
Effects of Percutaneous Electrical Nerve Stimulation on Countermovement Jump and Squat Performance Speed in Male Soccer Players: A Pilot Randomized Clinical Trial

 , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Material and Methods
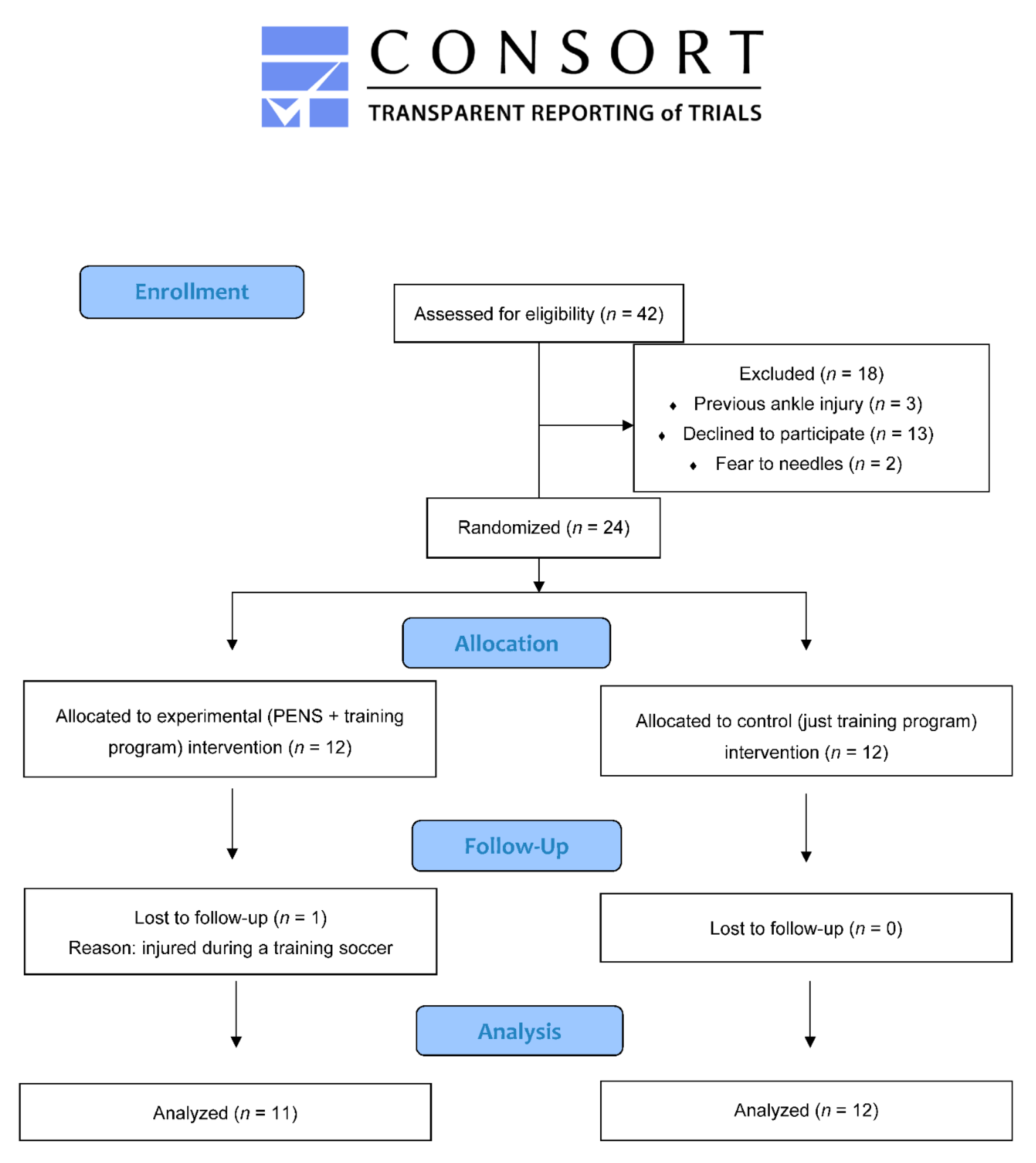
2.1. Study Design
2.2. Participants
2.3. Randomization and Masking
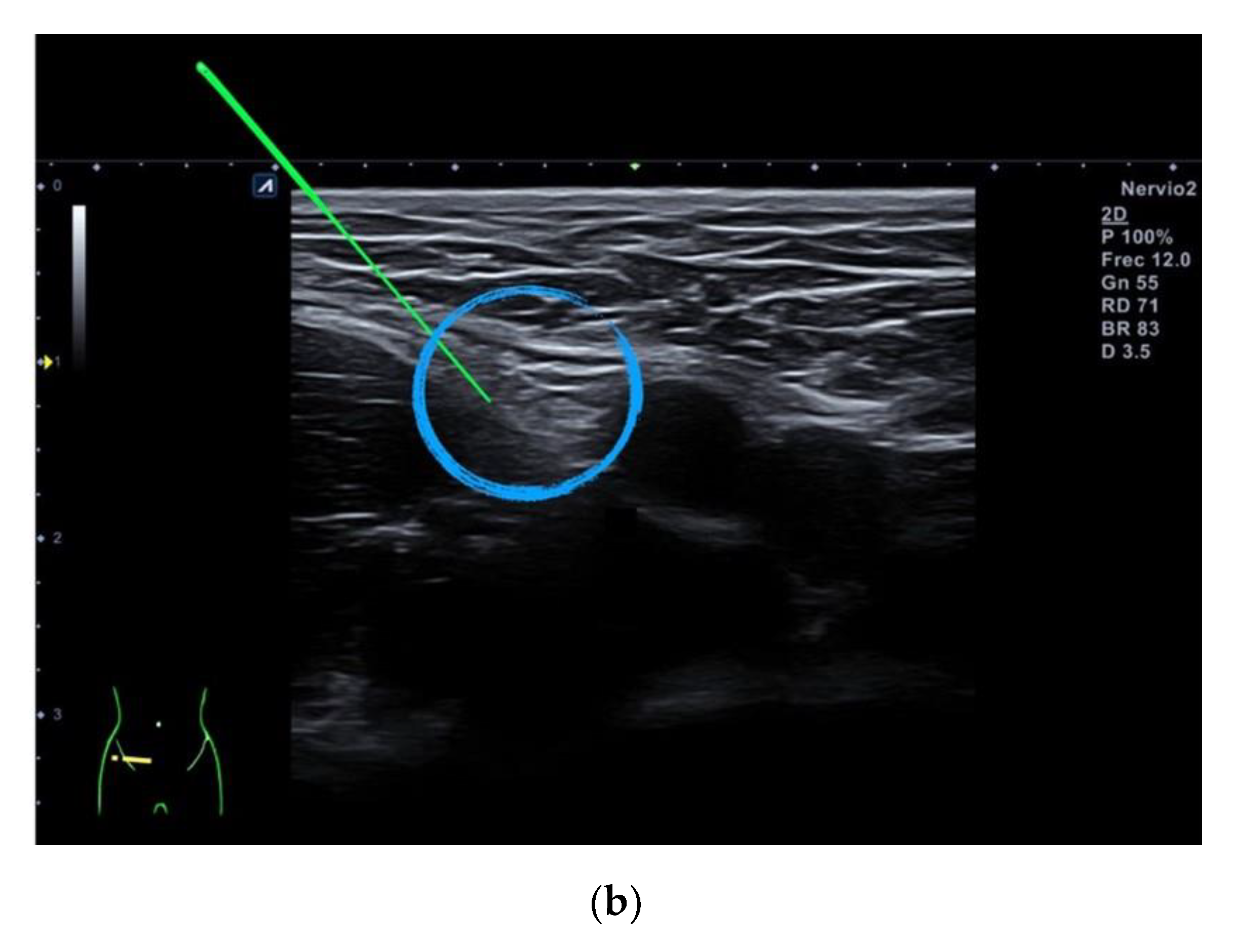
2.4. Percutaneous Electrical Nerve Stimulation
2.5. Training Program
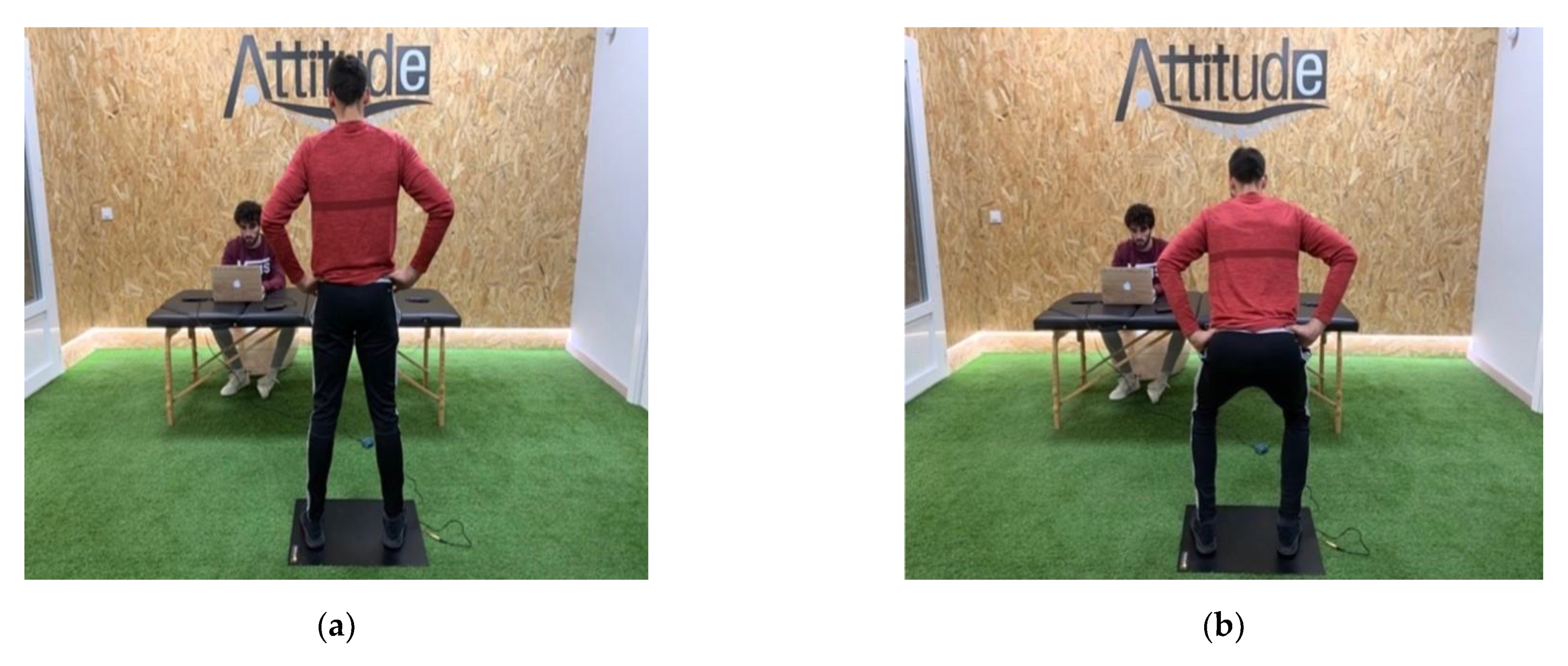
2.6. Outcomes
2.7. Treatment Side Effects
2.8. Sample Size Determination
2.9. Statistical Analysis
3. Results
4. Discussion
4.1. Findings
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Leontijevic, B.; Janković, A.; Tomić, L. Attacking performance profile of football teams in different national leagues according to UEFA rankings for club competitions. Facta Univ. Ser. Phys. Educ. Sport 2019, 697–708. [Google Scholar] [CrossRef]
- Kubayi, A.; Toriola, A. Physical demands analysis of soccer players during the extra-time periods of the UEFA Euro 2016. S. Afr. J. Sports Med. 2018, 30, 1–3. [Google Scholar] [CrossRef]
- Morgans, R.; Orme, P.; Anderson, L.; Drust, B. Principles and practices of training for soccer. J. Sport Health Sci. 2014, 3, 251–257. [Google Scholar] [CrossRef]
- Reilly, T.; Gilbourne, D. Science and football: A review of applied re- search in the football codes. J. Sports Sci. 2003, 21, 693–705. [Google Scholar] [CrossRef] [PubMed]
- Rowat, O.; Fenner, J.; Unnithan, V. Technical and physical determinants of soccer match-play performance in elite youth soccer players. J. Sports Med. Phys. Fit. 2017, 57, 369–379. [Google Scholar]
- Vaeyens, R.; Lenoir, M.; Williams, A.M.; Mazyn, L.; Philippaerts, R. The effects of task constraints on visual search behaviour and decision-making skill in youth soccer players. J. Sport Exerc. Psychol. 2007, 29, 147–169. [Google Scholar] [CrossRef] [PubMed]
