
Age and Overweight Are Not Contraindications for a Breast Reconstruction with a TMG-Flap—A Risk and Complication Analysis of a Retrospective Double Center Study Including 300 Patients

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chang, D.W.; Wang, B.-G.; Robb, G.L.; Reece, G.P.; Miller, M.J.; Evans, G.R.D.; Langstein, H.N.; Kroll, S.S. Effect of Obesity on Flap and Donor-Site Complications in Free Transverse Rectus Abdominis Myocutaneous Flap Breast Reconstruction. Plast. Reconstr. Surg. 2000, 105, 1640–1648. [Google Scholar] [CrossRef]
- Kroll, S.S.; Netscher, D.T. Complications of TRAM Flap Breast Reconstruction in Obese Patients. Plast. Reconstr. Surg. 1989, 84, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Seidenstuecker, K.; Munder, B.; Mahajan, A.L.; Richrath, P.; Behrendt, P.; Andree, C. Morbidity of Microsurgical Breast Reconstruction in Patients with Comorbid Conditions. Plast. Reconstr. Surg. 2011, 127, 1086–1092. [Google Scholar] [CrossRef]
- Boczar, D.; Huayllani, M.T.; Forte, A.J.; Rinker, B. Microsurgical Breast Reconstruction in the Obese Patient Using Abdominal Flaps: Complication Profile and Patient Satisfaction. Ann. Plast. Surg. 2020, 84, S361–S363. [Google Scholar] [CrossRef]
- Harii, K.; Ohmori, K.; Sekiguchi, J. The free musculocutaneous flap. Plast. Reconstr. Surg. 1976, 57, 294–303. [Google Scholar] [CrossRef]
- Schoeller, T.; Huemer, G.M.; Wechselberger, G. The Transverse Musculocutaneous Gracilis Flap for Breast Reconstruction: Guidelines for Flap and Patient Selection. Plast. Reconstr. Surg. 2008, 122, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Wechselberger, G.; Schoeller, T. The Transverse Myocutaneous Gracilis Free Flap: A Valuable Tissue Source in Autologous Breast Reconstruction. Plast. Reconstr. Surg. 2004, 114, 69–73. [Google Scholar] [CrossRef]
- Vega, S.J.; Sandeen, S.N.; Bossert, R.P.; Perrone, A.; Ortiz, L.; Herrera, H. Gracilis Myocutaneous Free Flap in Autologous Breast Reconstruction. Plast. Reconstr. Surg. 2009, 124, 1400–1409. [Google Scholar] [CrossRef] [PubMed]
- Craggs, B.; Vanmierlo, B.; Zeltzer, A.; Buyl, R.; Haentjens, P.; Hamdi, M. Donor-Site Morbidity following Harvest of the Transverse Myocutaneous Gracilis Flap for Breast Reconstruction. Plast. Reconstr. Surg. 2014, 134, 682e–691e. [Google Scholar] [CrossRef] [PubMed]
- Pülzl, P.; Schoeller, T.; Kleewein, K.; Wechselberger, G. Donor-site morbidity of the transverse musculocutaneous gracilis flap in autologous breast reconstruction: Short-term and long-term results. Plast. Reconstr. Surg. 2011, 128, 233e–242e. [Google Scholar] [CrossRef]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef]
- Beard, J.R.; Officer, A.; De Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef]
- Wong, C.; Mojallal, A.; Bailey, S.H.; Trussler, A.; Saint-Cyr, M. The extended transverse musculocutaneous gracilis flap: Vascular anatomy and clinical implications. Ann. Plast. Surg. 2011, 67, 170–177. [Google Scholar] [CrossRef]
- Defining Adult Overweight and Obesity. Available online: https://www.cdc.gov/obesity/adult/defining.html (accessed on 14 January 2021).
