
Analyzing Femorotibial Cartilage Thickness Using Anatomically Standardized Maps: Reproducibility and Reference Data

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Procedure
2.2. Anatomically Standardized Cartilage Thickness Map
2.3. Statistical Analysis
3. Results
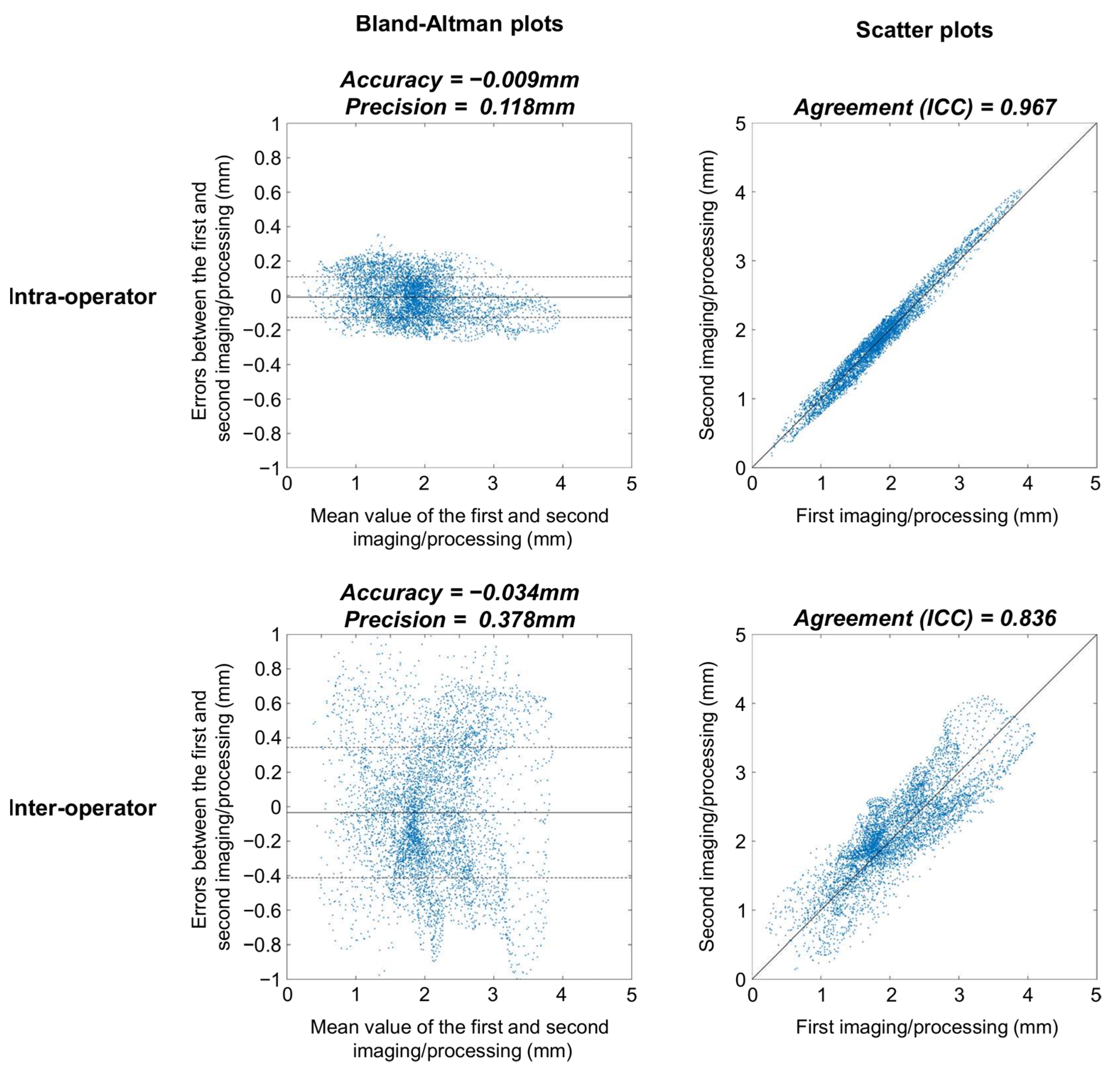
3.1. Intra- and Inter-Operator Reproducibility
3.2. Differences among Healthy Knees
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.D.; Golightly, Y.M. Epidemiology of osteoarthritis: State of the evidence. Curr. Opin. Rheumatol. 2015, 27, 276. [Google Scholar] [CrossRef] [PubMed]
- Recht, M.; Bobic, V.; Burstein, D.; Disler, D.; Gold, G.; Gray, M.; Kramer, J.; Lang, P.; McCauley, T.; Winalski, C. Magnetic resonance imaging of articular cartilage. Clin. Orthop. Relat. Res. 2001, 391, S379–S396. [Google Scholar] [CrossRef] [PubMed]
- Gold, G.E.; Chen, C.A.; Koo, S.; Hargreaves, B.A.; Bangerter, N.K. Recent advances in MRI of articular cartilage. AJR Am. J. Roentgenol. 2009, 193, 628–638. [Google Scholar] [CrossRef]
- Cohen, Z.A.; Mow, V.C.; Henry, J.H.; Levine, W.N.; Ateshian, G.A. Templates of the cartilage layers of the patellofemoral joint and their use in the assessment of osteoarthritic cartilage damage. Osteoarthr Cartil. 2003, 11, 569–579. [Google Scholar] [CrossRef]
- Koo, S.; Gold, G.E.; Andriacchi, T.P. Considerations in measuring cartilage thickness using MRI: Factors influencing reproducibility and accuracy. Osteoarthr. Cartil. 2005, 13, 782–789. [Google Scholar] [CrossRef]
- Andriacchi, T.P.; Koo, S.; Scanlan, S.F. Gait mechanics influence healthy cartilage morphology and osteoarthritis of the knee. J Bone Jt. Surg. Am. 2009, 91 (Suppl. 1), 95–101. [Google Scholar] [CrossRef]
- Wirth, W.; Benichou, O.; Kwoh, C.K.; Guermazi, A.; Hunter, D.; Putz, R.; Eckstein, F.; Investigators, O.A.I. Spatial patterns of cartilage loss in the medial femoral condyle in osteoarthritic knees: Data from the Osteoarthritis Initiative. Magn. Reson. Med. 2010, 63, 574–581. [Google Scholar] [CrossRef]
- Omoumi, P.; Babel, H.; Jolles, B.M.; Favre, J. Relationships between cartilage thickness and subchondral bone mineral density in non-osteoarthritic and severely osteoarthritic knees: In vivo concomitant 3D analysis using CT arthrography. Osteoarthr. Cartil. 2019, 27, 621–629. [Google Scholar] [CrossRef]
- Frobell, R.B.; Nevitt, M.C.; Hudelmaier, M.; Wirth, W.; Wyman, B.T.; Benichou, O.; Dreher, D.; Davies, R.; Lee, J.H.; Baribaud, F.; et al. Femorotibial subchondral bone area and regional cartilage thickness: A cross-sectional description in healthy reference cases and various radiographic stages of osteoarthritis in 1003 knees from the Osteoarthritis Initiative. Arthritis Care Res. 2010, 62, 1612–1623. [Google Scholar] [CrossRef]
- Favre, J.; Scanlan, S.F.; Erhart-Hledik, J.C.; Blazek, K.; Andriacchi, T.P. Patterns of femoral cartilage thickness are different in asymptomatic and osteoarthritic knees and can be used to detect disease-related differences between samples. J. Biomech. Eng. 2013, 135, 101002–101010. [Google Scholar] [CrossRef] [PubMed]
