
Comparison of Simultaneous Single-Position Oblique Lumbar Interbody Fusion and Percutaneous Pedicle Screw Fixation with Posterior Lumbar Interbody Fusion Using O-arm Navigated Technique for Lumbar Degenerative Diseases

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Surgical Settings and Procedures for Single-Position OLIF
2.2. Surgical Settings and Procedures for MI-PLIF/TLIF
2.3. Clinical Evaluation
2.4. Surgical Evaluation
2.5. Radiographic Evaluation
2.6. Statistical Analysis
3. Results
3.1. Clinical Evaluation
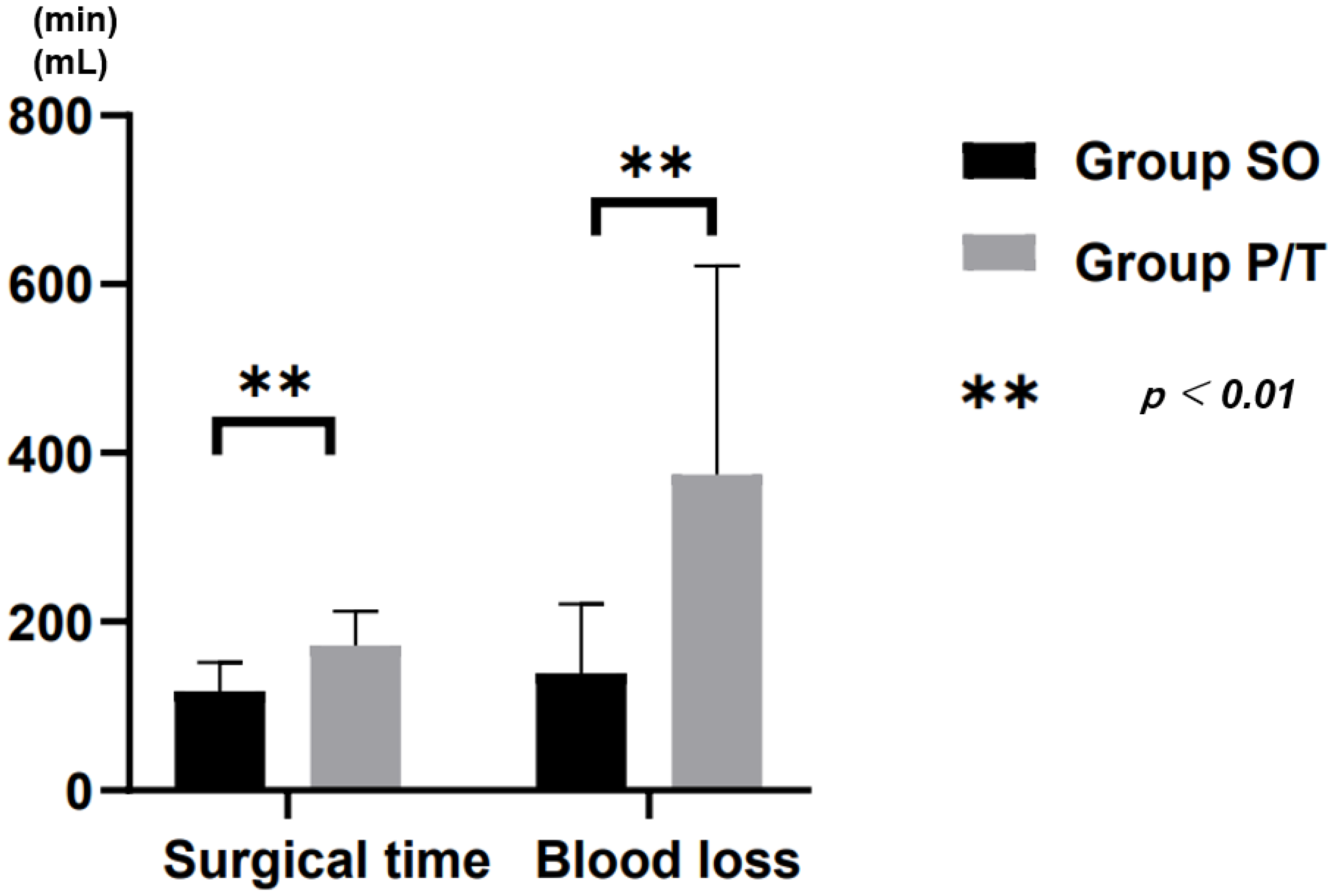
3.2. Surgical Evaluation
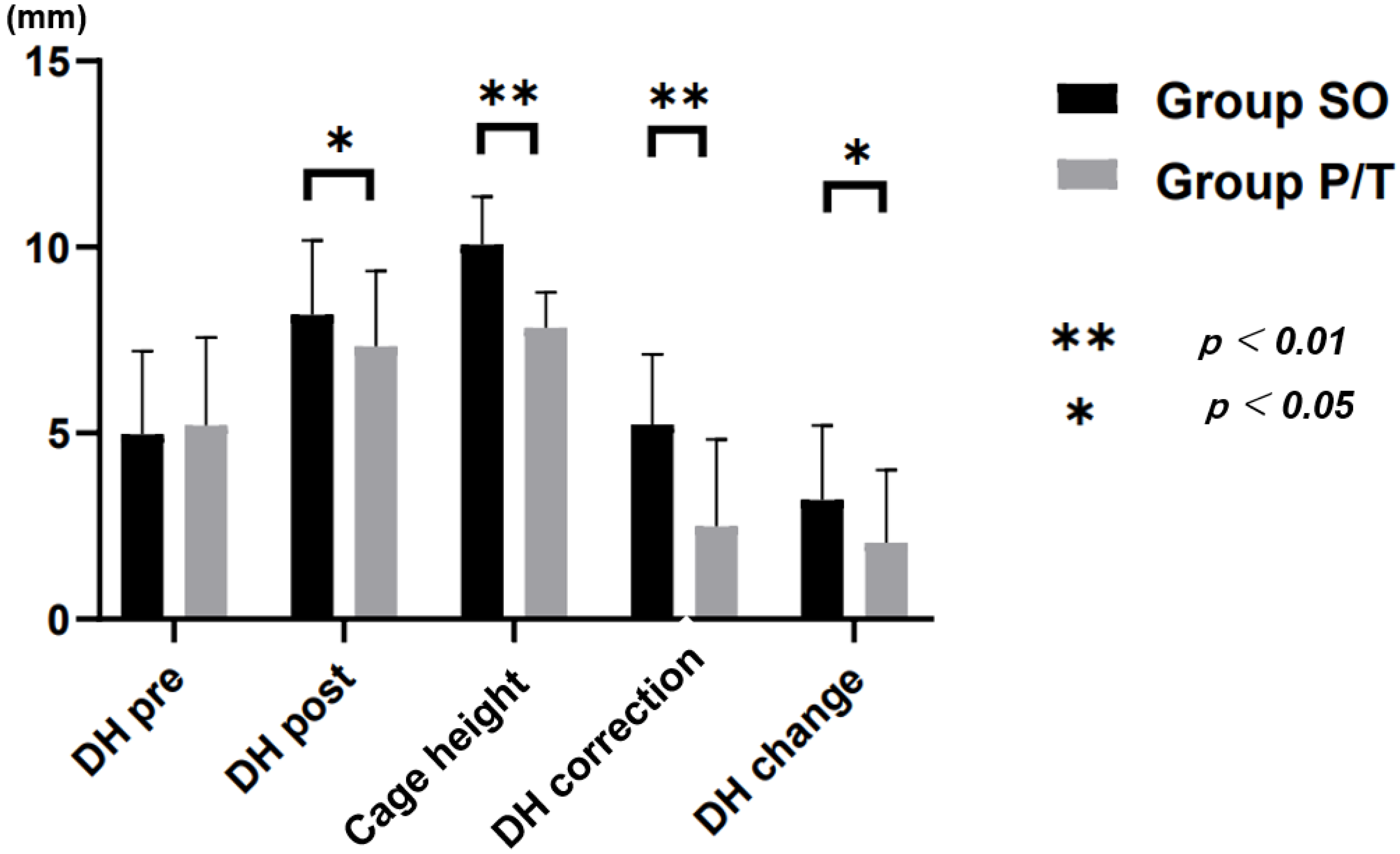
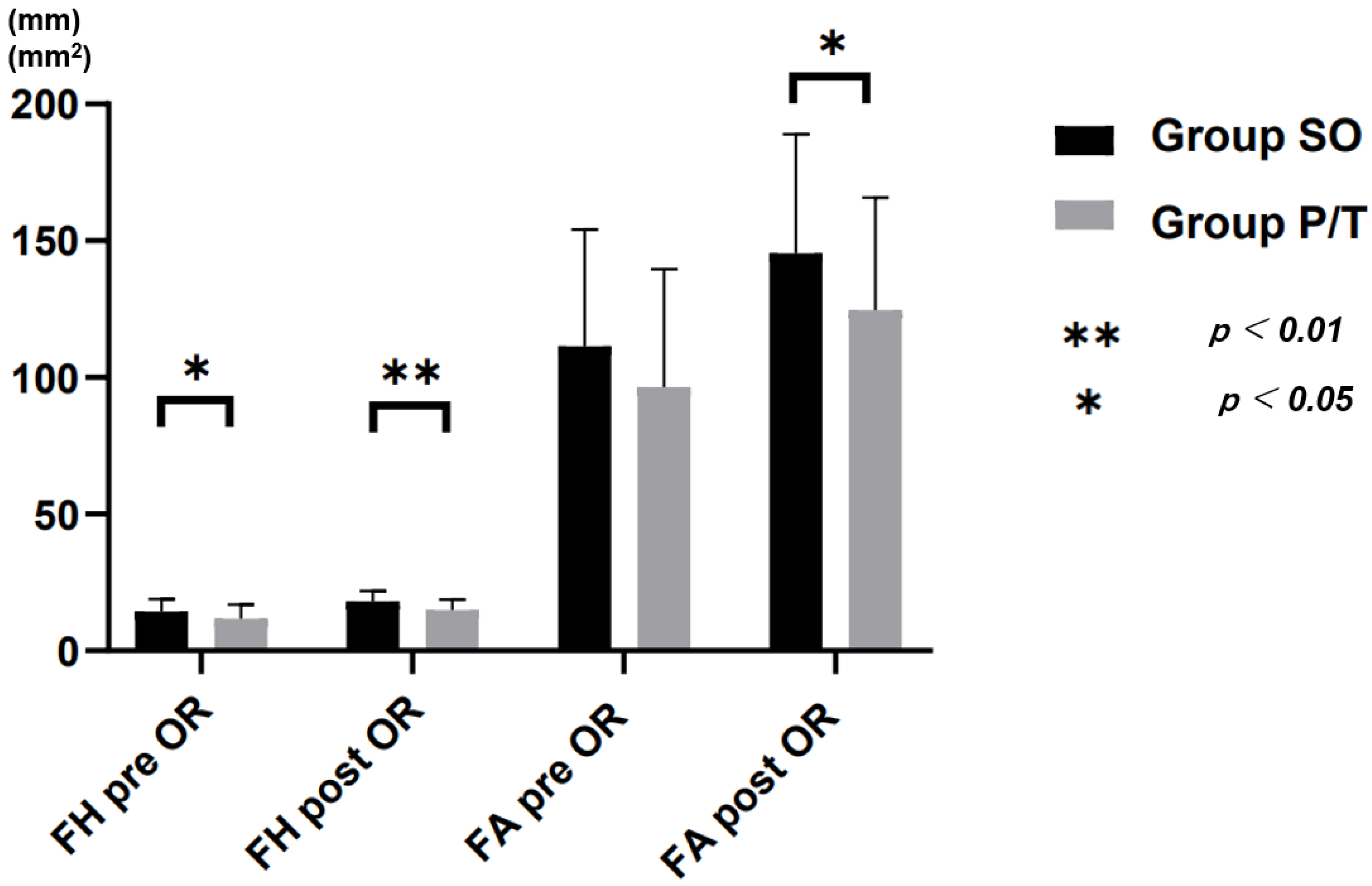
3.3. Radiographic Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mobbs, R.J.; Phan, K.; Malham, G.; Seex, K.; Rao, P.J. Lumbar interbody fusion: Techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J. Spine Surg. 2015, 1, 2–18. [Google Scholar] [PubMed]