- Neaman, K.C.; Armstrong, S.D.; Baca, M.E.; Albert, M.; Vander Woude, D.L.; Renucci, J.D. Outcomes of traditional cosmetic abdominoplasty in a community setting: A retrospective analysis of 1008 patients. Plast. Reconstr. Surg. März. 2013, 131, 403e–410e. [Google Scholar] [CrossRef] [PubMed]
- Wechselberger, G.; Schwaiger, K. Transverse Upper Gracilis Flap in Breast Reconstruction. In Breast Reconstruction; Springer: Cham, Switzerland, 2020; pp. 253–260. [Google Scholar]
- Nahabedian, M.Y.; Momen, B. Lower Abdominal Bulge after Deep Inferior Epigastric Perforator Flap (DIEP) Breast Reconstruction. Ann. Plast. Surg. 2005, 54, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Blondeel, P.; Boeckx, W.; Vanderstraeten, G.; Lysens, R.; Van Landuyt, K.; Tonnard, P.; Monstrey, S.; Matton, G. The fate of the oblique abdominal muscles after free TRAM flap surgery. Br. J. Plast. Surg. 1997, 50, 315–321. [Google Scholar] [CrossRef]
- Moran, S.L.; Serletti, J.M. Outcome comparison between free and pedicled TRAM flap breast reconstruction in the obese patient. Plast. Reconstr. Surg. 2001, 108, 1954–1960; discussion 1961–1962. [Google Scholar] [CrossRef]
- Greco, J.A., 3rd.; Castaldo, E.T.; Nanney, L.B.; Wu, Y.C.; Donahue, R.; Wendel, J.J.; Hagan, K.F.; Shack, R.B. Autologous breast reconstruction: The Vanderbilt experience (1998 to 2005) of independent predictors of displeasing outcomes. J. Am. Coll. Surg. 2008, 207, 49–56. [Google Scholar] [CrossRef]
- Ochoa, O.; Chrysopoulo, M.; Nastala, C.; Ledoux, P.; Pisano, S. Abdominal wall stability and flap complications after deep inferior epigastric perforator flap breast reconstruction: Does body mass index make a difference? Analysis of 418 patients and 639 flaps. Plast. Reconstr. Surg. 2012, 130, 21e–33e. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-T.; Mun, G.-H. Effects of Obesity on Postoperative Complications After Breast Reconstruction Using Free Muscle-Sparing Transverse Rectus Abdominis Myocutaneous, Deep Inferior Epigastric Perforator, and Superficial Inferior Epigastric Artery Flap. Ann. Plast. Surg. 2016, 76, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Palve, J.S.; Luukkaala, T.H.; Kääriäinen, M.T. Predictive risk factors of complications in different breast reconstruction methods. Breast Cancer Res. Treat. 2020, 182, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.I.; Liu, J. Prospective Evaluation of Obese Patients Undergoing Autologous Abdominal Free Flap Breast Reconstruction. Plast. Reconstr. Surg. 2018, 142, 120e–125e. [Google Scholar] [CrossRef]