- Favre, J.; Erhart-Hledik, J.C.; Blazek, K.; Fasel, B.; Gold, G.E.; Andriacchi, T.P. Anatomically Standardized Maps Reveal Distinct Patterns of Cartilage Thickness with Increasing Severity of Medial Compartment Knee Osteoarthritis. J. Orthop. Res. 2017, 35, 2442–2451. [Google Scholar] [CrossRef] [PubMed]
- Carballido-Gamio, J.; Bauer, J.S.; Stahl, R.; Lee, K.Y.; Krause, S.; Link, T.M.; Majumdar, S. Inter-subject comparison of MRI knee cartilage thickness. Med. Image. Anal. 2008, 12, 120–135. [Google Scholar] [CrossRef] [PubMed]
- Scanlan, S.F.; Favre, J.; Andriacchi, T.P. The relationship between peak knee extension at heel-strike of walking and the location of thickest femoral cartilage in ACL reconstructed and healthy contralateral knees. J. Biomech. 2013, 46, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Babel, H.; Omoumi, P.; Andriacchi, T.P.; Jolles, B.M.; Favre, J. New insight on the subchondral bone and cartilage functional unit: Bone mineral density and cartilage thickness are spatially correlated in non-osteoarthritic femoral condyles. Osteoarthr. Cartil. Open 2020, 2, 100079. [Google Scholar] [CrossRef]
- Haralick, R.M. Statistical and Structural Approaches to Texture. Proc. IEEE 1979, 67, 786–804. [Google Scholar] [CrossRef]
- Penny, W.D.; Friston, K.J.; Ashburner, J.T.; Kiebel, S.J.; Nichols, T.E. Statistical Parametric Mapping: The Analysis of Functional Brain Images; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar]
- Eckstein, F.; Cicuttini, F.; Raynauld, J.P.; Waterton, J.C.; Peterfy, C. Magnetic resonance imaging (MRI) of articular cartilage in knee osteoarthritis (OA): Morphological assessment. Osteoarthr. Cartil. 2006, 14 (Suppl. A), A46–A75. [Google Scholar] [CrossRef]
- McGibbon, C.A. Inter-rater and intra-rater reliability of subchondral bone and cartilage thickness measurement from MRI. Magn. Reson. Imaging 2003, 21, 707–714. [Google Scholar] [CrossRef]
- Glaser, C.; Burgkart, R.; Kutschera, A.; Englmeier, K.H.; Reiser, M.; Eckstein, F. Femoro-tibial cartilage metrics from coronal MR image data: Technique, test–retest reproducibility, and findings in osteoarthritis. J. Magn. Reson. Med. 2003, 50, 1229–1236. [Google Scholar] [CrossRef]
- Duryea, J.; Neumann, G.; Brem, M.H.; Koh, W.; Noorbakhsh, F.; Jackson, R.D.; Yu, J.; Eaton, C.B.; Lang, P. Novel fast semi-automated software to segment cartilage for knee MR acquisitions. Osteoarthr. Cartil. 2007, 15, 487–492. [Google Scholar] [CrossRef][Green Version]
