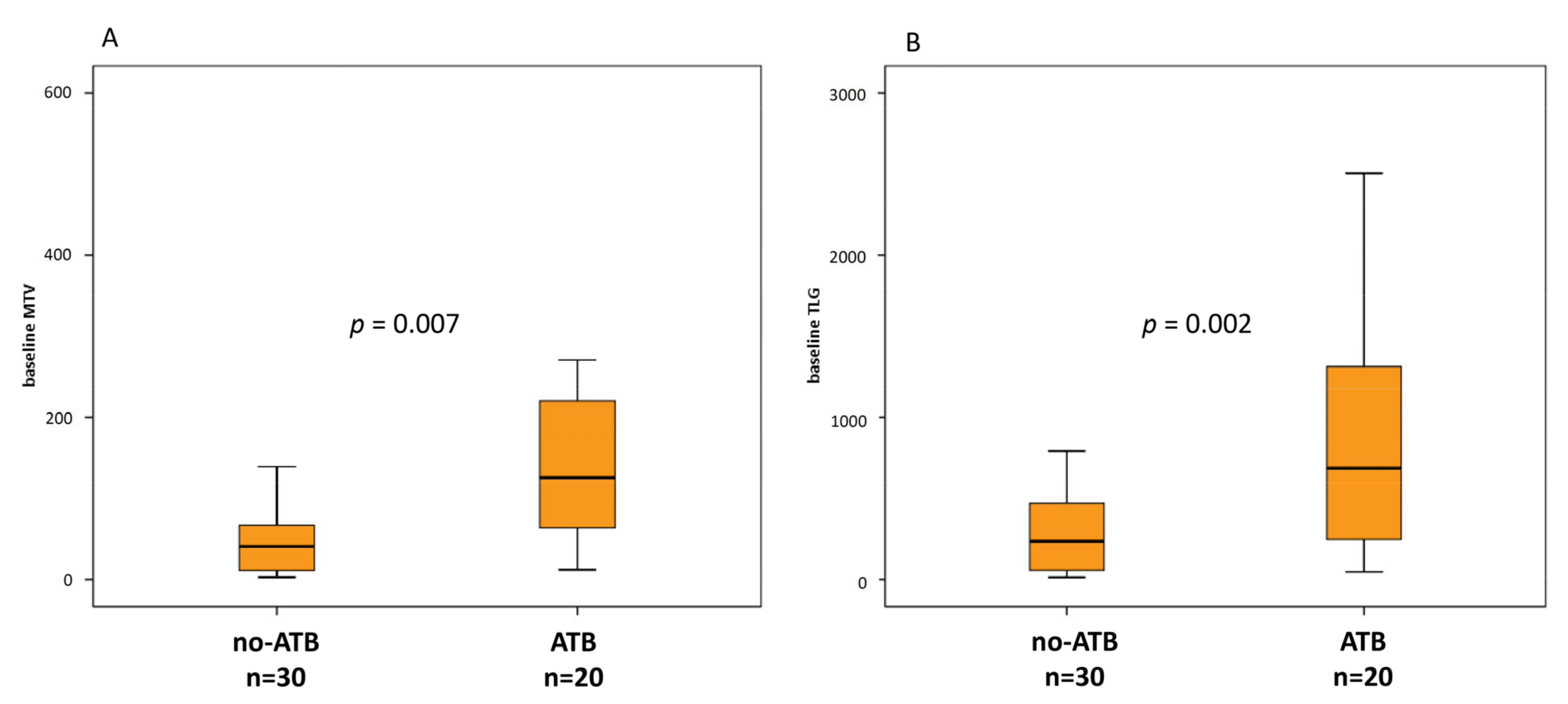
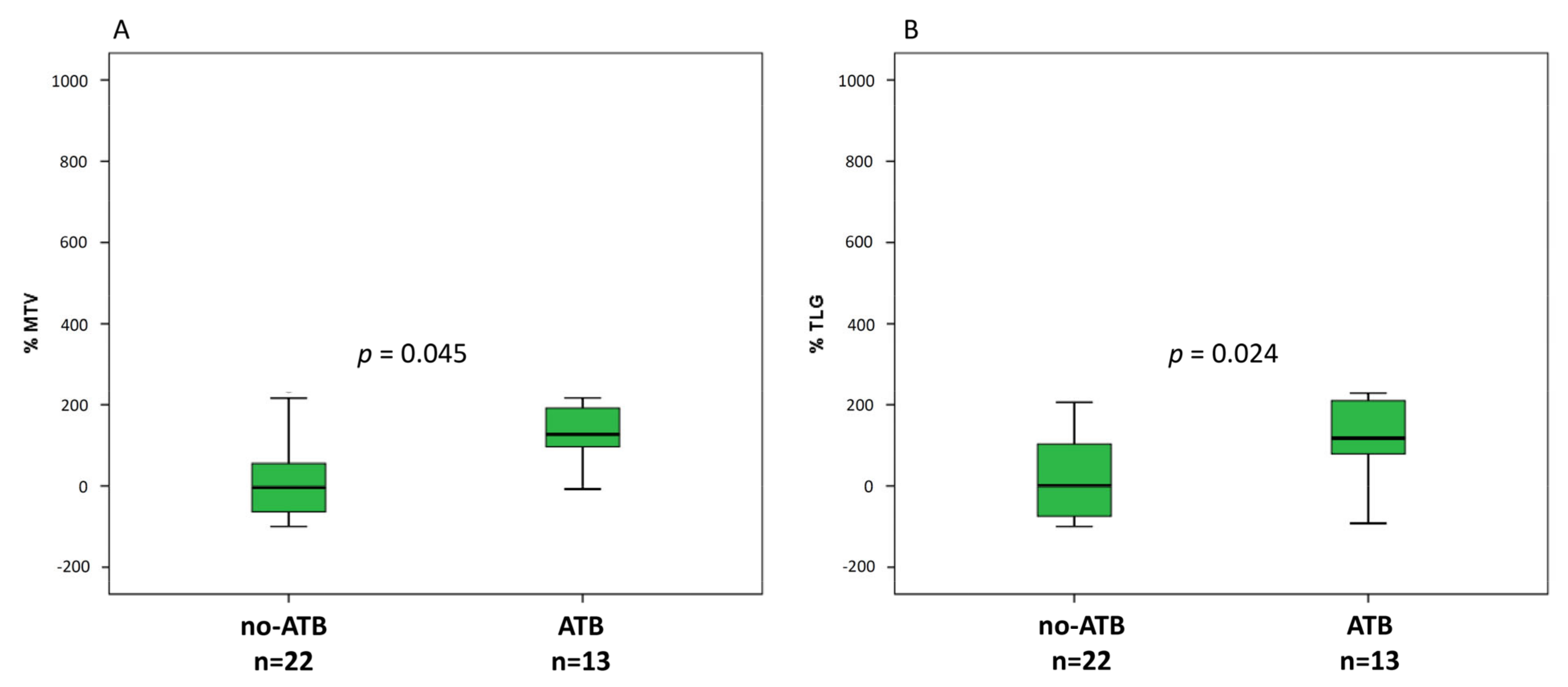
3.2. ATB Therapy and Metabolic Parameters
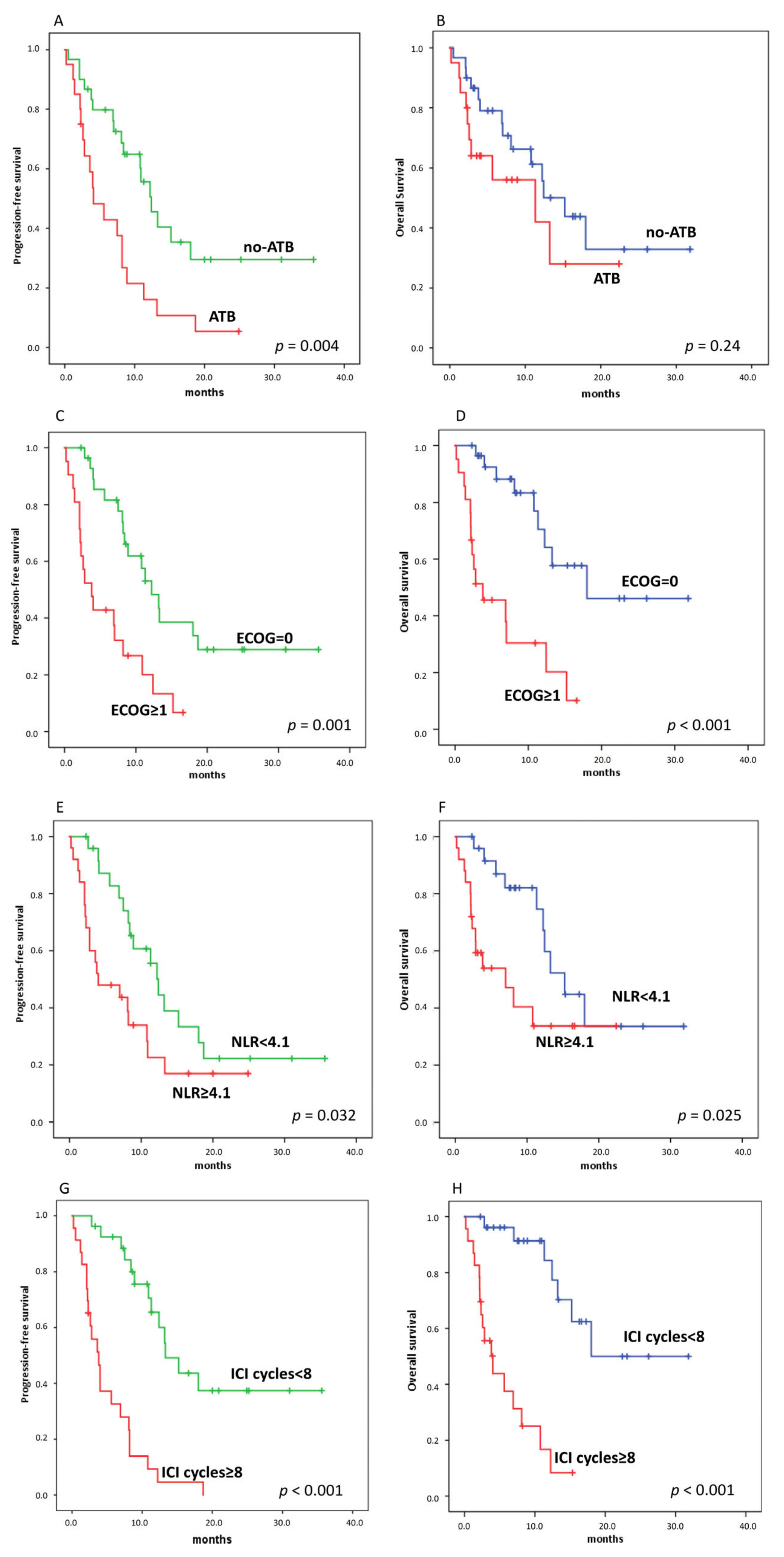
3.3. ATB Therapy and Clinical Outcomes (Progression-Free Survival (PFS) and Overall Survival (OS))
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef] [PubMed]
- R Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus ipilimumab in advanced melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus everolimus in advanced renal-cell carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef] [PubMed]
- Zitvogel, L.; Galluzzi, L.; Viaud, S.; Vétizou, M.; Daillère, R.; Merad, M.; Kroemer, G. Cancer and the gut microbiota: An unexpected link. Sci. Transl. Med. 2015, 7, 271ps1. [Google Scholar] [CrossRef] [PubMed]
- Peterson, D.A.; Frank, D.N.; Pace, N.R.; Gordon, J.I. Metagenomic approaches for defining the pathogenesis of inflammatory bowel diseases. Cell Host Microbe 2008, 3, 417–427. [Google Scholar] [CrossRef]
- Riiser, A. The human microbiome, asthma, and allergy. Allergy Asthma Clin. Immunol. 2015, 11, 35. [Google Scholar] [CrossRef] [PubMed]
- Upadhyaya, S.; Banerjee, G. Type 2 diabetes and gut microbiome: At the intersection of known and unknown. Gut Microbes 2015, 6, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, R.F.; Jobin, C. The microbiome and cancer. Nat. Rev. Cancer 2013, 13, 800–812. [Google Scholar] [CrossRef]
- Chaput, N.; Lepage, P.; Coutzac, C.; Soularue, E.; Le Roux, K.; Monot, C.; Boselli, L.; Routier, E.; Cassard, L.; Collins, M.; et al. Baseline gut microbiota predicts clinical response and colitis in metastatic melanoma patients treated with ipilimumab. Ann. Oncol. 2017, 28, 1368–1379. [Google Scholar] [CrossRef]
