
A Clot Waveform Analysis Showing a Hypercoagulable State in Patients with Malignant Neoplasms


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
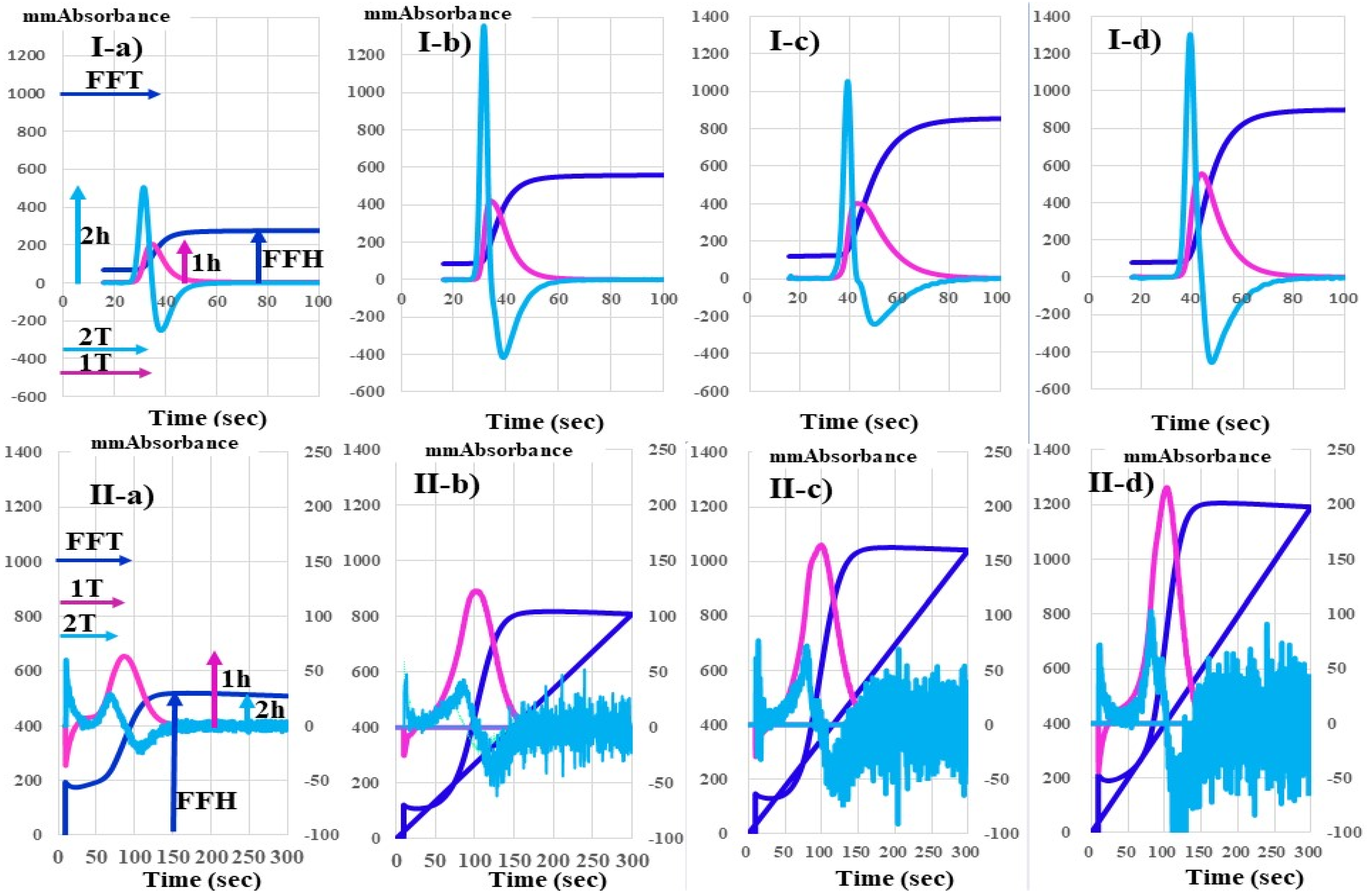
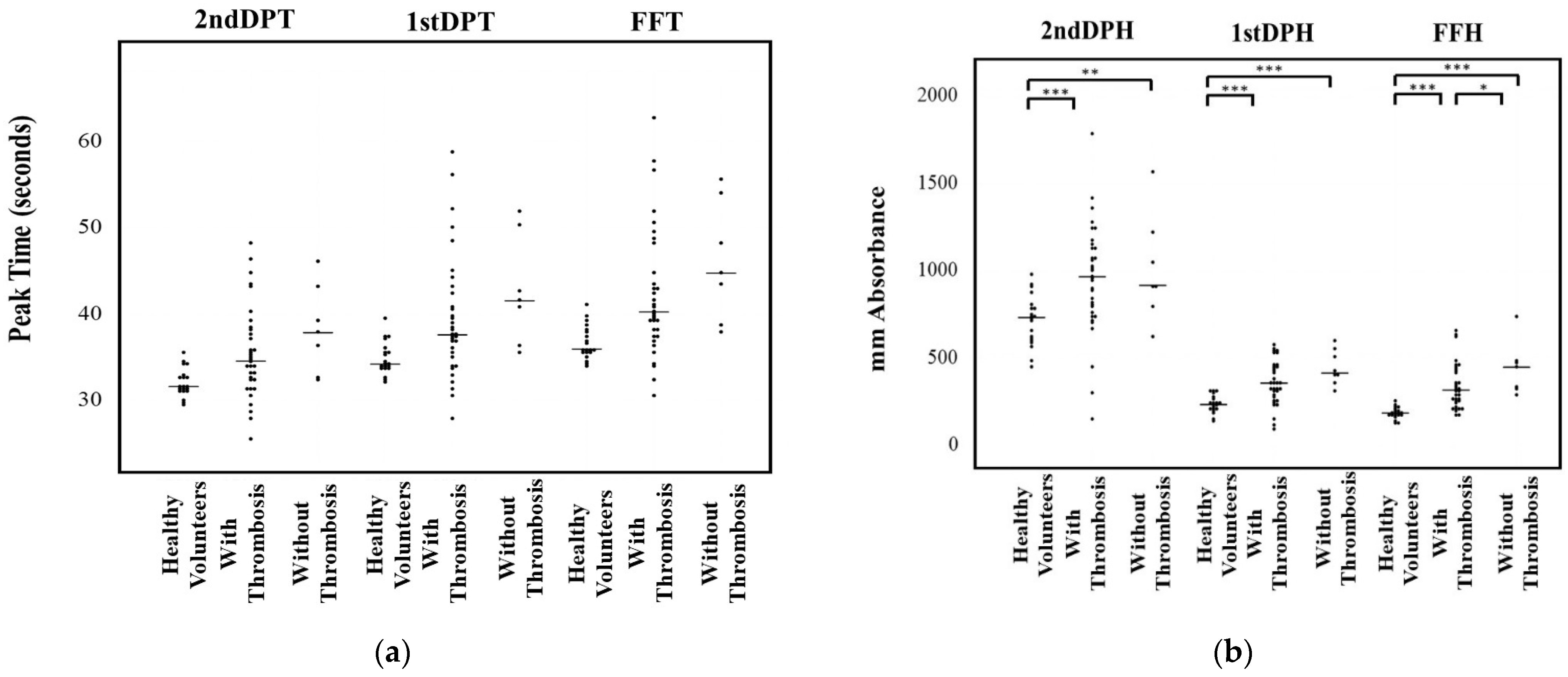
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hisada, Y.; Mackman, N. Cancer-associated pathways and biomarkers of venous thrombosis. Blood 2017, 130, 1499–1506. [Google Scholar] [CrossRef]
- Mahajan, A.; Brunson, A.; White, R.; Wun, T. The Epidemiology of Cancer-Associated Venous Thromboembolism: An Update. Semin. Thromb. Hemost. 2019, 45, 321–325. [Google Scholar] [CrossRef]
- Fernandes, C.J.; Morinaga, L.T.K.; Alves, J.L., Jr.; Castro, M.A.; Calderaro, D.; Jardim, C.V.P.; Souza, R. Cancer-associated thrombosis: The when, how and why. Eur. Respir. Rev. 2019, 28, 180119. [Google Scholar] [CrossRef] [Green Version]
- Kim, A.S.; Khorana, A.A.; McCrae, K.R. Mechanisms and biomarkers of cancer-associated thrombosis. Transl. Res. 2020, 225, 33–53. [Google Scholar] [CrossRef]
- Timp, J.F.; Braekkan, S.K.; Versteeg, H.H.; Cannegieter, S.C. Epidemiology of cancer-associated venous thrombosis. Blood 2013, 122, 1712–1723. [Google Scholar] [CrossRef] [Green Version]
- Varki, A. Trousseau’s syndrome: Multiple definitions and multiple mechanisms. Blood 2007, 110, 1723–1729. [Google Scholar] [CrossRef]
- Trousseau, A. Plegmasia alba dolens. In Lectures on Clinical Medicine; Hotel-Dieu: Paris, France, 1865; Volume 5, pp. 281–332. [Google Scholar]
- Sack, G.H.; Levin, J.; Bell, W.R. Trousseau’s syndrome and other manifestations of chronic disseminated coagulopathy in patients with neoplasms: Clinical, pathophysiologic, and therapeutic features. Medicine 1977, 56, 1–37. [Google Scholar] [CrossRef] [PubMed]
- Bao, L.; Zhang, S.; Gong, X.; Cui, G. Trousseau Syndrome Related Cerebral Infarction: Clinical Manifestations, Laboratory Findings and Radiological Features. J. Stroke Cereb. Dis. 2020, 29, 104891. [Google Scholar] [CrossRef] [PubMed]
- Winter, P.C. The pathogenesis of venous thromboembolism in cancer: Emerging links with tumour biology. Hematol. Oncol. 2006, 24, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A. Malignancy, thrombosis and Trousseau: The case for an eponym. J. Thromb. Haemost. 2003, 1, 2463–2465. [Google Scholar] [CrossRef]
