
Incidence and Radiological Risk Factors of Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis Following Pedicle Screw Instrumentation with Rod Derotation and Direct Vertebral Rotation: A Minimum 5-Year Follow-Up Study

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mika, A.P.; Mesfin, A.; Rubery, P.T.; Molinari, R.; Kebaish, K.M.; Menga, E.N. Proximal Junctional Kyphosis: A Pediatric and Adult Spinal Deformity Surgery Dilemma. JBJS Rev. 2019, 7, e4. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.K.; Kim, Y.J.; Lenke, L.G. Proximal Junctional Kyphosis Following Spinal Deformity Surgery in the Pediatric Patient. J. Am. Acad. Orthop. Surg. 2015, 23, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Hollenbeck, S.M.; Glattes, R.C.; Asher, M.A.; Lai, S.M.; Burton, D.C. The prevalence of increased proximal junctional flexion following posterior instrumentation and arthrodesis for adolescent idiopathic scoliosis. Spine 2008, 33, 1675–1681. [Google Scholar] [CrossRef]
- Helgeson, M.D.; Shah, S.A.; Newton, P.O.; Clements, D.H., 3rd; Betz, R.R.; Marks, M.C.; Bastrom, T. Evaluation of proximal junctional kyphosis in adolescent idiopathic scoliosis following pedicle screw, hook, or hybrid instrumentation. Spine 2010, 35, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.C.; Castelein, R.M.; Chu, W.C.; Danielsson, A.J.; Dobbs, M.B.; Grivas, T.B.; Gurnett, C.A.; Luk, K.D.; Moreau, A.; Newton, P.O.; et al. Adolescent idiopathic scoliosis. Nat. Rev. Dis. Primers 2015, 1, 15030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, S.L.; Dolan, L.A.; Cheng, J.C.; Danielsson, A.; Morcuende, J.A. Adolescent idiopathic scoliosis. Lancet 2008, 371, 1527–1537. [Google Scholar] [CrossRef] [Green Version]
- Suk, S.I.; Kim, J.H.; Kim, S.S.; Lim, D.J. Pedicle screw instrumentation in adolescent idiopathic scoliosis (AIS). Eur. Spine J. 2012, 21, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Suk, S.I. Pedicle screw instrumentation for adolescent idiopathic scoliosis: The insertion technique, the fusion levels and direct vertebral rotation. Clin. Orthop. Surg. 2011, 3, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Luo, M.; Li, N.; Shen, M.; Xia, L. Pedicle screw versus hybrid instrumentation in adolescent idiopathic scoliosis: A systematic review and meta-analysis with emphasis on complications and reoperations. Medicine 2017, 96, e7337. [Google Scholar] [CrossRef]