- Vétizou, M.; Pitt, J.M.; Daillère, R.; Lepage, P.; Waldschmitt, N.; Flament, C.; Rusakiewicz, S.; Routy, B.; Roberti, M.P.; Duong, C.P.; et al. Anticancer immunotherapy by CTLA-4 blockade relies on the gut microbiota. Science 2015, 350, 1079–1084. [Google Scholar] [CrossRef] [PubMed]
- Routy, B.; Le Chatelier, E.; Derosa, L.; Duong, C.; Alou, M.T.; Daillère, R.; Fluckiger, A.; Messaoudene, M.; Rauber, C.; Roberti, M.P.; et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science 2018, 359, 91–97. [Google Scholar] [CrossRef]
- Matson, V.; Fessler, J.; Bao, R.; Chongsuwat, T.; Zha, Y.; Alegre, M.L.; Luke, J.J.; Gajewski, T.F. The commensal microbiome is associated with anti-PD-1 efficacy in metastatic melanoma patients. Science 2018, 359, 104–108. [Google Scholar] [CrossRef]
- Ferris, R.L.; Blumenschein, G.; Harrington, K.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Vokes, E.; Gillison, M.; Even, C.; et al. Abstract CT022: Evaluation of oral microbiome profiling as a response biomarker in squamous cell carcinoma of the head and neck: Analyses from CheckMate 141. Cancer Res. 2017, 77 (Suppl. S13), CT022. [Google Scholar]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Seymour, L.; Bogaerts, J.; Perrone, A.; Ford, R.; Schwartz, L.H.; Mandrekar, S.; Lin, N.U.; Litière, S.; Dancey, J.; Chen, A.; et al. iRECIST: Guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017, 18, e143–e152. [Google Scholar] [CrossRef]
- Young, H.; Baum, R.; Cremerius, U.; Herholz, K.; Hoekstra, O.; Lammertsma, A.A.; Pruim, J.; Price, P. Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: Review and 1999 EORTC recommendations. European Organization for Research and Treatment of Cancer (EORTC) PET Study Group. Eur. J. Cancer 1999, 35, 1773–1782. [Google Scholar] [CrossRef]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Castello, A.; Rossi, S.; Toschi, L.; Mazziotti, E.; Lopci, E. Hyper-progressive Disease in Patients with Non-Small Cell Lung Cancer Treated with Checkpoint Inhibitors: The Role of 18F-FDG PET/CT. J. Nucl. Med. 2020, 61, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Derosa, L.; Hellmann, M.D.; Spaziano, M.; Halpenny, D.; Fidelle, M.; Rizvi, H.; Long, N.; Plodkowski, A.J.; Arbour, K.C.; Chaft, J.E.; et al. Negative association of antibiotics on clinical activity of immune checkpoint inhibitors in patients with advanced renal cell and non-small-cell lung cancer. Ann. Oncol. 2018, 29, 1437–1444. [Google Scholar] [CrossRef]
- Khan, U.; Peña, C.; Brouwer, J.; Hoffman, K.; Choudhury, A.R.; Zhang, C.; Thakkar, P.; Betel, D.; Sarkar, S.; Sonnenberg, G.; et al. Impact of antibiotic use on response to treatment with immune checkpoint inhibitors. J. Clin. Oncol. 2019, 37 (Suppl. S4), 143. [Google Scholar] [CrossRef]
- Tinsley, N.; Zhou, C.; Tan, G.; Rack, S.; Lorigan, P.; Blackhall, F.; Krebs, M.; Carter, L.; Thistlethwaite, F.; Graham, D.; et al. Cumulative Antibiotic Use Significantly Decreases Efficacy of Checkpoint Inhibitors in Patients with Advanced Cancer. Oncologist 2020, 25, 55–63. [Google Scholar] [CrossRef]
- Pinato, D.J.; Howlett, S.; Ottaviani, D.; Urus, H.; Patel, A.; Mineo, T.; Brock, C.; Power, D.; Hatcher, O.; Falconer, A.; et al. Antibiotic therapy and outcome from immune-checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 287. