Recurrence and Prognostic Value of Asymptomatic Spinal Cord Lesions in Multiple Sclerosis

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
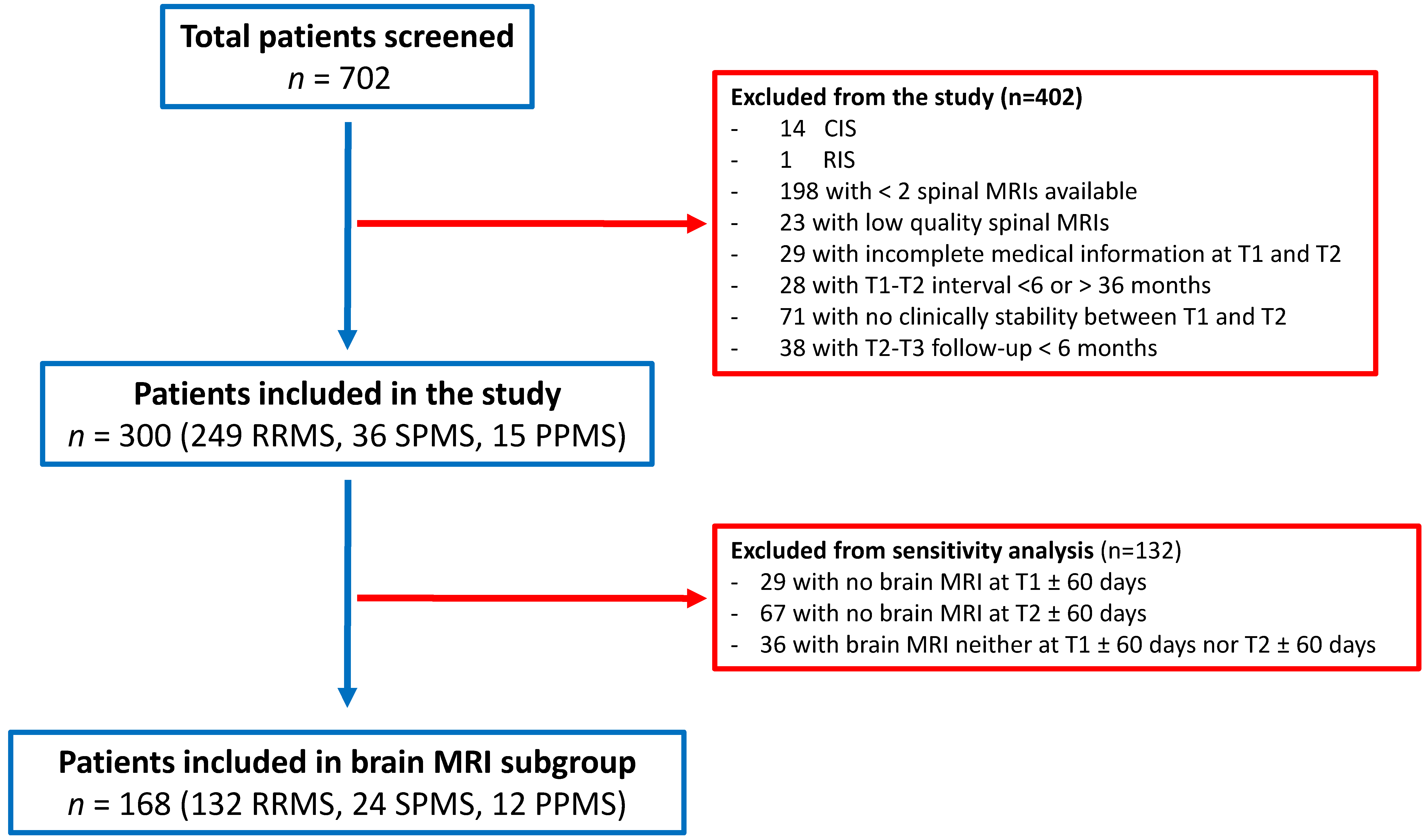
2.1. Study Population
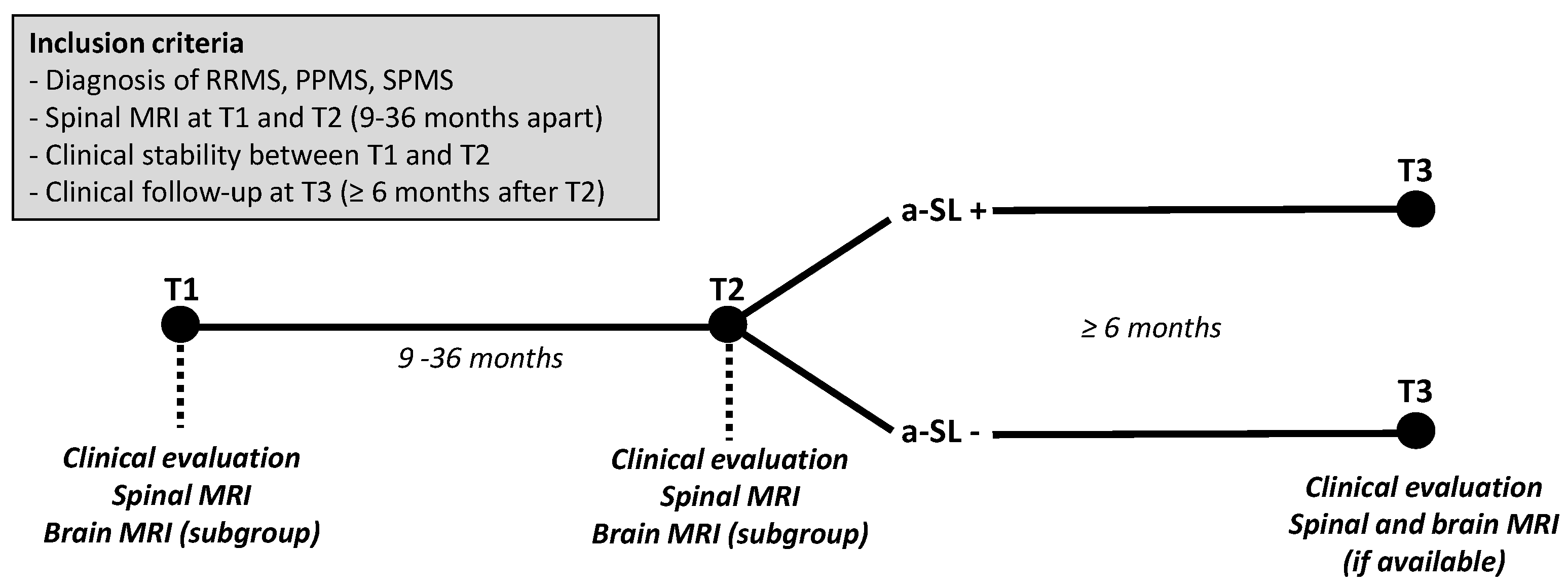
2.2. Inclusion Criteria and Study Design
2.3. Clinical Assessment
2.4. Neuroimaging Assessment
2.5. Study Objectives
2.6. Statistical Analysis
3. Results
3.1. Disability Progression
3.2. Relapses
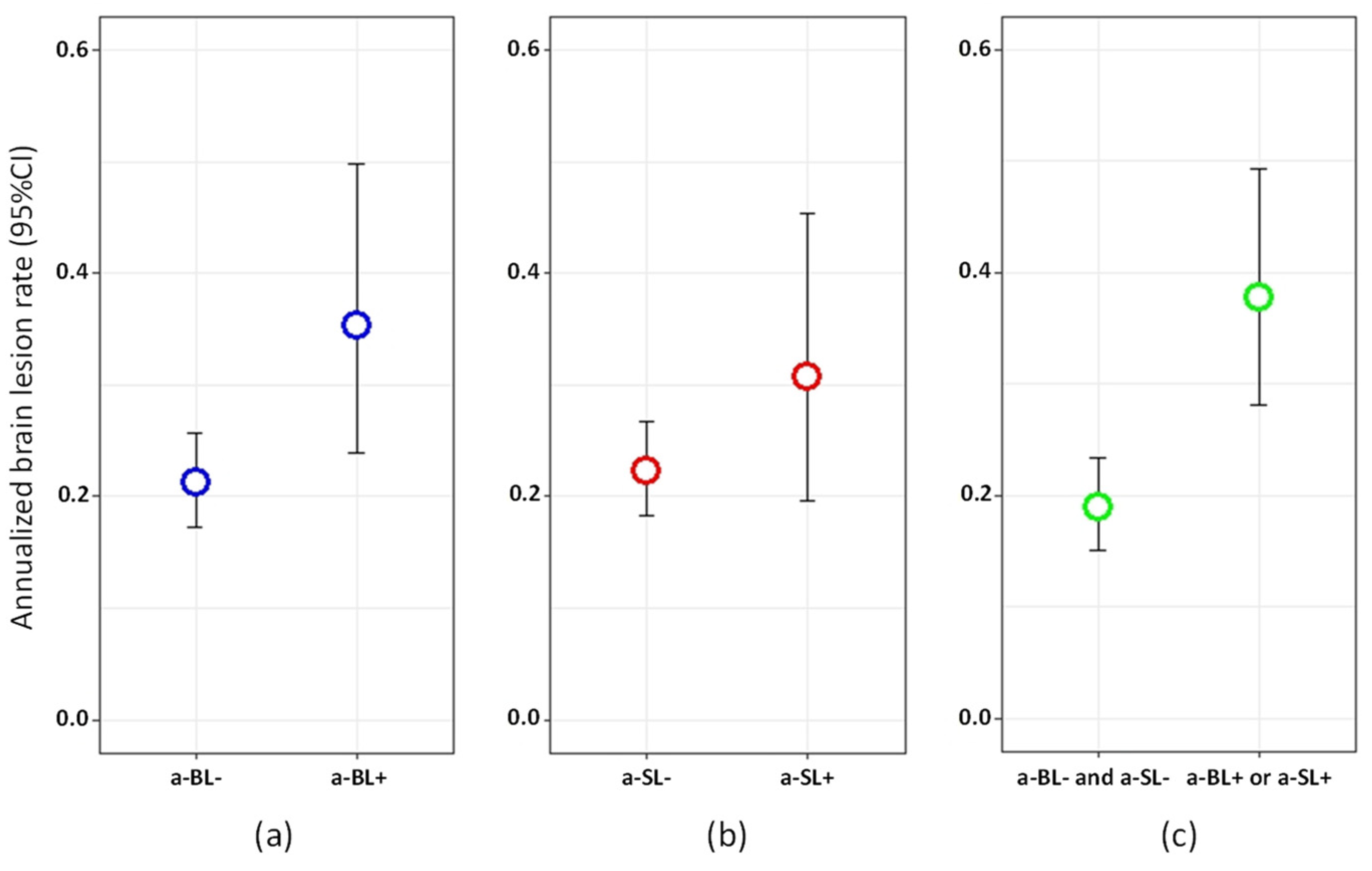
3.3. New Brain Demyelinating Lesions
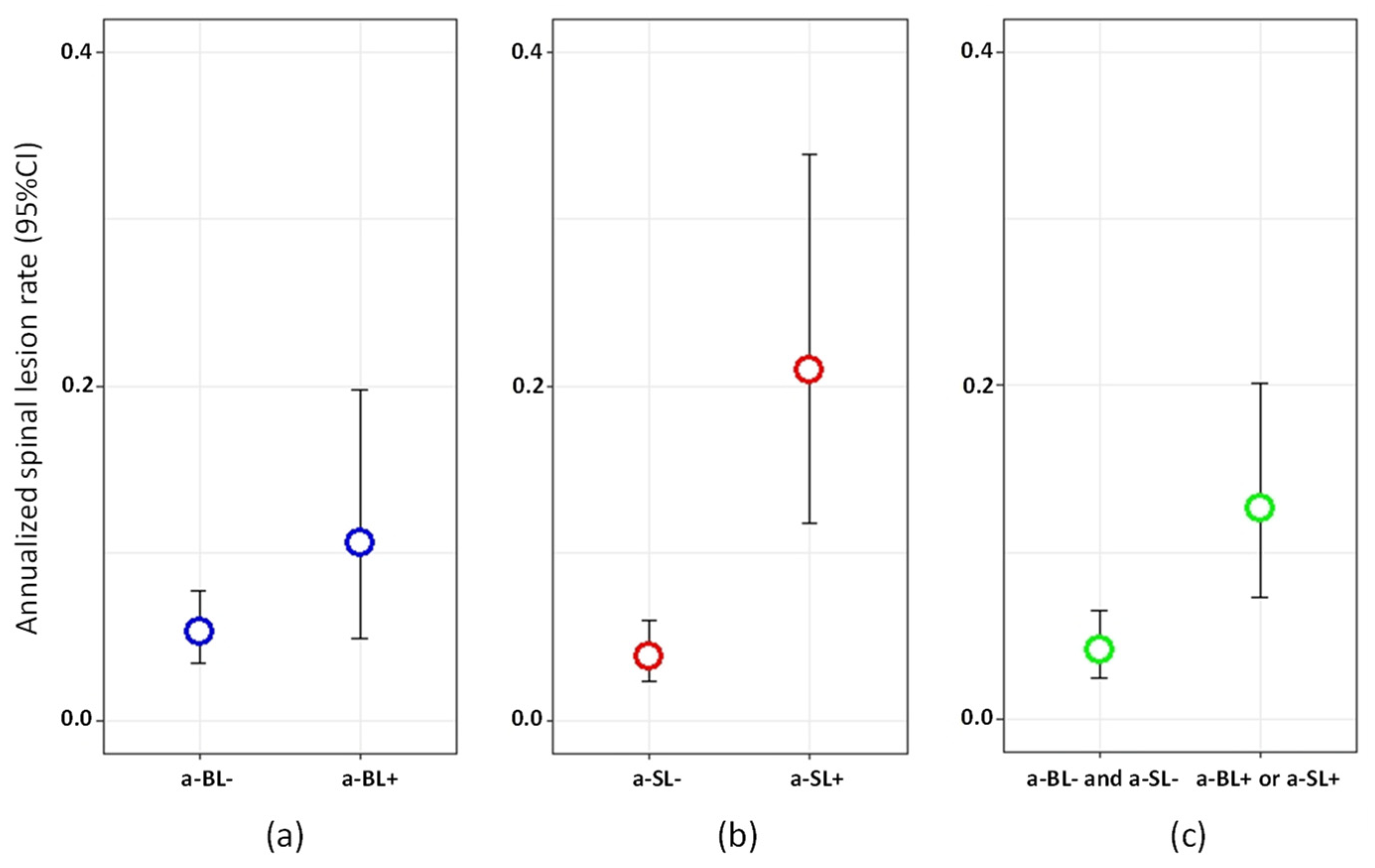
3.4. New Spinal Demyelinating Lesions
3.5. Subgroup of Patients with Available Brain MRI at T1 and T2
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ciccarelli, O.; Cohen, J.A.; Reingold, S.C.; Weinshenker, B.G.; Amato, M.P.; Banwell, B.; Barkhof, F.; Bebo, B.; Becher, B.; Bethoux, F.; et al. Spinal cord involvement in multiple sclerosis and neuromyelitis optica spectrum disorders. Lancet Neurol. 2019, 18, 185–197. [Google Scholar] [CrossRef]
- Bican, O.; Minagar, A.; Pruitt, A. The spinal cord: A review of functional neuroanatomy. Neurol. Clin. 2013, 31. [Google Scholar] [CrossRef]
- Filippi, M.; Rocca, M.A.; Ciccarelli, O.; De Stefano, N.; Evangelou, N.; Kappos, L.; Rovira, A.; Sastre-Garriga, J.; Tintorè, M.; Frederiksen, J.L.; et al. MRI criteria for the diagnosis of multiple sclerosis: MAGNIMS consensus guidelines. Lancet Neurol. 2016, 15, 292–303. [Google Scholar] [CrossRef]
- Montalban, X.; Gold, R.; Thompson, A.J.; Otero-Romero, S.; Amato, M.P.; Chandraratna, D.; Clanet, M.; Comi, G.; Derfuss, T.; Fazekas, F.; et al. ECTRIMS/EAN Guideline on the pharmacological treatment of people with multiple sclerosis. Mult. Scler. 2018, 24, 96–120. [Google Scholar] [CrossRef]
