
Medication-Related Problems in Older People with Multimorbidity in Catalonia: A Real-World Data Study with 5 Years’ Follow-Up

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
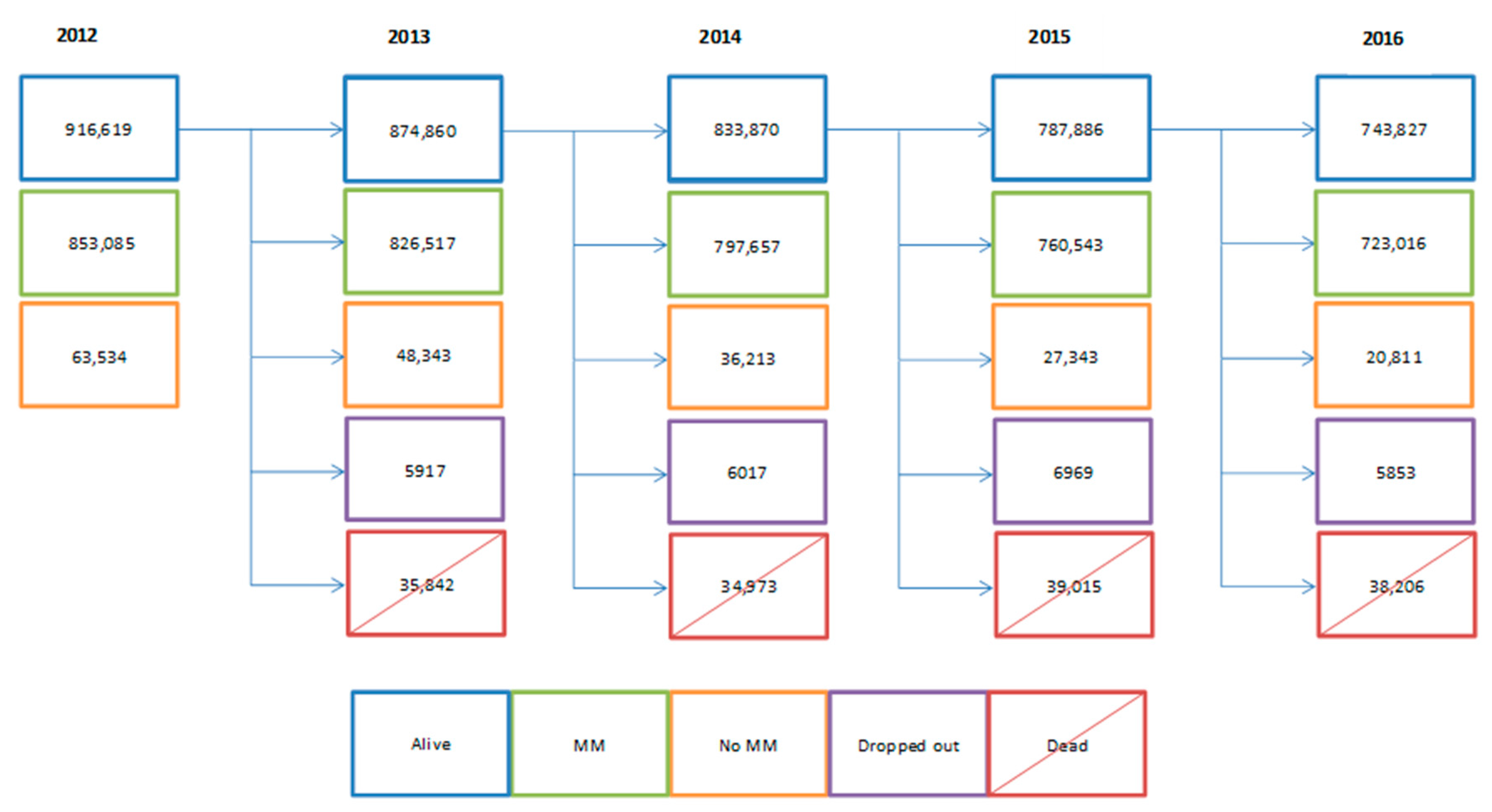
2.1. Design, Setting, and Study Population
2.2. Dataset
2.3. Variables
2.3.1. Chronic Diseases and Multimorbidity
2.3.2. Drugs
2.3.3. Kidney Function
2.3.4. Liver Function
2.3.5. Other Variables
2.3.6. Medication-Related Problems
- -
- Duplicate therapy: prescription of two or more drugs that have the same pharmacological activity. We included duplicate therapies that posed an important clinical risk, according to professional consensus. Our study did not consider combinations of active principles with the same pharmacological action that physicians used to achieve a synergistic effect or to adjust doses [23].