- Ryman Augustsson, S.; Arvidsson, J.; Haglund, E. Jump height as performance indicator for the selection of youth football players to national teams. J. Sports Med. Phys. Fit. 2019, 59, 1669–1675. [Google Scholar] [CrossRef]
- Helgerud, J.; Rodas, G.; Kemi, O.J.; Hoff, J. Strength and endurance in elite football players. Int. J. Sports Med. 2011, 32, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Bogdanis, G.; Papaspyrou, A.; Souglis, A.; Theos, A.; Sotiropoulos, A.; Maridaki, M. Effects of a hypertrophy and a maximal strength training programme on speed, force and power of soccer players. In The Sixth World Congress on Science and Football; Routledge: Antalya, Turkey, 2007; pp. 290–295. [Google Scholar]
- Wisløff, U.; Castagna, C.; Helgerud, J.; Jones, R.; Hoff, J. Strong correlation of maximal squat strength with sprint performance and vertical jump height in elite soccer players. Br. J. Sports Med. 2004, 38, 285–288. [Google Scholar]
- Li, H.; Xu, Q.R. Effect of percutaneous electrical nerve stimulation for the treatment of migraine. Medicine 2017, 96, e8108. [Google Scholar] [CrossRef] [PubMed]
- Ilfeld, B.M.; Finneran, J.J., 4th; Gabriel, R.A.; Said, E.T.; Nguyen, P.L.; Abramson, W.B.; Khatibi, B.; Sztain, J.F.; Swisher, M.W.; Jaeger, P.; et al. Ultrasound-guided percutaneous peripheral nerve stimulation: Neuromodulation of the suprascapular nerve and brachial plexus for postoperative analgesia following ambulatory rotator cuff repair. A proof-of-concept study. Reg. Anesth. Pain Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Arias-Buría, J.L.; Cleland, J.A.; El Bachiri, Y.R.; Plaza-Manzano, G.; Fernández-de-Las-Peñas, C. Ultrasound-Guided percutaneous electrical nerve stimulation of the radial nerve for a patient with lateral elbow pain: A case report with a 2-year follow-up. J. Orthop. Sports Phys. Ther. 2019, 49, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Ilfeld, B.M.; Gabriel, R.A.; Said, E.T.; Monahan, A.M.; Sztain, J.F.; Abramson, W.B.; Khatibi, B.; Finneran, J.J., 