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Gao, G.; Li, W.; Li, X.; Zhao, C.; Jiang, T.; Jia, Y.; He, Y.; Li, A.; Su, C.; et al. Antibiotics are associated with attenuated efficacy of anti-PD-1/PD-L1 therapies in Chinese patients with advanced non-small cell lung cancer. Lung Cancer 2019, 130, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Huemer, F.; Rinnerthaler, G.; Westphal, T.; Hackl, H.; Hutarew, G.; Gampenrieder, S.P.; Weiss, L.; Greil, R. Impact of antibiotic treatment on immune-checkpoint blockade efficacy in advanced non-squamous non-small cell lung cancer. Oncotarget 2018, 9, 16512–16520. [Google Scholar] [CrossRef]
- Ahmed, J.; Kumar, A.; Parikh, K.; Anwar, A.; Knoll, B.M.; Puccio, C.; Chun, H.; Fanucchi, M.; Lim, S.H. Use of broad-spectrum antibiotics impacts outcome in patients treated with immune checkpoint inhibitors. OncoImmunology 2018, 7, e1507670. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; Howlett, S.; Ottaviani, D.; Urus, H.; Patel, A.; Mineo, T.; Brock, C.; Power, D.; Hatcher, O.; Falconer, A.; et al. Association of prior antibiotic treatment with survival and response to immune checkpoint inhibitor therapy in patients with cancer. JAMA Oncol. 2019, 5, 1774–1778. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.C.; Lin, C.C.; Lin, C.Y.; Hsieh, M.S.; Kuo, H.Y.; Lien, M.Y.; Shao, Y.Y.; Huang, T.C.; Hsu, C.H. Neutrophil-to-lymphocyte Ratio and Use of Antibiotics Associated with Prognosis in Esophageal Squamous Cell Carcinoma Patients Receiving Immune Checkpoint Inhibitors. Anticancer Res. 2019, 39, 5675–5682. [Google Scholar] [CrossRef]
- Huang, A.C.; Postow, M.A.; Orlowski, R.J.; Mick, R.; Bengsch, B.; Manne, S.; Xu, W.; Harmon, S.; Giles, J.R.; Wenz, B.; et al. T-cell invigoration to tumour burden ratio associated with anti-PD-1 response. Nature 2017, 545, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Cheng, G.; Huang, H. Prognostic