- -
- Drug–drug interaction: when one drug’s activity or effect alters the action of another. We focused on interactions that were life-threatening due to therapeutic failure or toxicity, identifying interactions with the highest level of severity (contraindication) from the Thesaurus des interactions médicamenteuses from France’s Agence Nationale de Sécurité du Médicament et des Produits de Santé (ANSM) [26] and comparing that information with a second source [27,28] or contrasting it with professional consensus [23].
- -
- -
- -
- PIMs in older people (≥65 years old): when the risk of adverse events associated with the drug exceeded the expected clinical benefits, and there was no clear scientific evidence pointing to a specific indication or supporting its cost-effectiveness. We primarily used the STOPP/START criteria [31], which was complemented with Beers’ criteria [32], PRISCUS, and updates from other sources [33,34,35,36,37,38,39,40]. Different definitions of PIMs exist: Durán et al. defined them as drug combinations with a clinically relevant anticholinergic effect [38], while other authors have included drugs that increase the risk of falling or affect the QT interval with known risk, antiulcer agents administered without considering gastroprotection, and other drugs that are inadvisable for older people or patients needing gastroprotection [23].
2.4. Ethics
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Palladino, R.; Lee, J.T.; Ashworth, M.; Triassi, M.; Millett, C. Associations between Multimorbidity, Healthcare Utilisation and Health Status: Evidence from 16 European Countries. Age Ageing 2016, 45, 431–435. [Google Scholar] [CrossRef]
- Violan, C.; Foguet-Boreu, Q.; Flores-Mateo, G.; Salisbury, C.; Blom, J.; Freitag, M.; Glynn, L.; Muth, C.; Valderas, J.M. Prevalence, Determinants and Patterns of Multimorbidity in Primary Care: A Systematic Review of Observational Studies. PLoS ONE 2014, 9, 3–11. [Google Scholar] [CrossRef]
- Prados-Torres, A.; Poblador-Plou, B.; Calderón-Larrañaga, A.; Gimeno-Feliu, L.A.; González-Rubio, F.; Poncel-Falcó, A.; Sicras-Mainar, A.; Alcalá-Nalvaiz, J.T. Multimorbidity Patterns in Primary Care: Interactions among Chronic Diseases Using Factor Analysis. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- Marengoni, A.; Onder, G. Guidelines, Polypharmacy, and Drug-Drug Interactions in Patients with Multimorbidity: A Cascade of Failure. BMJ 2015, 350, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Rijken, M.; Struckmann, V.; Van der Heide, I.; Hujala, A.; Barbabella, F.; Van Ginneken, E.; Shellevis, F. How to Improve Care for People with Multimorbidity in Europe? Eur. Obs. Policy Briefs 2017, 1–31. [Google Scholar]
- Pharmaceutical Care Network Europe. Available online: https://www.pcne.org/ (accessed on 3 December 2019).
- Prados-Torres, A.; Del Cura-González, I.; Prados-Torres, D.; López-Rodríguez, J.A.; Leiva-Fernández, F.; Calderón-Larrañaga, A.; López-Verde, F.; Gimeno-Feliu, L.A.; Escortell-Mayor, E.; Pico-Soler, V.; et al. Effectiveness of an Intervention for Improving Drug Prescription in Primary Care Patients with Multimorbidity and Polypharmacy: Study Protocol of a Cluster Randomized Clinical Trial (Multi-PAP Project). Implement. Sci. 2017, 12, 1–10. [Google Scholar] [CrossRef]
- World Health Organization. Medication Without Harm; World Health Organization: Geneva, Switzerland, 2017; p. 16. [Google Scholar]
- APEAS Study. Patient Safety in Primary Health Care; Ministry of Health & Consumer Affairs: Madrid, Spain, 2008.