- Rae-Grant, A.; Day, G.S.; Marrie, R.A.; Rabinstein, A.; Cree, B.A.; Gronseth, G.S.; Haboubi, M.; Halper, J.; Hosey, J.P.; Jones, D.E.; et al. Comprehensive systematic review summary: Disease-modifying therapies for adults with multiple sclerosis: Report of the guideline development, dissemination, and implementation subcommittee of the American Academy of Neurology. Neurology. 2018, 90, 789–800. [Google Scholar] [CrossRef]
- Wattjes, M.P.; Rovira, À.; Miller, D.; Yousry, T.A.; Sormani, M.P.; De Stefano, N.; Tintor, M.; Auger, C.; Tur, C.; Filippi, M.; et al. Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis--establishing disease prognosis and monitoring patients. Nat. Rev. Neurol. 2015, 11, 597–606. [Google Scholar] [PubMed]
- Rocca, M.A.; Preziosa, P.; Filippi, M. What role should spinal cord MRI take in the future of multiple sclerosis surveillance? Expert Rev. Neurother. 2020, 25, 1–15. [Google Scholar] [CrossRef]
- Granella, F.; Tsantes, E.; Graziuso, S.; Bazzurri, V.; Crisi, G.; Curti, E. Spinal cord lesions are frequently asymptomatic in relapsing-remitting multiple sclerosis: A retrospective MRI survey. J. Neurol. 2019, 266, 3031–3037. [Google Scholar] [CrossRef]
- Zecca, C.; Disanto, G.; Sormani, M.P.; Riccitelli, G.C.; Cianfoni, A.; Del Grande, F.; Pravatà, E.; Gobbi, C. Relevance of asymptomatic spinal MRI lesions in patients with multiple sclerosis. Mult. Scler. 2016, 22, 782–791. [Google Scholar] [CrossRef]
- Okuda, D.T.; Mowry, E.M.; Cree, B.A.C.; Crabtree, E.C.; Goodin, D.S.; Waubant, E.; Pelletier, D. Asymptomatic spinal cord lesions predict disease progression in RIS. Neurology 2011, 76, 686–692. [Google Scholar] [CrossRef]
