
Novel Coronavirus Infection (COVID-19) Related Thrombotic and Bleeding Complications in Critically Ill Patients: Experience from an Academic Medical Center

 ,
, 
Abstract
:1. Introduction
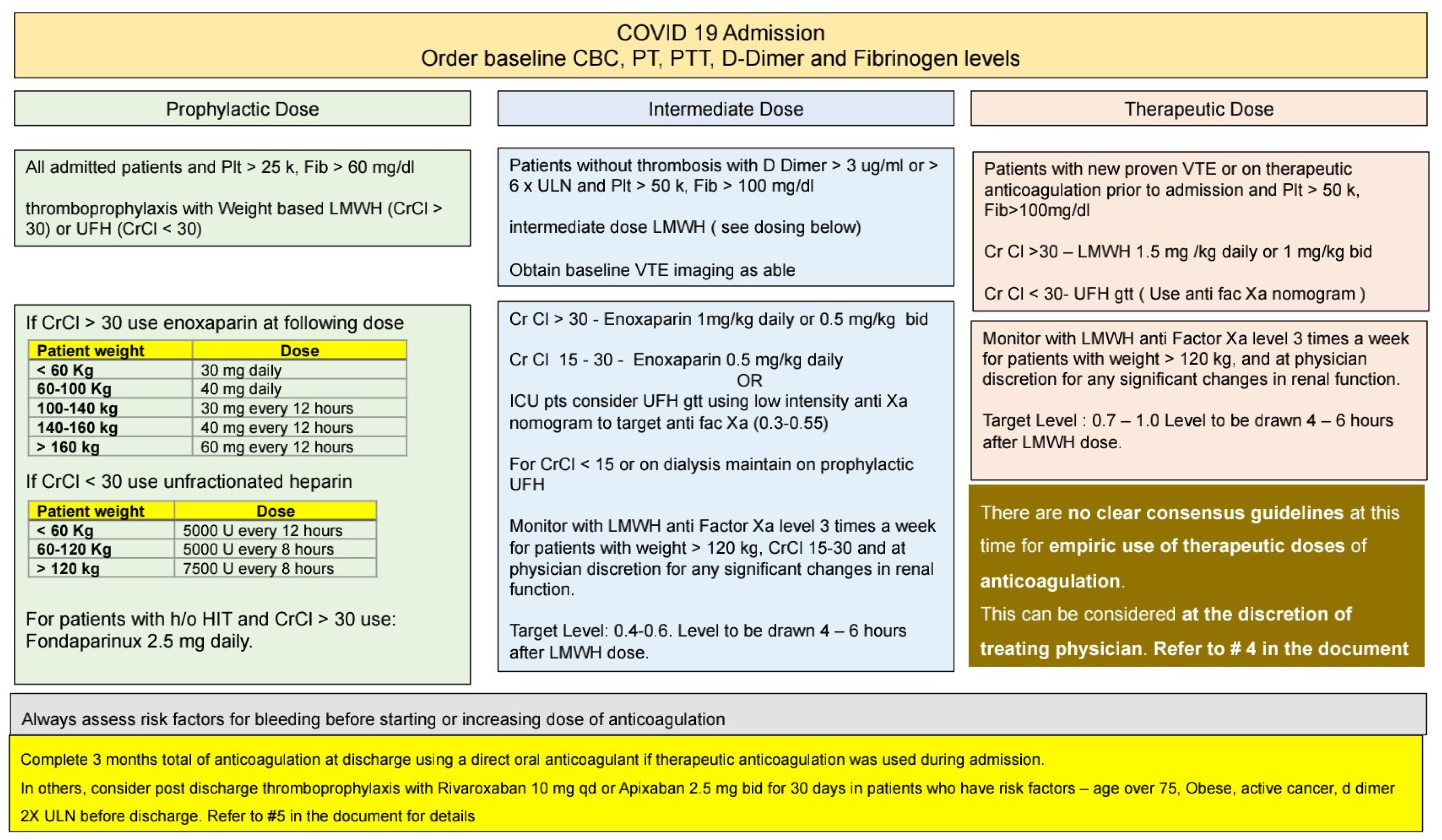