- Gnädinger, M.; Conen, D.; Herzig, L.; Puhan, M.A.; Staehelin, A.; Zoller, M.; Ceschi, A. Medication Incidents in Primary Care Medicine: A Prospective Study in the Swiss Sentinel Surveillance Network (Sentinella). BMJ Open 2017, 7, 1–12. [Google Scholar] [CrossRef]
- Baena, M.I.; Faus, M.J.; Fajardo, P.C.; Luque, F.M.; Sierra, F.; Martinez-Olmos, J.; Cabrera, A.; Fernandez-Llimos, F.; Martinez-Martinez, F.; Jiménez, J.; et al. Medicine-Related Problems Resulting in Emergency Department Visits. Eur. J. Clin. Pharmacol. 2006, 62, 387–393. [Google Scholar] [CrossRef]
- Parameswaran Nair, N.; Chalmers, L.; Bereznicki, B.J.; Curtain, C.M.; Bereznicki, L.R. Repeat Adverse Drug Reaction-Related Hospital Admissions in Elderly Australians: A Retrospective Study at the Royal Hobart Hospital. Drugs Aging 2017, 34, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of Multimorbidity and Implications for Health Care, Research, and Medical Education: A Cross-Sectional Study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Corsonello, A.; Pedone, C.; Incalzi, R. Age-Related Pharmacokinetic and Pharmacodynamic Changes and Related Risk of Adverse Drug Reactions. Curr. Med. Chem. 2010, 17, 571–584. [Google Scholar] [CrossRef] [PubMed]
- Idescat. Statistical Yearbook of Catalonia. Available online: https://www.idescat.cat/pub/?id=aec&lang=en (accessed on 27 November 2019).
- Memòria D’activitats 2012. Institut Català de la Salut. Available online: http://ics.gencat.cat/es/detall/publicacio/memoria_2012-00007 (accessed on 30 November 2019).
- Ramos, R.; Balló, E.; Marrugat, J.; Elosua, R.; Sala, J.; Grau, M.; Vila, J.; Bolíbar, B.; García-Gil, M.; Martí, R.; et al. Validez Del Sistema de Información Para El Desarrollo de La Investigación En Atención Primaria (SIDIAP) En El Estudio de Enfermedades Vasculares: Estudio EMMA. Rev. Esp. Cardiol. 2012, 65, 29–37. [Google Scholar] [CrossRef] [PubMed]
- García-Gil, M.; Hermosilla, E.; Prieto-Alhambra, D.; Fina, F.; Rosell, M.; Ramos, R.; Rodriguez, J.; Williams, T.; Van Staa, T.; Bolíbar, B. Construction and Validation of a Scoring System for the Selection of High-Quality Data in a Spanish Population Primary Care Database (SIDIAP). Inform. Prim. Care 2011, 19, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Larrañaga, A.; Vetrano, D.L.; Onder, G.; Gimeno-Feliu, L.A.; Coscollar-Santaliestra, C.; Carfí, A.; Pisciotta, M.S.; Angleman, S.; Melis, R.J.F.; Santoni, G.; et al. Assessing and Measuring Chronic Multimorbidity in the Older Population: A Proposal for Its Operationalization. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 1417–1423. [Google Scholar] [CrossRef]
- WHO. The Anatomical Therapeutic Chemical Classification System with Defined Daily Doses (ATC/DDD); WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What Is Polypharmacy? A Systematic Review of Definitions. BMC Geriatr. 2017, 17, 1–10. [Google Scholar] [CrossRef]
- Elorza-Ricart, J.M.; Tovillas-Morán, F.J.; Oliveras-Puig, A.; Galcerán, J.M.; Fina, F.; Dalfó-Baqué, A. Estudio Transversal Comparativo de Las Fórmulas CKD-EPI y MDRD-4 a Partir de La Historia Clínica Informatizada de Atención Primaria de Barcelona. Hipertens. Riesgo Vasc. 2012, 29, 118–129. [Google Scholar] [CrossRef]
- Troncoso-Mariño, A.; López-Jiménez, T.; Roso-Llorach, A.; Villén, N.; Amado-Guirado, E.; Guisado-Clavero, M.; Fernández-Bertolin, S.; Vigues, M.P.; Foguet-Boreu, Q.; Violán, C. Medication-related Problems in Older People in Catalonia: A Real-world Data Study. Pharmacoepidemiol. Drug Saf. 2020, 1–9. [Google Scholar] [CrossRef]