- Torabi, R.; Stalder, M.W.; Tessler, O.; Bartow, M.J.; Lam, J.; Patterson, C.; Wise, M.W.; Dupin, C.L.; Hilaire, H.S. Assessing Age as a Risk Factor for Complications in Autologous Breast Reconstruction. Plast. Reconstr. Surg. 2018, 142, 840e–846e. [Google Scholar] [CrossRef]
- Selber, J.C.; Bergey, M.; Sonnad, S.S.; Kovach, S.; Wu, L.; Serletti, J.M. Free Flap Breast Reconstruction in Advanced Age: Is It Safe? Plast. Reconstr. Surg. 2009, 124, 1015–1022. [Google Scholar] [CrossRef]
- Chang, E.I.; Vaca, L.; DaLio, A.L.; Festekjian, J.H.; Crisera, C.A. Assessment of Advanced Age as a Risk Factor in Microvascular Breast Reconstruction. Ann. Plast. Surg. 2011, 67, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.; Flitcroft, K.; Brennan, M.; Spillane, A. Patterns and outcomes of breast reconstruction in older women—A systematic review of the literature. Eur. J. Surg. Oncol. (EJSO) 2016, 42, 604–615. [Google Scholar] [CrossRef] [PubMed]
- Wechselberger, G.; Schoeller, T.; Bauer, T.; Schwabegger, A.; Ninkovic, M.; Rainer, C.; Ninkovic, M. Surgical technique and clinical application of the transverse gracilismyocutaneous free flap. Br. J. Plast. Surg. 2001, 54, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Locke, M.B.; Zhong, T.; Mureau, M.A.; Hofer, S.O. Tug ‘O’ war: Challenges of transverse upper gracilis (TUG) myocutaneous free flap breast reconstruction. J. Plast. Reconstr. Aesthetic Surg. 2012, 65, 1041–1050. [Google Scholar] [CrossRef]
- Bodin, F.; Dissaux, C.; Dupret-Bories, A.; Schohn, T.; Fiquet, C.; Bruant-Rodier, C. The transverse musculo-cutaneous gracilis flap for breast reconstruction: How to avoid complications. Microsurgery 2015, 36, 42–48. [Google Scholar] [CrossRef]
- Nickl, S.; Nedomansky, J.; Radtke, C.; Haslik, W.; Schroegendorfer, K.F. Optimization of breast reconstruction results using TMG flap in 30 cases: Evaluation of several refinements addressing flap design, shaping techniques, and reduction of donor site morbidity. Microsurgery 2018, 38, 489–497. [Google Scholar] [CrossRef]
- Kuhn, S.; Klettenheimer, A.; Küenzlen, L.; Kiehlmann, M.; Schlosshauer, T.; Djedovic, G.; Rieger, U.M. Outcome, complications, and body mass index correlation of horizontal and combined horizontal and vertical thigh lift: A 16-year single-center experience. J. Cutan. Aesthetic Surg. 2019, 12, 231. [Google Scholar] [CrossRef] [PubMed]
- Nemerofsky, R.B.; Oliak, D.A.; Capella, J.F. Body Lift: An Account of 200 Consecutive Cases in the Massive Weight Loss Patient. Plast. Reconstr. Surg. 2006, 117, 414–430. [Google Scholar] [CrossRef] [PubMed]