- Brownlee, W.J.; Altmann, D.R.; Alves Da Mota, P.; Swanton, J.K.; Miszkiel, K.A.; Wheeler-Kingshott, C.G.; Ciccarelli, O.; Miller, D.H. Association of asymptomatic spinal cord lesions and atrophy with disability 5 years after a CIS. Mult. Scler. 2017, 23, 665–674. [Google Scholar] [CrossRef]
- Kearney, H.; Altmann, D.R.; Samson, R.S.; Yiannakas, M.C.; Wheeler-Kingshott, C.A.; Ciccarelli, O.; Miller, D.H. Cervical cord lesion load is associated with disability independently from atrophy in MS. Neurology 2015, 84, 367–373. [Google Scholar] [CrossRef]
- Mowry, E.M.; Deen, S.; Malikova, I.; Pelletier, J.; Bacchetti, P.; Waubant, E. The onset location of multiple sclerosis predicts the location of subsequent relapses. J. Neurol. Neurosurg. Psychiatr. 2009, 80, 400–403. [Google Scholar] [CrossRef]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Okuda, D.T.; Mowry, E.M.; Beheshtian, A.; Waubant, E.; Baranzini, S.E.; Goodin, D.S.; Hauser, S.L.; Pelletier, D. Incidental MRI anomalies suggestive of multiple sclerosis: The radiologically isolated syndrome. Neurology 2009, 72, 800–805. [Google Scholar] [CrossRef]
- Thorpe, J.W.; Kidd, D.; Moseley, I.F.; Kendall, B.E.; Thompson, A.J.; MacManus, D.G.; McDonald, W.I.; Miller, D.H. Serial gadolinium-enhanced MRI of the brain and spinal cord in early relapsing–remitting multiple sclerosis. Neurology 1996, 46, 373–378. [Google Scholar] [CrossRef]
- Wiebe, S.; Lee, D.H.; Karlik, S.J.; Hopkins, M.; Vandervoort, M.K.; Wong, C.J.; Hewitt, L.; Rice, G.P.A.; Ebers, G.C.; Noseworthy, J.H. Serial cranial and spinal cord magnetic resonance imaging in multiple sclerosis. Ann. Neurol. 1992, 32, 643–650. [Google Scholar] [CrossRef]