- Forns, J.; Cainzos-Achirica, M.; Hellfritzsch, M.; Morros, R.; Poblador-Plou, B.; Hallas, J.; Giner-Soriano, M.; Prados-Torres, A.; Pottegård, A.; Cortés, J.; et al. Validity of ICD-9 and ICD-10 Codes Used to Identify Acute Liver Injury: A Study in Three European Data Sources. Pharmacoepidemiol. Drug Saf. 2019, 28, 965–975. [Google Scholar] [CrossRef]
- Domínguez-Berjón, M.F.; Borrell, C.; Cano-Serral, G.; Esnaola, S.; Nolasco, A.; Pasarín, M.I.; Ramis, R.; Saurina, C.; Escolar-Pujolar, A. Construcción de Un Índice de Privación a Partir de Datos Censales En Grandes Ciudades Españolas (Proyecto MEDEA). Gac. Sanit. 2008, 22, 179–187. [Google Scholar] [CrossRef]
- Thesaurus Des Interactions Médicamenteuses; Agence Nationale de Sécurité du Médicament et des Produits de Santé (ANSM): Saint-Denis, France, 2018.
- Joint Formulary Committee. British National Formulary (BNF). Available online: https://about.medicinescomplete.com/publication/british-national-formulary/ (accessed on 30 November 2019).
- Lexicomp® Drug Interactions-UpToDate. Available online: https://146.219.19.12/drug-interactions/?source=responsive_home#di-disclaimer (accessed on 27 November 2018).
- Pautes per a l’harmonització Del Tractament Farmacològic de La Malaltia Renal Crònica. In Programa d’Harmonització Farmacoterèutica de Medicaments en l’Àmbit l’Atenció Primària i Comunitària del Servei Català la Salut; Agència de Qualitat i Avaluació Sanitàries de Catalunya: Barcelona, España, 2014; pp. 1–31.
- Consejo General de Colegios Oficiales de Farmacéuticos. Botplusweb.portalfarma.com. BOT Plus 2. Base de Datos de Medicamentos. Available online: https://botplusweb.portalfarma.com/botplus.aspx?accion=INICIO (accessed on 27 November 2019).
- Delgado Silveira, E.; Montero Errasquín, B.; Muñoz García, M.; Vélez-Díaz-Pallarés, M.; Lozano Montoya, I.; Sánchez-Castellano, C.; Cruz-Jentoft, A.J. Mejorando La Prescripción de Medicamentos En Las Personas Mayores: Una Nueva Edición de Los Criterios STOPP-START. Rev. Esp. Geriatr. Gerontol. 2015, 50, 89–96. [Google Scholar] [CrossRef]
- Samuel, M.J. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2015, 63, 2227–2246. [Google Scholar] [CrossRef]
- Stefanie, H.; Sven Schmiedl, P.A.T. Potentially Inappropriate Medications in the Elderly: The PRISCUS List. Dtsch Arztebl Int. 2010, 107, 543–551. [Google Scholar] [CrossRef]
- Laroche, M.L.; Charmes, J.P.; Merle, L. Potentially Inappropriate Medications in the Elderly: A French Consensus Panel List. Eur. J. Clin. Pharmacol. 2007, 63, 725–731. [Google Scholar] [CrossRef]
- Matanović, S.M.; Vlahovic-Palcevski, V. Potentially Inappropriate Medications in the Elderly: A Comprehensive Protocol. Eur. J. Clin. Pharmacol. 2012, 68, 1123–1138. [Google Scholar] [CrossRef] [PubMed]
- Ferrandis Tebar, V.; Moreno Sánchez, E.; Obreo Pintos, J.; Viñuela Álvarez, D. Revisión de La Medicación En El Paciente Anciano. In Listado de Medicamentos Susceptibles de Ser Inadecuados; Junta de Castilla y León: León, España, 2018. [Google Scholar]
- Notas informativas de La AEMPS-Agencia Española de Medicamentos y Productos Sanitarios. Available online: https://www.aemps.gob.es/acciones-informativas/notas-informativas-de-la-aemps/?cat=49&tag=seguridad-8 (accessed on 27 November 2019).