- Sharma, B.K.; Flick, M.J.; Palumbo, J.S. Cancer-Associated Thrombosis: A Two-Way Street. Semin. Thromb. Hemost. 2019, 45, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Suzuki-Inoue, K. Platelets and cancer-associated thrombosis: Focusing on the platelet activation receptor CLEC-2 and podoplanin. Blood 2019, 134, 1912–1918. [Google Scholar] [CrossRef]
- Maestre, A.; Trujillo-Santos, J.; Visoná, A.; Lobo, J.L.; Grau, E.; Malý, R.; Duce, R.; Monreal, M.; RIETE Investigators. D-dimer levels and 90-day outcome in patients with acute pulmonary embolism with or without cancer. Thromb. Res. 2014, 133, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Gerotziafas, G.T.; Mahé, I.; Lefkou, E.; AboElnazar, E.; Abdel-Razeq, H.; Taher, A.; Antic, D.; Elalamy, I.; Syrigos, K.; Van Dreden, P. Overview of risk assessment models for venous thromboembolism in ambulatory patients with cancer. Thromb. Res. 2020, 191, S50–S57. [Google Scholar] [CrossRef]
- Wada, H.; Matsumoto, T.; Ohishi, K.; Shiraki, K.; Shimaoka, M. Update on the Clot Waveform Analysis. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620912027. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Tone, S.; Wada, H.; Naito, Y.; Matsumoto, T.; Yamashita, Y.; Shimaoka, M.; Sudo, A. The evaluation of hemostatic abnormalities using a CWA-small amount tissue factor induced FIX activation assay in major orthopedic surgery patients. Clin. Appl. Thromb. Hemost. 2021, 27, 1076029620976913. [Google Scholar] [CrossRef]
- Wada, H.; Shiraki, K.; Matsumoto, T.; Ohishi, K.; Shimpo, H.; Shimaoka, M. Effects of platelet and phospholipids on clot formation activated by a small amount of tissue factor. Thromb. Res. 2020, 193, 146–153. [Google Scholar] [CrossRef]
- Kobayashi, N.; Maegawa, T.; Takada, M.; Tanaka, H.; Gonmori, H. Criteria for diagnosis of DIC based on the analysis of clinical and laboratory findings in 345 DIC patients collected by the Research Committee on DIC in Japan. Bibl. Haemotol. 1983, 49, 265–275. [Google Scholar]