Value of 18F-Fluorodeoxyglucose PET/Computed Tomography in Non-Small-Cell Lung Cancer. PET Clin. 2018, 13, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Dumenil, C.; Massiani, M.A.; Dumoulin, J.; Giraud, V.; Labrune, S.; Chinet, T.; Giroux Leprieur, E. Clinical factors associated with early progression and grade 3-4 toxicity in patients with advanced non-small-cell lung cancers treated with nivolumab. PLoS ONE 2018, 13, e0195945. [Google Scholar] [CrossRef]
- Diem, S.; Schmid, S.; Krapf, M.; Flatz, L.; Born, D.; Jochum, W.; Templeton, A.J.; Fueh, M. Neutrophil-to-Lymphocyte ratio (NLR) and Platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer 2017, 111, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Castello, A.; Toschi, L.; Rossi, S.; Mazziotti, E.; Lopci, E. The immune-metabolic-prognostic index and clinical outcomes in patients with non-small cell lung carcinoma under checkpoint inhibitors. J. Cancer Res. Clin. Oncol. 2020, 146, 1235–1243. [Google Scholar] [CrossRef] [PubMed]
- Ouaknine Krief, J.; Helly de Tauriers, P.; Dumenil, C.; Neveux, N.; Dumoulin, J.; Giraud, V.; Labrune, S.; Tisserand, J.; Julie, C.; Emile, J.F.; et al. Role of antibiotic use, plasma citrulline and blood microbiome in advanced non-small cell lung cancer patients treated with nivolumab. J. Immunother. Cancer 2019, 7, 176. [Google Scholar] [CrossRef]
- Kaderbhai, C.; Richard, C.; Fumet, J.D.; Aarnink, A.; Foucher, P.; Coudert, B.; Favier, L.; Lagrange, A.; Limagne, E.; Boidot, R.; et al. Antibiotic Use Does Not Appear to Influence Response to Nivolumab. Anticancer Res. 2017, 37, 3195–3200. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients n = 50 (%) | ATB n = 20 (%) | no-ATB n = 30 (%) | p | |
|---|---|---|---|---|
