
Is There Pathological Uniformity between the Periphery and Center of a Gastrointestinal Stromal Tumor?

 , and
, and
Abstract
1. Introduction
2. Methods
2.1. Patients
2.2. Surgical Resection
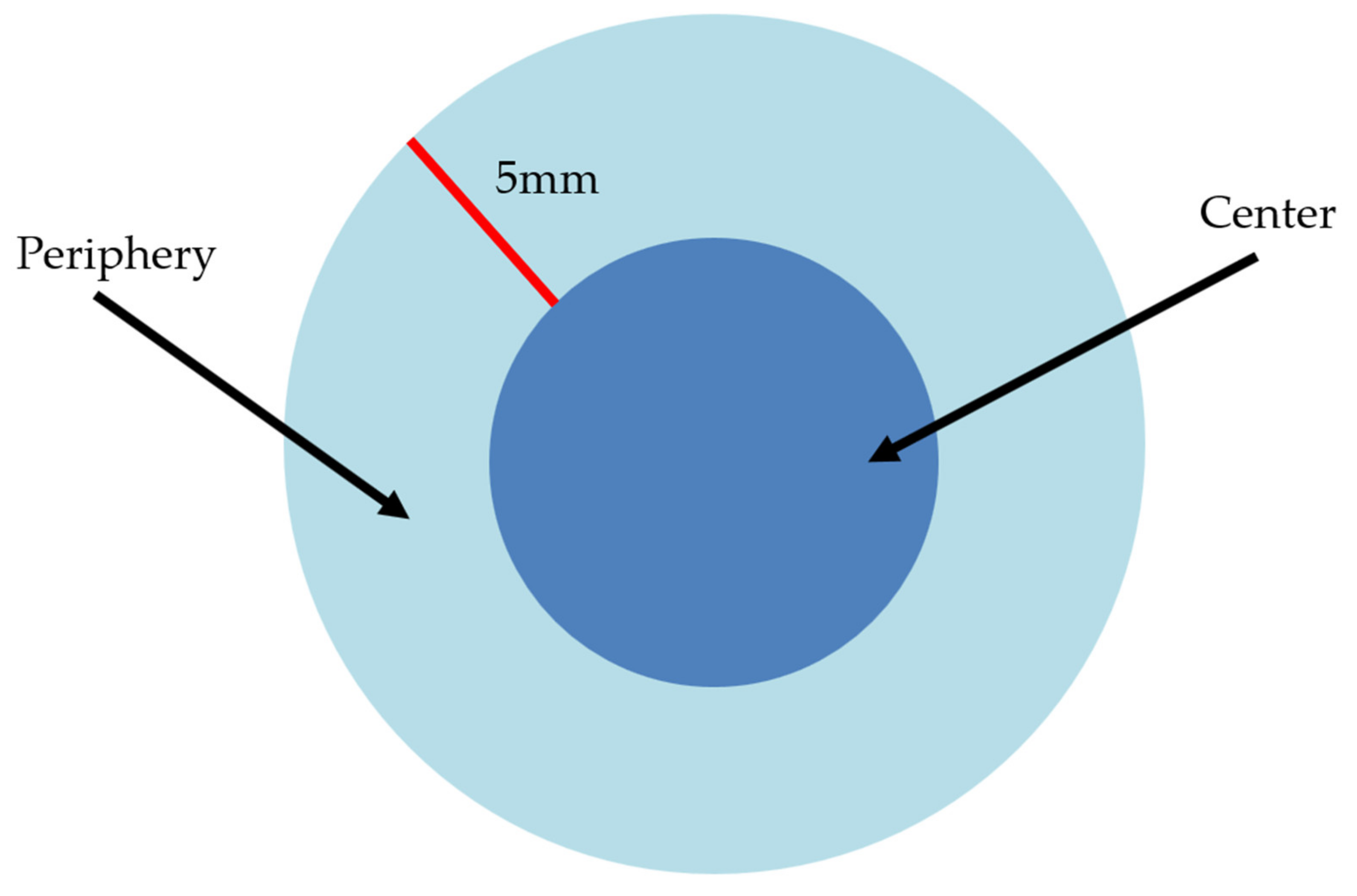
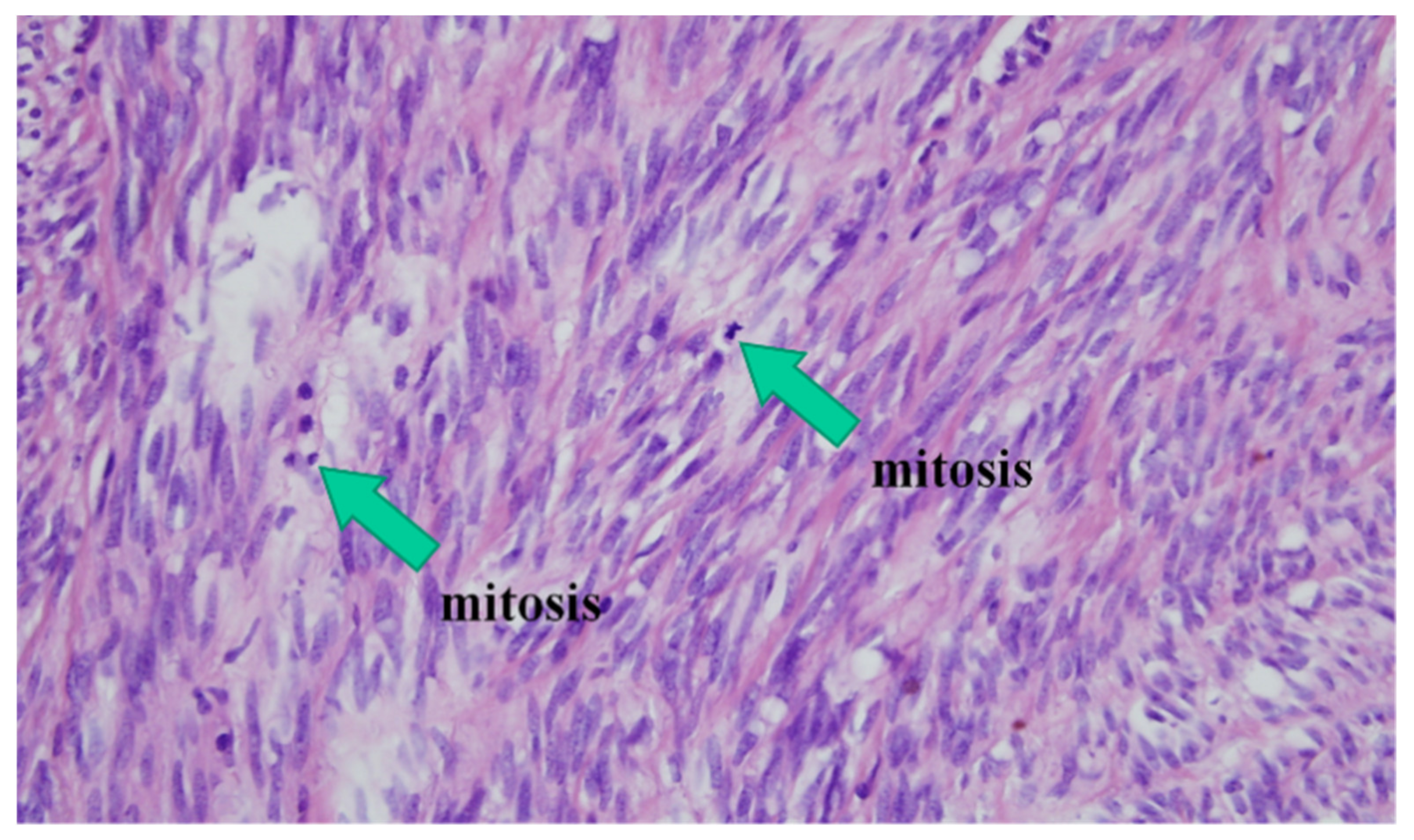
2.3. Pathological Diagnosis of Gastric GISTs
2.4. Risk Stratification
2.5. Statistical Analysis
3. Results
3.1. Clinical Features of Gastric GISTs
3.2. Primary Pathologic Reports
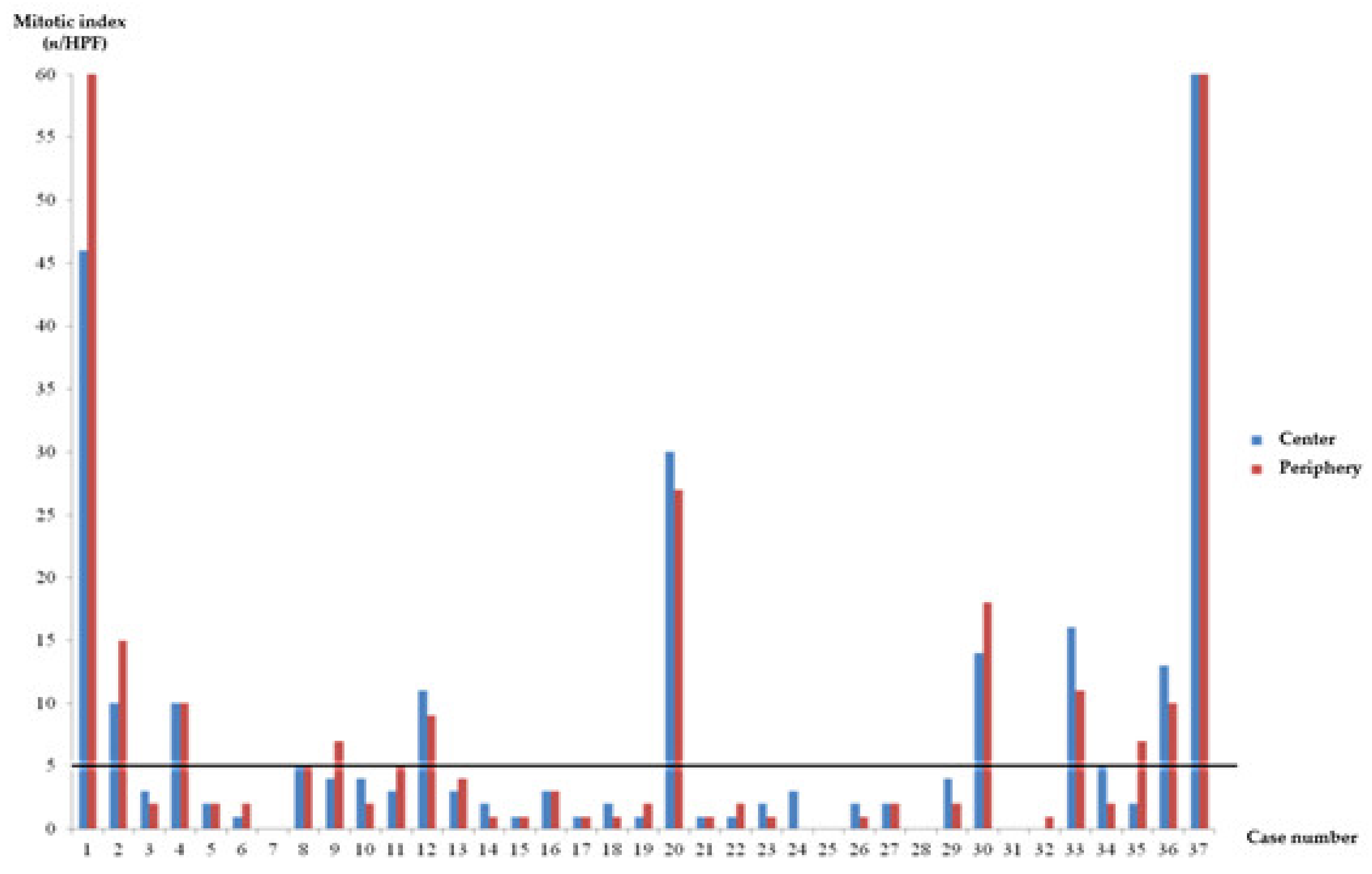
3.3. Comparison of Risk Stratification between the Periphery and Center of Gastric GISTs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El-Menyar, A.; Mekkodathil, A.; Al-Thani, H. Diagnosis and management of gastrointestinal stromal tumors: An up-to-date literature review. J. Cancer Res. Ther. 2017, 13, 889. [Google Scholar] [PubMed]
- Nomura, E.; Ioka, A.; Tsukuma, H. Incidence of soft tissue sarcoma focusing on gastrointestinal stromal sarcoma in Osaka, Japan, during 1978–2007. Jpn. J. Clin. Oncol. 2013, 43, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.A.; Livingstone, A.S.; Franceschi, D.; Rocha-Lima, C.; Lee, D.J.; Hodgson, N.; Jorda, M.; Koniaris, L.G. Current incidence and outcomes of gastrointestinal mesenchymal tumors including gastrointestinal stromal tumors. J. Am. Coll. Surg. 2006, 202, 623–629. [Google Scholar] [CrossRef]
- Chiang, N.-J.; Chen, L.-T.; Tsai, C.-R.; Chang, J.S. The epidemiology of gastrointestinal stromal tumors in Taiwan, 1998–2008: A nation-wide cancer registry-based study. BMC Cancer 2014, 14, 102. [Google Scholar] [CrossRef] [PubMed]
- Parab, T.M.; DeRogatis, M.J.; Boaz, A.M.; Grasso, S.A.; Issack, P.S.; Duarte, D.A.; Urayeneza, O.; Vahdat, S.; Qiao, J.-H.; Hinika, G.S. Gastrointestinal stromal tumors: A comprehensive review. J. Gastrointest. Oncol. 2019, 10, 144. [Google Scholar] [CrossRef] [PubMed]
