
Post-Transplant Cyclophosphamide and Tacrolimus—Mycophenolate Mofetil Combination Governs GVHD and Immunosuppression Need, Reducing Late Toxicities in Allogeneic Peripheral Blood Hematopoietic Cell Transplantation from HLA-Matched Donors

 ,
,  , , ,
, , , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Conditioning Regimen, Postgraft Immunosuppression, and Supportive Care
2.2. Monitoring after Transplant
2.3. Long Term Follow-Up
2.4. Statistical Analyses
3. Results
3.1. Engraftment
3.2. Infections
3.3. Long-Term Toxicity
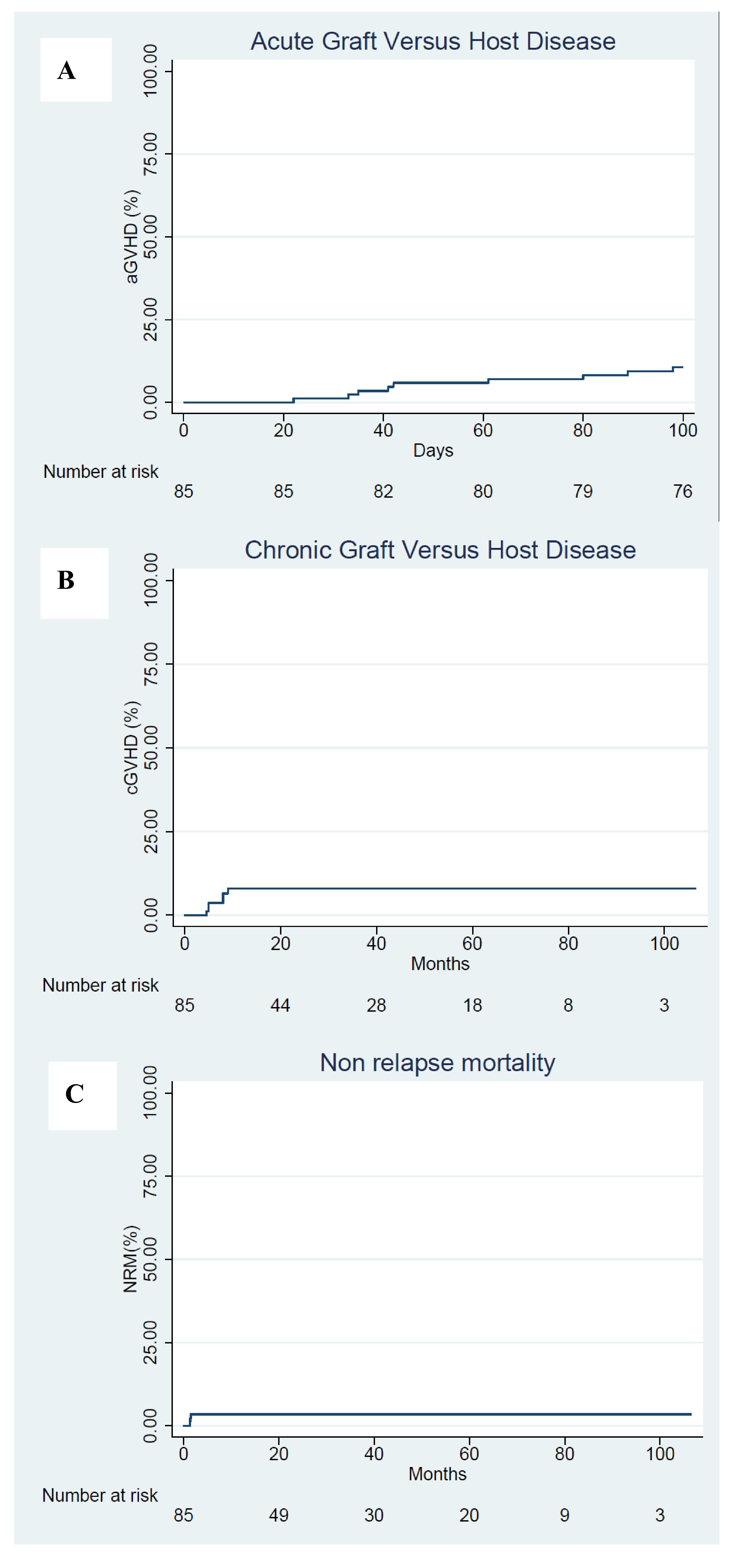
3.4. GVHD
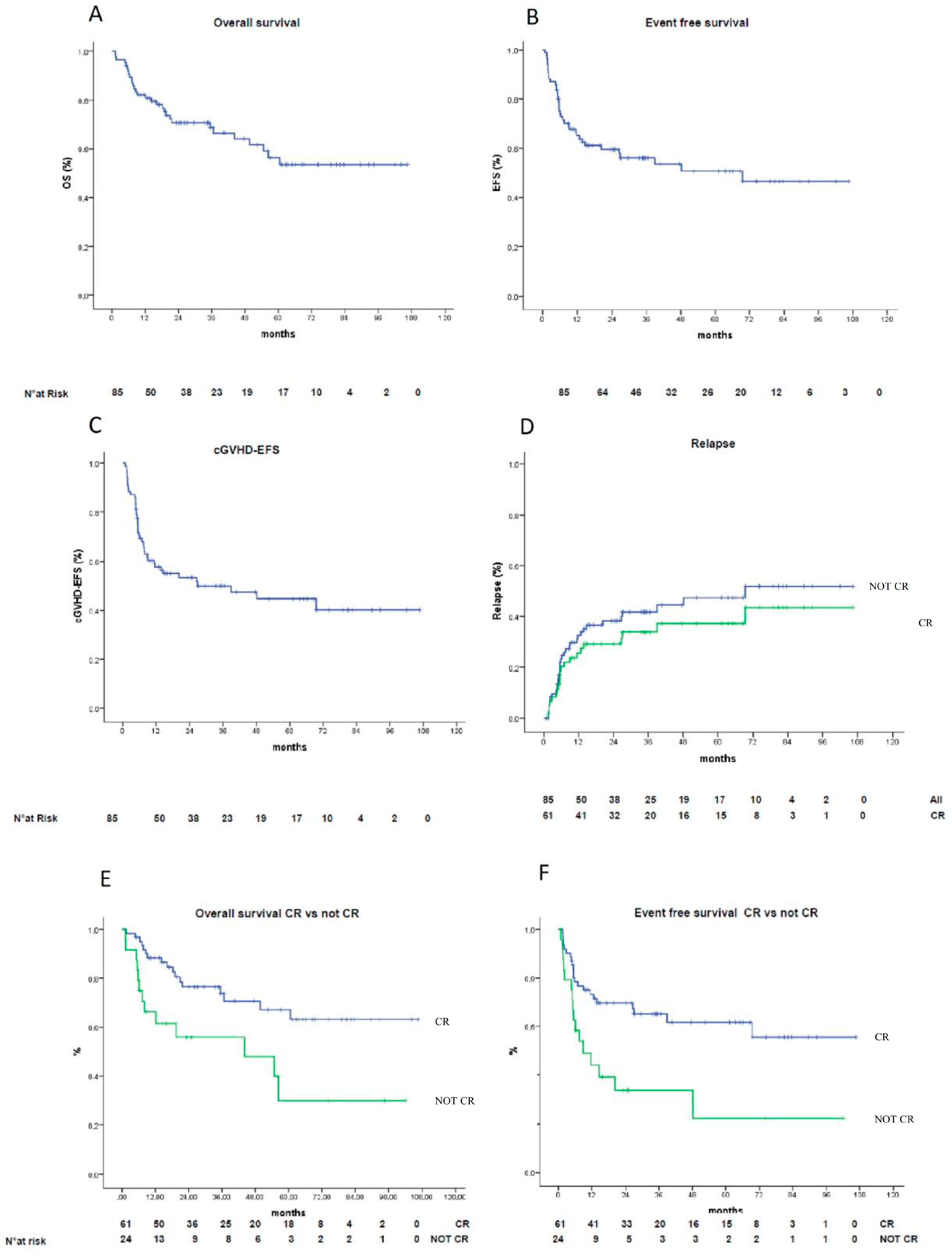
3.5. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- June, C.H.; O’Connor, R.S.; Kawalekar, O.U.; Ghassemi, S.; Milone, M.C. CAR T cell immunotherapy for human cancer. Science 2018, 359, 1361–1365. [Google Scholar] [CrossRef] [PubMed]
- Storb, R.; Gyurkocza, B.; Storer, B.E.; Sorror, M.L.; Blume, K.; Niederwieser, D.; Chauncey, T.R.; Pulsipher, M.A.; Petersen, F.B.; Sahebi, F.; et al. Graft-versus-host disease and graft-versus-tumor effects after allogeneic hematopoietic cell transplantation. J. Clin. Oncol. 2013, 31, 1530–1538. [Google Scholar] [CrossRef]
- Appelbaum, F.R. Hematopoietic-cell transplantation at 50. N. Engl. J. Med. 2007, 357, 1472–1475. [Google Scholar] [CrossRef] [PubMed]
- Gooley, T.A.; Chien, J.W.; Pergam, S.A.; Hingorani, S.; Sorror, M.L.; Boeckh, M.; Martin, P.J.; Sandmaier, B.M.; Marr, K.A.; Appelbaum, F.R.; et al. Reduced mortality after allogeneic hematopoietic-cell transplantation. N. Engl. J. Med. 2010, 363, 2091–2101. [Google Scholar] [CrossRef]
- McDonald, G.B.; Sandmaier, B.M.; Mielcarek, M.; Sorror, M.; Pergam, S.A.; Cheng, G.S.; Hingorani, S.; Boeckh, M.; Flowers, M.D.; Lee, S.J.; et al. Survival, Nonrelapse Mortality, and Relapse-Related Mortality After Allogeneic Hematopoietic Cell Transplantation: Comparing 2003–2007 Versus 2013–2017 Cohorts. Ann. Intern. Med. 2020, 172, 229–239. [Google Scholar] [CrossRef]
- Gratwohl, A.; Pasquini, M.C.; Aljurf, M.; Atsuta, Y.; Baldomero, H.; Foeken, L.; Gratwohl, M.; Bouzas, L.F.; Confer, D.; Frauendorfer, K.; et al. One million haemopoietic stem-cell transplants: A retrospective observational study. Lancet Haematol. 2015, 2, e91–e100. [Google Scholar] [CrossRef]
- Shouval, R.; Fein, J.A.; Labopin, M.; Kröger, N.; Duarte, R.F.; Bader, P.; Chabannon, C.; Kuball, J.; Basak, G.W.; Dufour, C.; et al. Outcomes of allogeneic haematopoietic stem cell transplantation from HLA-matched and alternative donors: A European Society for Blood and Marrow Transplantation registry retrospective analysis. Lancet Haematol. 2019, 6, e573–e584. [Google Scholar] [CrossRef]
- Flowers, M.E.; Inamoto, Y.; Carpenter, P.A.; Lee, S.J.; Kiem, H.P.; Petersdorf, E.W.; Pereira, S.E.; Nash, R.A.; Mielcarek, M.; Fero, M.L.; et al. Comparative analysis of risk factors for acute graft-versus-host disease and for chronic graft-versus-host disease according to National Institutes of Health consensus criteria. Blood 2011, 117, 3214–3219. [Google Scholar] [CrossRef] [PubMed]
- Penack, O.; Marchetti, M.; Ruutu, T.; Aljurf, M.; Bacigalupo, A.; Bonifazi, F.; Ciceri, F.; Cornelissen, J.; Malladi, R.; Duarte, R.F.; et al. Prophylaxis and management of graft versus host disease after stem-cell transplantation for haematological malignancies: Updated consensus recommendations of the European Society for Blood and Marrow Transplantation. Lancet Haematol. 2020, 7, e157–e167. [Google Scholar] [CrossRef]