- Lee, G.A.; Betz, R.R.; Clements, D.H., 3rd; Huss, G.K. Proximal kyphosis after posterior spinal fusion in patients with idiopathic scoliosis. Spine 1999, 24, 795–799. [Google Scholar] [CrossRef]
- Kim, Y.J.; Lenke, L.G.; Bridwell, K.H.; Kim, J.; Cho, S.K.; Cheh, G.; Yoon, J. Proximal junctional kyphosis in adolescent idiopathic scoliosis after 3 different types of posterior segmental spinal instrumentation and fusions: Incidence and risk factor analysis of 410 cases. Spine 2007, 32, 2731–2738. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhao, Y.; Shen, B.; Wang, C.; Li, M. Risk factor analysis of proximal junctional kyphosis after posterior fusion in patients with idiopathic scoliosis. Injury 2010, 41, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Qiu, G.; Zhao, Y.; Guo, S.; Wang, Y.; Zhang, J.; Shen, J. Risk factors of proximal junctional angle increase after selective posterior thoracolumbar/lumbar fusion in patients with adolescent idiopathic scoliosis. Eur. Spine J. 2015, 24, 290–297. [Google Scholar] [CrossRef]
- Lonner, B.S.; Ren, Y.; Newton, P.O.; Shah, S.A.; Samdani, A.F.; Shufflebarger, H.L.; Asghar, J.; Sponseller, P.; Betz, R.R.; Yaszay, B. Risk Factors of Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis-The Pelvis and Other Considerations. Spine Deform. 2017, 5, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Yagi, M.; Nyugen, J.; Cunningham, M.E.; Boachie-Adjei, O. Combined anterior-posterior surgery is the most important risk factor for developing proximal junctional kyphosis in idiopathic scoliosis. Clin. Orthop. Relat. Res. 2012, 470, 1633–1639. [Google Scholar] [CrossRef] [Green Version]
- Alzakri, A.; Vergari, C.; Van den Abbeele, M.; Gille, O.; Skalli, W.; Obeid, I. Global Sagittal Alignment and Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis. Spine Deform. 2019, 7, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.U.; Yang, J.H.; Chang, D.G.; Suk, S.I.; Suh, S.W.; Song, K.S.; Nam, K.Y.; Oh, I.S.; Park, H.Y.; Kim, S.I.; et al. Effect of Direct Vertebral Rotation in Single Thoracic Adolescent Idiopathic Scoliosis: Better 3-Dimensional Deformity Correction. World Neurosurg. 2019, 129, e401–e408. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Suk, S.I.; Chung, E.R. Direct vertebral rotation: A new technique of three-dimensional deformity correction with segmental pedicle screw fixation in adolescent idiopathic scoliosis. Spine 2004, 29, 343–349. [Google Scholar] [CrossRef]