- Losco, L.; Roxo, A.C.; Roxo, C.W.; Torto, F.L.; Bolletta, A.; De Sire, A.; Aksoyler, D.; Ribuffo, D.; Cigna, E. Lower Body Lift After Bariatric Surgery: 323 Consecutive Cases Over 10-Year Experience. Aesthetic Plast. Surg. 2019, 44, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Arthurs, Z.M.; Cuadrado, D.; Sohn, V.; Wolcott, K.; Lesperance, K.; Carter, P.; Sebesta, J. Post-bariatric panniculectomy: Pre-panniculectomy body mass index impacts the complication profile. Am. J. Surg. 2007, 193, 567–570. [Google Scholar] [CrossRef] [PubMed]
- Oranges, C.M.; Sisti, A. Medial Thigh Lift in the Massive Weight Loss Population: Outcomes and Complications. Plast. Reconstr. Surg. 2015, 136, 273e–274e. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
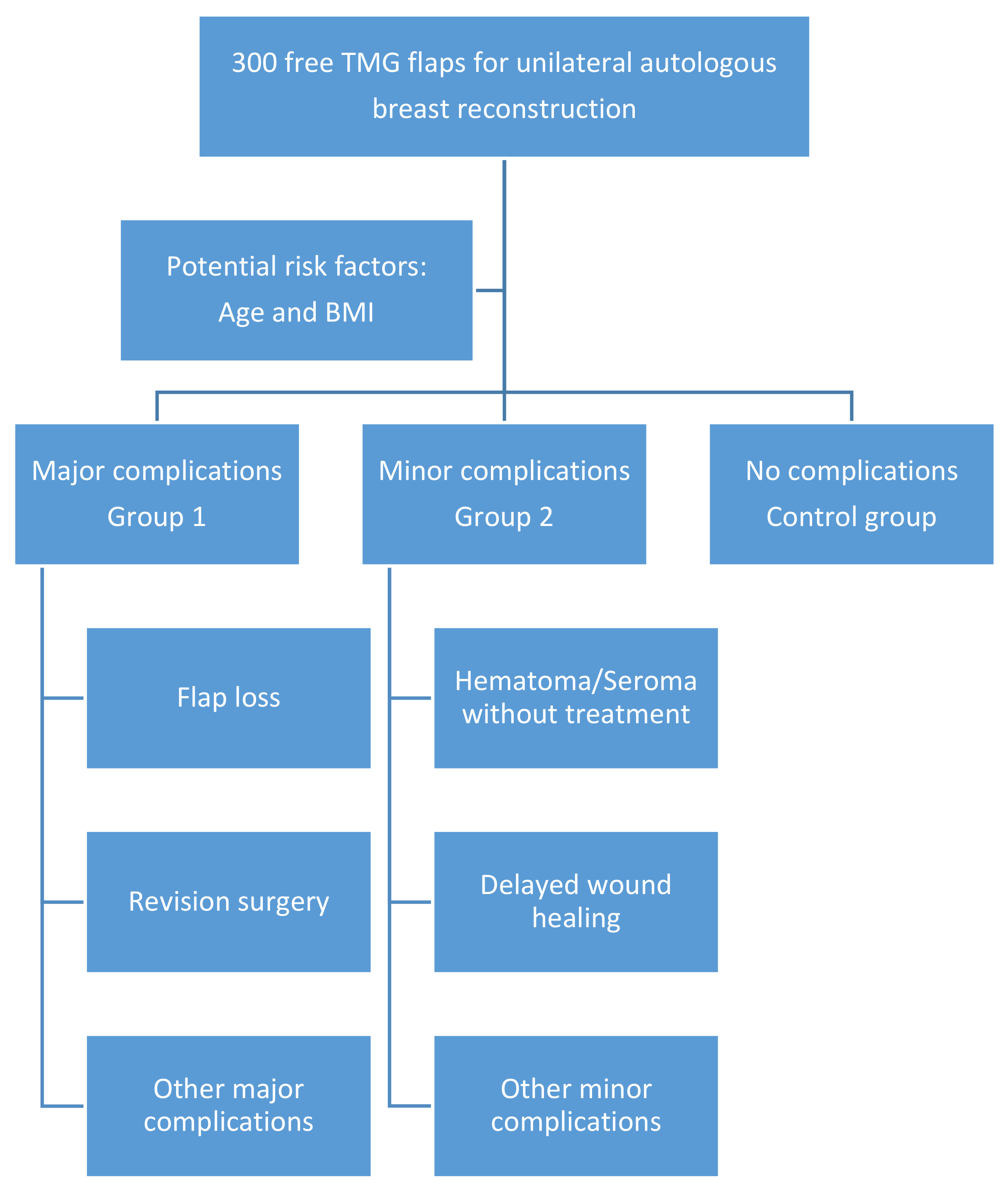
| Major complications | 1. Hematoma or flap insufficiency requiring surgical intervention |
| 2. Seroma requiring aspiration or surgery | |
| 3. Wound-healing problems (also flap or fat necrosis) requiring surgery | |
| 4. Infection requiring iv antibiotics | |
| 5. Deep vein thrombosis/pulmonary embolism | |
| Minor complications | 1. Hematoma without treatment (+erythrocyte substitution with no other treatment necessary) |
| 2. Seroma without treatment | |
| 3. Delayed wound healing | |
| 4. Cellulitis (also fat necrosis) treated with oral antibiotics without hospitalization |
| Patient Characteristics | Number | % | |
|---|---|---|---|
| Cases included | 300 | 100 | |
| Age, years | |||
| Median | 48.0 | ||
| SD | 10.6 | ||
| BMI, kg/m2 | |||
| Mean | 22.9 | ||
| SD | 3.0 | ||
| Radiotherapy | |||
| Yes | 116 | 38.7 | |
| No | 183 | 61.0 | |
| Unknown | 1 | 0.3 | |
| Hormone therapy | |||
| Yes | 120 | 40.0 | |
| No | 180 | 60.0 | |
| Unknown | 0 | ||
| Minor complications | 70 | 23.3 | |
| Major complications | 83 | 27.6 | |
| No complications | 153 | 51.0 | |
| Revision needed | 78 | 26.0 |
| <40 Years | ≥40 Years | p Value | |
|---|---|---|---|
| Minor complication | 18 (25.00%) | 52 (22.81%) | p = 0.644 |
| No complication | 35 | 118 | |
| Relative risk for minor complication for ≥ 40: 0.91 | |||
| Major complication | 21 (29.17%) | 62 (27.19%) | p = 0.676 |
| No complication | 35 | 118 | |
| Relative risk for major complication for ≥40: 0.93 | |||
| All complications | 37 (51.39%) | 110 (48.25%) | p = 0.642 |
| No complication | 35 | 118 | |
| Relative risk for any complication for ≥ 40: 0.94 | |||
| Flap loss | 4 (5.56%) | 15 (6.58%) | p = 0.756 |
| No flap loss | 68 | 213 | |
| Relative risk for flap loss for ≥40: 1.18 | |||
| Revision surgery | 20 (27.78%) | 52 (22.81%) | p = 0.389 |
| No revision surgery | 52 | 176 | |
