

Early Prediction of Seven-Day Mortality in Intensive Care Unit Using a Machine Learning Model: Results from the SPIN-UTI Project

 , , ,
, , ,  on behalf of the SPIN-UTI network
on behalf of the SPIN-UTI network
Abstract
1. Introduction
2. Materials and Methods
2.1. The SPIN-UTI Project
2.2. Definition of SAPS II and Other Predictors
2.3. Dataset of “Real” Records
2.4. Dataset of Synthetic Records
2.5. Statistical Analysis
2.6. Machine Learning Algorithm
3. Results
3.1. Characteristics of the Dataset of “Real” Records
3.2. Applying Logistic Regression Models to Predict the Risk of 7-Day Mortality
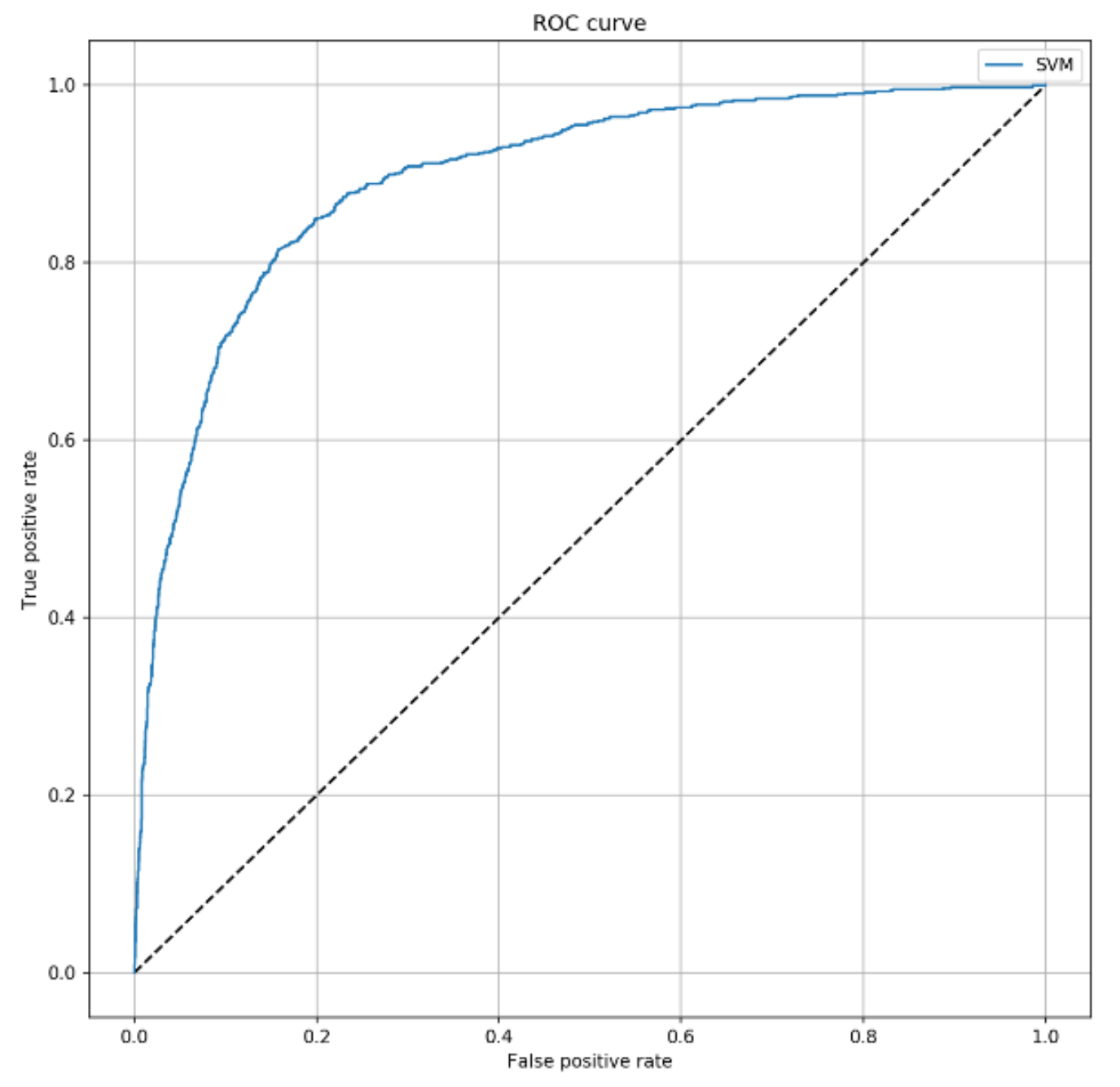
3.3. The SVM Algorithm Improved the Prediction of Patients Who Died
3.4. The SVM Algorithm Maintained Its Predictive Ability among Patients Who Did Not Develop HAIs
3.5. The Predictivie Performance of the SVM Model by Removing SAPS II
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haque, M.; Sartelli, M.; McKimm, J.; Bin Abu Bakar, M. Health care-associated infections—An overview. Infect. Drug Resist. 2018, 11, 2321–2333. [Google Scholar] [CrossRef]
- Revelas, A. Healthcare-associated infections: A public health problem. Niger. Med. J. 2012, 53, 59–64. [Google Scholar] [CrossRef]
- Hughes, R.G. Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Zhang, Y.; Du, M.; Johnston, J.M.; Andres, E.B.; Suo, J.; Yao, H.; Huo, R.; Liu, Y.; Fu, Q. Incidence of healthcare-associated infections in a tertiary hospital in Beijing, China: Results from a real-time surveillance system. Antimicrob. Resist. Infect. Control. 2019, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Allegranzi, B.; Nejad, S.B.; Combescure, C.; Graafmans, W.; Attar, H.; Donaldson, L.; Pittet, D. Burden of endemic health-care-associated infection in developing countries: Systematic review and meta-analysis. Lancet 2011, 377, 228–241. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Rello, J.; Marshall, J.K.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International Study of the Prevalence and Outcomes of Infection in Intensive Care Units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef]
- Alp, E.; Damani, N. Healthcare-associated infections in Intensive Care Units: Epidemiology and infection control in low-to-middle income countries. J. Infect. Dev. Ctries. 2015, 9, 1040–1045. [Google Scholar] [CrossRef]
- Wang, W.; Zhu, S.; He, Q.; Zhang, R.; Kang, Y.; Wang, M.; Zou, K.; Zong, Z.; Sun, X. Developing a Registry of Healthcare-Associated Infections at Intensive Care Units in West China: Study Rationale and Patient Characteristics. Clin. Epidemiol. 2019, 11, 1035–1045. [Google Scholar] [CrossRef]
- Scardoni, A.; Balzarini, F.; Signorelli, C.; Cabitza, F.; Odone, A. Artificial intelligence-based tools to control healthcare associated infections: A systematic review of the literature. J. Infect. Public Health 2020, 13, 1061–1077. [Google Scholar] [CrossRef] [PubMed]