- Bruyere, O.; Genant, H.; Kothari, M.; Zaim, S.; White, D.; Peterfy, C.; Burlet, N.; Richy, F.; Ethgen, D.; Montague, T.; et al. Longitudinal study of magnetic resonance imaging and standard X-rays to assess disease progression in osteoarthritis. Osteoarthr. Cartil. 2007, 15, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Reichenbach, S.; Yang, M.; Eckstein, F.; Niu, J.; Hunter, D.J.; McLennan, C.E.; Guermazi, A.; Roemer, F.; Hudelmaier, M.; Aliabadi, P.; et al. Does cartilage volume or thickness distinguish knees with and without mild radiographic osteoarthritis? The Framingham Study. Ann. Rheum. Dis. 2010, 69, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Cotofana, S.; Buck, R.; Wirth, W.; Roemer, F.; Duryea, J.; Nevitt, M.; Eckstein, F.; Osteoarthritis Initiative Investigators Group. Cartilage thickening in early radiographic knee osteoarthritis: A within-person, between-knee comparison. Arthritis Care Res. 2012, 64, 1681–1690. [Google Scholar] [CrossRef] [PubMed]
- Favre, J.; Erhart-Hledik, J.C.; Chehab, E.F.; Andriacchi, T.P. Baseline ambulatory knee kinematics are associated with changes in cartilage thickness in osteoarthritic patients over 5 years. J. Biomech. 2016, 49, 1859–1864. [Google Scholar] [CrossRef] [PubMed]
- Blazek, K.; Favre, J.; Asay, J.; Erhart-Hledik, J.; Andriacchi, T. Age and obesity alter the relationship between femoral articular cartilage thickness and ambulatory loads in individuals without osteoarthritis. J. Orthop. Res. 2014, 32, 394–402. [Google Scholar] [CrossRef] [PubMed]
- De Boor, C. On calculating with B-splines. J. Approx. Theory 1972, 6, 50–62. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Measurement in Medicine—The Analysis of Method Comparison Studies. J. R. Stat. Soc. Series D Stat. 1983, 32, 307–317. [Google Scholar] [CrossRef]
- Shannon, C.E. A mathematical theory of communication. J. ACM Sigmobile 2001, 5, 3–55. [Google Scholar] [CrossRef]
- McGraw, K.O.; Wong, S.P. Forming inferences about some intraclass correlation coefficients. J. Psychol. Methods 1996, 1, 30. [Google Scholar] [CrossRef]
- Van Leersum, M.D.; Schweitzer, M.E.; Gannon, F.; Vinitski, S.; Finkel, G.; Mitchell, D.G. Thickness of patellofemoral articular cartilage as measured on MR imaging: Sequence comparison of accuracy, reproducibility, and interobserver variation. Skelet. Radiol. 1995, 24, 431–435. [Google Scholar] [CrossRef]
- Favre, J.; Fasel, B.; Andriacchi, T.P. Pattern in Femoral Cartilage Thickness Map Allows Subtle Scoring of Medial Compartment Knee Osteoarthritis Severity. Osteoarthr. Cartil. 2013, 21, S231–S232. [Google Scholar] [CrossRef]
- Andriacchi, T.P.; Favre, J.; Erhart-Hledik, J.C.; Chu, C.R. A Systems View of Risk Factors for Knee Osteoarthritis Reveals Insights into the Pathogenesis of the Disease. Ann. Biomed. Eng. 2015, 43, 376–387. [Google Scholar] [CrossRef] [PubMed]
- Edd, S.N.; Omoumi, P.; Andriacchi, T.P.; Jolles, B.M.; Favre, J. Modeling knee osteoarthritis pathophysiology using an integrated joint system (IJS): A systematic review of relationships among cartilage thickness, gait mechanics, and subchondral bone mineral density. Osteoarthr. Cartil. 2018, 26, 1425–1437. [Google Scholar] [CrossRef] [PubMed]
- Koo, S.; Andriacchi, T.P. A comparison of the influence of global functional loads vs. local contact anatomy on articular cartilage thickness at the knee. J. Biomech. 2007, 40, 2961–2966. [Google Scholar] [CrossRef]