- Kim, Y.J.; Bridwell, K.H.; Lenke, L.G.; Kim, J.; Cho, S.K. Proximal junctional kyphosis in adolescent idiopathic scoliosis following segmental posterior spinal instrumentation and fusion: Minimum 5-year follow-up. Spine 2005, 30, 2045–2050. [Google Scholar] [CrossRef]
- Ilharreborde, B. Sagittal balance and idiopathic scoliosis: Does final sagittal alignment influence outcomes, degeneration rate or failure rate? Eur. Spine J. 2018, 27, 48–58. [Google Scholar] [CrossRef]
- Zhao, J.; Yang, M.; Yang, Y.; Chen, Z.; Li, M. Proximal junctional kyphosis following correction surgery in the Lenke 5 adolescent idiopathic scoliosis patient. J. Orthop. Sci. 2018, 23, 744–749. [Google Scholar] [CrossRef] [PubMed]
- Balikci, T.; Kiyak, G.; Heydar, A.M.; Bawaneh, M.K.; Bezer, M. Mid-length pedicle screw in posterior instrumentation of scoliosis. Asian Spine J. 2019, 13, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Yang, J.H.; Chang, D.-G.; Suk, S.-I.; Suh, S.W.; Nam, Y.; Kim, S.-I.; Song, K.-S. Long-Term Influence of Paraspinal Muscle Quantity in Adolescent Idiopathic Scoliosis Following Deformity Correction by Posterior Approach. J. Clin. Med. 2021, 10, 4790. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.G.; Suk, S.I.; Kim, J.H.; Song, K.S.; Suh, S.W.; Kim, S.Y.; Kim, G.U.; Yang, J.H.; Lee, J.H. Long-term Outcome of Selective Thoracic Fusion Using Rod Derotation and Direct Vertebral Rotation in the Treatment of Thoracic Adolescent Idiopathic Scoliosis: More Than 10-Year Follow-up Data. Clin. Spine Surg. 2020, 33, E50–E57. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Yang, J.H.; Chang, D.G.; Suk, S.I.; Suh, S.W.; Kim, S.I.; Song, K.S.; Park, J.B.; Cho, W. Proximal Junctional Kyphosis in Adult Spinal Deformity: Definition, Classification, Risk Factors, and Prevention Strategies. Asian Spine J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Moradi, V.; Babaee, T.; Shariat, A.; Khosravi, M.; Saeedi, M.; Parent-Nichols, J.; Cleland, J.A. Predictive Factors for Outcomes of Overcorrection Nighttime Bracing in Adolescent Idiopathic Scoliosis: A Systematic Review. Asian Spine J. 2021. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Non-PJK (N = 62) | PJK (N = 7) | p Value |