4th; Jaeger, P.T.; Schwartz, A.K.; et al. Ultrasound-Guided percutaneous peripheral nerve stimulation: Neuromodulation of the sciatic nerve for postoperative analgesia following ambulatory foot surgery, a proof-of-concept study. Reg. Anesth. Pain Med. 2018, 43, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Verrills, P.; Russo, M. Peripheral nerve stimulation for back pain. Prog. Neurol. Surg. 2015, 29, 127–138. [Google Scholar]
- Álvarez-Prats, D.; Carvajal-Fernández, O.; Pérez-Mallada, N.; Minaya-Muñoz, F. Changes in maximal isometric quadriceps strength after the application of ultrasound-guided percutaneous neuromodulation of the femoral nerve: A case series. J. Invasive Tech. Phys. Ther. 2019, 2, 39–45. [Google Scholar] [CrossRef]
- De-la-Cruz-Torres, B.; Carrasco-Iglesias, C.; Minaya-Muñoz, F.; Romero-Morales, C. Crossover effects of ultrasound-guided percutaneous neuromodulation on contralateral hamstring flexibility. Acupunct. Med. 2020, 13. [Google Scholar] [CrossRef] [PubMed]
- Zwarenstein, M.; Treweek, S.; Gagnier, J.J.; Altman, D.G.; Tunis, S.; Haynes, B.; Oxman, A.D.; Moher, D.; CONSORT group; Pragmatic Trials in Healthcare group. Improving the reporting of pragmatic trials: An extension of the CONSORT statement. BMJ 2008, 337, 2390. [Google Scholar] [CrossRef]
- Gustafson, K.J.; Pinault, G.C.J.; Neville, J.J.; Syed, I.; Davis, J.A., Jr.; Jean-Claude, J.; Triolo, R.J. Fascicular anatomy of human femoral nerve: Implications for neural prostheses using nerve cuff electrodes. J. Rehabil. Res. 2009, 46, 973–984. [Google Scholar] [CrossRef] [PubMed]
- Makhlouf, I.; Castagna, C.; Manzi, V.; Laurencelle, L.; Behm, D.G.; Chaouachi, A. Effect of Sequencing Strength and Endurance Training in Young Male Soccer Players. J. Strength Cond. Res. 2016, 30, 841–850. [Google Scholar] [CrossRef]
