
Comparing Ventricular Synchrony in Left Bundle Branch and Left Ventricular Septal Pacing in Pacemaker Patients

 , , , ,
, , , ,
Abstract
1. Introduction
2. Methods
2.1. Patient Selection
2.2. Implantation Procedure
2.3. Pacing and Capture Definitions
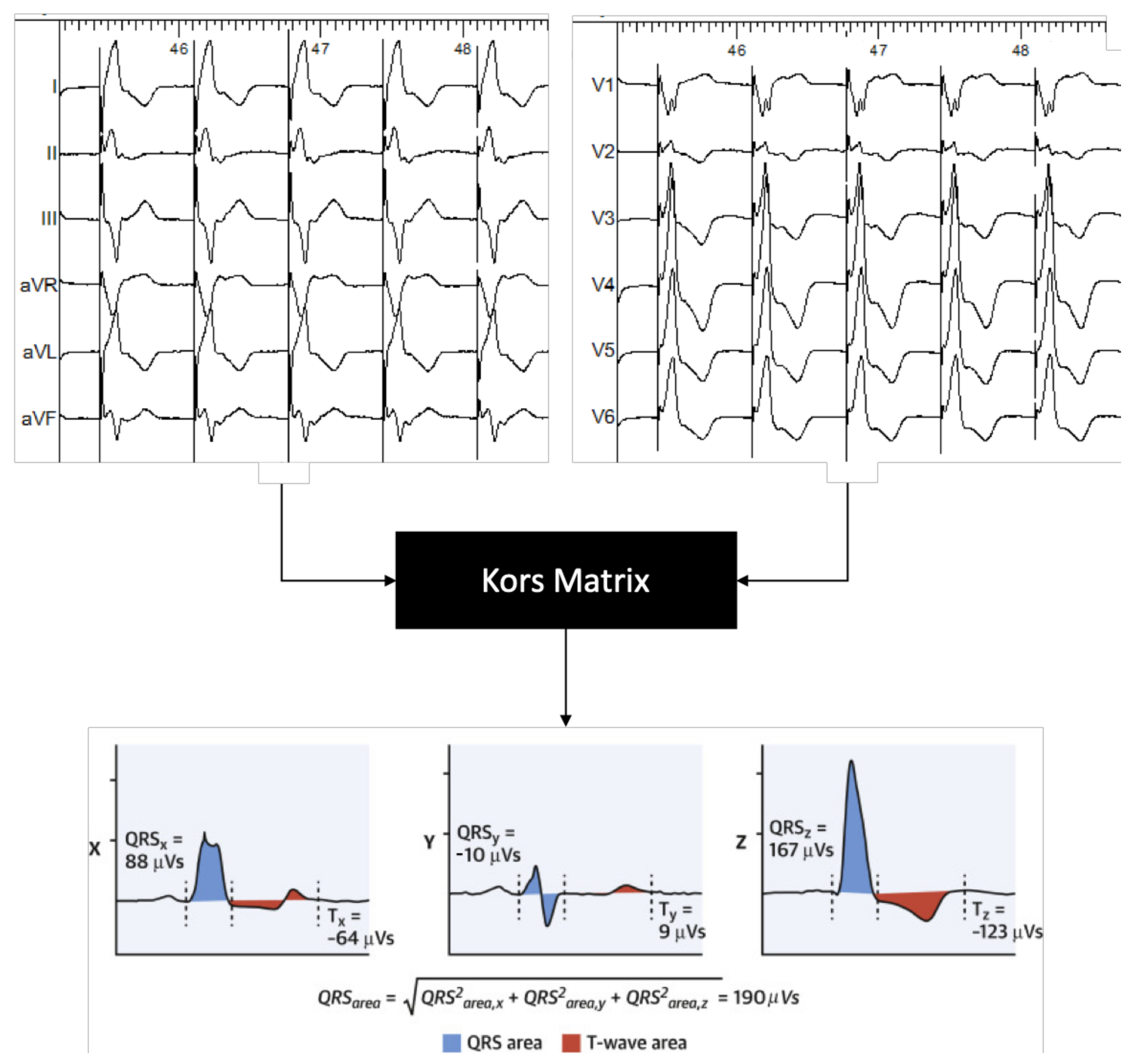
2.4. Electrical Measurements
2.5. Data Collection and Analysis
2.6. Statistical Analysis
3. Results
3.1. Procedure-Related Measurements
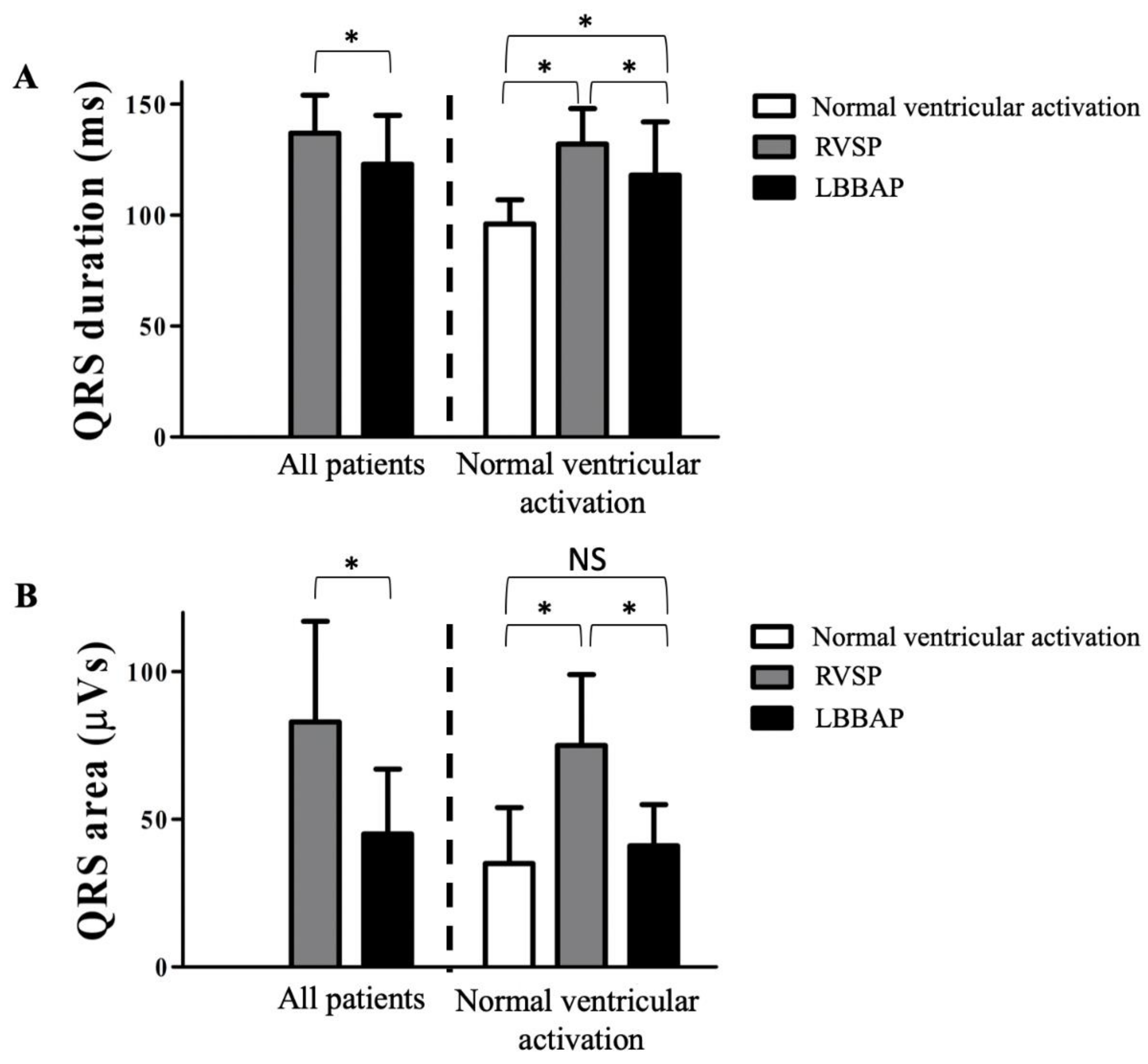
3.2. Electrophysiological Effects of LBBAP
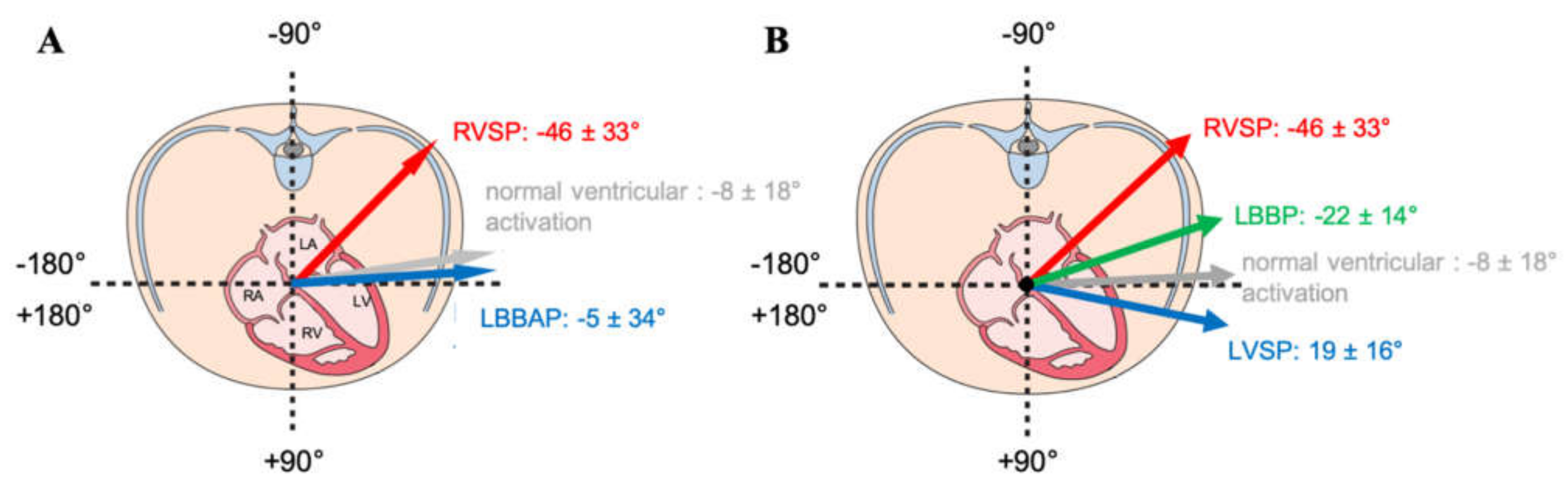
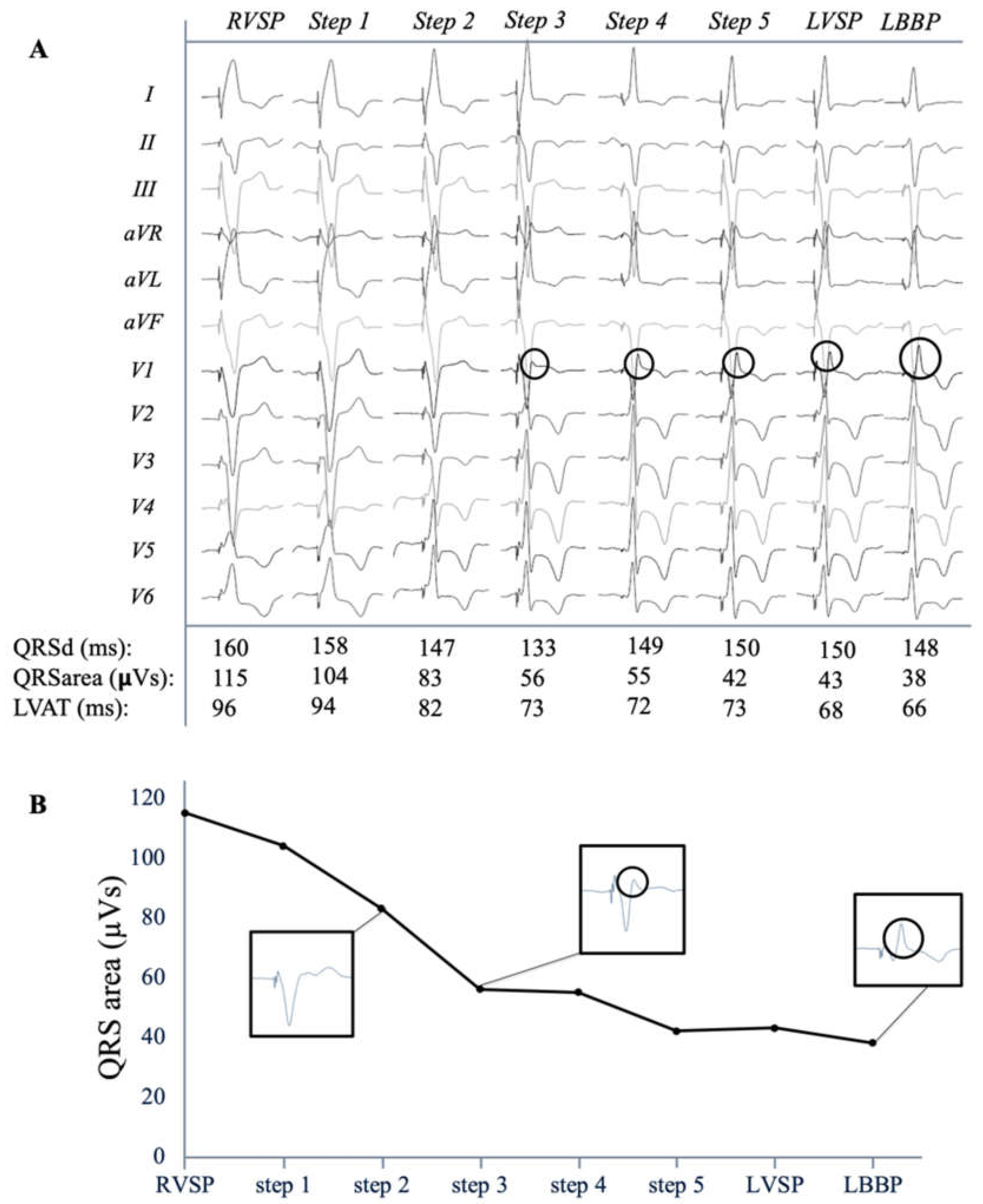
3.3. Electrical Characteristics of LVSP and LBBP
4. Discussion
4.1. QRS Duration in LBBAP
4.2. QRS Morphology in LBBAP
4.3. QRS Area as Measurement for Ventricular Synchrony
4.4. QRS Area in LBBAP
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mills, R.W.; Cornelussen, R.N.; Mulligan, L.J.; Strik, M.; Rademakers, L.M.; Skadsberg, N.D.; van Hunnik, A.; Kuiper, M.; Lampert, A.; Delhaas, T.; et al. Left ventricular septal and left ven-tricular apical pacing chronically maintain cardiac contractile coordination, pump function and efficiency. Circ. Arrhythmia Electrophysiol. 2009, 2, 571–579. [Google Scholar] [CrossRef]
- Mafi-Rad, M.; Luermans, J.G.L.M.; Blaauw, Y.; Janssen, M.; Crijns, H.J.; Prinzen, F.W.; Vernooy, K. Feasibility and Acute Hemodynamic Effect of Left Ventricular Septal Pacing by Transvenous Approach Through the Interventricular Septum. Circ. Arrhythmia Electrophysiol. 