- Khoo, C.Y.; Chai, X.; Richard, Q.; Teo, M.C.; Goh, B.K. Systematic review of current prognostication systems for primary gastrointestinal stromal tumors. Eur. J. Surg. Oncol. 2018, 44, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Joensuu, H. Risk stratification of patients diagnosed with gastrointestinal stromal tumor. Hum. Pathol. 2008, 39, 1411–1419. [Google Scholar] [CrossRef]
- Miettinen, M.; Sobin, L.H.; Lasota, J. Gastrointestinal stromal tumors of the stomach: A clinicopathologic, immunohistochemical, and molecular genetic study of 1765 cases with long-term follow-up. Am. J. Surg. Pathol. 2005, 29, 52–68. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.D.; Berman, J.J.; Corless, C.; Gorstein, F.; Lasota, J.; Longley, B.J.; Miettinen, M.; O’Leary, T.J.; Remotti, H.; Rubin, B.P. Diagnosis of gastrointestinal stromal tumors: A consensus approach. Int. J. Surg. Pathol. 2002, 10, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Miettinen, M.; Lasota, J. Gastrointestinal stromal tumors: Pathology and prognosis at different sites. Semin. Diagn. Pathol. 2006, 23, 70–83. [Google Scholar] [CrossRef] [PubMed]
- DeMatteo, R.P.; Gold, J.S.; Saran, L.; Gönen, M.; Liau, K.H.; Maki, R.G.; Singer, S.; Besmer, P.; Brennan, M.F.; Antonescu, C.R. Tumor mitotic rate, size, and location independently predict recurrence after resection of primary gastrointestinal stromal tumor (GIST). Cancer Interdiscip. Int. J. Am. Cancer Soc. 2008, 112, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Yasui, H.; Konishi, E.; Urasaki, K.; Yasukawa, S.; Yanagisawa, A. Intratumoral heterogeneity of MIB-1 labelling index in gastric gastrointestinal stromal tumor (GIST). Gastric Cancer 2006, 9, 223–228. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Søreide, K.; Sandvik, O.M.; Søreide, J.A.; Giljaca, V.; Jureckova, A.; Bulusu, V.R. Global epidemiology of gastrointestinal stromal tumours (GIST): A systematic review of population-based cohort studies. Cancer Epidemiol. 2016, 40, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Wardelmann, E.; Hohenberger, P.; Reichardt, P.; Merkelbach-Bruse, S.; Schildhaus, H.U.; Büttner, R. Gastrointestinale Stromatumoren des Magens. Der Pathol. 2010, 31, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.; Davila, J.A.; El-Serag, H.B. The epidemiology of malignant gastrointestinal stromal tumors: An analysis of 1458 cases from 1992 to 2000. Am. J. Gastroenterol. 2005, 100, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, B.; Bümming, P.; Meis-Kindblom, J.M.; Odén, A.; Dortok, A.; Gustavsson, B.; Sablinska, K.; Kindblom, L.G. Gastrointestinal stromal tumors: The incidence, prevalence, clinical course, and prognostication in the preimatinib mesylate era: A population-based study in western Sweden. Cancer 2005, 103, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Supsamutchai, C.; Wilasrusmee, C.; Hiranyatheb, P.; Jirasiritham, J.; Rakchob, T.; Choikrua, P. A cohort study of prognostic factors associated with recurrence or metastasis of gastrointestinal stromal tumor (GIST) of stomach. Ann. Med. Surg. 2018, 35, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Joensuu, H.; Vehtari, A.; Riihimäki, J.; Nishida, T.; Steigen, S.E.; Brabec, P.; Plank, L.; Nilsson, B.; Cirilli, C.; Braconi, C. Risk of recurrence of gastrointestinal stromal tumour after surgery: An analysis of pooled population-based cohorts. Lancet Oncol. 2012, 13, 265–274. [Google Scholar] [CrossRef]
- Ishikawa, T.; Kanda, T.; Kameyama, H.; Wakai, T. Neoadjuvant therapy for gastrointestinal stromal tumor. Transl. Gastroenterol. Hepatol. 2018, 3, 3. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Risk of Progression (%) | Mitotic Index (High-Power Field) | Tumor Size (cm) |