- Dekker, I.; Sombekke, M.H.; Balk, L.J.; Moraal, B.; Geurts, J.J.; Barkhof, F.; Uitdehaag, B.M.; Killestein, J.; Wattjes, M.P. Infratentorial and spinal cord lesions: Cumulative predictors of long-term disability? Mult. Scler. 2019, 2. [Google Scholar] [CrossRef]
- Brownlee, W.J.; Altmann, D.R.; Prados, F.; Miszkiel, K.A.; Eshaghi, A.; Gandini Wheeler-Kingshott, C.A.; Barkhof, F.; Ciccarelli, O. Early imaging predictors of long-term outcomes in relapse-onset multiple sclerosis. Brain 2019, 142, 2276–2287. [Google Scholar] [CrossRef]
- Bot, J.C.; Barkhof, F.; Polman, C.H.; à Nijeholt, G.L.; De Groot, V.; Bergers, E.; Ader, H.J.; Castelijns, J.A. Spinal cord abnormalities in recently diagnosed MS patients: Added value of spinal MRI examination. Neurology 2004, 62, 226–233. [Google Scholar] [CrossRef]
- Schee, J.P.; Viswanathan, S. Pure spinal multiple sclerosis: A possible novel entity within the multiple sclerosis disease spectrums. Mult. Scler. J. 2019, 25, 1189–1195. [Google Scholar] [CrossRef]
- Swanton, J.K.; Fernando, K.T.; Dalton, C.M.; Miszkiel, K.A.; Altmann, D.R.; Plant, G.T.; Thompson, A.J.; Miller, D.H. Early MRI in optic neuritis: The risk for disability. Neurology 2009, 72, 542–550. [Google Scholar] [CrossRef]
- D’Amico, E.; Patti, F.; Leone, C.; Lo Fermo, S.; Zappia, M. Negative prognostic impact of MRI spinal lesions in the early stages of relapsing-remitting multiple sclerosis. Mult. Scler. J. Exp. Transl. Clin. 2016, 2. [Google Scholar] [CrossRef]