2016, 9, e003344. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Su, L.; Wu, S.; Xu, L.; Xiao, F.; Zhou, X.; Ellenbogen, K.A. A Novel Pacing Strategy with Low and Stable Output: Pacing the Left Bundle Branch Immediately Beyond the Conduction Block. Can. J. Cardiol. 2017, 33, 1736.e1–1736.e3. [Google Scholar] [CrossRef] [PubMed]
- Hua, W.; Fan, X.; Li, X.; Niu, H.; Gu, M.; Ning, X.; Hu, Y.; Gold, M.R.; Zhang, S. Comparison of Left Bundle Branch and His Bundle Pacing in Bradycardia Patients. JACC Clin. Electrophysiol. 2020, 6, 1291–1299. [Google Scholar] [CrossRef]
- Hou, X.; Qian, Z.; Wang, Y.; Qiu, Y.; Chen, X.; Jiang, H.; Jiang, Z.; Wu, H.; Zhao, Z.; Zhou, W.; et al. Feasibility and cardiac synchrony of permanent left bundle branch pacing through the interventricular septum. EP Eur. 2019, 21, 1694–1702. [Google Scholar] [CrossRef]
- Engels, E.B.; AlShehri, S.; Van Deursen, C.J.; Wecke, L.; Bergfeldt, L.; Vernooy, K.; Prinzen, F.W. The synthesized vectorcardiogram resembles the measured vectorcardiogram in patients with dyssynchronous heart failure. J. Electrocardiol. 2015, 48, 586–592. [Google Scholar] [CrossRef]
- Mafi Rad, M.; Wijntjens, G.W.; Engels, E.B.; Blaauw, Y.; Luermans, J.G.; Pison, L.; Crijns, H.J.; Prinzen, F.W.; Vernooy, K. Vectorcardiographic QRS area identifies delayed left ventricular lateral wall activation determined by electroanatomic mapping in candidates for cardiac resynchronization therapy. Heart Rhythm. 2016, 13, 217–225. [Google Scholar] [CrossRef] [PubMed]