| Relative risk for revision surgery for ≥40: 0.82 | |||
| <50 years | ≥50 years | ||
| Minor complication | 41 (24.55%) | 29 (21.80%) | p = 0.811 |
| No complication | 87 | 66 | |
| Relative risk for minor complication for ≥ 50: 0.89 | |||
| Major complication | 42 (25.15%) | 41 (30.83%) | p = 0.356 |
| No complication | 87 | 66 | |
| Relative risk for major complication for ≥ 50: 1.23 | |||
| All complications | 80 (47.90%) | 67 (50.38%) | p = 0.671 |
| No complication | 87 | 66 | |
| Relative risk for any complication for ≥ 50: 1.05 | |||
| Flap loss | 11 (6.59%) | 8 (6.02%) | p = 0.839 |
| No flap loss | 156 | 125 | |
| Relative risk for flap loss for ≥ 50: 0.91 | |||
| Revision surgery | 36 (21.56%) | 36 (27.07%) | p = 0.267 |
| No revision surgery | 131 | 97 | |
| Relative risk for revision surgery for ≥50: 1.26 | |||
| <60 years | ≥60 years | ||
| Minor complication | 60 (22.22%) | 10 (33.33%) | p = 0.408 |
| No complication | 137 | 16 | |
| Relative risk for minor complication for ≥ 60: 1.50 | |||
| Major complication | 78 (28.89%) | 5 (16.67%) | p = 0.253 |
| No complication | 137 | 16 | |
| Relative risk for major complication for ≥ 60: 0.58 | |||
| All complications | 133 (49.26%) | 14 (46.67%) | p = 0.788 |
| No complication | 137 | 16 | |
| Relative risk for any complication for ≥ 60: 0.95 | |||
| Flap loss | 19 (7.04%) | 0 (0.00%) | p = 0.133 |
| No flap loss | 251 | 30 | |
| Relative risk for flap loss for ≥ 60: 0.0 | |||
| Revision surgery | 66 (24.44%) | 6 (20.00%) | p = 0.589 |
| No revision surgery | 204 | 24 | |
| Relative risk for revision surgery for ≥60: 0.82 | |||
| <25 BMI (kg/m2) | ≥25 BMI (kg/m2) | Total, p Value | |
|---|---|---|---|
| Minor complication | 56 (24.24%) | 14 (20.29%) | p = 0.708 |
| No complication | 119 | 34 | |
| Relative risk for minor complication for patients with BMI ≥ 25: 0.84 | |||
| Major complication | 61 (26.41%) | 22 (31.88%) | p = 0.460 |
| No complication | 119 | 34 | |
| Relative risk for major complication for patients with BMI ≥ 25: 1.21 | |||
| All complications | 112 (48.48%) | 35 (50.72%) | p = 0.744 |
| No complication | 119 | 34 | |
| Relative risk for any complication for patients with BMI ≥ 25: 1.05 | |||
| Flap loss | 14 (6.06%) | 5 (7.25%) | p = 0.723 |
| No flap loss | 217 | 64 | |
| Relative risk for flap loss for patients with BMI ≥ 25: 1.20 | |||
| Revision surgery | 54 (23.38%) | 18 (26.09%) | p = 0.644 |
| No revision surgery | 177 | 51 | |
| Relative risk for revision surgery for patients with BMI ≥ 25: 1.12 | |||
| <25 BMI (kg/m2) and < 50 Years | ≥25 BMI (kg/m2) and ≥ 50 Years | Total, p Value | |