- Hoff, J. Training and testing physical capacities for elite soccer players. J. Sports Sci. 2005, 23, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Pueo, B.; Jimenez-Olmedo, J.M.; Lipińska, P.; Buśko, K.; Penichet-Tomas, A. Concurrent validity and reliability of proprietary and open-source jump mat systems for the assessment of vertical jumps in sport sciences. Acta Bioeng. Biomech. 2018, 20, 51–57. [Google Scholar] [PubMed]
- Rago, V.; Brito, J.; Figueiredo, P.; Carvalho, T.; Fernandes, T.; Fonseca, P.; Rebelo, A. Countermovement Jump Analysis Using Different Portable Devices: Implications for Field Testing. Sports 2018, 6, 91. [Google Scholar] [CrossRef]
- Jakobsen, M.D.; Sundstrup, E.; Randers, M.B.; Kjær, M.; Andersen, L.L.; Krustrup, P.; Aagaard, P. The effect of strength training, recreational soccer and running exercise on stretch-shortening cycle muscle performance during countermovement jumping. Hum. Mov. Sci. 2012, 31, 970–986. [Google Scholar] [CrossRef]
- Pérez-Castilla, A.; Piepoli, A.; Delgado-García, G.; Garrido-Blanca, G.; García-Ramos, A. Reliability and concurrent validity of seven commercially available devices for the assessment of movement velocity at different intensities during the bench press. J. Strength Cond. Res. 2019, 33, 1258–1265. [Google Scholar] [CrossRef] [PubMed]
- Capili, B.; Anastasi, J.K.; Geiger, J.N. Adverse event reporting in acupuncture clinical trials focusing on pain. Clin. J. Pain 2010, 26, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Van Breukelen, G.J.P. ANCOVA versus change from baseline had more power in randomized studies and more bias in nonrandomized studies. J. Clin. Epidemiol. 2006, 59, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Gray, C.D.; Kinnear, P.R. IBM SPSS Statistics 19; Psychology Press: East Sussex, UK, 2012. [Google Scholar]