- Duval, A.; Obadia, T.; Martinet, L.; Boëlle, P.-Y.; Fleury, E.; Guillemot, D.; Opatowski, L.; Temime, L.; I-Bird study group. Measuring dynamic social contacts in a rehabilitation hospital: Effect of wards, patient and staff characteristics. Sci. Rep. 2018, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lambert, M.-L.; Silversmit, G.; Savey, A.; Palomar, M.; Hiesmayr, M.; Agodi, A.; Van Rompaye, B.; Mertens, K.; Vansteelandt, S. Preventable Proportion of Severe Infections Acquired in Intensive Care Units: Case-Mix Adjusted Estimations from Patient-Based Surveillance Data. Infect. Control. Hosp. Epidemiology 2014, 35, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Barchitta, M.; Maugeri, A.; La Rosa, M.C.; La Mastra, C.; Murolo, G.; Agodi, A. Three-Year Trends of Healthcare-Associated Infections and Antibiotic Use in Acute Care Hospitals: Findings from 2016–2018 Point Prevalence Surveys in Sicily, Italy. Antibiotics 2020, 10, 1. [Google Scholar] [CrossRef]
- Barchitta, M.; Maugeri, A.; La Rosa, M.C.; La Mastra, C.; Murolo, G.; Basile, G.; Agodi, A. Carbapenem Consumption and Rate of carbapenem-resistant gram-negative bacteria: Results from the Sicilian Surveillance System. Ann. Ig. 2020. [Google Scholar] [CrossRef]
- Barchitta, M.; Quattrocchi, A.; Maugeri, A.; La Rosa, M.C.; La Mastra, C.; Sessa, L.; Cananzi, P.; Murolo, G.; Oteri, A.; Basile, G.; et al. Antibiotic Consumption and Resistance during a 3-Year Period in Sicily, Southern Italy. Int. J. Environ. Res. Public Health 2019, 16, 2253. [Google Scholar] [CrossRef] [PubMed]
- Agodi, A.; Barchitta, M.; Quattrocchi, A.; Maugeri, A.; Aldisio, E.; Marchese, A.E.; Mattaliano, A.R.; Tsakris, A. Antibiotic trends of Klebsiella pneumoniae and Acinetobacter baumannii resistance indicators in an intensive care unit of Southern Italy, 2008–2013. Antimicrob. Resist. Infect. Control. 2015, 4, 43. [Google Scholar] [CrossRef]
- Sulzgruber, P.; Schnaubelt, S.; Koller, L.; Laufer, G.; Pilz, A.; Kazem, N.; Winter, M.-P.; Steinlechner, B.; Andreas, M.; Fleck, T.; et al. An Extended Duration of the Pre-Operative Hospitalization is Associated with an Increased Risk of Healthcare-Associated Infections after Cardiac Surgery. Sci. Rep. 2020, 10, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Zimlichman, E.; Henderson, D.; Tamir, O.; Franz, C.; Song, P.; Yamin, C.K.; Keohane, C.; Denham, C.R.; Bates, D.W. Health Care–Associated Infections. JAMA Intern. Med. 2013, 173, 2039–2046. [Google Scholar] [CrossRef]
- World Health Organization. Report on the Burden of Endemic Health Care-Associated Infection Worldwide; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Garrouste-Orgeas, M.; Timsit, J.F.; Tafflet, M.; Misset, B.; Zahar, J.-R.; Soufir, L.; Lazard, T.; Jamali, S.; Mourvillier, B.; Cohen, Y.; et al. Excess Risk of Death from Intensive Care Unit--Acquired Nosocomial Bloodstream Infections: A Reappraisal. Clin. Infect. Dis. 2006, 42, 1118–1126. [Google Scholar] [CrossRef]