|---|---|---|---|
| Minor complication | 34 (26.77%) | 7 (24.14%) | p = 0.931 |
| No complication | 66 | 13 | |
| Relative risk for minor complication for patients with BMI ≥ 25 and over 50: 0.90 | |||
| Major complication | 29 (22.83%) | 9 (31.03%) | p = 0.349 |
| No complication | 66 | 13 | |
| Relative risk for major complication for patients with BMI ≥ 25 and over 50: 1.36 | |||
| All complications | 61 (48.03%) | 16 (55.17%) | p = 0.488 |
| No complication | 66 | 13 | |
| Relative risk for any complication for patients with BMI ≥ 25 and over 50: 1.15 | |||
| Flap loss | 8 (6.30%) | 2 (6.90%) | p = 0.906 |
| No flap loss | 119 | 27 | |
| Relative risk for flap loss for patients with BMI ≥ 25 and over 50: 1.10 | |||
| Revision surgery | 25 (19.69%) | 7 (24.14%) | p = 0.592 |
| No revision surgery | 102 | 22 | |
| Relative risk for revision surgery for patients with BMI ≥ 25 and over 50: 1.23 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwaiger, K.; Weitgasser, L.; Mahrhofer, M.; Bachleitner, K.; Abed, S.; Wimbauer, J.; Russe, E.; Schoeller, T.; Wechselberger, G. Age and Overweight Are Not Contraindications for a Breast Reconstruction with a TMG-Flap—A Risk and Complication Analysis of a Retrospective Double Center Study Including 300 Patients. J. Clin. Med. 2021, 10, 926. https://doi.org/10.3390/jcm10050926
Schwaiger K, Weitgasser L, Mahrhofer M, Bachleitner K, Abed S, Wimbauer J, Russe E, Schoeller T, Wechselberger G. Age and Overweight Are Not Contraindications for a Breast Reconstruction with a TMG-Flap—A Risk and Complication Analysis of a Retrospective Double Center Study Including 300 Patients. Journal of Clinical Medicine. 2021; 10(5):926. https://doi.org/10.3390/jcm10050926
Chicago/Turabian StyleSchwaiger, Karl, Laurenz Weitgasser, Maximilian Mahrhofer, Kathrin Bachleitner, Selim Abed, Julia Wimbauer, Elisabeth Russe, Thomas Schoeller, and Gottfried Wechselberger. 2021. "Age and Overweight Are Not Contraindications for a Breast Reconstruction with a TMG-Flap—A Risk and Complication Analysis of a Retrospective Double Center Study Including 300 Patients" Journal of Clinical Medicine 10, no. 5: 926. https://doi.org/10.3390/jcm10050926
APA StyleSchwaiger, K., Weitgasser, L., Mahrhofer, M., Bachleitner, K., Abed, S., Wimbauer, J., Russe, E., Schoeller, T., & Wechselberger, G. (2021). Age and Overweight Are Not Contraindications for a Breast Reconstruction with a TMG-Flap—A Risk and Complication Analysis of a Retrospective Double Center Study Including 300 Patients. Journal of Clinical Medicine, 10(5), 926. https://doi.org/10.3390/jcm10050926