- Matsumoto, T.; Wada, H.; Fujimoto, N.; Toyoda, J.; Abe, Y.; Ohishi, K.; Yamashita, Y.; Ikejiri, M.; Hasegawa, K.; Suzuki, K.; et al. An Evaluation of the Activated Partial Thromboplastin Time Waveform. Clin. Appl. Thromb. Hemost. 2018, 24, 764–770. [Google Scholar] [CrossRef]
- Falanga, A.; Marchetti, M.; Russo, L. Hemostatic Biomarkers and cancer prognosis: Where Do We Stand? Semin. Thromb. Hemost. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Rak, J.; Milsom, C.; May, L.; Klement, P.; Yu, J. Tissue factor in cancer and angiogenesis: The molecular link between genetic tumor progression, tumor neovascularization, and cancer coagulopathy. Semin. Thromb. Hemost. 2006, 32, 54–70. [Google Scholar] [CrossRef]
- Gordon, S.G.; Cross, B.A. A factor X-activating cysteine protease from malignant tissue. J. Clin. Investig. 1981, 67, 1665–1671. [Google Scholar] [CrossRef] [PubMed]
- Denko, N.C.; Giaccia, A.J. Tumor hypoxia, the physiological link between Trousseau’s syndrome (carcinoma-induced coagulopathy) and metastasis. Cancer Res. 2001, 61, 795–798. [Google Scholar] [PubMed]
- Wahrenbrock, M.; Borsig, L.; Le, D.; Varki, N.; Varki, A. Selectin-mucin interactions as a probable molecular explanation for the association of Trousseau syndrome with mucinous adenocarcinomas. J. Clin. Investig. 2003, 112, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Boccaccio, C.; Sabatino, G.; Medico, E.; Girolami, F.; Follenzi, A.; Reato, G.; Sottile, A.; Naldini, L.; Comoglio, P. The MET oncogene drives a genetic programme linking cancer to haemostasis. Nature 2005, 434, 396–400. [Google Scholar] [CrossRef]
- Hwang, I.G.; Choi, J.H.; Park, S.H.; Oh, S.Y.; Kwon, H.C.; Lee, S.I.; Lim, D.H.; Lee, G.W.; Kang, J.H. Chemotherapy in advanced gastric cancer patients associated with disseminated intravascular coagulation. Cancer Res. Treat. 2014, 46, 27–32. [Google Scholar] [CrossRef]
- Wada, H.; Matsumoto, T.; Yamashita, Y.; Hatada, T. Disseminated Intravascular Coagulation: Testing and Diagnosis. Clin. Chim. Acta 2014, 436C, 130–134. [Google Scholar] [CrossRef]