- Harris, A.C.; Levine, J.E.; Ferrara, J.L. Have we made progress in the treatment of GVHD? Best Pract. Res. Clin. Haematol. 2012, 25, 473–478. [Google Scholar] [CrossRef][Green Version]
- Storb, R.; Deeg, H.J.; Whitehead, J.; Appelbaum, F.; Beatty, P.; Bensinger, W.; Buckner, C.D.; Clift, R.; Doney, K.; Farewell, V. Methotrexate and cyclosporine compared with cyclosporine alone for prophylaxis of acute graft versus host disease after marrow transplantation for leukemia. N. Engl. J. Med. 1986, 314, 729–735. [Google Scholar] [CrossRef]
- Nash, R.A.; Antin, J.H.; Karanes, C.; Fay, J.W.; Avalos, B.R.; Yeager, A.M.; Przepiorka, D.; Davies, S.; Petersen, F.B.; Bartels, P.; et al. Phase 3 study comparing methotrexate and tacrolimus with methotrexate and cyclosporine for prophylaxis of acute graft-versus-host disease after marrow transplantation from unrelated donors. Blood 2000, 96, 2062–2068. [Google Scholar]
- Finke, J.; Bethge, W.A.; Schmoor, C.; Ottinger, H.D.; Stelljes, M.; Zander, A.R.; Volin, L.; Ruutu, T.; Heim, D.A.; Schwerdtfeger, R.; et al. Standard graft-versus-host disease prophylaxis with or without anti-T-cell globulin in haematopoietic cell transplantation from matched unrelated donors: A randomised, open-label, multicentre phase 3 trial. Lancet Oncol. 2009, 10, 855–864. [Google Scholar] [CrossRef]
- Kröger, N.; Solano, C.; Bonifazi, F. Antilymphocyte Globulin for Chronic Graft-versus-Host Disease. N. Engl. J. Med. 2016, 374, 1894–1895. [Google Scholar] [CrossRef]
- Soiffer, R.J.; Kim, H.T.; McGuirk, J.; Horwitz, M.E.; Johnston, L.; Patnaik, M.M.; Rybka, W.; Artz, A.; Porter, D.L.; Shea, T.C.; et al. Prospective, Randomized, Double-Blind, Phase III Clinical Trial of Anti-T-Lymphocyte Globulin to Assess Impact on Chronic Graft-Versus-Host Disease-Free Survival in Patients Undergoing HLA-Matched Unrelated Myeloablative Hematopoietic Cell Transplantation. J. Clin. Oncol. 2017, 35, 4003–4011. [Google Scholar] [CrossRef]
- Walker, I.; Panzarella, T.; Couban, S.; Couture, F.; Devins, G.; Elemary, M.; Gallagher, G.; Kerr, H.; Kuruvilla, J.; Lee, S.J.; et al. Pretreatment with anti-thymocyte globulin versus no anti-thymocyte globulin in patients with haematological malignancies undergoing haemopoietic cell transplantation from unrelated donors: A randomised, controlled, open-label, phase 3, multicentre trial. Lancet Oncol. 2016, 17, 164–173. [Google Scholar] [CrossRef]
- Strauss, G.; Osen, W.; Debatin, K.M. Induction of apoptosis and modulation of activation and effector function in T cells by immunosuppressive drugs. Clin. Exp. Immunol. 2002, 128, 255–266. [Google Scholar] [CrossRef]
- Luznik, L.; O’Donnell, P.V.; Symons, H.J.; Chen, A.R.; Leffell, M.S.; Zahurak, M.; Gooley, T.A.; Piantadosi, S.; Kaup, M.; Ambinder, R.F.; et al. HLA-haploidentical bone marrow transplantation for hematologic malignancies using nonmyeloablative conditioning and high-dose, posttransplantation cyclophosphamide. Biol. Blood Marrow Transplant. 2008, 14, 641–650. [Google Scholar] [CrossRef]
- Kanakry, C.G.; Tsai, H.L.; Bolaños-Meade, J.; Smith, B.D.; Gojo, I.; Kanakry, J.A.; Kasamon, Y.L.; Gladstone, D.E.; Matsui, W.; Borrello, I.; et al. Single-agent GVHD prophylaxis with posttransplantation cyclophosphamide after myeloablative, HLA-matched BMT for AML, ALL, and MDS. Blood 2014, 124, 3817–3827. [Google Scholar] [CrossRef]