- Molsberger, A.; McCaig, C.D. Percutaneous direct current stimulation-a new electroceutical solution for severe neurological pain and soft tissue injuries. Med. Devices 2018, 11, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Miao, Q.; Qiang, J.H.; Jin, Y.L. Effectiveness of percutaneous neuromuscular electrical stimulation for neck pain relief in patients with cervical spondylosis. Medicine 2018, 97, e11080. [Google Scholar] [CrossRef]
- Requena-Sánchez, B.; Padial-Puche, P.; González-Badillo, J.J. Percutaneous electrical stimulation in strength training: An update. J. Strength Cond. Res. 2005, 19, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Pietrosimone, B.G.; Saliba, S.A. Changes in voluntary quadriceps activation predict changes in quadriceps strength after therapeutic exercise in patients with knee osteoarthritis. Knee 2012, 19, 939–943. [Google Scholar] [CrossRef]
- Herrero, A.J.; Martín, J.; Martín, T.; Abadía, O.; Fernández, B.; García-López, D. Short-term effect of strength training with and without superimposed electrical stimulation on muscle strength and anaerobic performance. A randomized controlled trial. Part I. J. Strength Cond. Res. 2010, 24, 1609–1615. [Google Scholar] [CrossRef] [PubMed]
- Krommes, K.; Petersen, J.; Nielsen, M.B.; Aagaard, P.; Hölmich, P.; Thorborg, K. Sprint and jump performance in elite male soccer players following a 10-week Nordic Hamstring exercise Protocol: A randomised pilot study. BMC Res. Notes 2017, 10, 669. [Google Scholar] [CrossRef] [PubMed]
- Serpell, B.G.; Scarvell, J.M.; Ball, N.B.; Smith, P.N. Mechanisms and risk factors for noncontact ACL injury in age mature athletes who engage in field or court sports: A summary of the literature since 1980. J. Strength Cond. Res. 2012, 26, 3160–3176. [Google Scholar] [CrossRef] [PubMed]
- Acevedo, R.J.; Rivera-Vega, A.; Miranda, G.; Micheo, W. Anterior cruciate ligament injury: Identification of risk factors and prevention strategies. Curr. Sports Med. Rep. 2014, 13, 186–191. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcomes | PENS + Training Group | Training Group |
|---|---|---|
| Age (years) | 26 ± 4.5 | 25 ± 4.0 |