- Durán, C.E.; Azermai, M.; Stichele, R.H.V. Systematic Review of Anticholinergic Risk Scales in Older Adults. Eur. J. Clin. Pharmacol. 2013, 69, 1485–1496. [Google Scholar] [CrossRef]
- Rochon, P.A. Drug Prescribing for Older Adults; Schmader, K.E., Givens, J., Eds.; Uptodate: Waltham, MA, USA, 2020. [Google Scholar]
- Woosley, R.L.; Heise, C.W.; Gallo, T.; Tate, J.; Woosley, D.; Romero, K.A. QTdrugs List. Available online: www.CredibleMeds.org (accessed on 27 November 2019).
- Mannucci, P.M.; Nobili, A.; REPOSI Investigators. Multimorbidity and Polypharmacy in the Elderly: Lessons from REPOSI. Intern. Emerg. Med. 2014, 9, 723–734. [Google Scholar] [CrossRef] [PubMed]
- Pintor-Mármol, A.; Baena, M.I.; Fajardo, P.C.; Sabater-Hernández, D.; Sáez-Benito, L.; García-Cárdenas, M.V.; Fikri-Benbrahim, N.; Azpilicueta, I.; José, F.M. Terms Used in Patient Safety Related to Medication: A Literature Review. Pharmacoepidemiol. Drug Saf. 2012, 21, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Cahir, C.; Fahey, T.; Teeling, M.; Teljeur, C.; Feely, J.; Bennett, K. Potentially Inappropriate Prescribing and Cost Outcomes for Older People: A National Population Study. Br. J. Clin. Pharmacol. 2010, 69, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Dima, M.Q.; Jocelyn, W.; Philip, L.S.; Victoria Gillet, G.C.A. Changes in Prescription and Over-the-Counter Medication and Dietary Supplement Use Among Older Adults in the United States, 2005 vs 2011. JAMA Intern. Med. 2016, 176, 473–482. [Google Scholar] [CrossRef]
- Tesfaye, W.H.; Castelino, R.L.; Wimmer, B.C.; Zaidi, S.T.R. Inappropriate Prescribing in Chronic Kidney Disease: A Systematic Review of Prevalence, Associated Clinical Outcomes and Impact of Interventions. Int. J. Clin. Pract. 2017, 71, 1–16. [Google Scholar] [CrossRef]
- Moriarty, F.; Bennett, K.; Fahey, T.; Kenny, R.A.; Cahir, C. Longitudinal Prevalence of Potentially Inappropriate Medicines and Potential Prescribing Omissions in a Cohort of Community-Dwelling Older People. Eur. J. Clin. Pharmacol. 2015, 71, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Bruin-Huisman, L.; Abu-Hanna, A.; Van Weert, H.C.P.M.; Beers, E. Potentially Inappropriate Prescribing to Older Patients in Primary Care in the Netherlands: A Retrospective Longitudinal Study. Age Ageing 2017, 46, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Classen, D.C.; Pestotnik, S.L.; Evans, R.S.; Lloyd, J.F.; Burke, J.P. Adverse Drug Events in Hospitalized Patients: Excess Length of Stay, Extra Costs, and Attributable Mortality. JAMA 1997, 277, 301–306. [Google Scholar] [CrossRef]
- Munir, P.; Sally, J.; Shaun, M.; Chris, G.; Andrew, K.S.; Thomas, J.W.; Keith Farrar, B.; Kevin Park, A.M.B. Adverse Drug Reactions as Cause of Admission to Hospital: Prospective Analysis of 18 820 Patients. BMJ 2004, 329, 15–19. [Google Scholar] [CrossRef]