- Alexopoulos, E.C.; Batzi, E.; Messolora, F.; Jelastopulu, E. Wide range of point prevalences of healthcare-associated infections in Western Greece. Epidemiol. Infect. 2010, 139, 1734–1739. [Google Scholar] [CrossRef][Green Version]
- Barchitta, M.; Maugeri, A.; Favara, G.; Riela, P.; La Mastra, C.; La Rosa, M.; Lio, R.M.S.; Gallo, G.; Mura, I.; Agodi, A.; et al. Cluster analysis identifies patients at risk of catheter-associated urinary tract infections in intensive care units: Findings from the SPIN-UTI Network. J. Hosp. Infect. 2021, 107, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Zarrilli, R.; Di Popolo, A.; Bagattini, M.; Giannouli, M.; Martino, D.; Barchitta, M.; Quattrocchi, A.; Iula, V.; De Luca, C.; Scarcella, A.; et al. Clonal spread and patient risk factors for acquisition of extensively drug-resistant Acinetobacter baumannii in a neonatal intensive care unit in Italy. J. Hosp. Infect. 2012, 82, 260–265. [Google Scholar] [CrossRef]
- Gerry, S.; Bonnici, T.; Birks, J.; Kirtley, S.; Virdee, P.S.; Watkinson, P.J.; Collins, G.S. Early warning scores for detecting deterioration in adult hospital patients: Systematic review and critical appraisal of methodology. BMJ 2020, 369, m1501. [Google Scholar] [CrossRef]
- Brennan, T.A.; Leape, L.L.; Laird, N.M.; Hebert, L.; Localio, A.R.; Lawthers, A.G.; Newhouse, J.P.; Weiler, P.C.; Hiatt, H.H. Incidence of adverse events and negligence in hospitalized patients: Results of the Harvard Medical Practice Study I. Qual. Saf. Health Care 2004, 13, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on Quality of Health Care in America. To Err is Human: Building a Safer Health System; Kohn, L.T., Corrigan, J.M., Donaldson, M.S., Eds.; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Vincent, C.; Neale, G.; Woloshynowych, M. Adverse events in British hospitals: Preliminary retrospective record review. BMJ 2001, 322, 517–519. [Google Scholar] [CrossRef] [PubMed]
- Hillman, K.M.; Bristow, P.J.; Chey, T.; Daffurn, K.; Jacques, T.; Norman, S.L.; Bishop, G.F.; Simmons, G. Duration of life-threatening antecedents prior to intensive care admission. Intensiv. Care Med. 2002, 28, 1629–1634. [Google Scholar] [CrossRef]
- Allyn, J.; Ferdynus, C.; Bohrer, M.; Dalban, C.; Valance, D.; Allou, N. Simplified Acute Physiology Score II as Predictor of Mortality in Intensive Care Units: A Decision Curve Analysis. PLoS ONE 2016, 11, e0164828. [Google Scholar] [CrossRef] [PubMed]
- Gilani, M.T.; Razavi, M.; Azad, A.M. A comparison of Simplified Acute Physiology Score II, Acute Physiology and Chronic Health Evaluation II and Acute Physiology and Chronic Health Evaluation III scoring system in predicting mortality and length of stay at surgical intensive care unit. Niger. Med. J. 2014, 55, 144–147. [Google Scholar] [CrossRef]
- Sadaka, F.; EthmaneAbouElMaali, C.; Cytron, M.A.; Fowler, K.; Javaux, V.M.; O’Brien, J. Predicting Mortality of Patients With Sepsis: A Comparison of APACHE II and APACHE III Scoring Systems. J. Clin. Med. Res. 2017, 9, 907–910. [Google Scholar] [CrossRef]