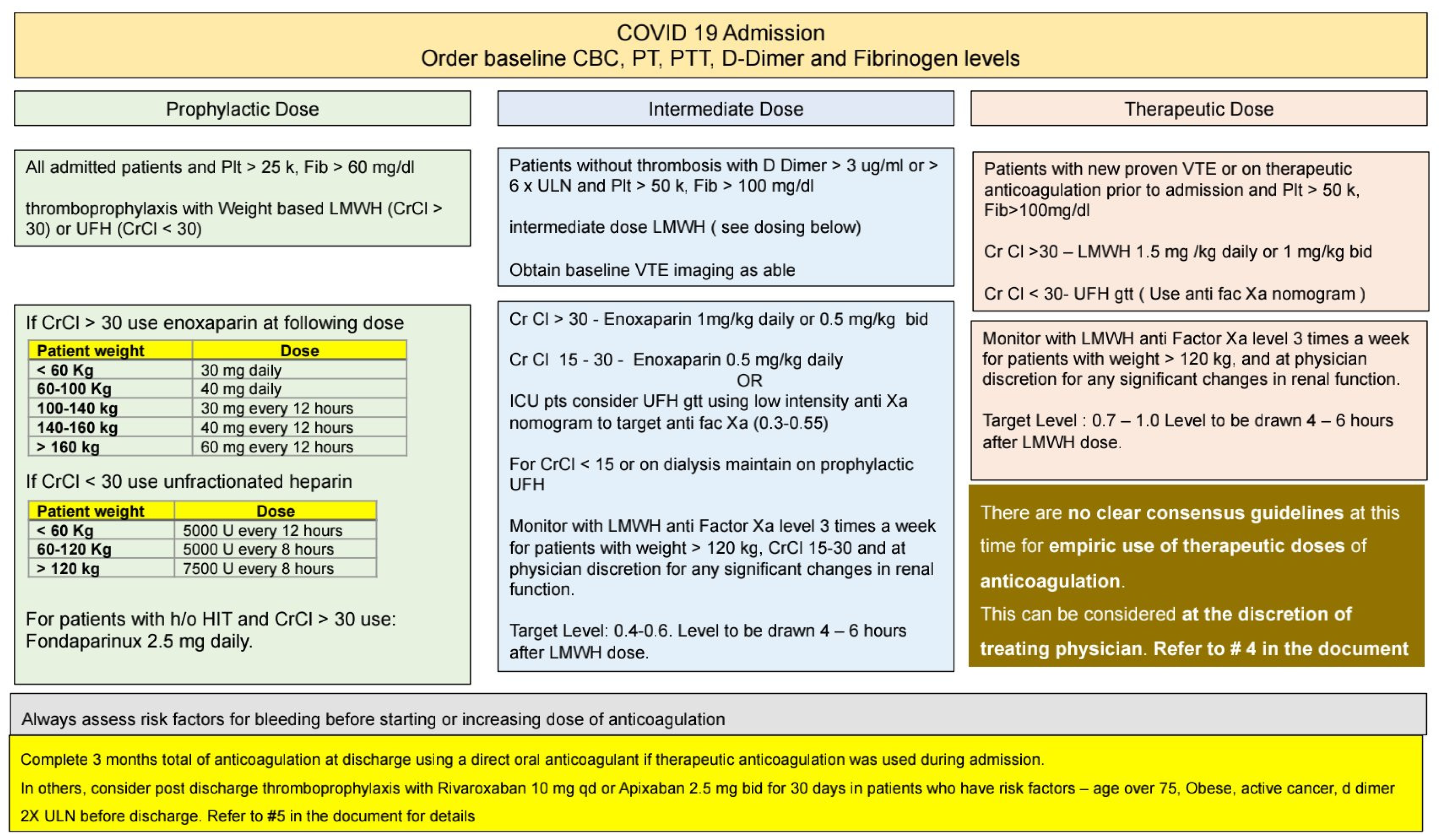
2. Methods
2.1. Study Population
2.2. Outcomes Analyzed Were as Follows
2.2.1. Primary Outcomes
- Clinically significant thrombosis of the different types, including DVT, hepatic vein thrombosis, and arterial thrombosis.