- Luznik, L.; Bolaños-Meade, J.; Zahurak, M.; Chen, A.R.; Smith, B.D.; Brodsky, R.; Huff, C.A.; Borrello, I.; Matsui, W.; Powell, J.D.; et al. High-dose cyclophosphamide as single-agent, short-course prophylaxis of graft-versus-host disease. Blood 2010, 115, 3224–3230. [Google Scholar] [CrossRef]
- Anasetti, C.; Logan, B.R.; Lee, S.J.; Waller, E.K.; Weisdorf, D.J.; Wingard, J.R.; Cutler, C.S.; Westervelt, P.; Woolfrey, A.; Couban, S.; et al. Peripheral-blood stem cells versus bone marrow from unrelated donors. N. Engl. J. Med. 2012, 367, 1487–1496. [Google Scholar] [CrossRef] [PubMed]
- Alousi, A.M.; Brammer, J.E.; Saliba, R.M.; Andersson, B.; Popat, U.; Hosing, C.; Jones, R.; Shpall, E.J.; Khouri, I.; Qazilbash, M.; et al. Phase II Trial of Graft-versus-Host Disease Prophylaxis with Post-Transplantation Cyclophosphamide after Reduced-Intensity Busulfan/Fludarabine Conditioning for Hematological Malignancies. Biol. Blood Marrow Transplant. 2015, 21, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Holtick, U.; Chemnitz, J.M.; Shimabukuro-Vornhagen, A.; Theurich, S.; Chakupurakal, G.; Krause, A.; Fiedler, A.; Luznik, L.; Hellmich, M.; Wolf, D.; et al. OCTET-CY: A phase II study to investigate the efficacy of post-transplant cyclophosphamide as sole graft-versus-host prophylaxis after allogeneic peripheral blood stem cell transplantation. Eur. J. Haematol. 2016, 96, 27–35. [Google Scholar] [CrossRef]
- Moiseev, I.S.; Pirogova, O.V.; Alyanski, A.L.; Babenko, E.V.; Gindina, T.L.; Darskaya, E.I.; Slesarchuk, O.A.; Bondarenko, S.N.; Afanasyev, B.V. Graft-versus-Host Disease Prophylaxis in Unrelated Peripheral Blood Stem Cell Transplantation with Post-Transplantation Cyclophosphamide, Tacrolimus, and Mycophenolate Mofetil. Biol. Blood Marrow Transplant. 2016, 22, 1037–1042. [Google Scholar] [CrossRef]
- Mielcarek, M.; Furlong, T.; O’Donnell, P.V.; Storer, B.E.; McCune, J.S.; Storb, R.; Carpenter, P.A.; Flowers, M.E.; Appelbaum, F.R.; Martin, P.J. Posttransplantation cyclophosphamide for prevention of graft-versus-host disease after HLA-matched mobilized blood cell transplantation. Blood 2016, 127, 1502–1508. [Google Scholar] [CrossRef]
- Carnevale-Schianca, F.; Caravelli, D.; Gallo, S.; Coha, V.; D’Ambrosio, L.; Vassallo, E.; Fizzotti, M.; Nesi, F.; Gioeni, L.; Berger, M.; et al. Post-Transplant Cyclophosphamide and Tacrolimus-Mycophenolate Mofetil Combination Prevents Graft-versus-Host Disease in Allogeneic Peripheral Blood Hematopoietic Cell Transplantation from HLA-Matched Donors. Biol. Blood Marrow Transplant. 2017, 23, 459–466. [Google Scholar] [CrossRef]
- Choi, S.W.; Reddy, P. Current and emerging strategies for the prevention of graft-versus-host disease. Nat. Rev. Clin. Oncol. 2014, 11, 536–547. [Google Scholar] [CrossRef] [PubMed]
- Przepiorka, D.; Weisdorf, D.; Martin, P.; Klingemann, H.G.; Beatty, P.; Hows, J.; Thomas, E.D. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995, 15, 825–828. [Google Scholar]
- Lee, S.J.; Vogelsang, G.; Flowers, M.E. Chronic graft-versus-host disease. Biol. Blood Marrow. Transplant. 2003, 9, 215–233. [Google Scholar] [CrossRef]
- Filipovich, A.H.; Weisdorf, D.; Pavletic, S.; Socie, G.; Wingard, J.R.; Lee, S.J.; Martin, P.; Chien, J.; Przepiorka, D.; Couriel, D.; et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol. Blood Marrow Transplant. 2005, 11, 945–956. [Google Scholar] [CrossRef]
- Armand, P.; Kim, H.T.; Logan, B.R.; Wang, Z.; Alyea, E.P.; Kalaycio, M.E.; Maziarz, R.T.; Antin, J.H.; Soiffer, R.J.; Weisdorf, D.J.; et al. Validation and refinement of the Disease Risk Index for allogeneic stem cell transplantation. Blood 2014, 123, 3664–3671. [Google Scholar] [CrossRef] [PubMed]