- Mungan, I.; Bektaş, S.; Çavuş, M.A.; Sarı, S.; Turan, S. The predictive power of SAPS-3 and SOFA scores and their relations with patient outcomes in the Surgical Intensive Care Unit. Turk. J. Surg. 2019, 35, 124–130. [Google Scholar] [CrossRef]
- Haddadi, A.; Ledmani, M.; Gainier, M.; Hubert, H.; Tagne, J.; De Micheaux, P. Comparing the APACHE II, SOFA, LOD, and SAPS II scores in patients who have developed a nosocomial infection. Bangladesh Crit. Care J. 2014, 2, 4–9. [Google Scholar] [CrossRef]
- Agodi, A.; Barchitta, M.; Auxilia, F.; Brusaferro, S.; D’Errico, M.M.; Montagna, M.T.; Pasquarella, C.; Tardivo, S.; Arrigoni, C.; Fabiani, L.; et al. Epidemiology of intensive care unit-acquired sepsis in Italy: Results of the SPIN-UTI network. Ann. Ig. Med. Prev. Comunita 2018, 30, 15–21. [Google Scholar]
- Beck, D.H.; Smith, G.B.; Pappachan, J.V.; Millar, B. External validation of the SAPS II, APACHE II and APACHE III prognostic models in South England: A multicentre study. Intensiv. Care Med. 2003, 29, 249–256. [Google Scholar] [CrossRef]
- Le Gall, J.R. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Nielsen, A.B.; Thorsen-Meyer, H.-C.; Belling, K.; Nielsen, A.P.; Thomas, C.E.; Chmura, P.J.; Lademann, M.; Moseley, P.L.; Heimann, M.; Dybdahl, L.; et al. Survival prediction in intensive-care units based on aggregation of long-term disease history and acute physiology: A retrospective study of the Danish National Patient Registry and electronic patient records. Lancet Digit. Health 2019, 1, e78–e89. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Favara, G.; Riela, P.M.; Maugeri, A.; Barchitta, M.; Gallo, G.; Agodi, A. Risk of Pneumonia and Associated Outcomes in Intensive Care Unit: An Integrated Approach of Visual and Cluster Analysis. In Proceedings of the 2019 IEEE World Congress Services, Milan, Italy, 8–13 July 2019; IEEE: New York, NY, USA; pp. 289–294. [Google Scholar]
- Kong, G.; Lin, K.; Hu, Y. Using machine learning methods to predict in-hospital mortality of sepsis patients in the ICU. BMC Med Inform. Decis. Mak. 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Parreco, J.P.; Hidalgo, A.E.; Badilla, A.D.; Ilyas, O.; Rattan, R. Predicting central line-associated bloodstream infections and mortality using supervised machine learning. J. Crit. Care 2018, 45, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Deo, R.C. Machine Learning in Medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef]
- Deo, R.C. Machine Learning in Medicine. Circulation 2020, 142, 1521–1523. [Google Scholar] [CrossRef]
- Yu, W.; Liu, T.; Valdez, R.; Gwinn, M.; Khoury, M.J. Application of support vector machine modeling for prediction of common diseases: The case of diabetes and pre-diabetes. BMC Med. Inform. Decis. Mak. 2010, 10, 16. [Google Scholar] [CrossRef]