- Schmiedl, S.; Rottenkolber, M.; Hasford, J.; Rottenkolber, D.; Farker, K.; Drewelow, B.; Hippius, M.; Saljé, K.; Thürmann, P. Self-Medication with over-the-Counter and Prescribed Drugs Causing Adverse-Drug-Reaction-Related Hospital Admissions: Results of a Prospective, Long-Term Multi-Centre Study. Drug Saf. 2014, 37, 225–235. [Google Scholar] [CrossRef]
- Farmer, C.; Fenu, E.; O’Flynn, N.; Guthrie, B. Clinical Assessment and Management of Multimorbidity: Summary of NICE Guidance. BMJ 2016, 354, 1–5. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | N Comorbidities | |||||||
|---|---|---|---|---|---|---|---|---|
| 2–4 Diseases N = 137,799 | 5–9 Diseases N = 393,672 | ≥10 Diseases N = 191,545 | Total N = 723,016 | |||||
| n (%) * | n (%) * | n (%) * | n (%) * | |||||
| Sex, women, n (%) | 73,137 (53.1) | 229,870 (58.4) | 123,014 (64.2) | 426,021 (58.9) | ||||
| Age, median (IQR) | 71.00 [67.00,76.00] | 73.00 [68.00;79.00] | 76.00 [71.00;80.00] | 74.00 [68.00;79.00] | ||||
| Rural | 30,094 (22.5) | 78,760 (20.6) | 31,752 (17.2) | 140,606 (20.1) | ||||
| MEDEA Index † | ||||||||
| Q1 | 26,608 (19.9) | 63,322 (16.6) | 27,986 (15.1) | 117,916 (16.8) | ||||
| Q2 | 22,006 (16.5) | 62,570 (16.4) | 30,182 (16.3) | 114,758 (16.4) | ||||
| Q3 | 20,866 (15.6) | 63,789 (16.7) | 31,480 (17.0) | 116,135 (16.6) | ||||
| Q4 | 19,243 (14.4) | 61,187 (16.0) | 32,159 (17.4) | 112,589 (16.1) | ||||
| Q5 | 14,944 (11.2) | 52,323 (13.7) | 31,567 (17.1) | 98,834 (14.1) | ||||
| Number of drugs | 2012 | 2016 | 2012 | 2016 | 2012 | 2016 | 2012 | 2016 |
| 0 | 34,937 (25.4) | 26,903 (19.5) | 32,578 (8.3) | 16,833 (4.3) | 7104 (3.7) | 1918 (1.0) | 74,619 (10.3) | 45,654 (6.3) |
| 1 | 21,226 (15.4) | 21,234 (15.4) | 24,267 (6.2) | 19,235 (4.9) | 2774 (1.5) | 1661 (0.9) | 48,267 (6.7) | 42,130 (5.8) |
| 2–4 | 57,435 (41.7) | 62,554 (45.4) | 136,887 (34.8) | 130,158 (33.1) | 26,751 (14.0) | 19,860 (10.4) | 221,073 (30.6) | 212,572 (29.4) |
| 5–9 | 22,892 (16.6) | 25,954 (18.8) | 169,574 (43.1) | 191,213 (48.6) | 95,389 (49.8) | 94,522 (49.4) | 287,855 (39.8) | 311,689 (43.1) |
| ≥10 | 1309 (1.0) | 1154 (0.8) | 30,366 (7.7) | 36,233 (9.2) | 59,527 (31.1) | 73,584 (38.4) | 91,202 (12.6) | 110,971 (15.4) |
| Number of visits | ||||||||
| 0 | 13,639 (9.9) | 10,299 (7.5) | 12,374 (3.1) | 5901 (1.5) | 3147 (1.6) | 858 (0.5) | 29,160 (4.0) | 17,058 (2.4) |
| 1 | 11,341 (8.2) | 10,419 (7.6) | 10,723 (2.7) | 9130 (2.3) | 1523 (0.8) | 1276 (0.7) | 23,587 (3.3) | 20,825 (2.9) |
| 2–4 | 38,129 (27.7) | 38,161 (27.7) | 57,257 (14.5) | 52,043 (13.2) | 10,123 (5.3) | 8725 (4.6) | 105,509 (14.6) | 98,929 (13.7) |