- Arrambide, G.; Rovira, A.; Sastre-Garriga, J.; Tur, C.; Castilló, J.; Río, J.; Vidal-Jordana, A.; Galán, I.; Rodríguez-Acevedo, B.; Midaglia, L.; et al. Spinal cord lesions: A modest contributor to diagnosis in clinically isolated syndromes but a relevant prognostic factor. Mult. Scler. 2018, 24, 301–312. [Google Scholar] [CrossRef]
- Leray, E.; Yaouanq, J.; Le Page, E.; Coustans, M.; Laplaud, D.; Oger, J.; Edan, G. Evidence for a two-stage disability progression in multiple sclerosis. Brain 2010, 133, 1900–1913. [Google Scholar] [CrossRef]
- Coles, A.J.; Cox, A.; Le Page, E.; Jones, J.; Trip, S.A.; Deans, J.; Seaman, S.; Miller, D.H.; Hale, G.; Waldmann, H.; et al. The window of therapeutic opportunity in multiple sclerosis: Evidence from monoclonal antibody therapy. Neurology 2006, 253, 98–108. [Google Scholar] [CrossRef]
- Lukas, C.; Sombekke, M.H.; Bellenberg, B.; Hahn, H.K.; Popescu, V.; Bendfeldt, K.; Radue, E.W.; Gass, A.; Borgwardt, S.J.; Kappos, L.; et al. Relevance of spinal cord abnormalities to clinical disability in multiple sclerosis: MR imaging findings in a large cohort of patients. Radiology 2013, 269, 542–552. [Google Scholar] [CrossRef]
- Gass, A.; Rocca, M.A.; Agosta, F.; Ciccarelli, O.; Chard, D.; Valsasina, P.; Brooks, J.C.; Bischof, A.; Eisele, P.; Kappos, L.; et al. MRI monitoring of pathological changes in the spinal cord in patients with multiple sclerosis. Lancet Neurol. 2015, 14, 443–454. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients Included (n = 300) | Brain MRI Available at T1 and T2 (n = 168) | Brain MRI Not Available at T1 and T2 (n = 132) | p-Value | |
|---|---|---|---|---|
| Female sex, n (%) | 209 (69.67) | 119 (70.83) | 90 (68.18) | 0.620 |