- van Stipdonk, A.M.W.; Ter Horst, I.; Kloosterman, M.; Engels, E.B.; Rienstra, M.; Crijns, H.; Vos, M.; Van Gelder, I.; Prinzen, F.W.; Meine, M.; et al. QRS Area Is a Strong Determinant of Outcome in Cardiac Resynchronization Therapy. Circ. Arrhythmia Electrophysiol. 2018, 11, e006497. [Google Scholar] [CrossRef]
- Huang, W.; Chen, X.; Su, L.; Wu, S.; Xia, X.; Vijayaraman, P. A beginner’s guide to permanent left bundle branch pacing. Hearth Rhythm. 2019, 16, 1791–1796. [Google Scholar] [CrossRef]
- Engels, E.B.; Vegh, E.M.; Van Deursen, C.J.; Vernooy, K.; Singh, J.P.; Prinzen, F.W. T-wave area predicts response to cardiac resyn-chronization therapy in patients with left bundle branch block. J. Cardiovasc. Electrophysiol. 2015, 26, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Kors, J.A.; van Herpen, G.; Sittig, A.C.; van Bemmel, J.H. Reconstruction of the Frank vectorcardiogram from standard electro-cardiographic leads: Diagnostic comparison of different methods. Eur. Heart J. 1990, 11, 1083–1092. [Google Scholar] [CrossRef]
- Gupta, A.; Parakh, N.; Bansal, R.; Verma, S.K.; Roy, A.; Sharma, G.; Yadav, R.; Naik, N.; Juenja, R.; Bahl, V.K. Correlation of pacing site in right ventricle with paced QRS complex duration. Indian Pacing Electrophysiol. J. 2018, 18, 210–216. [Google Scholar] [CrossRef]
- Khurshid, S.; Liang, J.J.; Owens, A.; Lin, D.; Schaller, R.; Epstein, A.E.; Marchlinski, F.E.; Frankel, D.S. Longer Paced QRS Duration is Associated with Increased Prevalence of Right Ventricular Pacing-Induced Cardiomyopathy. J. Cardiovasc. Electrophysiol. 2016, 27, 1174–1179. [Google Scholar] [CrossRef]