|---|---|---|
| None (0%) | ≤5/50 | ≤2 |
| None (0%, small cases) ** | >5/50 | ≤2 |
| Very low (1.9%) | ≤5/50 | >2, ≤5 |
| Low (3.6%) | ≤5/50 | >5, ≤10 |
| Moderate (12%) | ≤5/50 | >10 |
| (16%) | >5/50 | >2, ≤5 |
| High (55%) | >5/50 | >5, ≤10 |
| (86%) | >5/50 | >10 |
| Gastric GISTs (n = 37) | |
|---|---|
| Age, years | 58.65 ± 9.44 (40–76) |
| Sex (M/F) | 18(48.6%)/19 (51.4%) |
| Weight (kg) | 66.62 ± 10.08 (46–86) |
| Height (meters) | 1.62 ± 0.92 (1.44–1.88) |
| BMI (kg/m2) | 25.30 ± 2.92 (19.40–30.86) |
| Symptomatic GISTs, n (%) | 10 (27%) |
| Abdominal pain | 4 (10.8%) |
| Hematemesis | 1 (2.7%) |
| Nausea, anorexia | 5 (13.5%) |
| Incidental GISTs, n (%) | 27 (73%) |
| DM, n (%) | 10 (27%) |
| Hypertension, n (%) | 19 (51.4%) |
| Hepatitis, n (%) | 1 (2.7%) |
| Malignancy, n (%) | 2 (5.4%) |
| Size (cm) | 3.56 ± 2.10 (2.0–11.5) |
| Location, n (%) | |
| Antrum | 3 (8.1%) |
| Body | 14 (37.8%) |
| Fundus | 11 (29.7%) |
| Cardia | 9 (24.3%) |
| EUS findings | |
| Echogenicity, n (%) | |
| Hypoechoic/hyperechoic | 37 (100%)/0 (0%) |
| Homogeneity, n (%) | |
| Homogenous | 13 (35.1%) |
| Heterogenous | 24 (64.9%) |
| Cystic change | |
| Negative/positive | 20 (54.1%)/17 (45.9%) |
| Ulcer of gastric mucosa | 6 (16.2%) |
| Immunohistochemistry, n (%) | |
| c-Kit | 37 (100%) |
| CD34 | 35 (94.6%) |
| Desmin | 1 (2.7%) |
| SMA | 4 (10.8%) |
| S-100 | 2 (5.4%) |
| Primary risk stratification | |
| No risk | 3 (8.1%) |
| Very Low | 22 (59.65%) |
| Low | 1 (2.7%) |
| Moderate | 8 (21.6%) |
| High | 3 (8.1%) |
| Postoperative chemotherapy, n (%) | 4 (10.8%) |
| Recurrence, n (%) | 1 (2.7%) |