- Clinically significant bleeding of the different types as defined by the ISTH definition of having a symptomatic presentation and (1) fatal bleeding and/or (2) bleeding in a critical area or organ (such as intracranial, intraspinal, intraocular, retroperitoneal, intra-articular, pericardial, or intramuscular bleeding with compartment syndrome) and/or (3) bleeding causing a fall in hemoglobin level to 20 g L−1 (1.24 mmol L−1) or less or leading to the transfusion of two or more units of whole blood or red cells [24].
2.2.2. Secondary Outcomes
- Mortality.
- Correlative analysis of development of thrombus with the type of anticoagulation.
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Patients Admitted to ICU
3.2. ICU Treatments
3.3. Thrombotic or Bleeding Complications
3.4. ICU Complications and Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- CDC Coronavirus Disease 2019 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/racial-ethnic-minorities.html (accessed on 6 May 2020).
- Leentjens, J.; van Haaps, T.F.; Wessels, P.F.; Schutgens, R.E.G.; Middeldorp, S. COVID-19-associated coagulopathy and antithrombotic agents—Lessons after 1 year. Lancet Haematol. 2021. [Google Scholar] [CrossRef]
- Słomka, A.; Kowalewski, M.; Żekanowska, E. Hemostasis in Coronavirus Disease 2019-Lesson from Viscoelastic Methods: A Systematic Review. Thromb. Haemost. 2021, 121, 1181–1192. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Gupta, S.; Leaf, R.K.; Wang, W.; Rosovsky, R.P.; Brenner, S.K.; Hayek, S.S.; Berlin, H.; Kapoor, R.; Shaefi, S.; et al. Thrombosis, Bleeding, and the Observational Effect of Early Therapeutic Anticoagulation on Survival in Critically Ill Patients With COVID-19. Ann. Intern. Med. 2021, 174, 622–632. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Karp Leaf, R.S.; Dzik, W.H.; Carlson, J.C.T.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID-19 and coagulation: Bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Giovini, M.; Leone, M.; Pizzilli, G.; Kortgen, A.; Bauer, M.; Tonetti, T.; Duclos, G.; Zieleskiewicz, L.; Buschbeck, S.; et al. Pulmonary embolism in patients with coronavirus disease-2019 (COVID-19) pneumonia: A narrative review. Ann. Intensive Care 2020, 10, 124. [Google Scholar] [CrossRef] [PubMed]
- McBane, R.D.; Torres Roldan, V.D.; Niven, A.S.; Pruthi, R.K.; Franco, P.M.; Linderbaum, J.A.; Casanegra, A.I.; Oyen, L.J.; Houghton, D.E.; Marshall, A.L.; et al. Anticoagulation in COVID-19: A Systematic Review, Meta-analysis, and Rapid Guidance From Mayo Clinic. Mayo Clin. Proc. 2020, 95, 2467–2486. [Google Scholar] [CrossRef] [PubMed]
- Ionescu, F.; Jaiyesimi, I.; Petrescu, I.; Lawler, P.R.; Castillo, E.; Munoz-Maldonado, Y.; Imam, Z.; Narasimhan, M.; Abbas, A.E.; Konde, A.; et al. Association of anticoagulation dose and survival in hospitalized COVID-19 patients: A retrospective propensity score-weighted analysis. Eur. J. Haematol. 2021, 106, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: An updated analysis. Thromb. Res. 2020, 191, 148–150. [Google Scholar] [CrossRef]