- Cortes, C.; Vapnik, V. Support-Vector Networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Agodi, A.; Barchitta, M.; Quattrocchi, A.; Spera, E.; Gallo, G.; Auxilia, F.; Brusaferro, S.; D’Errico, M.M.; Montagna, M.T.; Pasquarella, C.; et al. Preventable proportion of intubation-associated pneumonia: Role of adherence to a care bundle. PLoS ONE 2017, 12, e0181170. [Google Scholar] [CrossRef]
- Agodi, A.; Auxilia, F.; Barchitta, M.; Brusaferro, S.; D’Errico, M.M.; Montagna, M.T.; Pasquarella, C.; Tardivo, S.; Mura, I. Antibiotic consumption and resistance: Results of the SPIN-UTI project of the GISIO-SItI. Epidemiol. Prev. 2015, 39, 94–98. [Google Scholar]
- Agodi, A.; Auxilia, F.; Barchitta, M.; Brusaferro, S.; D’Alessandro, D.; Grillo, O.; Montagna, M.; Pasquarella, C.; Righi, E.; Tardivo, S.; et al. Trends, risk factors and outcomes of healthcare-associated infections within the Italian network SPIN-UTI. J. Hosp. Infect. 2013, 84, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Agodi, A.; Auxilia, F.; Barchitta, M.; Brusaferro, S.; D’Alessandro, D.; Montagna, M.; Orsi, G.B.; Pasquarella, C.; Torregrossa, V.; Suetens, C.; et al. Building a benchmark through active surveillance of intensive care unit-acquired infections: The Italian network SPIN-UTI. J. Hosp. Infect. 2010, 74, 258–265. [Google Scholar] [CrossRef]
- Agodi, A.; Auxilia, F.; Barchitta, M.; D’Errico, M.M.; Montagna, M.T.; Pasquarella, C.; Tardivo, S.; Mura, I. Control of intubator associated pneumonia in intensive care unit: Results of the GISIO-SItI SPIN-UTI Project. Epidemiol. Prev. 2014, 38, 51–56. [Google Scholar]
- Agodi, A.; Barchitta, M.; Mura, I.; Pasquarella, C.; Torregrossa, M.V.; SItI, G. The commitment of the GISIO-SItI to contrast Healthcare-Associated Infections and the experience of prevalence studies in Sicily. Ann. Ig. 2018, 30, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Masia, M.; Barchitta, M.; Liperi, G.; Cantù, A.; Alliata, E.; Auxilia, F.; Torregrossa, V.; Mura, I.; Agodi, A. Validation of intensive care unit-acquired infection surveillance in the Italian SPIN-UTI network. J. Hosp. Infect. 2010, 76, 139–142. [Google Scholar] [CrossRef]
- European Center for Disease Prevention and Control. European Surveillance of Healthcare-Associated Infections in Intensive Care Units- HAI-Net ICU Protocol- Protocol Version 1.02; ECDC: Stockholm, Sweden, 2015. [Google Scholar]
- European Centre for Disease Prevention and Control. European Surveillance of Healthcare-Associated Infections in Intensive Care Units; ECDC HAIICU protocol V1.01 Standard and Light; ECDC: Stockholm, Sweden, 2010. [Google Scholar]
- Malarvizhi, R.; Thanamani, A. K-nearest neighbor in missing data imputation. Int. J. Eng. Res. Dev. 2012, 5, 5–7. [Google Scholar]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Lovejoy, C.A.; Buch, V.; Maruthappu, M. Artificial intelligence in the intensive care unit. Crit. Care 2019, 23, 1–3. [Google Scholar] [CrossRef]
- Strand, K.; Flaatten, H. Severity scoring in the ICU: A review. Acta Anaesthesiol. Scand. 2008, 52, 467–478. [Google Scholar] [CrossRef]