| Age | 0.77 | |||
| <73 | 25 (50) | 11 (55) | 14 (46.7) | |
| ≥73 | 25 (50) | 9 (45) | 16 (53.3) | |
| Gender | 0.76 | |||
| male | 34 (68) | 13 (65) | 21 (70) | |
| female | 16 (32) | 7 (35) | 9 (30) | |
| ECOG performance status | ||||
| 0 | 29 (58) | 12 (60) | 17 (56.7) | 0.82 |
| ≥1 | 21 (42) | 8 (40) | 13 (43.3) | |
| Smoking status | >0.99 | |||
| Current/former | 44 (88) | 26 (86.7) | 18 (90) | |
| None | 6 (12) | 4 (13.3) | 2 (10) | |
| Prior lines of treatment | ||||
| 0 | 12 (24) | 5 (25) | 7 (23.3) | 0.32 |
| 1 | 25 (50) | 12 (60) | 13 (43.4) | |
| 2 | 11 (22) | 3 (15) | 8 (26.7) | |
| 3 | 2 (4) | 0 | 2 (6.6) | |
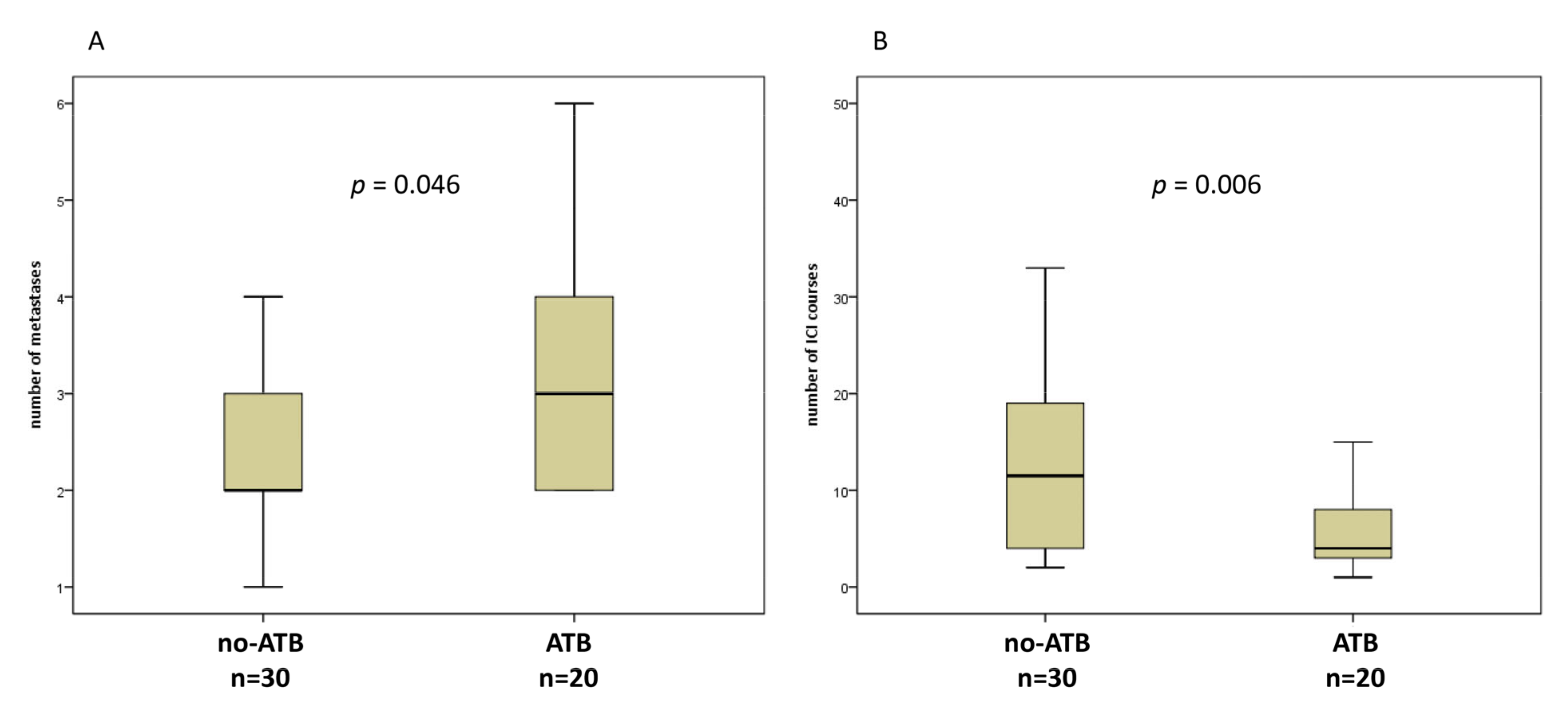
| Metastatic sites (median) | 0.046 | |||
| ≤2 | 26 (52) | 7 (35) | 19 (63.3) | |
| >2 | 24 (48) | 13 (65) | 11 (36.7) | |
| Histology | 0.32 | |||
| Non-squamous | 31 (62) | 10 (50) | 21 (70) | |
| Squamous others | 14 (28) 5 (0.1) | 7 (35) | 7 (23.3) | |
| Tumor PD-L1 status | 0.83 | |||
| negative | 9 (18) | 3 (15) | 6 (20) | |
| positive 1–49% | 8 (16) | 5 (25) | 3 (10) | |
| positive ≥50% | 10 (20) | 3 (15) | 7 (23.3) | |
| missing | 23 (46) | 9 (45) | 14 (46.7) | |
| Cycles of ICI (median) | 8 | 4 | 12 | |
| range | (1–47) | (1–32) | (2–47) | 0.006 |
| WBC (median) | 7.8 | 8.5 | 7.8 | |
| range | (3.8–24.5) | (4.3–24.5) | (3.8–21.3) | 0.32 |
| NLR (median) | 4.1 | 4.6 | 4.1 | |
| range | (0.81–32) | (0.81–32) | (1.3–13.2) | 0.31 |
| Platelets (median) | 248 | 270 | 248 | |
| range | (118–517) | (144–517) | (118–449) | 0.08 |
| Variable | All Patients (n = 50) | ATB (n = 20) | No-ATB (n = 30) | p |
| SUVmax_baseline | 13.7 (4.9–35.7) | 16.9 (4.9–35.7) | 13.5 (5.3–25.7) | 0.076 |
| SUVmean_baseline | 5.9 (3.2–10.3) | 6 (3.2–9.8) | 5.9 (3.4–10.3) | 0.572 |