|---|---|---|---|
| Age (years) | 14.2 ± 2.2 | 13.9 ± 0.9 | 0.890 |
| Follow-up (years) | 9.4 ± 2.8 | 8.3 ± 3.5 | 0.329 |
| Risser stage | 2.6 ± 1.5 | 2.1 ± 1.8 | 0.503 |
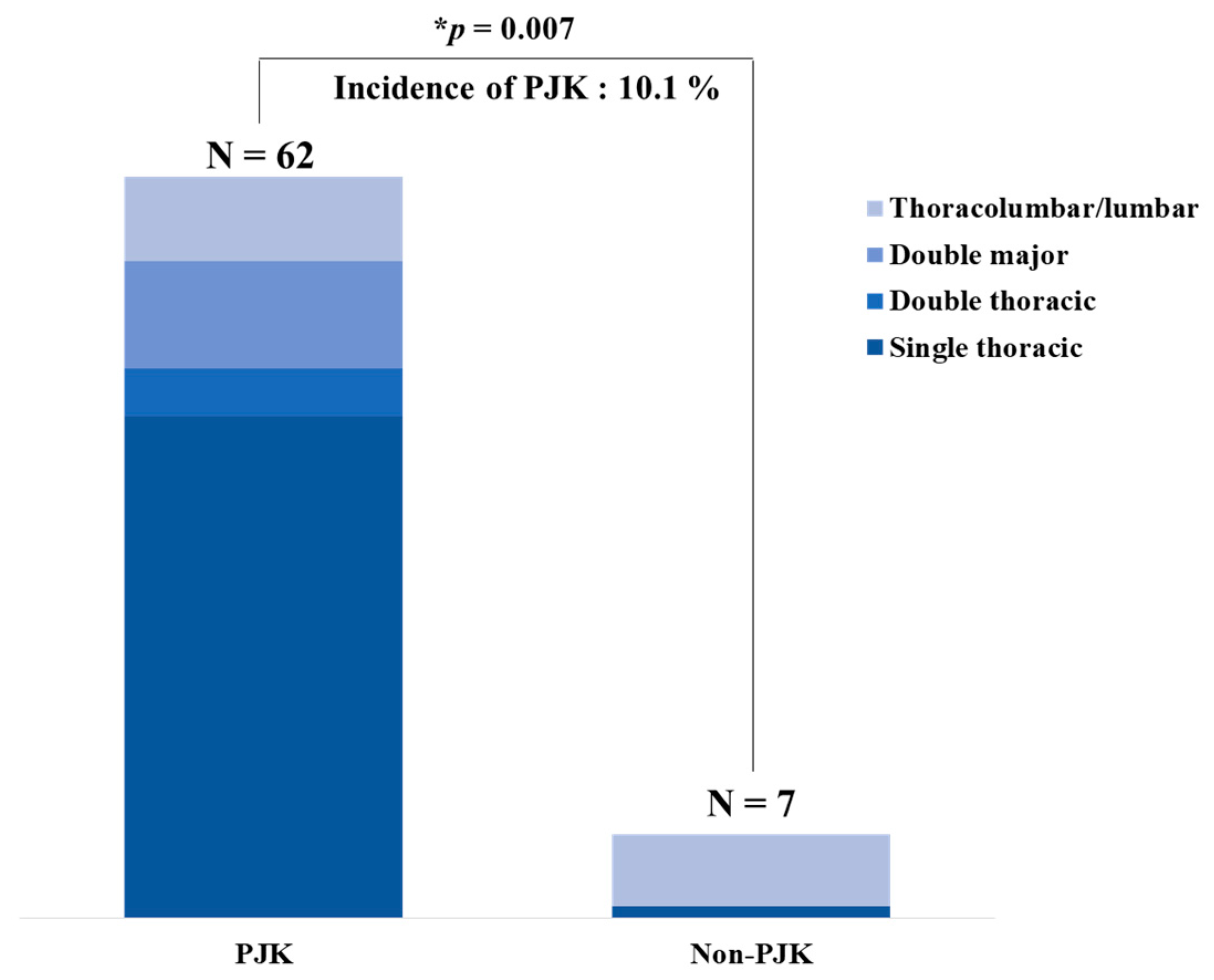
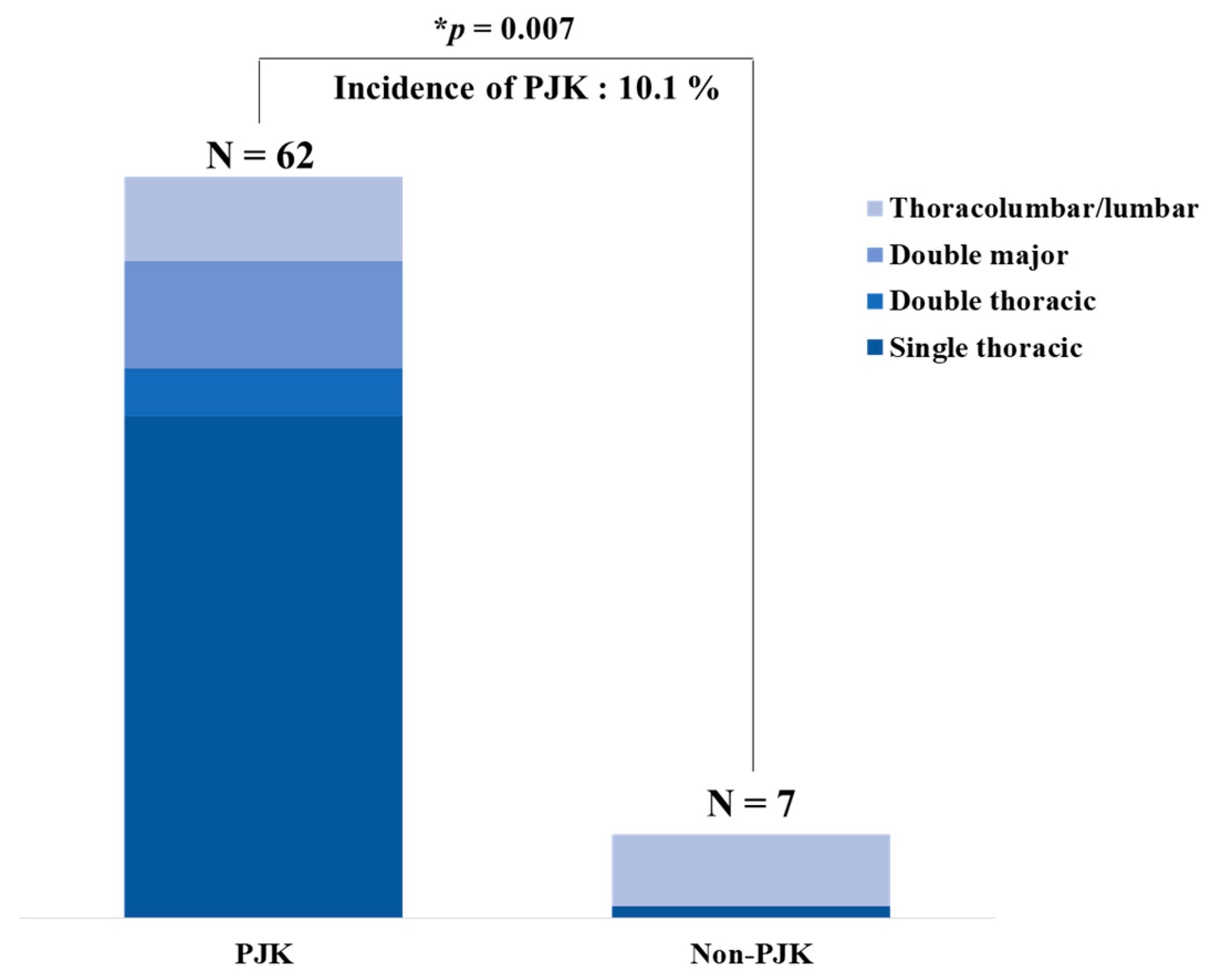
| Suk classification Single thoracic Double thoracic Double major Thoracolumbar/lumbar | 42 4 9 7 | 1 0 0 6 | 0.007 † |
| Lenke classifciation Type I Type II Type IIIType IV Type V Type VI | 41 2 1 4 6 8 | 2 0 0 0 5 0 | 0.015 † |
| Fusion segments | 11.4 ± 1.9 | 11.5 ± 2.4 | 0.020 |
| Operative time (min) | 222.1 ± 69.6 | 188.6 ± 50.1 | 0.116 |
| Estimated blood loss (mL) | 2093.0 ± 1314.8 | 1400.0 ± 838.6 | 0.078 |
| Thoracoplasty (number of patients) | 46 | 3 | 0.085 |
| Number of resected ribs | 6.2 ± 1.0 | 6.0 ± 1.0 | 0.747 |
| Variable | Non-PJK (N = 62) | PJK (N = 7) | p Value |
|---|---|---|---|
| Main thoracic curve (°) | |||
| Preoperative | 50.2 ± 13.6 | 47.4 ± 13.0 | 0.129 |
| Postoperative | 11.9 ± 6.9 | 9.2 ± 9.1 | 0.169 |
| Correction angle | 38.4 ± 13.7 | 38.2 ± 7.2 | 0.688 |
| Correction rate (%) | 76.8 ± 11.6 | 82.8 ± 13.5 | 0.202 |
| Last follow-up | 14.1 ± 8.7 | 14.0 ± 10.0 | 0.973 |
| Loss of correction | 2.2 ± 5.9 | 4.8 ± 7.2 | 0.587 |
| Flexibility (%) | 37.2 ± 19.1 | 40.3 ± 20.6 | 0.522 |
| Proximal CC (°) | |||
| Preoperative | 26.0 ± 10.8 | 17.7 ± 5.7 | 0.027 |
| Postoperative | 12.4 ± 6.4 | 4.0 ± 2.6 | 0.001 |
| Correction angle | 13.6 ± 10.5 | 13.7 ± 5.9 | 0.979 |
| Correction rate (%) | 53.6 ± 23.5 | 75.7 ± 15.3 | 0.018 |
| Last follow-up | 16.6 ± 26.7 | 7.0 ± 3.7 | 0.041 |
| Loss of correction | 4.4 ± 25.8 | 1.7 ± 5.2 | 0.688 |
| Distal CC (°) | |||
| Preoperative | 28.5 ± 11.2 | 13.2 ± 10.7 | 0.006 |
| Postoperative | 7.8 ± 6.0 | 8.2 ± 8.1 | 0.926 |
| Correction angle | 20.7 ± 10.3 | 10.7 ± 14.9 | 0.007 |
| Correction rate (%) | 75.8 ± 16.7 | 54.8 ± 28.8 | 0.008 |
| Last follow-up | 9.3 ± 7.8 | 8.4 ± 8.9 | 0.926 |
| Loss of correction | 1.3 ± 7.6 | 1.3 ± 6.9 | 0.735 |
| Variable | Non-PJK (N = 62) | PJK (N = 7) | p Value |