| Weight (kg) | 73.5 ± 5.5 | 74.5 ± 9.5 |
| Height (m) | 1.8 ± 0.05 | 1.8 ± 0.1 |
| BMI (kg/cm2) | 23.5 ± 1.95 | 23.5 ± 2.9 |
| Countermovement Jump Height (cm) | 31.5 ± 3.5 | 32.0 ± 5.0 |
| Countermovement Jump Flight Time (s) | 0.507 ± 0.029 | 0.509 ± 5.0 |
| Squat Performance Speed (m/s) | 0.55 ± 0.3 | 0.6 ± 0.3 |
| PENS + Training Group (n = 11) | Training Group (n = 12) | Within-Group Differences | Between-Groups Differences | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PENS + Training | Training Group | ||||||||||
| CMJ Flight Time (s) | Immediate Differences | Baseline/Session 2 | Baseline/Follow-Up | Immediate Differences | Baseline/Session 2 | Baseline/Follow-Up | Immediate Differences | Baseline/Session 2 | Baseline/Follow-Up | ||
| Before Session 1 (Day 1) | 0.507 ± 0.029 (0.487, 0.526) | 0.509 ± 0.041 (0.482, 0.534) | 0.016 ± 0.012 (0.008, 0.024) 0.001 | 0.017 ± 0.006 (0.012, 0.021) <0.001 | 0.010 ± 0.008 (0.004, 0.015) 0.003 | −0.001 ± 0.008 (−0.006, 0.004) 0.620 | 0.005 ± 0.016 (−0.005, 0.015) 0.299 | 0.008 ± 0.020 (−0.004, 0.020) 0.184 | 0.017 ± 0.004 (0.008, 0.026) <0.001 | 0.011 ± 0.005 (0.001, 0.022) 0.032 | 0.001 ± 0.006 (−0.011, 0.015) 0.792 |
| After Session 1 (Day 1) | 0.523 ± 0.031 (0.502, 0.544) | 0.507 ± 0.041 (0.480, 0.533) | |||||||||
| Before Session 2 (Day 7) | 0.510 ± 0.029 (0.490, 0.528) | 0.522 ± 0.046 (0.492, 0.551) | 0.014 ± 0.009 (0.008, 0.020) <0.001 | −0.008 ± 0.010 (−0.014, −0.001) 0.017 | 0.022 ± 0.003 (0.014, 0.030) <0.001 | ||||||
| After Session 2 (Day 7) | 0.524 ± 0.030 (0.503, 0.544) | 0.514 ± 0.048 (0.482; 0.544) | |||||||||
| Follow-up (after 30 days) | 0.517 ± 0.030 (0.496, 0.545) | 0.517 ± 0.045 (0.487, 0.545) | |||||||||
| PENS + Training Group (n = 11) | Training Group (n = 12) | Within-Group Differences | Between-Groups Differences | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PENS + Training | Training Group | ||||||||||