- Rimassa, L.; Personeni, N.; Czauderna, C.; Foerster, F.; Galle, P. Systemic treatment of HCC in special populations. J. Hepatol. 2021, 74, 931–943. [Google Scholar] [CrossRef]
- Khan, A.R.; Wei, X.; Xu, X. Portal Vein Tumor Thrombosis and Hepatocellular Carcinoma—The Changing Tides. J. Hepatocell. Carcinoma 2021, 8, 1089–1115. [Google Scholar] [CrossRef]
- White, R.H.; Chew, H.K.; Zhou, H.; Parikh-Patel, A.; Harris, D.; Harvey, D.; Wun, T. Incidence of venous thromboembolism in the year before the diagnosis of cancer in 528,693 adults. Arch. Intern. Med. 2005, 165, 1782–1787. [Google Scholar] [CrossRef] [Green Version]
- Johnson, E.D.; Schell, J.C.; Rodgers, G.M. The D-dimer assay. Am. J. Hematol. 2019, 94, 833–839. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Disease | N | Age | Male | PAVTE | ACI | ACS | DIC | TMA | Mortality |
|---|---|---|---|---|---|---|---|---|---|
| Hepatocellular carcinoma * | 23 | 73.4 ± 6.9 | 18 | 3 | 2 | 1 | 0 | 0 | 0 (0%) |
| Colon cancer * | 4 | 74.8 ± 11.2 | 3 | 1 | 0 | 0 | 0 | 0 | 0 (0%) |
| Stomach cancer #,&,+ | 8 | 76.6 ± 9.6 | 8 | 0 | 1 | 0 | 1 | 1 | 3 (37.5%) |
| Prostate cancer # | 5 | 80.4 ± 5.9 | 5 | 1 | 1 | 0 | 0 | 0 | 1 # (20.0%) |
| Biliary tract cancer & | 7 | 79.3 ± 6.4 | 3 | 1 | 0 | 0 | 0 | 0 | 1 (14.3%) |
| Lung cancer + | 6 | 70.3 ± 11.0 | 6 | 0 | 0 | 0 | 0 | 0 | 1 + (16.7%) |
| Pancreatic cancer | 10 | 67.6 ± 10.3 | 7 | 1 | 1 | 0 | 0 | 0 | 2 (20.0%) |
| Esophageal cancer | 4 | 65.8 ± 10.7 | 4 | 0 | 1 | 0 | 0 | 0 | 0 (0%) |
| Malignant lymphoma | 14 | 77.4 ± 6.0 | 8 | 2 | 1 | 2 | 0 | 0 | 1 (7.1%) |
| Myelodysplastic syndrome | 10 | 78.2 ± 11.3 | 4 | 1 | 0 | 0 | 1 | 0 | 0 (0%) |
| Others | 5 | 67.7 ± 9.4 | 2 | 2 | 0 | 1 | 0 | 0 | 0 (0%) |
| Total | 96 | 73.9 ± 9.3 | 68 | 12 | 7 | 4 | 2 | 1 | 9 (9.4%) |
| 2nd DPT | 1st DPT | FFT | 2nd DPH | 1st DPH | FFH | |
|---|---|---|---|---|---|---|
| Cancer Type | Seconds | mm Absorbance | ||||
| Hepatocellular carcinoma | 32.7 (26.8–42.0) | 35.2 (28.9–46.1) | 38.2 (31.1–53.4) | 883 ** (264–1981) | 283 * (139–801) | 250 *** (164–759) |
| Colon cancer | 33.5 (31.2–39.3) | 36.7 (33.8–42.7) | 40.4 (36.2–45.9) | 1235 ** (1024–1452) | 460 ** (330–509) | 387 ** (286–447) |