|---|---|---|---|
| UIV tilt (°) | |||
| Preoperative | 14.8 ± 8.5 | 14.5 ± 11.2 | 0.643 |
| Postoperative | 5.9 ± 4.0 * (60.1%) | 5.0 ± 3.2 * (65.5%) | 0.55 |
| Correction angle | 8.9 ± 8.4 (39.9%) | 9.5 ± 8.7 (34.5%) | 0.901 |
| Last follow-up | 6.5 ± 4.3 (56.1%) | 5.3 ± 4.7 (63.4%) | 0.392 |
| Loss of correction | 0.6 ± 3.6 | 0.3 ± 4.1 | 0.443 |
| UIV disc angle (°) | |||
| Preoperative | 3.7 ± 3.0 | 3.3 ± 3.0 | 0.742 |
| Postoperative | 3.2 ± 2.6 (13.5%) | 2.1 ± 1.5 (26.4%) | 0.293 |
| Correction angle | 0.5 ± 3.2 (86.5%) | 1.2 ± 3.3 (63.6%) | 0.817 |
| Last follow-up | 3.9 ± 3.0 (−5.4%) | 3.2 ± 2.1 (3.0%) | 0.605 |
| Loss of correction | 0.7 ± 2.5 | 1.1 ± 2.6 | 0.51 |
| LIV tilt (°) | |||
| Preoperative | 18.2 ± 7.9 | 17.1 ± 10.1 | 0.915 |
| Postoperative | 4.3 ± 4.0 * (76.4%) | 6.4 ± 4.3 (62.6%) | 0.154 |
| Correction angle | 13.9 ± 7.2 (23.6%) | 10.7 ± 10.2 (37.4%) | 0.359 |
| Last follow-up | 5.4 ± 4.2 (70.3%) | 6.7 ± 4.8 (60.8%) | 0.428 |
| Loss of correction | 1.2 ± 4.2 | 0.3 ± 3.1 | 0.438 |
| LIV disc angle (°) | |||
| Preoperative | 6.2 ± 4.9 | 4.6 ± 2.4 | 0.423 |
| Postoperative | 3.0 ± 2.8 * (51.6%) | 3.2 ± 2.7 (30.4%) | 0.769 |
| Correction angle | 3.2 ± 6.0 (48.4%) | 1.5 ± 2.5 (69.6%) | 0.137 |
| Last follow-up | 3.6 ± 3.1 (41.9%) | 3.1 ± 1.7 (32.6%) | 0.831 |
| Loss of correction | 0.6 ± 3.4 | −0.1 ± 3.1 | 0.544 |
| Variable | Non-PJK (N = 62) | PJK (N = 7) | p Value |
|---|---|---|---|
| Coronal balance (mm) | |||
| Preoperative | 12.6 ± 8.5 | 19.1 ± 10.9 | 0.166 |
| Postoperative | 10.7 ± 7.5 | 6.0 ± 5.8 | 0.072 |
| Correction angle | 2.5 ± 9.7 | 7.1 ± 19.3 | 0.199 |
| Last follow-up | 7.0 ± 5.5 | 8.9 ± 3.6 | 0.169 |
| Loss of correction | −3.3 ± 8.6 | −0.4 ± 14.6 | 0.123 |
| Sagittal vertical axis (mm) | |||
| Preoperative | −3.5 ± 28.4 | −20.5 ± 24.1 | 0.127 |
| Postoperative | 5.3 ± 27.3 | 4.2 ± 38.7 | 0.767 |
| Correction angle | 8.9 ± 41.2 | 24.7 ± 54.8 | 0.367 |
| Last follow-up | 5.8 ± 22.5 | −3.8 ± 33.6 | 0.717 |
| Loss of correction | 0.5 ± 37.5 | −8.0 ± 62.3 | 0.345 |
| Thoracic kyphosis (°) | |||
| Preoperative | 16.6 ± 10.4 | 27.2 ± 20.4 | 0.132 |
| Postoperative | 21.4 ± 8.1 * | 25.3 ± 8.4 | 0.225 |
| Correction angle | −4.9 ± 10.1 | 0.9 ± 15.0 | 0.407 |
| Last follow-up | 29.6 ± 32.6 * | 28.2 ± 11.3 | 0.415 |