| EUS Findings | Pathologic Findings | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case | Gender | Age (range) | Location | Size (cm) | Layer | Echogenecity | Heterogeneity | Cystic change | Size (cm) | Original (n/HPF) | Center (n/HPF) | Periphery (n/HPF) | Original (risk) | Center (risk) | Periphery (risk) |
| 1 | 1 | 60–70 | Fundus | 4 | 4th | Hypo | Homo | Present | 3.5 | 104 | 46 | 120 | Moderate | Moderate | Moderate |
| 2 | 2 | 50–60 | Cardia | 3.6 | 4th | Hypo | Hetero | Present | 5.3 | 8 | 10 | 15 | High | High | High |
| 3 | 1 | 50–60 | Antrum | 2.6 | 4th | Hypo | Hetero | Present | 2.7 | 3 | 3 | 2 | Very low | Very low | Very low |
| 4 | 2 | 50–60 | Fundus | 3.1 | 4th | Hypo | Hetero | Present | 3.1 | 8 | 10 | 10 | Moderate | Moderate | Moderate |
| 5 | 2 | 60–708 | Fundus | 4.2 | 4th | Hypo | Hetero | Absent | 5.5 | 1 | 2 | 2 | Low | Low | Low |
| 6 | 1 | 50–60 | Body | 3.4 | 4th | Hypo | Hetero | Absent | 2.7 | 1 | 1 | 2 | Very low | Very low | Very low |
| 7 | 1 | 60–70 | Antrum | 2.4 | 4th | Hypo | Homo | Absent | 2.2 | 2 | 0 | 0 | Very low | Very low | Very low |
| 8 | 2 | 60–70 | Body | 2.2 | 4th | Hypo | Homo | Absent | 3 | 2 | 5 | 5 | Very low | Very low | Very low |
| 9 | 1 | 50–60 | Body | 3.2 | 4th | Hypo | Hetero | Absent | 3 | 7 | 4 | 7 | Moderate | Very low | Moderate |
| 10 | 1 | 70–80 | Fundus | 4.5 | 4th | Hypo | Homo | Present | 4.5 | 2 | 4 | 2 | Very low | Very low | Very low |
| 11 | 1 | 70–80 | Body | 2.3 | 4th | Hypo | Homo | Absent | 3 | 1 | 3 | 5 | Very low | Very low | Very low |
| 12 | 2 | 60–70 | Cardia | 2.4 | 4th | Hypo | Homo | Present | 2.5 | 7 | 11 | 9 | Moderate | Moderate | Moderate |
| 13 | 1 | 60–70 | Antrum | 2.1 | 4th | Hypo | Hetero | Present | 2 | 3 | 3 | 4 | No risk | No risk | No risk |
| 14 | 2 | 60–70 | Fundus | 2.5 | 3rd | Hypo | Hetero | Absent | 2 | 0 | 2 | 1 | No risk | No risk | No risk |
| 15 | 1 | 40–50 | Cardia | 2.5 | 4th | Hypo | Homo | Absent | 3 | 0 | 1 | 1 | Very low | Very low | Very low |