- Khurshid, S.; Epstein, A.E.; Verdino, R.J.; Lin, D.; Goldberg, L.R.; Marchlinski, F.E.; Frankel, D.S. Incidence and predictors of right ventricular pacing-induced cardiomyopathy. Heart Rhythm. 2014, 11, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.C.; Kristensen, L.; Andersen, H.R.; Mortensen, P.T.; Pedersen, O.L.; Pedersen, A.K. A randomized comparison of atrial and dual-chamber pacing in 177 consecutive patients with sick sinus syndrome: Echocardiographic and clinical outcome. J. Am. Coll. Cardiol. 2003, 42, 614–623. [Google Scholar] [CrossRef]
- Sweeney, M.O.; Hellkamp, A.S.; Ellenbogen, K.A.; Greenspon, A.J.; Freedman, R.A.; Lee, K.L.; Lamas, G.A. Adverse Effect of Ventricular Pacing on Heart Failure and Atrial Fibrillation Among Patients with Normal Baseline QRS Duration in a Clinical Trial of Pacemaker Therapy for Sinus Node Dysfunction. Circulation 2003, 107, 2932–2937. [Google Scholar] [CrossRef]
- Chen, K.; Li, Y.; Dai, Y.; Sun, Q.; Luo, B.; Li, C.; Zhang, S. Comparison of electrocardiogram characteristics and pacing parameters between left bundle branch pacing and right ventricular pacing in patients receiving pacemaker therapy. EP Eur. 2018, 21, 673–680. [Google Scholar] [CrossRef]