- Majhail, N.S.; Rizzo, J.D.; Lee, S.J.; Aljurf, M.; Atsuta, Y.; Bonfim, C.; Burns, L.J.; Chaudhri, N.; Davies, S.; Okamoto, S.; et al. Recommended screening and preventive practices for long-term survivors after hematopoietic cell transplantation. Bone Marrow Transplant. 2012, 47, 337–341. [Google Scholar] [CrossRef]
- Kanakry, C.G.; Bolaños-Meade, J.; Kasamon, Y.L.; Zahurak, M.; Durakovic, N.; Furlong, T.; Mielcarek, M.; Medeot, M.; Gojo, I.; Smith, B.D.; et al. Low immunosuppressive burden after HLA-matched related or unrelated BMT using posttransplantation cyclophosphamide. Blood 2017, 129, 1389–1393. [Google Scholar] [CrossRef] [PubMed]
- Inamoto, Y.; Flowers, M.E.; Sandmaier, B.M.; Aki, S.Z.; Carpenter, P.A.; Lee, S.J.; Storer, B.E.; Martin, P.J. Failure-free survival after initial systemic treatment of chronic graft-versus-host disease. Blood 2014, 124, 1363–1371. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Maude, S.L.; Laetsch, T.W.; Buechner, J.; Rives, S.; Boyer, M.; Bittencourt, H.; Bader, P.; Verneris, M.R.; Stefanski, H.E.; Myers, G.D.; et al. Tisagenlecleucel in Children and Young Adults with B-Cell Lymphoblastic Leukemia. N. Engl. J. Med. 2018, 378, 439–448. [Google Scholar] [CrossRef]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jäger, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef]
- Raje, N.; Berdeja, J.; Lin, Y.; Siegel, D.; Jagannath, S.; Madduri, D.; Liedtke, M.; Rosenblatt, J.; Maus, M.V.; Turka, A.; et al. Anti-BCMA CAR T-Cell Therapy bb2121 in Relapsed or Refractory Multiple Myeloma. N. Engl. J. Med. 2019, 380, 1726–1737. [Google Scholar] [CrossRef]
- Kantarjian, H.; Jabbour, E.; Topp, M.S. Blinatumomab for Acute Lymphoblastic Leukemia. N. Engl. J. Med. 2017, 376, e49. [Google Scholar] [CrossRef]
- Kantarjian, H.; Stein, A.; Gökbuget, N.; Fielding, A.K.; Schuh, A.C.; Ribera, J.M.; Wei, A.; Dombret, H.; Foà, R.; Bassan, R.; et al. Blinatumomab versus Chemotherapy for Advanced Acute Lymphoblastic Leukemia. N. Engl. J. Med. 2017, 376, 836–847. [Google Scholar] [CrossRef]
- Amirouchene-Angelozzi, N.; Swanton, C.; Bardelli, A. Tumor Evolution as a Therapeutic Target. Cancer Discov. 2017. [Google Scholar] [CrossRef]
- Campbell, J.D.; Whittington, M.D. Paying for CAR-T Therapy Amidst Limited Health System Resources. J. Clin. Oncol. 2019, 37, 2095–2097. [Google Scholar] [CrossRef]
- Khera, N.; Deeg, H.J.; Kodish, E.; Rondelli, D.; Majhail, N. Allogeneic Hematopoietic Cell Transplantation and Other Expensive Cellular Therapies: A Miracle for the Few but Off Limits to Many? J. Clin. Oncol. 2020, 38, 1268–1272. [Google Scholar] [CrossRef]
- Kanakry, C.G.; O’Donnell, P.V.; Furlong, T.; de Lima, M.J.; Wei, W.; Medeot, M.; Mielcarek, M.; Champlin, R.E.; Jones, R.J.; Thall, P.F.; et al. Multi-institutional study of post-transplantation cyclophosphamide as single-agent graft-versus-host disease prophylaxis after allogeneic bone marrow transplantation using myeloablative busulfan and fludarabine conditioning. J. Clin. Oncol. 2014, 32, 3497–3505. [Google Scholar] [CrossRef]
- Sandmaier, B.M.; Kornblit, B.; Storer, B.E.; Olesen, G.; Maris, M.B.; Langston, A.A.; Gutman, J.A.; Petersen, S.L.; Chauncey, T.R.; Bethge, W.A.; et al. Addition of sirolimus to standard cyclosporine plus mycophenolate mofetil-based graft-versus-host disease prophylaxis for patients after unrelated non-myeloablative haemopoietic stem cell transplantation: A multicentre, randomised, phase 3 trial. Lancet Haematol. 2019, 6, e409–e418. [Google Scholar] [CrossRef]