- Middeldorp, S.; Coppens, M.; van Haaps, T.F.; Foppen, M.; Vlaar, A.P.; Müller, M.C.A.; Bouman, C.C.S.; Beenen, L.F.M.; Kootte, R.S.; Heijmans, J.; et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. JTH 2020, 18, 1995–2002. [Google Scholar] [CrossRef]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.-D.; Sacco, C.; Bertuzzi, A.; et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb. Res. 2020, 191, 9–14. [Google Scholar] [CrossRef]
- Llitjos, J.-F.; Leclerc, M.; Chochois, C.; Monsallier, J.-M.; Ramakers, M.; Auvray, M.; Merouani, K. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J. Thromb. Haemost. JTH 2020, 18, 1743–1746. [Google Scholar] [CrossRef]
- INSPIRATION Investigators; Sadeghipour, P.; Talasaz, A.H.; Rashidi, F.; Sharif-Kashani, B.; Beigmohammadi, M.T.; Farrokhpour, M.; Sezavar, S.H.; Payandemehr, P.; Dabbagh, A.; et al. Effect of Intermediate-Dose vs Standard-Dose Prophylactic Anticoagulation on Thrombotic Events, Extracorporeal Membrane Oxygenation Treatment, or Mortality Among Patients With COVID-19 Admitted to the Intensive Care Unit: The INSPIRATION Randomized Clinical Trial. JAMA 2021, 325, 1620–1630. [Google Scholar] [CrossRef]
- Malas, M.B.; Naazie, I.N.; Elsayed, N.; Mathlouthi, A.; Marmor, R.; Clary, B. Thromboembolism risk of COVID-19 is high and associated with a higher risk of mortality: A systematic review and meta-analysis. EClinicalMedicine 2020, 29. [Google Scholar] [CrossRef]
- Cuker, A.; Tseng, E.K.; Nieuwlaat, R.; Angchaisuksiri, P.; Blair, C.; Dane, K.; Davila, J.; DeSancho, M.T.; Diuguid, D.; Griffin, D.O.; et al. American Society of Hematology 2021 guidelines on the use of anticoagulation for thromboprophylaxis in patients with COVID-19. Blood Adv. 2021, 5, 872–888. [Google Scholar] [CrossRef]
- Zarychanski, R.; ATTACC Investigators. Therapeutic Anticoagulation in Critically Ill Patients with Covid-19—Preliminary Report. medRxiv 2021. [Google Scholar] [CrossRef]
- Neal, M. A Multicenter, Adaptive, Randomized Controlled Platform Trial of the Safety and Efficacy of Antithrombotic Strategies in Hospitalized Adults with COVID-19. 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT04505774 (accessed on 29 July 2021).
- University of Manitoba. Antithrombotic Therapy to Ameliorate Complications of COVID-19 (ATTACC), in Collaboration with Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV-4). 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT04372589 (accessed on 29 July 2021).
- Allegheny Health Network. Wikipedia. 2020. Available online: https://en.wikipedia.org/w/index.php?title=Allegheny_Health_Network&oldid=964656458 (accessed on 5 July 2021).
- Coronavirus Response. Allegheny Health Network. Available online: https://www.ahn.org/coronavirus.html (accessed on 5 July 2020).
- Boden, S. Allegheny Health Network Starts Drive-Through Testing for COVID-19. Available online: https://www.wesa.fm/post/allegheny-health-network-starts-drive-through-testing-covid-19 (accessed on 5 July 2020).