| 16 | 2 | 60–70 | Body | 2.7 | 4th | Hypo | Hetero | Absent | 3 | 5 | 3 | 3 | Very low | Very low | Very low |
| 17 | 2 | 50–60 | Body | 3.1 | 4th | Hypo | Homo | Absent | 2.5 | 1 | 1 | 1 | Very low | Very low | Very low |
| 18 | 2 | 40–50 | Body | 2.8 | 4th | Hypo | Hetero | Absent | 3 | 3 | 2 | 1 | Very low | Very low | Very low |
| 19 | 1 | 40–50 | Body | 4.2 | 4th | Hypo | Hetero | Absent | 4 | 2 | 1 | 2 | Very low | Very low | Very low |
| 20 | 1 | 60–70 | Fundus | 4.1 | 4th | Hypo | Hetero | Absent | 5 | 50 | 30 | 27 | Moderate | Moderate | Moderate |
| 21 | 1 | 50–60 | Cardia | 4 | 4th | Hypo | Homo | Absent | 4 | 3 | 1 | 1 | Very low | Very low | Very low |
| 22 | 2 | 60–70 | Cardia | 3 | 4th | Hypo | Hetero | Present | 3.3 | 2 | 1 | 2 | Very low | Very low | Very low |
| 23 | 2 | 50–60 | Fundus | 2.5 | 3rd | Hypo | Hetero | Absent | 2.7 | 3 | 2 | 1 | Very low | Very low | Very low |
| 24 | 1 | 50–60 | Body | 4 | 4th | Hypo | Homo | Absent | 3.5 | 1 | 3 | 0 | Very low | Very low | Very low |
| 25 | 1 | 40–50 | Cardia | 2.3 | 4th | Hypo | Hetero | Present | 2.2 | 2 | 0 | 0 | Very low | Very low | Very low |
| 26 | 2 | 40–50 | Cardia | 4.7 | 4th | Hypo | Hetero | Present | 4.5 | 4 | 2 | 1 | Very low | Very low | Very low |
| 27 | 2 | 70–80 | Body | 2.2 | 4th | Hypo | Homo | Absent | 2 | 1 | 2 | 2 | No risk | No risk | No risk |
| 28 | 2 | 60–70 | Body | 11 | 4th | Hypo | Hetero | Present | 10.5 | 1 | 0 | 0 | Moderate | Moderate | Moderate |
| 29 | 2 | 40–50 | Cardia | 4.5 | 4th | Hypo | Hetero | Present | 3.8 | 2 | 4 | 2 | Very low | Very low | Very low |
| 30 | 2 | 50–60 | Fundus | 11 | 4th | Hypo | Hetero | Present | 11.5 | 16 | 14 | 18 | High | High | High |
| 31 | 2 | 50–60 | Fundus | 3.5 | 4th | Hypo | Hetero | Absent | 2.3 | 0 | 0 | 0 | Very low | Very low | Very low |