| CMJ (cm) | Immediate Differences | Baseline/Session 2 | Baseline/Follow-Up | Immediate Differences | Baseline/Session 2 | Baseline/Follow-Up | Immediate Differences | Baseline/Session 2 | Baseline/Follow-Up | ||
| Before Session 1 (Day 1) | 31.5 ± 3.5 (29.0, 34.0) | 32.0 ± 5.0 (29.0, 35.0) | 2.0 ± 1.5 (1.0, 3.0) <0.001 | 2.5 ± 1.04 (1.5, 3.5) <0.001 | 1.5 ± 1.0 (0.5, 2.5) 0.002 | −0.5 ± 1.0 (−1.6, 0.6) 0.645 | 0.5 ± 2.5 (−0.5, 1.5) 0.257 | 0.7 ± 2.0 (−0.6, 2.0) 0.174 | 2.5 ± 0.5 (1.0, 4.0) 0.001 | 2.0 ± 1.0 (0.5, 3.5) 0.043 | 0.8 ± 0.8 (−1.0, 2.6) 0.828 |
| After Session 1 (Day 1) | 33.5 ± 4.0 (31.0, 36.0) | 31.5 ± 5.0 (28.5, 34.5) | |||||||||
| Before Session 2 (Day 7) | 32.0 ± 3.5 (29.5, 34.50) | 33.5 ± 6.0 (30.0, 37.0) | 2.0 ± 1.0 (1.0, 3.0) <0.001 | −1.00 ± 1.5 (−2.5, 0.5) 0.615 | 3.0 ± 0.5 (1.8, 4.2) <0.001 | ||||||
| After Session 2 (Day 7) | 34.0 ± 4.0 (31.0, 37.0) | 32.5 ± 6.0 (28.5, 36.5) | |||||||||
| Follow-up (after 30 days) | 33.0 ± 3.5 (30.5, 35.5) | 33.0 ± 5.5 (29.5, 36.5) | |||||||||
| PENS + Training Group (n = 11) | Training Group (n = 12) | Within-Group Differences | Between Groups Differences | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PENS + Training | Training Group | ||||||||||
| SPS (m/s) | Immediate Differences | Baseline/Session 2 | Baseline/Follow-Up | Immediate Differences | Baseline/Session 2 | Baseline/Follow-Up | Immediate Differences | Baseline/Session 2 | Baseline/Follow-Up | ||
| Before Session 1 (Day 1) | 0.55 ± 0.3 (0.35, 0.75) | 0.6 ± 0.3 (0.4, 0.8) | 0.35 ± 0.3 (0.15, 0.55) 0.004 | 0.35 ± 0.3 (0.2, 0.6) 0.001 | 0.35 ± 0.3 (0.15, 0.55) 0.003 | 0.1 ± 0.3 (−0.1, 0.3) 0.279 | 0.15 ± 0.35 (−0.05, 0.35) 0.151 | 0.25 ± 0.25 (0.1, 0.4) 0.008 | 0.2 ± 0.15 (−0.05, 0.45) 0.98 | 0.2 ± 0.15 (0.0, 0.4) 0.07 | 0.1 ± 0.1 (−0.15, 0.4) 0.483 |
| After Session 1 (Day 1) | 0.9 ± 0.2 (0.7, 1.1) | 0.7 ± 0.3 (0.5, 0.9) | |||||||||
| Before Session 2 (Day 7) | 0.7 ± 0.1 (0.6, 0.8) | 0.9 ± 0.25 (0.7, 1.1) | 0.25 ± 0.15 (0.15, 0.35) <0.001 | −0.15 ± 0.15 (−0.3, 0.0) 0.07 | 0.4 ± 0.05 (0.2, 0.6) <0.001 | ||||||