- Gao, M.-Y.; Tian, Y.; Shi, L.; Wang, Y.-J.; Xie, B.-Q.; Qi, J.; Zeng, L.-J.; Li, X.-X.; Yang, X.-C.; Liu, X.-P. Electrocardiographic morphology during left bundle branch area pacing: Characteristics, underlying mechanisms, and clinical implications. Pacing Clin. Electrophysiol. 2020, 43, 297–307. [Google Scholar] [CrossRef]
- Jastrzębski, M.; Kiełbasa, G.; Moskal, P.; Bednarek, A.; Kusiak, A.; Sondej, T.; Bednarski, A.; Rajzer, M.; Vijayaraman, P. Fixation beats: A novel marker for reaching the left bundle branch area during deep septal lead implantation. Heart Rhythm. 2020. online ahead of print. [Google Scholar] [CrossRef]
- Ghossein, M.A.; van Stipdonk, A.M.W.; Plesinger, F.; Kloosterman, M.; Wouters, P.C.; Salden, O.A.E.; Meine, M.; Maass, A.H.; Prinzen, F.W.; Vernooy, K. Reduction in the QRS area after cardiac resynchronization therapy is associated with survival and echocardiographic response. J. Cardiovasc. Electrophysiol. 2021. [Google Scholar] [CrossRef]
- Li, X.; Li, H.; Ma, W.; Ning, X.; Liang, E.; Pang, K.; Yao, Y.; Hua, W.; Zhang, S.; Fan, X. Permanent left bundle branch area pacing for atrioventricular block: Feasibility, safety, and acute effect. Heart Rhythm. 2019, 16, 1766–1773. [Google Scholar] [CrossRef]
- Cai, B.; Huang, X.; Li, L.; Guo, J.; Chen, S.; Meng, F.; Wang, H.; Lin, B.; Su, M. Evaluation of cardiac synchrony in left bundle branch pacing: Insights from echocardiographic research. J. Cardiovasc. Electrophysiol. 2020, 31, 560–569. [Google Scholar] [CrossRef]
- Chan, J.Y.S.; Huang, W.J.; Yan, B. Non-invasive electrocardiographic imaging of His-bundle and peri-left bundle pacing in left bundle branch block. Europace 2018, 21, 837. [Google Scholar] [CrossRef] [PubMed]