| MTV_baseline | 63.7 (2.7–1772) | 125.6 (2.7–1772) | 40.6 (12–1323.7) | 0.007 |
| TLG_baseline | 330.1 (12.3–2504) | 687 (46.5–2504.1) | 235.3 (12.3–1645.4) | 0.002 |
| All patients (n = 35) | ATB (n = 13) | no-ATB (n = 22) | ||
| ∆SUVmax | −16.9 (−100 +144.5) | −18.9 (−61 +144.5) | −8.1 (−100 +107.1) | 0.555 |
| ∆SUVmean | −1.8 (−100 +130) | −4.1 (−58.2 +130) | 0 (−100 +104.9) | >0.99 |
| ∆MTV | 67.7 (−100 +1245.1) | 127.3 (−81.3 +755.5) | −3.7 (−100 +1245.1) | 0.045 |
| ∆TLG | 36.5 (−100 +1295.2) | 117.6 (−92.1 +505.5) | −0.8 (−100 +1295.2) | 0.024 |
| Parameters | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% IC | p Value | Hazard Ratio | 95% IC | p Value | |
| Age (<73 vs. ≥73) | 1.2 | 0.6–2.3 | 0.61 | - | - | - |
| ECOG (0 vs. 1–2) | 3.2 | 1.6–6.4 | 0.001 | 5.0 | 1.9–13.7 | 0.002 |
| Number of metastases (≥2) | 3.1 | 1.6–6.1 | 0.001 | - | - | - |
| no-ATB vs. ATB | 2.6 | 1.3–5.0 | 0.006 | 4.2 | 1.6–11.3 | 0.004 |
| NLR (<4.1) | 0.5 | 0.25–0.95 | 0.04 | - | - | - |
| SUVmax_baseline (≥13.6) | 0.9 | 0.5–1.8 | 0.75 | - | - | - |
| SUVmean_baseline (≥5.9) | 0.9 | 1.0–1.7 | 0.75 | - | - | - |
| TLG_baseline (≥330.1) | 1.8 | 0.9–3.6 | 0.08 | - | - | - |
| MTV_baseline (≥63.7) | 2.5 | 1.2–4.8 | 0.01 | - | - | - |
| ∆SUVmax (<−16.9) | 2.9 | 1.2–6.8 | 0.015 | 4.2 | 1.6-10.6 | 0.003 |
| ∆SUVmean (<−1.75) | 1.9 | 0.8–4.3 | 0.13 | - | - | - |
| ∆TLG (<67.7) | 3.1 | 1.3–7.4 | 0.013 | - | - | - |
| ∆MTV (<36.4) | 3.3 | 1.4–8.0 | 0.008 | - | - | - |
| Parameters | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% IC | p Value | Hazard Ratio | 95% IC | p Value | |
| Age (<73 vs. ≥73) | 1.0 | 0.5–2.3 | 0.91 | - | - | - |
| ECOG (0 vs. 1–2) | 5.1 | 2.1–12.3 | <0.001 | 4.0 | 1.3–12.1 | 0.015 |