| Disease course, n (%) | 0.048 | |||
| RRMS | 249 (83.00) | 132 (78.57) | 117 (88.64) | |
| SPMS | 36 (12.00) | 24 (14.29) | 12 (9.09) | |
| PPMS | 15 (5.00) | 12 (7.14) | 3 (2.27) | |
| Age, years, mean (SD) | 42.45 (11.87) | 42.53 (11.67) | 42.35 (12.16) | 0.619 |
| Years since MS symptoms onset, mean (SD) | 9.81 (8.92) | 9.49 (8.83) | 10.22 (9.04) | 0.774 |
| EDSS score, median (range) | 2.5 (0.0–7.0) | 2.5 (0.0–7.0) | 2.0 (0.0–6.5) | 0.166 |
| Interval range t1–t2, median (range), months | 14.30 (12.00–20.83) | 13.15 (11.70–19.25) | 16.03 (11.74–20.10) | 0.347 |
| Interval range t2–t3, median (range), months | 31.07 (17.14–49.99) | 37.28 (19.96–65.57) | 23.47 (14.00–39.12) | <0.0001 |
| Treatments, n (%) | 0.151 | |||
| Injectable DMT | 110 (36.67) | 66 (36.29) | 44 (33.33) | |
| Oral DMT | 63 (21.00) | 28 (16.67) | 35 (26.52) | |
| Monoclonal antibodies | 89 (29.67) | 48 (28.57) | 41 (30.06) | |
| Others | 17 (5.67) | 12 (7.14) | 5 (3.79) | |
| None | 21 (7.00) | 14 (8.33) | 7 (5.30) | |
| Brain MRI at T1, n (%) | ||||
| T2 lesions ≥ 9 | 296 (98.67) | 164 (97.62) | 132 (100) | 0.133 |
| Spinal MRI at T1, n (%) | ||||
| T2 lesions ≥ 1 | 269 (89.67) | 157 (93.45) | 112 (84.45) | 0.015 |
| Cervical lesions ≥ 1 | 253 (84.33) | 150 (89.29) | 103 (78.03) | 0.008 |
| Thoracic lesions ≥ 1 | 194 (64.67) | 113 (67.26) | 81 (61.36) | 0.289 |
| Variable | Disability in All Patients (n = 300) | Relapses in RRMS (n = 249) | |||||
|---|---|---|---|---|---|---|---|
| Time to EDSS Progression | TTFR | ARR | |||||
| HR (95% CI) | p | HR (95% CI) | p | RR (95% CI) | p | ||
| a-SL | no | - | - | - | - | - | - |