- Salden, F.C.; Luermans, J.G.; Westra, S.W.; Weijs, B.; Engels, E.B.; Heckman, L.I.; Lamerichs, L.J.; Janssen, M.H.; Clerx, K.J.; Cornelussen, R.; et al. Short-Term Hemodynamic and Electrophysiological Effects of Cardiac Resynchronization by Left Ventricular Septal Pacing. J. Am. Coll. Cardiol. 2020, 75, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Jurak, P.; Curila, K.; Leinveber, P.; Prinzen, F.W.; Viscor, I.; Plesinger, F.; Smisek, R.; Prochazkova, R.; Osmancik, P.; Halamek, J.; et al. Novel ultra-high-frequency electrocardiogram tool for the description of the ventricular depolarization pattern before and during cardiac resynchronization. J. Cardiovasc. Electrophysiol. 2019, 31, 300–307. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 50) | Mean ± SD or %. |
|---|---|
| Male sex | 61% |
| Age (years) | 74 ± 10 |
| Medical history | |
| Hypertension | 61% |
| Atrial fibrillation | 44% |
| Coronary artery disease | 37% |
| Myocardial infarction | 17% |
| Echocardiographic parameters | |
| LVEF (%) | 57 ± 7 |
| LV end diastolic diameter (mm) | 51 ± 7 |
| LV end systolic diameter (mm) | 36 ± 8 |
| IVS thickness (mm) | 9 ± 1 |
| Electrocardiographic parameters | |
| Heart rate (bpm) | 66 ± 21 |
| QRS duration (ms) | |
| all patients | 113 ± 29 |
| normal ventricular activation | 95 ± 13 |
| Other (escape, LBTB/RBTB) | 141 ± 25 |
| Pacemaker indication | |