- Pidala, J.; Martens, M.; Anasetti, C.; Carreras, J.; Horowitz, M.; Lee, S.J.; Antin, J.; Cutler, C.; Logan, B. Factors Associated with Successful Discontinuation of Immune Suppression after Allogeneic Hematopoietic Cell Transplantation. JAMA Oncol. 2019. [Google Scholar] [CrossRef]
- Mielcarek, M.; Furlong, T.; Storer, B.E.; Green, M.L.; McDonald, G.B.; Carpenter, P.A.; Flowers, M.E.; Storb, R.; Boeckh, M.; Martin, P.J. Effectiveness and safety of lower dose prednisone for initial treatment of acute graft-versus-host disease: A randomized controlled trial. Haematologica 2015, 100, 842–848. [Google Scholar] [CrossRef]
- Bonifazi, F.; Solano, C.; Wolschke, C.; Sessa, M.; Patriarca, F.; Zallio, F.; Nagler, A.; Selleri, C.; Risitano, A.M.; Messina, G.; et al. Acute GVHD prophylaxis plus ATLG after myeloablative allogeneic haemopoietic peripheral blood stem-cell transplantation from HLA-identical siblings in patients with acute myeloid leukaemia in remission: Final results of quality of life and long-term outcome analysis of a phase 3 randomised study. Lancet Haematol. 2019, 6, e89–e99. [Google Scholar] [CrossRef]
- Finke, J.; Schmoor, C.; Bethge, W.A.; Ottinger, H.; Stelljes, M.; Volin, L.; Heim, D.; Bertz, H.; Grishina, O.; Socie, G. Long-term outcomes after standard graft-versus-host disease prophylaxis with or without anti-human-T-lymphocyte immunoglobulin in haemopoietic cell transplantation from matched unrelated donors: Final results of a randomised controlled trial. Lancet Haematol. 2017, 4, e293–e301. [Google Scholar] [CrossRef]
- Bolaños-Meade, J.; Reshef, R.; Fraser, R.; Fei, M.; Abhyankar, S.; Al-Kadhimi, Z.; Alousi, A.M.; Antin, J.H.; Arai, S.; Bickett, K.; et al. Three prophylaxis regimens (tacrolimus, mycophenolate mofetil, and cyclophosphamide; tacrolimus, methotrexate, and bortezomib; or tacrolimus, methotrexate, and maraviroc) versus tacrolimus and methotrexate for prevention of graft-versus-host disease with haemopoietic cell transplantation with reduced-intensity conditioning: A randomised phase 2 trial with a non-randomised contemporaneous control group (BMT CTN 1203). Lancet Haematol. 2019, 6, e132–e143. [Google Scholar] [CrossRef] [PubMed]
- Battipaglia, G.; Labopin, M.; Kröger, N.; Vitek, A.; Afanasyev, B.; Hilgendorf, I.; Schetelig, J.; Ganser, A.; Blaise, D.; Itälä-Remes, M.; et al. Posttransplant cyclophosphamide vs. antithymocyte globulin in HLA-mismatched unrelated donor transplantation. Blood 2019, 134, 892–899. [Google Scholar] [CrossRef] [PubMed]
- De Jong, C.N.; Meijer, E.; Bakunina, K.; Nur, E.; van Marwijk Kooij, M.; de Groot, M.R.; van Gelder, M.; Maertens, J.A.; Kuball, J.H.; Deeren, D.; et al. Post-Transplantation Cyclophosphamide after Allogeneic Hematopoietic Stem Cell Transplantation: Results of the Prospective Randomized HOVON-96 Trial in Recipients of Matched Related and Unrelated Donors. Blood 2019, 134 (Suppl. 1). [Google Scholar] [CrossRef]
- Norkin, M.; Shaw, B.E.; Brazauskas, R.; Tecca, H.R.; Leather, H.L.; Gea-Banacloche, J.; Kamble, R.T.; DeFilipp, Z.; Jacobsohn, D.A.; Ringden, O.; et al. Characteristics of Late Fatal Infections after Allogeneic Hematopoietic Cell Transplantation. Biol. Blood Marrow Transplant. 2019, 25, 362–368. [Google Scholar] [CrossRef]