| yes | 0.68 (0.29–1.58) | 0.367 | 1.79 (0.67–4.79) | 0.240 | 1.76 (0.75–3.62) | 0.154 | |
| Age at MS onset | per year | 1.01 (0.99–1.04) | 0.229 | 1.01 (0.97–1.04) | 0.747 | 0.99 (0.96–1.02) | 0.623 |
| Disease duration | per year | 0.99 (0.95–1.02) | 0.386 | 0.99 (0.94–1.04) | 0.684 | 0.98 (0.93–1.02) | 0.346 |
| Gender | female | - | - | - | - | - | - |
| male | 0.85 (0.49–1.49) | 0.571 | 0.82 (0.35–1.96) | 0.661 | 0.83 (0.40–1.62) | 0.609 | |
| EDSS score | per point | 1.01 (0.84–1.20) | 0.947 | 0.75 (0.53–1.05) | 0.099 | 0.69 (0.52–0.91) | 0.010 |
| Treatment history | untreated | - | - | - | - | - | - |
| treated | 0.56 (0.26–1.24) | 0.151 | 1.02 (0.24–4.33) | 0.975 | 0.74 (0.30–2.47) | 0.568 | |
| Disease course | RRMS | - | - | - | - | - | - |
| PPMS | 4.33 (2.08–9.02) | <0.0001 | - | - | - | - | |
| SPMS | 2.63 (1.41–4.89) | <0.0001 | - | - | - | - | |
| Variable | New Brain Lesions at T3 | New Spinal Lesions at T3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | ||||||
| RR (95% CI) | p | RR (95% CI) | p | RR (95% CI) | p | RR (95% CI) | p | ||
| a-SL | no | - | - | - | - | - | - | - | - |
| yes | 1.67 (1.19–2.30) | 0.002 | 1.63 (1.16–2.25) | 0.003 | 7.99 (4.44–14.42) | <0.0001 | 7.28 (4.02–13.22) | <0.0001 | |
| Age at MS onset | per year | 0.96 (0.95–0.97) | <0.0001 | 0.98 (0.97–1.00) | 0.024 | 0.98 (0.95–1.00) | 0.096 | - | - |
| Disease duration | per year | 0.96 (0.94–0.98) | <0.0001 | - | - | 0.93 (0.89–0.98) | 0.005 | - | - |
| Gender | female | - | - | - | - | - | - | - | - |
| male | 0.58 (0.42–0.79) | 0.001 | 0.72 (0.52–0.99) | 0.046 | 0.79 (0.39–1.49) | 0.491 | |||