- Koo, S.; Rylander, J.H.; Andriacchi, T.P. Knee joint kinematics during walking influences the spatial cartilage thickness distribution in the knee. J. Biomech. 2011, 44, 1405–1409. [Google Scholar] [CrossRef]
- Chao, E.Y.; Laughman, R.K.; Schneider, E.; Stauffer, R.N. Normative data of knee joint motion and ground reaction forces in adult level walking. J. Biomech. 1983, 16, 219–233. [Google Scholar] [CrossRef]
- Chehab, E.F.; Andriacchi, T.P.; Favre, J. Speed, age, sex, and body mass index provide a rigorous basis for comparing the kinematic and kinetic profiles of the lower extremity during walking. J. Biomech. 2017, 58, 11–20. [Google Scholar] [CrossRef]
- Eckstein, F.; Kwoh, C.K.; Link, T.M.; OAI Investigators. Imaging research results from the osteoarthritis initiative (OAI): A review and lessons learned 10 years after start of enrolment. Ann. Rheum. Dis. 2014, 73, 1289–1300. [Google Scholar] [CrossRef]
- Zijdenbos, A.P.; Dawant, B.M.; Margolin, R.A.; Palmer, A.C. Morphometric analysis of white matter lesions in MR images: Method and validation. IEEE Trans. Med. Imaging 1994, 13, 716–724. [Google Scholar] [CrossRef]
- Erhart-Hledik, J.C.; Favre, J.; Andriacchi, T.P. New insight in the relationship between regional patterns of knee cartilage thickness, osteoarthritis disease severity, and gait mechanics. J. Biomech. 2015, 48, 3868–3875. [Google Scholar] [CrossRef]
- Fripp, J.; Crozier, S.; Warfield, S.K.; Ourselin, S. Automatic segmentation and quantitative analysis of the articular cartilages from magnetic resonance images of the knee. IEEE Trans. Med. Imaging 2010, 29, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Shan, L.; Zach, C.; Charles, C.; Niethammer, M. Automatic atlas-based three-label cartilage segmentation from MR knee images. Med. Image Anal. 2014, 18, 1233–1246. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, F.; Yang, M.; Guermazi, A.; Roemer, F.; Hudelmaier, M.; Picha, K.; Baribaud, F.; Wirth, W.; Felson, D. Reference values and Z-scores for subregional femorotibial cartilage thickness–results from a large population-based sample (Framingham) and comparison with the non-exposed Osteoarthritis Initiative reference cohort. Osteoarthr. Cartil. 2010, 18, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Janvier, T.; Jennane, R.; Toumi, H.; Lespessailles, E. Subchondral tibial bone texture predicts the incidence of radiographic knee osteoarthritis: Data from the Osteoarthritis Initiative. Osteoarthr. Cartil. 2017, 25, 2047–2054. [Google Scholar] [CrossRef]
- Carballido-Gamio, J.; Joseph, G.B.; Lynch, J.A.; Link, T.M.; Majumdar, S. Longitudinal analysis of MRI T2 knee cartilage laminar organization in a subset of patients from the osteoarthritis initiative: A texture approach. Magn. Reson. Med. 2011, 65, 1184–1194. [Google Scholar] [CrossRef]