- Foord, A.M.; Cushing-Haugen, K.L.; Boeckh, M.J.; Carpenter, P.A.; Flowers, M.E.D.; Lee, S.J.; Leisenring, W.M.; Mueller, B.A.; Hill, J.A.; Chow, E.J. Late infectious complications in hematopoietic cell transplantation survivors: A population-based study. Blood Adv. 2020, 4, 1232–1241. [Google Scholar] [CrossRef]
- Walker, I.; Panzarella, T.; Couban, S.; Couture, F.; Devins, G.; Elemary, M.; Gallagher, G.; Kerr, H.; Kuruvilla, J.; Lee, S.J.; et al. Addition of anti-thymocyte globulin to standard graft-versus-host disease prophylaxis versus standard treatment alone in patients with haematological malignancies undergoing transplantation from unrelated donors: Final analysis of a randomised, open-label, multicentre, phase 3 trial. Lancet Haematol. 2020, 7, e100–e111. [Google Scholar] [CrossRef]
- Socié, G.; Stone, J.V.; Wingard, J.R.; Weisdorf, D.; Henslee-Downey, P.J.; Bredeson, C.; Cahn, J.Y.; Passweg, J.R.; Rowlings, P.A.; Schouten, H.C.; et al. Long-term survival and late deaths after allogeneic bone marrow transplantation. Late Effects Working Committee of the International Bone Marrow Transplant Registry. N. Engl. J. Med. 1999, 341, 14–21. [Google Scholar] [CrossRef]
- Wingard, J.R.; Majhail, N.S.; Brazauskas, R.; Wang, Z.; Sobocinski, K.A.; Jacobsohn, D.; Sorror, M.L.; Horowitz, M.M.; Bolwell, B.; Rizzo, J.D.; et al. Long-term survival and late deaths after allogeneic hematopoietic cell transplantation. J. Clin. Oncol. 2011, 29, 2230–2239. [Google Scholar] [CrossRef]
- Martin, P.J.; Counts, G.W.; Appelbaum, F.R.; Lee, S.J.; Sanders, J.E.; Deeg, H.J.; Flowers, M.E.; Syrjala, K.L.; Hansen, J.A.; Storb, R.F.; et al. Life expectancy in patients surviving more than 5 years after hematopoietic cell transplantation. J. Clin. Oncol. 2010, 28, 1011–1016. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.J.; Cushing-Haugen, K.L.; Cheng, G.S.; Boeckh, M.; Khera, N.; Lee, S.J.; Leisenring, W.M.; Martin, P.J.; Mueller, B.A.; Schwartz, S.M.; et al. Morbidity and Mortality Differences Between Hematopoietic Cell Transplantation Survivors and Other Cancer Survivors. J. Clin. Oncol. 2017, 35, 306–313. [Google Scholar] [CrossRef]
- Castagna, L.; Sarina, B.; Bramanti, S.; Perseghin, P.; Mariotti, J.; Morabito, L. Donor lymphocyte infusion after allogeneic stem cell transplantation. Transfus. Apher. Sci. 2016, 54, 345–355. [Google Scholar] [CrossRef] [PubMed]
- McSweeney, P.A.; Niederwieser, D.; Shizuru, J.A.; Sandmaier, B.M.; Molina, A.J.; Maloney, D.G.; Chauncey, T.R.; Gooley, T.A.; Hegenbart, U.; Nash, R.A.; et al. Hematopoietic cell transplantation in older patients with hematologic malignancies: Replacing high-dose cytotoxic therapy with graft-versus-tumor effects. Blood 2001, 97, 3390–3400. [Google Scholar] [CrossRef]
- Bruno, B.; Rotta, M.; Patriarca, F.; Mordini, N.; Allione, B.; Carnevale-Schianca, F.; Giaccone, L.; Sorasio, R.; Omedè, P.; Baldi, I.; et al. A comparison of allografting with autografting for newly diagnosed myeloma. N. Engl. J. Med. 2007, 356, 1110–1120. [Google Scholar] [CrossRef] [PubMed]
- Giaccone, L.; Storer, B.; Patriarca, F.; Rotta, M.; Sorasio, R.; Allione, B.; Carnevale-Schianca, F.; Festuccia, M.; Brunello, L.; Omedè, P.; et al. Long-term follow-up of a comparison of nonmyeloablative allografting with autografting for newly diagnosed myeloma. Blood 2011, 117, 6721–6727. [Google Scholar] [CrossRef] [PubMed]