| EDSS score | per point | 0.64 (0.57–0.71) | <0.0001 | 0.72 (0.63–0.83) | <0.0001 | 0.70 (0.55–0.88) | 0.003 | 0.74 (0.56–0.96) | 0.032 |
| Treatment history | untreated | - | - | - | - | - | - | - | - |
| treated | 0.81 (0.53–1.33) | 0.38 | - | - | 0.69 (0.30–1.99) | 0.430 | - | - | |
| Disease course | RRMS | - | - | - | - | - | - | - | - |
| Progressive MS | 0.37 (0.23–0.58) | <0.0001 | - | - | 0.51 (0.17–1.17) | 0.153 | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ostini, C.; Bovis, F.; Disanto, G.; Ripellino, P.; Pravatà, E.; Sacco, R.; Padlina, G.; Sormani, M.P.; Gobbi, C.; Zecca, C. Recurrence and Prognostic Value of Asymptomatic Spinal Cord Lesions in Multiple Sclerosis. J. Clin. Med. 2021, 10, 463. https://doi.org/10.3390/jcm10030463
Ostini C, Bovis F, Disanto G, Ripellino P, Pravatà E, Sacco R, Padlina G, Sormani MP, Gobbi C, Zecca C. Recurrence and Prognostic Value of Asymptomatic Spinal Cord Lesions in Multiple Sclerosis. Journal of Clinical Medicine. 2021; 10(3):463. https://doi.org/10.3390/jcm10030463
Chicago/Turabian StyleOstini, Camilla, Francesca Bovis, Giulio Disanto, Paolo Ripellino, Emanuele Pravatà, Rosaria Sacco, Giovanna Padlina, Maria Pia Sormani, Claudio Gobbi, and Chiara Zecca. 2021. "Recurrence and Prognostic Value of Asymptomatic Spinal Cord Lesions in Multiple Sclerosis" Journal of Clinical Medicine 10, no. 3: 463. https://doi.org/10.3390/jcm10030463
APA StyleOstini, C., Bovis, F., Disanto, G., Ripellino, P., Pravatà, E., Sacco, R., Padlina, G., Sormani, M. P., Gobbi, C., & Zecca, C. (2021). Recurrence and Prognostic Value of Asymptomatic Spinal Cord Lesions in Multiple Sclerosis. Journal of Clinical Medicine, 10(3), 463. https://doi.org/10.3390/jcm10030463