| 32 | 1 | 60–70 | Fundus | 3 | 4th | Hypo | Hetero | Absent | 2.2 | 0 | 0 | 1 | Very low | Very low | Very low |
| 33 | 1 | 70–80 | Cardia | 2 | 4th | Hypo | Hetero | Present | 2.1 | 7 | 16 | 11 | Moderate | Moderate | Moderate |
| 34 | 2 | 60–70 | Body | 2 | 4th | Hypo | Hetero | Present | 2.2 | 3 | 5 | 2 | Very low | Very low | Very low |
| 35 | 2 | 60–70 | Body | 4.2 | 4th | Hypo | Hetero | Present | 3.7 | 7 | 2 | 7 | Moderate | Very low | Moderate |
| 36 | 1 | 50–60 | Body | 2.2 | 4th | Hypo | Homo | Present | 2.3 | 11 | 13 | 10 | Moderate | Moderate | Moderate |
| 37 | 1 | 40–50 | Fundus | 4.5 | 4th | Hypo | Hetero | Absent | 5.3 | 118 | 160 | 125 | High | High | High |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.J.; Lee, K.H.; Yoo, C.K.; Yoon, J.H.; Jang, K.S.; Kim, Y.J.; Lee, H.L. Is There Pathological Uniformity between the Periphery and Center of a Gastrointestinal Stromal Tumor? J. Clin. Med. 2021, 10, 687. https://doi.org/10.3390/jcm10040687
Choi SJ, Lee KH, Yoo CK, Yoon JH, Jang KS, Kim YJ, Lee HL. Is There Pathological Uniformity between the Periphery and Center of a Gastrointestinal Stromal Tumor? Journal of Clinical Medicine. 2021; 10(4):687. https://doi.org/10.3390/jcm10040687
Chicago/Turabian StyleChoi, Seong Ji, Kwan Hong Lee, Chan Kyoo Yoo, Jai Hoon Yoon, Ki Seok Jang, Youn Jeong Kim, and Hang Lak Lee. 2021. "Is There Pathological Uniformity between the Periphery and Center of a Gastrointestinal Stromal Tumor?" Journal of Clinical Medicine 10, no. 4: 687. https://doi.org/10.3390/jcm10040687
APA StyleChoi, S. J., Lee, K. H., Yoo, C. K., Yoon, J. H., Jang, K. S., Kim, Y. J., & Lee, H. L. (2021). Is There Pathological Uniformity between the Periphery and Center of a Gastrointestinal Stromal Tumor? Journal of Clinical Medicine, 10(4), 687. https://doi.org/10.3390/jcm10040687