| Number of metastases (≥2) | 2.6 | 1.1–5.9 | 0.023 | - | - | - |
| no-ATB vs. ATB | 1.6 | 0.7–53.7 | 0.25 | - | - | - |
| NLR (<4.1) | 0.4 | 0.18–0.92 | 0.03 | 0.3 | 0.08–0.88 | 0.03 |
| SUVmax_baseline (≥13.6) | 0.9 | 0.4–2.0 | 0.75 | - | - | - |
| SUVmean_baseline (≥5.9) | 0.8 | 0.4–1.9 | 0.71 | - | - | - |
| TLG_baseline (≥330.1) | 1.5 | 0.7–3.6 | 0.27 | - | - | - |
| MTV_baseline (≥63.7) | 2.3 | 1.0–5.3 | 0.04 | - | - | - |
| ∆SUVmax (<−16.9) | 5.1 | 1.5–18.1 | 0.011 | 7.2 | 1.8–28.6 | 0.005 |
| ∆SUVmean (<−1.75) | 3.0 | 0.9–9.3 | 0.06 | - | - | - |
| ∆TLG (<67.7) | 2.0 | 0.7–5.5 | 0.18 | - | - | - |
| ∆MTV (<36.4) | 2.8 | 1–8.2 | 0.06 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castello, A.; Rossi, S.; Toschi, L.; Lopci, E. Impact of Antibiotic Therapy and Metabolic Parameters in Non-Small Cell Lung Cancer Patients Receiving Checkpoint Inhibitors. J. Clin. Med. 2021, 10, 1251. https://doi.org/10.3390/jcm10061251
Castello A, Rossi S, Toschi L, Lopci E. Impact of Antibiotic Therapy and Metabolic Parameters in Non-Small Cell Lung Cancer Patients Receiving Checkpoint Inhibitors. Journal of Clinical Medicine. 2021; 10(6):1251. https://doi.org/10.3390/jcm10061251
Chicago/Turabian StyleCastello, Angelo, Sabrina Rossi, Luca Toschi, and Egesta Lopci. 2021. "Impact of Antibiotic Therapy and Metabolic Parameters in Non-Small Cell Lung Cancer Patients Receiving Checkpoint Inhibitors" Journal of Clinical Medicine 10, no. 6: 1251. https://doi.org/10.3390/jcm10061251
APA StyleCastello, A., Rossi, S., Toschi, L., & Lopci, E. (2021). Impact of Antibiotic Therapy and Metabolic Parameters in Non-Small Cell Lung Cancer Patients Receiving Checkpoint Inhibitors. Journal of Clinical Medicine, 10(6), 1251. https://doi.org/10.3390/jcm10061251