- Schulman, S.; Kearon, C. Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. JTH 2005, 3, 692–694. [Google Scholar] [CrossRef]
- Gómez-Mesa, J.E.; Galindo-Coral, S.; Montes, M.C.; Muñoz Martin, A.J. Thrombosis and Coagulopathy in COVID-19. Curr. Probl. Cardiol. 2021, 46, 100742. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet Lond. Engl. 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Subashchandran, V.; Yuriditsky, E.; Horowitz, J.M.; Reynolds, H.R.; Hochman, J.S.; Berger, J.S. Thrombosis in hospitalized patients with viral respiratory infections versus COVID-19. Am. Heart J. 2021, 231, 93–95. [Google Scholar] [CrossRef]
- Bunce, P.E.; High, S.M.; Nadjafi, M.; Stanley, K.; Liles, W.C.; Christian, M.D. Pandemic H1N1 influenza infection and vascular thrombosis. Clin. Infect. Dis. 2011, 52, e14–e17. [Google Scholar] [CrossRef] [Green Version]
- Lim, W.; Meade, M.; Lauzier, F.; Zarychanski, R.; Mehta, S.; Lamontagne, F.; Dodek, P.; McIntyre, L.; Hall, R.; Heels-Ansdell, D.; et al. Failure of anticoagulant thromboprophylaxis: Risk factors in medical-surgical critically ill patients. Crit. Care Med. 2015, 43, 401–410. [Google Scholar] [CrossRef]
- Piscoya, A.; Ng-Sueng, L.F.; del Riego, A.P.; Cerna-Viacava, R.; Pasupuleti, V.; Roman, Y.M.; Thota, P.; White, C.M.; Hernandez, A.V. Efficacy and harms of remdesivir for the treatment of COVID-19: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0243705. [Google Scholar] [CrossRef]
- Sanfilippo, F.; La Rosa, V.; Oliveri, F.; Astuto, M. Convalescent plasma for COVID-19: The risk of pulmonary embolism should not be underestimated! Crit. Care 2020, 24, 531. [Google Scholar] [CrossRef]
- Lynn, L.; Reyes, J.A.; Hawkins, K.; Panda, A.; Linville, L.; Aldhahri, W.; Kango, G.; Shah, S.; Ayanian, S.; Teufel, K. The effect of anticoagulation on clinical outcomes in novel Coronavirus (COVID-19) pneumonia in a U.S. cohort. Thromb. Res. 2021, 197, 65–68. [Google Scholar] [CrossRef]
- Godier, A.; Clausse, D.; Meslin, S.; Bazine, M.; Lang, E.; Huche, F.; Cholley, B.; Hamada, S.R. Major bleeding complications in critically ill patients with COVID-19 pneumonia. J. Thromb. Thrombolysis 2021, 52, 18–21. [Google Scholar] [CrossRef]
- Rentsch, C.T.; Beckman, J.A.; Tomlinson, L.; Gellad, W.F.; Alcorn, C.; Kidwai-Khan, F.; Skanderson, M.; Brittain, E.; King, J.T.; Ho, Y.-L.; et al. Early initiation of prophylactic anticoagulation for prevention of coronavirus disease 2019 mortality in patients admitted to hospital in the United States: Cohort study. BMJ 2021, 372, n311. [Google Scholar] [CrossRef]
- The REMAP-CAP Investigators; The ACTIV-4a Investigators; The ATTACC Investigators. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with Covid-19. N. Engl. J. Med. 2021, NEJMoa2103417. [Google Scholar] [CrossRef]
- NEJM. Therapeutic Anticoagulation with Heparin in Noncritically Ill Patients with Covid-19. Available online: https://www.nejm.org/doi/full/10.1056/NEJMoa2105911 (accessed on 1 November 2021).