| Sinus bradycardia | 16% |
| Bradycardia-tachycardia syndrome | 12% |
| 3rd degree AV-block | 35% |
| Ablate and pace | 10% |
| Other | 27% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heckman, L.I.B.; Luermans, J.G.L.M.; Curila, K.; Van Stipdonk, A.M.W.; Westra, S.; Smisek, R.; Prinzen, F.W.; Vernooy, K. Comparing Ventricular Synchrony in Left Bundle Branch and Left Ventricular Septal Pacing in Pacemaker Patients. J. Clin. Med. 2021, 10, 822. https://doi.org/10.3390/jcm10040822
Heckman LIB, Luermans JGLM, Curila K, Van Stipdonk AMW, Westra S, Smisek R, Prinzen FW, Vernooy K. Comparing Ventricular Synchrony in Left Bundle Branch and Left Ventricular Septal Pacing in Pacemaker Patients. Journal of Clinical Medicine. 2021; 10(4):822. https://doi.org/10.3390/jcm10040822
Chicago/Turabian StyleHeckman, Luuk I.B., Justin G.L.M. Luermans, Karol Curila, Antonius M.W. Van Stipdonk, Sjoerd Westra, Radovan Smisek, Frits W. Prinzen, and Kevin Vernooy. 2021. "Comparing Ventricular Synchrony in Left Bundle Branch and Left Ventricular Septal Pacing in Pacemaker Patients" Journal of Clinical Medicine 10, no. 4: 822. https://doi.org/10.3390/jcm10040822
APA StyleHeckman, L. I. B., Luermans, J. G. L. M., Curila, K., Van Stipdonk, A. M. W., Westra, S., Smisek, R., Prinzen, F. W., & Vernooy, K. (2021). Comparing Ventricular Synchrony in Left Bundle Branch and Left Ventricular Septal Pacing in Pacemaker Patients. Journal of Clinical Medicine, 10(4), 822. https://doi.org/10.3390/jcm10040822