- Komorowski, M. Artificial intelligence in intensive care: Are we there yet? Intensiv. Care Med. 2019, 45, 1298–1300. [Google Scholar] [CrossRef] [PubMed]
- Fralick, M.; Colak, E.; Mamdani, M. Machine Learning in Medicine. New Engl. J. Med. 2019, 380, 2588–2590. [Google Scholar] [CrossRef]
- Meiring, C.; Dixit, A.; Harris, S.; Maccallum, N.S.; Brealey, D.A.; Watkinson, P.J.; Jones, A.; Ashworth, S.; Beale, R.; Brett, S.J.; et al. Optimal intensive care outcome prediction over time using machine learning. PLoS ONE 2018, 13, e0206862. [Google Scholar] [CrossRef]
- Desautels, T.; Calvert, J.; Hoffman, J.; Jay, M.; Kerem, Y.; Shieh, L.; Shimabukuro, D.; Chettipally, U.; Feldman, M.D.; Barton, C.; et al. Prediction of Sepsis in the Intensive Care Unit With Minimal Electronic Health Record Data: A Machine Learning Approach. JMIR Med. Inform. 2016, 4, e28. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Moreno, R. Clinical review: Scoring systems in the critically ill. Crit. Care 2010, 14, 207. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Respiratory Medicine. Opening the black box of machine learning. Lancet Respir. Med. 2018, 6, 801. [Google Scholar] [CrossRef]
- Luz, C.; Vollmer, M.; Decruyenaere, J.; Nijsten, M.; Glasner, C.; Sinha, B. Machine learning in infection management using routine electronic health records: Tools, techniques, and reporting of future technologies. Clin. Microbiol. Infect. 2020, 26, 1291–1299. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Agodi, A. A Clustering Approach to Classify Italian Regions and Provinces Based on Prevalence and Trend of SARS-CoV-2 Cases. Int. J. Environ. Res. Public Health 2020, 17, 5286. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Battiato, S.; Agodi, A. Modeling the Novel Coronavirus (SARS-CoV-2) Outbreak in Sicily, Italy. Int. J. Environ. Res. Public Health 2020, 17, 4964. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Battiato, S.; Agodi, A. Estimation of Unreported Novel Coronavirus (SARS-CoV-2) Infections from Reported Deaths: A Susceptible–Exposed–Infectious–Recovered–Dead Model. J. Clin. Med. 2020, 9, 1350. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, A.; Barchitta, M.; Battiato, S.; Agodi, A. Estimation of unreported SARS-CoV-2 cases in Italy using a Susceptible-Exposed-Infectious-Recovered-Dead model. J. Glob. Health 2020, 10, 21105. [Google Scholar] [CrossRef]
- Peiffer-Smadja, N.; Rawson, T.; Ahmad, R.; Buchard, A.; Georgiou, P.; Lescure, F.-X.; Birgand, G.; Holmes, A. Corrigendum to ‘machine learning for clinical decision support in infectious diseases: A narrative review of current applications’ clinical microbiology and infection (2020) 584–595. Clin. Microbiol. Infect. 2020, 26, 1118. [Google Scholar] [CrossRef]
- Ripoli, A.; Sozio, E.; Sbrana, F.; Bertolino, G.; Pallotto, C.; Cardinali, G.; Meini, S.; Pieralli, F.; Azzini, A.M.; Concia, E.; et al. Personalized machine learning approach to predict candidemia in medical wards. Infection 2020, 48, 749–759. [Google Scholar] [CrossRef] [PubMed]