- Edd, S.N.; Babel, H.; Kerkour, N.; Jolles, B.M.; Omoumi, P.; Favre, J.J.T.K. Comprehensive description of T2 value spatial variations in non-osteoarthritic femoral cartilage using three-dimensional registration of morphological and relaxometry data. Knee 2019, 26, 555–563. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Intra-Operator | Inter-Operator | |||
|---|---|---|---|---|
| Median | IQR | Median | IQR | |
| Accuracy (µ), mm | ||||
| Femur | −0.002 | 0.059 | −0.056 | 0.196 |
| Tibia | 0.005 | 0.054 | −0.098 | 0.616 |
| Femur + tibia | −0.006 | 0.045 | −0.003 | 0.186 |
| Precision (σ), mm | ||||
| Femur * | 0.136 | 0.085 | 0.371 | 0.131 |
| Tibia * | 0.146 | 0.061 | 0.467 | 0.258 |
| Femur + tibia * | 0.152 | 0.070 | 0.496 | 0.132 |
| Entropy (H) | ||||
| Femur | 7.27 | 0.65 | 7.26 | 0.56 |
| Tibia | 7.13 | 0.66 | 7.17 | 0.39 |
| Femur + tibia | 7.02 | 0.71 | 6.92 | 0.32 |
| Agreement (ICC) | ||||
| Femur * | 0.974 | 0.017 | 0.823 | 0.094 |
| Tibia * | 0.976 | 0.025 | 0.769 | 0.145 |
| Femur + tibia * | 0.975 | 0.020 | 0.808 | 0.108 |
| Differences Compared to | ||||||
|---|---|---|---|---|---|---|
| Same Knee | Contralateral Knee | Matched Knee | ||||
| Median | IQR | Median | IQR | Median | IQR | |
| Offset (µ), mm | ||||||
| Femur | −0.002 | 0.059 | −0.033 | 0.107 | 0.064 | 0.261 |
| Tibia | 0.005 | 0.054 | −0.086 | 0.180 | 0.103 | 0.215 |
| Femur + tibia | −0.006 | 0.045 | −0.036 | 0.137 | 0.063 | 0.254 |
| Dispersion (σ), mm | ||||||
| Femur *,#,¶ | 0.136 | 0.085 | 0.219 | 0.092 | 0.458 | 0.125 |
| Tibia *,# | 0.146 | 0.061 | 0.241 | 0.077 | 0.248 | 0.051 |
| Femur + tibia * | 0.152 | 0.070 | 0.233 | 0.074 | Ø | |
| Agreement (ICC) | ||||||
| Femur *,#,¶ | 0.974 | 0.017 | 0.936 | 0.031 | 0.749 | 0.049 |
| Tibia *,# | 0.976 | 0.025 | 0.936 | 0.062 | 0.934 | 0.033 |
| Femur + tibia * | 0.975 | 0.020 | 0.936 | 0.020 | Ø | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Favre, J.; Babel, H.; Cavinato, A.; Blazek, K.; Jolles, B.M.; Andriacchi, T.P. Analyzing Femorotibial Cartilage Thickness Using Anatomically Standardized Maps: Reproducibility and Reference Data. J. Clin. Med. 2021, 10, 461. https://doi.org/10.3390/jcm10030461
Favre J, Babel H, Cavinato A, Blazek K, Jolles BM, Andriacchi TP. Analyzing Femorotibial Cartilage Thickness Using Anatomically Standardized Maps: Reproducibility and Reference Data. Journal of Clinical Medicine. 2021; 10(3):461. https://doi.org/10.3390/jcm10030461
Chicago/Turabian StyleFavre, Julien, Hugo Babel, Alessandro Cavinato, Katerina Blazek, Brigitte M. Jolles, and Thomas P. Andriacchi. 2021. "Analyzing Femorotibial Cartilage Thickness Using Anatomically Standardized Maps: Reproducibility and Reference Data" Journal of Clinical Medicine 10, no. 3: 461. https://doi.org/10.3390/jcm10030461
APA StyleFavre, J., Babel, H., Cavinato, A., Blazek, K., Jolles, B. M., & Andriacchi, T. P. (2021). Analyzing Femorotibial Cartilage Thickness Using Anatomically Standardized Maps: Reproducibility and Reference Data. Journal of Clinical Medicine, 10(3), 461. https://doi.org/10.3390/jcm10030461