| Stomach cancer | 34.7 (28.7–38.5) | 37.5 (31.5–42.4) | 40.0 (34.0–49.5) * | 773 (450–1278) | 307 * (147–457) | 279 *** (172–480) |
| Prostate cancer | 34.8 (29.5–60.7) | 37.7 (32.2–65.4) | 39.9 (34.4–67.8) | 810 (647–1220) | 317 ** (254–427) | 296 ** (214–330) |
| Biliary tract cancer | 34.0 * (25.7–48.3) | 37.0 * (28.0–58.8) | 40.6 * (30.5–62.7) | 784 (151–1789) | 315 (90.7–544) | 257 *** (221–621) |
| Lung cancer | 34.0 (29.9–40.3) | 36.6 (32.3–45.1) | 39.5 (34.2–49.5) | 752 (443–1004) | 259 (132–450) | 224 * (178–480) |
| Pancreatic cancer | 35.2 *** (32.6–39.3) | 38.5 *** (36.2–42.8) | 41.4 *** (38.1–48.2) | 973 * (302–1422) | 353 ** (254–559) | 336 *** (172–489) |
| Esophageal cancer | 37.9 (31.4–44.7) | 42.6 (34.1–50.0) | 44.8 * (36.9–51.9) | 1215 ** (972–1572) | 491 ** (418–595) | 448 ** (317–477) |
| malignant lymphoma | 36.1 * (28.0–56.2) | 39.7 * (30.5–60.5) | 43.9 ** (32.5–68.7) | 863 (274–1361) | 311 ** (157–577) | 323 *** (195–634) |
| Myelodysplastic syndrome | 37.5 *** (31.5–78.5) | 40.0 ** (34.1–88.5) | 46.9 ** (35.8–90.3) | 712 (128–1144) | 337 (157–577) | 256 *** (182–653) |
| Others | 38.1 (31.1–44.5) | 43.3 * (33.8–52.1) | 44.9 * (35.8–55.6) | 845 (596–1246) | 328 (187–552) | 319 (163–738) |
| Healthy volunteers | 31.7 (29.6–35.7) | 34.3 (32.1–39.7) | 36.0 (34.0–41.1) | 734 (453–975) | 235 (137–316) | 187 (131–256) |
| 2nd DPT | 1st DPT | FFT | 2nd DPH | 1st DPH | FFH | |
|---|---|---|---|---|---|---|
| Cancer Type | Seconds | mm Absorbance | ||||
| Hepatocellular carcinoma | 77.9 (52.2–105) | 95.6 (76.4–130) | 95.9 (78.2–127) | 48.0 (21.0–108) | 97.9 *** (49.9–270) | 352 (205–938) |
| Colon cancer | 83.2 (76.6–97.6) | 101.5 (92.8–133) | 102 (87.2–134) | 68.9 (28.6–111) | 139 ** (110–193) | 543 * (334–639) |
| Stomach cancer | 82.2 (63.9–148) | 97.0 (81.9–207) | 97.2 (82.4–196) | 46.3 (11.4–102) | 106 * (28.3–178) | 370 (156–564) |
| Prostate cancer | 72.7 (38.6–93.9) | 91.8 (62.3–105) | 89.6 (65.6–93.9) | 46.4 (36.9–95.0) | 80.9 * (64.8–178) | 455 (257–934) |
| Biliary tract cancer | 83.0 (46.3–148) | 103 (79.3–207) | 102 (83.1–196) | 70.5 (13.8–109) | 111 (28.3–250) | 364 (184–702) |