| 5–9 | 45,344 (32.9) | 46,684 (33.9) | 128,738 (32.7) | 123,262 (31.3) | 37,760 (19.7) | 32,163 (16.8) | 211,842 (29.3) | 202,109 (28.0) |
| ≥10 | 29,346 (21.3) | 32,236 (23.4) | 184,580 (46.9) | 203,336 (51.7) | 138,992 (72.6) | 148,523 (77.5) | 352,918 (48.8) | 384,095 (53.1) |
| CKD | 6809 (4.9) | 10,907 (7.9) | 53,110 (13.5) | 96,875 (24.6) | 49,182 (25.7) | 88,954 (46.4) | 109,101 (15.1) | 196,736 (27.2) |
| Chronic liver disease | 4495 (3.3) | 5228 (3.8) | 22,105 (5.6) | 26,888 (6.8) | 16,883 (8.8) | 22,511 (11.8) | 43,483 (6.0) | 54,627 (7.6) |
| N Comorbidities | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Medication-Related Problems | 2–4 Diseases N = 137,799 | 5–9 Diseases N = 393,672 | ≥10 Diseases N = 191,545 | Total N = 723,016 | |||||
| n (%) | n (%) | n (%) | n (%) | ||||||
| 2012 | 2016 | 2012 | 2016 | 2012 | 2016 | 2012 | 2016 | ||
| Duplicate therapy | 6853 (5.0) | 3565 (2.6) | 40,507 (10.3) | 22,070 (5.6) | 33,997 (17.8) | 19,370 (10.1) | 81,357 (11.3) | 45,005 (6.2) | |
| Drug–drug interactions | 396 (0.3) | 172 (0.1) | 2616 (0.7) | 1473 (0.4) | 3100 (1.6) | 1817 (1.0) | 6112 (0.9) | 3462 (0.5) | |
| Contraindicated drugs in CKD | 3606 (2.6) | 5199 (3.8) | 37,386 (9.5) | 62,808 (16.0) | 39,474 (20.6) | 65,962 (34.4) | 80,466 (11.1) | 133,969 (18.5) | |
| Contraindicated drugs in liver disease | 2012 (1.5) | 2495 (1.8) | 13,812 (3.5) | 17,959 (4.6) | 12,302 (6.4) | 17,790 (9.3) | 28,126 (3.9) | 38,244 (5.3) | |
| Potentially inappropriate medication | 49,999 (36.3) | 60,353 (43.8) | 245,447 (62.4) | 282,150 (71.7) | 156,710 (81.8) | 171,641 (89.6) | 452,156 (62.5) | 514,144 (71.1) | |
| N Comorbidities | ||||||||
|---|---|---|---|---|---|---|---|---|
| Reason for Drug Inappropriateness | 2–4 Diseases N = 60,353 | 5–9 Diseases N = 282,150 | ≥10 Diseases N = 171,641 | Total N = 514,144 | ||||
| n (%) | n (%) | n (%) | n (%) | |||||
| 2012 | 2016 | 2012 | 2016 | 2012 | 2016 | 2012 | 2016 | |
| Anticholinergic effect–anticholinergic load* | ||||||||
| Score = 1 | 7011 (11.6) | 10,910 (18.1) | 42,699 (15.1) | 61,400 (21.8) | 34,069 (19.9) | 45,155 (26.3) | 83,779 (16.3) | 117,465 (22.9) |
| Score = 2 | 3614 (6.0) | 5104 (8.5) | 25,833 (9.2) | 32,771 (11.6) | 22,269 (13.0) | 27,232 (15.9) | 51,716 (10.1) | 65,107 (12.7) |
| Score = 3–5 | 1209 (2.0) | 1499 (2.5) | 9929 (3.5) | 13,023 (4.6) | 11,885 (6.9) | 15,429 (9.0) | 23,023 (4.5) | 29,951 (5.8) |
| Score ≥ 6 | 39 (0.1) | 37 (0.1) | 307 (0.1) | 315 (0.1) | 484 (0.3) | 436 (0.3) | 830 (0.2) | 788 (0.2) |
| Increase in fall risk | 26,366 (43.7) | 36,430 (60.4) | 145,741 (51.7) | 184,449 (65.4) | 107,661 (62.7) | 125,913 (73.4) | 279,768 (54.4) | 346,792 (67.5) |
| Effect on QT interval | 4834 (8.0) | 6814 (11.3) | 34,387 (12.2) | 43,157 (15.3) | 32,334 (18.8) | 37,491 (21.8) | 71,555 (13.9) | 87,462 (17.0) |