- Ten Cate, H. Surviving Covid-19 with Heparin? N. Engl. J. Med. 2021, 385, 845–846. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics (n = 144) | Percentage or Median (IQR) |
|---|---|
| Age (in years) | 64 (54.5–75) |
| Gender | |
| Male | 85 (59.0%) |
| Female | 59 (41.0) |
| Race | |
| Non-Hispanic White | 90 (62.5%) |
| Non-Hispanic Black | 36 (25.0%) |
| Others | 18 (12.5%) |
| Comorbidities | |
| Cardiovascular a | 102 (70.8%) |
| Obesity (BMI > 30 kg/m2) | 76 (52.8%) |
| Diabetes | 57 (39.6%) |
| Chronic obstructive pulmonary disease | 18 (12.5%) |
| Renal b | 24 (16.7%) |
| CCI | 1 (0–3) |
| Coagulation Labs at Transfer | |
| d-dimer | 1.5 mg/mL (1.1–4.7) |
| Platelets | 217.5 k/mcl (150–288) |
| International normalized ratio (INR) | 1.4 (1.1–1.3) |
| ICU Admission Severity of Illness | |
| APACHE-2 (40) | 12.5 (9.5–22) |
| Treatment Strategies | |
| Mechanical ventilation | 99 (68.8%) |
| Pressors | 80 (55.6%) |
| Neuromuscular blockade use | 49 (35.0%) |
| Steroids | 46 (31.9%) |
| Renal replacement therapy | 20 (13.8%) |
| Mechanical circulatory support | 7 (4.9%) |
| Convalascent plasma | 75 (52.1%) |
| Remdesivir | 69 (47.9%) |
| Prophylactic Anticoagulation | Intermediate Dose Anticoagulation | Therapeutic Anticoagulation | None | Total | |
|---|---|---|---|---|---|
| Number of patients | 89 (61.8%) | 8 (5.6%) | 35 (24.3%) | 12 (8.3%) | 144 |
| Thrombotic Complications | 7 | 1 | 9 | 0 | 17 (11.8%) |
| Major Bleeding Complications | 6 | 1 | 8 | 4 | 19 (13.2%) |
| Death | 36 (54.6%) | 6 (9.1%) | 17 (25.8%) | 7 (12%) | 66 (45.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jayakrishnan, T.; Haag, A.; Mealy, S.; Minich, C.; Attah, A.; Turk, M.; Alrifai, N.; Alhuneafat, L.; Khoury, F.; Nasrullah, A.; et al. Novel Coronavirus Infection (COVID-19) Related Thrombotic and Bleeding Complications in Critically Ill Patients: Experience from an Academic Medical Center. J. Clin. Med. 2021, 10, 5652. https://doi.org/10.3390/jcm10235652
Jayakrishnan T, Haag A, Mealy S, Minich C, Attah A, Turk M, Alrifai N, Alhuneafat L, Khoury F, Nasrullah A, et al. Novel Coronavirus Infection (COVID-19) Related Thrombotic and Bleeding Complications in Critically Ill Patients: Experience from an Academic Medical Center. Journal of Clinical Medicine. 2021; 10(23):5652. https://doi.org/10.3390/jcm10235652
Chicago/Turabian StyleJayakrishnan, Thejus, Aaron Haag, Shane Mealy, Corbyn Minich, Abraham Attah, Michael Turk, Nada Alrifai, Laith Alhuneafat, Fadi Khoury, Adeel Nasrullah, and et al. 2021. "Novel Coronavirus Infection (COVID-19) Related Thrombotic and Bleeding Complications in Critically Ill Patients: Experience from an Academic Medical Center" Journal of Clinical Medicine 10, no. 23: 5652. https://doi.org/10.3390/jcm10235652
APA StyleJayakrishnan, T., Haag, A., Mealy, S., Minich, C., Attah, A., Turk, M., Alrifai, N., Alhuneafat, L., Khoury, F., Nasrullah, A., Wedgeworth, P., Mosley, M., Vashistha, K., Bakalov, V., Chaturvedi, A., & Sangli, S. (2021). Novel Coronavirus Infection (COVID-19) Related Thrombotic and Bleeding Complications in Critically Ill Patients: Experience from an Academic Medical Center. Journal of Clinical Medicine, 10(23), 5652. https://doi.org/10.3390/jcm10235652