| Lung cancer | 72.6 (66.6–115) | 82.6 (76.4–146) | 84.9 (78.0–152) | 49.1 (26.6–84.1) | 92.0 (46.1–181) * | 314 (183–645) |
| Pancreatic cancer | 80.9 (70.6–102) | 102 (91.2–133) | 103 (88.7–132) | 36.0 (19.0–72.6) | 121 (46.2–165) ** | 411 (163–602) * |
| Esophageal cancer | 74.8 (73.6–85.0) | 98.7 (90.9–113) | 98.9 (89.9–115) | 69.8 (43.5–112) * | 173 (123–213) ** | 600 (464–645) ** |
| malignant lymphoma | 76.1 (50.0–147) | 93.1 (72.0–178) | 92.0 (74.9–174) | 45.6 (17.3–173) | 101 (62.5–304) *** | 437 (246–751) ** |
| Myelodysplastic syndrome | 90.5 (52.2–189) | 113 (60.2–237) | 111 (61.2–225) | 58.6 (9.8–69.8) | 91.4 (33.6–222) | 329 (265–734) |
| Others | 106 (73.6–132) * | 129 (84.8–171) | 126 (84.2–169) | 38.9 (15.1–47.7) | 69.6 (36.4–189) | 406 (285–832) |
| Healthy volunteers | 76.9 (62.5–106) | 95.3 (76.7–140) | 94.6 (80.3–139) | 37.4 (21.2–60.9) | 67.8 (37.2–88.3) | 341 (221–495) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobayashi, M.; Wada, H.; Fukui, S.; Mizutani, H.; Ichikawa, Y.; Shiraki, K.; Moritani, I.; Inoue, H.; Shimaoka, M.; Shimpo, H. A Clot Waveform Analysis Showing a Hypercoagulable State in Patients with Malignant Neoplasms. J. Clin. Med. 2021, 10, 5352. https://doi.org/10.3390/jcm10225352
Kobayashi M, Wada H, Fukui S, Mizutani H, Ichikawa Y, Shiraki K, Moritani I, Inoue H, Shimaoka M, Shimpo H. A Clot Waveform Analysis Showing a Hypercoagulable State in Patients with Malignant Neoplasms. Journal of Clinical Medicine. 2021; 10(22):5352. https://doi.org/10.3390/jcm10225352
Chicago/Turabian StyleKobayashi, Mayu, Hideo Wada, Shunsuke Fukui, Hiroki Mizutani, Yuhuko Ichikawa, Katsuya Shiraki, Isao Moritani, Hidekazu Inoue, Motomu Shimaoka, and Hideto Shimpo. 2021. "A Clot Waveform Analysis Showing a Hypercoagulable State in Patients with Malignant Neoplasms" Journal of Clinical Medicine 10, no. 22: 5352. https://doi.org/10.3390/jcm10225352
APA StyleKobayashi, M., Wada, H., Fukui, S., Mizutani, H., Ichikawa, Y., Shiraki, K., Moritani, I., Inoue, H., Shimaoka, M., & Shimpo, H. (2021). A Clot Waveform Analysis Showing a Hypercoagulable State in Patients with Malignant Neoplasms. Journal of Clinical Medicine, 10(22), 5352. https://doi.org/10.3390/jcm10225352