- Dreger, P.; Fenske, T.S.; Montoto, S.; Pasquini, M.C.; Sureda, A.; Hamadani, M.; the European Society for Blood and Marrow Transplantation (EBMT) and the Center for International Blood and Marrow Transplant Research (CIBMTR). Cellular Immunotherapy for Refractory Diffuse Large B Cell Lymphoma in the Chimeric Antigen Receptor-Engineered T Cell Era: Still a Role for Allogeneic Transplantation? Biol. Blood Marrow Transplant. 2020, 26, e77–e85. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients’ and Donors’ Characteristics | Total (N = 85) |
|---|---|
| Age at transplant (years) | |
| Median | 51 y |
| Range | 19–74 |
| Sex | |
| Male | 51 (60%) |
| Female | 34 (40%) |
| Disease | |
| AML | 33 (39%) |
| AML | 25 (75%) |
| Relapsed AML | 8 (25%) |
| ALL | 14 (16%) |
| ALL | 6 (43%) |
| Relapsed ALL | 8 (57%) |
| Non-Hodgkin Lymphoma | 17 (20%) |
| Multiple Myeloma | 12 (14%) |
| MDS | 4 (5%) |
| Hodgkin Lymphoma | 3 (4%) |
| Aplastic Anemia | 1 (1%) |
| Myelofibrosis | 1 (1%) |
| Disease status at Transplant | |
| 1° CR | 40 (47%) |
| >1° CR | 22 (26%) |
| Active disease | 23 (27%) |
| CIBMTR risk group | |
| Very High | 6 (7%) |
| High | 29 (34%) |
| Intermediate | 32 (38%) |
| Low | 17 (20%) |
| Not applicable | 1 (1%) |
| Source of stem cell | |
| peripheral blood stem cell | 85 (100%) |
| Sex mismatch | |
| No | 47 (55%) |
| Yes | 38 (45%) |
| Female into male | 20 (24%) |
| Donor age, years | |
| Median | 29 y |
| Range | 16–68 |
| Source of graft | |
| sibling | 20 (24%) |
| unrelated | 65 (76%) |
| HLA match | |
| 10/10 | 47 (55%) |
| 9/10 | 23 (27%) |
| 8 */10 | 15 (18%) |
| CMV serology | |
| CMV D−R− | 2 (2%) |
| CMV D+R− | 31 (37%) |
| CMV D−R+ | 2 (2%) |
| CMV D+R+ | 50 (59%) |
| Conditioning regimen | |
| Busulfan + Cyclophosphamide | 25 (30%) |
| Thiotepa + Treosulfan | 11 (13%) |
| Fludarabine + Treosulfan + Thiotepa | 7 (8%) |
| Treosulfan + Fludarabine + Cyclophosphamide | 5 (6%) |
| Treosulfan + Cyclophosphamide | 11 (13%) |
| Melphalan + Cyclophosphamide | 5 (6%) |
| Treosulfan + Cyclophosphamide + TBI 2Gy ° | 4 (5%) |
| Melphalan + Cyclophosphamide + TBI 2Gy ° | 4 (5%) |
| Busulfane + Fludarabine | 5 (6%) |
| Fludarabine + Melphalan + TBI 2Gy ° | 3 (2%) |
| Fludarabine + Thiotepa + Cyclophosphamide | 4 (5%) |
| Cyclophosphamide + ATG + Fludarabine | 1 (1%) |
| Infused cell dose * CD34+ cell × 106/kg, | |
| Median | 7 (range 2–15) |
| CD3+ cell × 108 kg | |
| Median | 2.89 (range 1.123–10.372) |
| Total Nucleated Cells × 108/kg | |
| Median | 12.1 (range 6.9–15.739) |
| Post-Transplant Data (n = 85) | |
|---|---|
| Engraftment median time | |
| Neutrophils engraftment > 0.5 × 109/L | 14 days (range 11–32) |
| Platelets engraftment > 20 × 109/L | 16 days (range 10–201) |
| Peripheral Blood Lymphocyte count ° | |
| Day+28 Median (U/µL) | 400 (range 10–3640) |
| Day+56 Median (U/µL) | 1200 (range 250–5000) |
| Day+84 Median (U/µL) | 1200 (range 360–5000) |
| Day+180 Median (U/µL) | 1800 (range 400–4900) |
| Day+365 Median (U/µL) | 2100 (range 110–5600) |
| Chimerism § | |
| Day+28 | >97% of patients alive and not relapsed |
| Day+56 | >97% of patients alive and not relapsed |
| Day+84, +180, +365 | >97% of patients alive and not relapsed |
| CMV reactivation | |
| Incidence | 55 (65%) |
| Median day of reactivation | 37 (range 13–330) |
| Bloodstream infection during engraftment | |
| (day 0–26) | |
| Incidence | 14 (16%) |
| Sort of microorganism | |
| E. Coli | 5 (36%) |
| Pseudomonas aeruginosa | 4 (29%) |
| Klebsiella pneumoniae carbapenemase-producing | 3 (21%) |
| Klebsiella Oxytoca | 1 (7%) |
| Enterococcus Faecium | 1 (7%) |
| Invasive Fungal infection at 1 year | |
| Incidence | 3 (4%) |
| Toxicity (G3–G4) † | |
| Mucositis | 16 (19%) |
| Hemorrhage ‡ | 6 (7%) |