| After Session 2 (Day 7) | 1.0 ± 0.1 (0.9, 1.1) | 0.75 ± 0.25 (0.6, 0.9) | |||||||||
| Follow-up (after 30 days) | 0.9 ± 0.1 (0.8, 1.0) | 0.85 ± 0.15 (0.75, 0.95) | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallego-Sendarrubias, G.M.; Arias-Buría, J.L.; Úbeda-D’Ocasar, E.; Hervás-Pérez, J.P.; Rubio-Palomino, M.A.; Fernández-de-las-Peñas, C.; Valera-Calero, J.A. Effects of Percutaneous Electrical Nerve Stimulation on Countermovement Jump and Squat Performance Speed in Male Soccer Players: A Pilot Randomized Clinical Trial. J. Clin. Med. 2021, 10, 690. https://doi.org/10.3390/jcm10040690
Gallego-Sendarrubias GM, Arias-Buría JL, Úbeda-D’Ocasar E, Hervás-Pérez JP, Rubio-Palomino MA, Fernández-de-las-Peñas C, Valera-Calero JA. Effects of Percutaneous Electrical Nerve Stimulation on Countermovement Jump and Squat Performance Speed in Male Soccer Players: A Pilot Randomized Clinical Trial. Journal of Clinical Medicine. 2021; 10(4):690. https://doi.org/10.3390/jcm10040690
Chicago/Turabian StyleGallego-Sendarrubias, Gracia María, José Luis Arias-Buría, Edurne Úbeda-D’Ocasar, Juan Pablo Hervás-Pérez, Manuel Antonio Rubio-Palomino, César Fernández-de-las-Peñas, and Juan Antonio Valera-Calero. 2021. "Effects of Percutaneous Electrical Nerve Stimulation on Countermovement Jump and Squat Performance Speed in Male Soccer Players: A Pilot Randomized Clinical Trial" Journal of Clinical Medicine 10, no. 4: 690. https://doi.org/10.3390/jcm10040690
APA StyleGallego-Sendarrubias, G. M., Arias-Buría, J. L., Úbeda-D’Ocasar, E., Hervás-Pérez, J. P., Rubio-Palomino, M. A., Fernández-de-las-Peñas, C., & Valera-Calero, J. A. (2021). Effects of Percutaneous Electrical Nerve Stimulation on Countermovement Jump and Squat Performance Speed in Male Soccer Players: A Pilot Randomized Clinical Trial. Journal of Clinical Medicine, 10(4), 690. https://doi.org/10.3390/jcm10040690