- Amer, A.Y.A.; Vranken, J.; Wouters, F.; Mesotten, D.; Vandervoort, P.; Storms, V.; Luca, S.; Vanrumste, B.; Aerts, J.-M. Feature Engineering for ICU Mortality Prediction Based on Hourly to Bi-Hourly Measurements. Appl. Sci. 2019, 9, 3525. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients (n = 3782) | Died Patients (n = 875) | Alive Patients (n = 2907) | p-Value |
|---|---|---|---|---|
| Age, years | 70.0 (20.0) | 74.0 (17.0) | 69.0 (21.0) | <0.001 |
| Sex (% men) | 60.2% | 55.0% | 61.7% | <0.001 |
| Patient’s origin | ||||
| Other ward/healthcare facility | 70.9% | 70.1% | 71.1% | <0.001 |
| Community | 29.1% | 29.9% | 28.9% | |
| SAPS II at admission | 49.0 (27.0) | 59.0 (27.0) | 46.0 (25.0) | <0.001 |
| Type of ICU admission | ||||
| Medical | 56.9% | 59.3% | 56.1% | <0.001 |
| Surgical | 43.1% | 40.7% | 43.9% | |
| Trauma | 4.7% | 2.4% | 5.4% | <0.001 |
| Impaired immunity | 11.4% | 15.0% | 10.3% | <0.001 |
| Non-surgical treatment for acute coronary disease | 9.0% | 10.2% | 8.7% | 0.174 |
| Surgical intervention | 34.8% | 32.5% | 35.5% | 0.306 |
| Antibiotic therapy in 48 h before or after ICU admission | 62.6% | 62.2% | 62.8% | 0.744 |
| Presence of urinary catheter at ICU admission | 77.0% | 75.9% | 77.4% | 0.351 |
| Presence of intubation at ICU admission | 62.4% | 61.7% | 62.6% | 0.646 |
| Presence of central venous catheter at ICU admission | 40.5% | 38.5% | 41.0% | 0.182 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barchitta, M.; Maugeri, A.; Favara, G.; Riela, P.M.; Gallo, G.; Mura, I.; Agodi, A., on behalf of the SPIN-UTI network. Early Prediction of Seven-Day Mortality in Intensive Care Unit Using a Machine Learning Model: Results from the SPIN-UTI Project. J. Clin. Med. 2021, 10, 992. https://doi.org/10.3390/jcm10050992
Barchitta M, Maugeri A, Favara G, Riela PM, Gallo G, Mura I, Agodi A on behalf of the SPIN-UTI network. Early Prediction of Seven-Day Mortality in Intensive Care Unit Using a Machine Learning Model: Results from the SPIN-UTI Project. Journal of Clinical Medicine. 2021; 10(5):992. https://doi.org/10.3390/jcm10050992
Chicago/Turabian StyleBarchitta, Martina, Andrea Maugeri, Giuliana Favara, Paolo Marco Riela, Giovanni Gallo, Ida Mura, and Antonella Agodi on behalf of the SPIN-UTI network. 2021. "Early Prediction of Seven-Day Mortality in Intensive Care Unit Using a Machine Learning Model: Results from the SPIN-UTI Project" Journal of Clinical Medicine 10, no. 5: 992. https://doi.org/10.3390/jcm10050992
APA StyleBarchitta, M., Maugeri, A., Favara, G., Riela, P. M., Gallo, G., Mura, I., & Agodi, A., on behalf of the SPIN-UTI network. (2021). Early Prediction of Seven-Day Mortality in Intensive Care Unit Using a Machine Learning Model: Results from the SPIN-UTI Project. Journal of Clinical Medicine, 10(5), 992. https://doi.org/10.3390/jcm10050992