| Liver enzymes elevation | 5 (6%) |
| Sinusoidal obstruction disease (SOS) | 4 (5%) |
| Hypocalcemia | 1 (1%) |
| Hyperbilirubinemia | 1 (1%) |
| Long Term Toxicities (All Data Reflect Median Follow Up of 36 Months) | |
|---|---|
| Modification of PFT °: | |
| Global Incidence | 16 (32%) |
| New obstructive disorder | 6 (12%) |
| New restrictive disorder | 5 (10%) |
| Worsening of a preexistent disorder | 5 (10%) |
| Emergence of Thyroid disfunctionx | 4 (5%) |
| Hypothyroidism | 3 (4%) |
| Hyperthyroidism | 1 (1%) |
| Emergence of Dyslipidemiaa | |
| Global incidence | 7 (15%) |
| Emergence of Diabetesb | |
| Global incidence | 2 (3%) |
| Cardiovascular disorders | |
| Emergence of Hypertensionc | |
| Global incidence | 5 (8%) |
| Emergence of Hypokinetic Cardiomyopathyd | |
| Global incidence | 1 (1%) |
| DLI (n = 14 Patients) * | |
|---|---|
| Indication for treatment | |
| disease relapse | 14 (100%) |
| Source of DLI | |
| matched sibling | 6 (43%) |
| HLA-matched unrelated donors | 8 (57%) |
| Median time between transplant and DLI Median number of DLI infusions = 3 | 10 months (range 3–89) 3 months (range 1–13) |
| Overall response rate | 57% |
| Disease control rate | 78% |
| Incidence of acute GVHD grade I–II | 33% |
| Incidence of acute GVHD grade III–IV | 0% |
| Estimated 1-year EFS | 52% (95% CI, 26–78%) |
| Estimated 1-year OS | 71% (95% CI, 47–95%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carnevale-Schianca, F.; Caravelli, D.; Gallo, S.; Becco, P.; Paruzzo, L.; Poletto, S.; Polo, A.; Mangioni, M.; Salierno, M.; Berger, M.; et al. Post-Transplant Cyclophosphamide and Tacrolimus—Mycophenolate Mofetil Combination Governs GVHD and Immunosuppression Need, Reducing Late Toxicities in Allogeneic Peripheral Blood Hematopoietic Cell Transplantation from HLA-Matched Donors. J. Clin. Med. 2021, 10, 1173. https://doi.org/10.3390/jcm10061173
Carnevale-Schianca F, Caravelli D, Gallo S, Becco P, Paruzzo L, Poletto S, Polo A, Mangioni M, Salierno M, Berger M, et al. Post-Transplant Cyclophosphamide and Tacrolimus—Mycophenolate Mofetil Combination Governs GVHD and Immunosuppression Need, Reducing Late Toxicities in Allogeneic Peripheral Blood Hematopoietic Cell Transplantation from HLA-Matched Donors. Journal of Clinical Medicine. 2021; 10(6):1173. https://doi.org/10.3390/jcm10061173
Chicago/Turabian StyleCarnevale-Schianca, Fabrizio, Daniela Caravelli, Susanna Gallo, Paolo Becco, Luca Paruzzo, Stefano Poletto, Alessandra Polo, Monica Mangioni, Milena Salierno, Massimo Berger, and et al. 2021. "Post-Transplant Cyclophosphamide and Tacrolimus—Mycophenolate Mofetil Combination Governs GVHD and Immunosuppression Need, Reducing Late Toxicities in Allogeneic Peripheral Blood Hematopoietic Cell Transplantation from HLA-Matched Donors" Journal of Clinical Medicine 10, no. 6: 1173. https://doi.org/10.3390/jcm10061173
APA StyleCarnevale-Schianca, F., Caravelli, D., Gallo, S., Becco, P., Paruzzo, L., Poletto, S., Polo, A., Mangioni, M., Salierno, M., Berger, M., Pessolano, R., Saglio, F., Gottardi, D., Rota-Scalabrini, D., Grignani, G., Fizzotti, M., Ferrero, I., Frascione, P. M. M., D’Ambrosio, L., ... Fagioli, F. (2021). Post-Transplant Cyclophosphamide and Tacrolimus—Mycophenolate Mofetil Combination Governs GVHD and Immunosuppression Need, Reducing Late Toxicities in Allogeneic Peripheral Blood Hematopoietic Cell Transplantation from HLA-Matched Donors. Journal of Clinical Medicine, 10(6), 1173. https://doi.org/10.3390/jcm10061173