| Antiulcer agents without criteria for gastroprotection | 11,821 (19.6) | 15,761 (26.1) | 81,766 (29.0) | 99,292 (35.2) | 65,395 (38.1) | 74,812 (43.6) | 158,982 (30.9) | 189,865 (36.9) |
| Other drugs not recommended for older people | 9396 (15.6) | 24,069 (39.9) | 72,664 (25.8) | 141,221 (50.1) | 65,478 (38.2) | 109,566 (63.8) | 147,538 (28.7) | 274,856 (53.5) |
| Patients needing gastroprotection | 70 (0.1) | 132 (0.2) | 524 (0.2) | 683 (0.2) | 344 (0.2) | 325 (0.2) | 938 (0.2) | 1140 (0.2) |
| Medication-Related Problems | HR (Crude) 95% CI | Complete Case Analysis HR (Adjusted) * 95% CI | Multiple Imputation HR (Adjusted) * 95% CI |
|---|---|---|---|
| Duplicate therapy | 1.14 (1.12–1.16) | 1.06 (1.04–1.07) | 1.06 (1.04–1.08) |
| Drug–drug interactions | 2.02 (1.95–2.10) | 1.62 (1.55–1.70) | 1.60 (1.54–1.66) |
| Contraindicated drugs in chronic kidney disease | 1.74 (1.72–1.76) | 1.06 (1.05–1.08) | 1.08 (1.06–1.09) |
| Contraindicated drugs in liver disease | 1.59 (1.56–1.62) | 1.59 (1.56–1.63) | 1.54 (1.50–1.57) |
| Potentially inappropriate medication in older people | 1.76 (1.74–1.78) | 1.31 (1.29–1.32) | 1.30 (1.29–1.32) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Troncoso-Mariño, A.; Roso-Llorach, A.; López-Jiménez, T.; Villen, N.; Amado-Guirado, E.; Fernández-Bertolin, S.; Carrasco-Ribelles, L.A.; Borras, J.M.; Violán, C. Medication-Related Problems in Older People with Multimorbidity in Catalonia: A Real-World Data Study with 5 Years’ Follow-Up. J. Clin. Med. 2021, 10, 709. https://doi.org/10.3390/jcm10040709
Troncoso-Mariño A, Roso-Llorach A, López-Jiménez T, Villen N, Amado-Guirado E, Fernández-Bertolin S, Carrasco-Ribelles LA, Borras JM, Violán C. Medication-Related Problems in Older People with Multimorbidity in Catalonia: A Real-World Data Study with 5 Years’ Follow-Up. Journal of Clinical Medicine. 2021; 10(4):709. https://doi.org/10.3390/jcm10040709
Chicago/Turabian StyleTroncoso-Mariño, Amelia, Albert Roso-Llorach, Tomás López-Jiménez, Noemí Villen, Ester Amado-Guirado, Sergio Fernández-Bertolin, Lucía A. Carrasco-Ribelles, Josep Ma Borras, and Concepción Violán. 2021. "Medication-Related Problems in Older People with Multimorbidity in Catalonia: A Real-World Data Study with 5 Years’ Follow-Up" Journal of Clinical Medicine 10, no. 4: 709. https://doi.org/10.3390/jcm10040709
APA StyleTroncoso-Mariño, A., Roso-Llorach, A., López-Jiménez, T., Villen, N., Amado-Guirado, E., Fernández-Bertolin, S., Carrasco-Ribelles, L. A., Borras, J. M., & Violán, C. (2021). Medication-Related Problems in Older People with Multimorbidity in Catalonia: A Real-World Data Study with 5 Years’ Follow-Up. Journal of Clinical Medicine, 10(4), 709. https://doi.org/10.3390/jcm10040709