| Loss of correction | 8.0 ± 33.3 | 3.5 ± 5.8 | 0.908 |
| Lumbar lordosis (°) | |||
| Preoperative | 47.2 ± 12.0 | 55.3 ± 14.2 | 0.166 |
| Postoperative | 46.2 ± 12.7 | 49.6 ± 12.0 | 0.563 |
| Correction angle | 1.1 ± 11.9 | 3.7 ± 13.9 | 0.748 |
| Last follow-up | 55.0 ± 11.7 | 58.9 ± 15.2 | 0.555 |
| Loss of correction | 9.1 ± 11.6 | 7.1 ± 14.1 | 0.515 |
| Pelvic tilt (°) | |||
| Preoperative | 15.8 ± 2.6 | 13.5 ± 6.0 | 0.373 |
| Postoperative | 18.1 ± 5.4 | 17.1 ± 8.0 | 0.887 |
| Last follow-up | 14.5 ± 5.2 | 16.8 ± 7.9 | 0.522 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.J.; Yang, J.H.; Chang, D.-G.; Suk, S.-I.; Suh, S.W.; Kim, J.S.; Kim, S.-I.; Song, K.-S.; Cho, W. Incidence and Radiological Risk Factors of Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis Following Pedicle Screw Instrumentation with Rod Derotation and Direct Vertebral Rotation: A Minimum 5-Year Follow-Up Study. J. Clin. Med. 2021, 10, 5351. https://doi.org/10.3390/jcm10225351
Kim HJ, Yang JH, Chang D-G, Suk S-I, Suh SW, Kim JS, Kim S-I, Song K-S, Cho W. Incidence and Radiological Risk Factors of Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis Following Pedicle Screw Instrumentation with Rod Derotation and Direct Vertebral Rotation: A Minimum 5-Year Follow-Up Study. Journal of Clinical Medicine. 2021; 10(22):5351. https://doi.org/10.3390/jcm10225351
Chicago/Turabian StyleKim, Hong Jin, Jae Hyuk Yang, Dong-Gune Chang, Se-Il Suk, Seung Woo Suh, Ji Su Kim, Sang-Il Kim, Kwang-Sup Song, and Woojin Cho. 2021. "Incidence and Radiological Risk Factors of Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis Following Pedicle Screw Instrumentation with Rod Derotation and Direct Vertebral Rotation: A Minimum 5-Year Follow-Up Study" Journal of Clinical Medicine 10, no. 22: 5351. https://doi.org/10.3390/jcm10225351
APA StyleKim, H. J., Yang, J. H., Chang, D.-G., Suk, S.-I., Suh, S. W., Kim, J. S., Kim, S.-I., Song, K.-S., & Cho, W. (2021). Incidence and Radiological Risk Factors of Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis Following Pedicle Screw Instrumentation with Rod Derotation and Direct Vertebral Rotation: A Minimum 5-Year Follow-Up Study. Journal of Clinical Medicine, 10(22), 5351. https://doi.org/10.3390/jcm10225351