- Okuda, S.; Miyauchi, A.; Oda, T.; Haku, T.; Yamamoto, T.; Iwasaki, M. Surgical complications of posterior lumbar interbody fusion with total facetectomy in 251 patients. J. Neurosurg. Spine 2006, 4, 304–309. [Google Scholar] [CrossRef]
- Foley, K.T.; Holly, L.T.; Schwender, J.D. Minimally Invasive Lumbar Fusion. Spine 2003, 28, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Mayer, M. A new microsurgical technique for minimally invasive anterior lumbar interbody fusion. Spine 1997, 22, 691–699. [Google Scholar] [CrossRef]
- Wu, M.; Li, J.; Zhang, M.; Zhang, M.; Ding, X.; Qi, D.; Li, G.; Shen, Y. Efficacy and radiographic analysis of oblique lumbar interbody fusion for degenerative lumbar spondylolisthesis. J. Orthop. Surg. Res. 2019, 14, 399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, G.X.; Akbary, K.; Kotheeranurak, V. Clinical and Radiologic Outcomes of Direct Versus Indirect Decompression with Lumbar Interbody Fusion: A Matched-Pair Comparison Analysis. World Neurosurg. 2018, 119, 898–909. [Google Scholar] [CrossRef]
- Drazin, D.; Kim, T.T.; Johnson, J.P. Simultaneous Lateral Interbody Fusion and Posterior Percutaneous Instrumentation: Early Experience and Technical Considerations. Biomed. Res. Int. 2015, 2015, 458284. [Google Scholar] [CrossRef] [Green Version]
- Uotani, K.; Yasuyuki, S.; Yoshihira, S.; Tanaka, M. LLIF and Percutaneous Pedicle Screw Fixation Performed All in Lateral Position with O-arm. JCS Med. Assoc. 2017, 29, 39–42. (In Japanese) [Google Scholar]
- Tanaka, M.; Ruparel, S.; Fujiwara, Y.; Uotani, K.; Yamauchi, T. Simultaneous Oblique Lumbar Interbody Fusion (OLIF) and Lateral Percutaneous Pedicle Screw Fixation (Lateral PPS): A Technical Note. Res. Arthritis Bone Stud. 2019, 1, 1–8. [Google Scholar]
- Fairbank, J.C.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2952. [Google Scholar] [CrossRef] [PubMed]
- Poppenborg, P.; Liljenqvist, U.; Gosheger, G.; Boevingloh, A.S.; Lampe, L.; Schmeil, S.; Schulte, T.L.; Lange, T. Complications in TLIF spondylodesis—do they influence the outcome for patients? A prospective two-center study. Eur. Spine J. 2021, 30, 1320–1328. [Google Scholar] [CrossRef]
- Kepler, C.K.; Sharma, A.K.; Huang, R.C. Indirect foraminal decompression after lateral transpsoas interbody fusion: Clinical article. J. Neurosurg. Spine 2012, 16, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Pawar, A.Y.; Hughes, A.P.; Sama, A.A.; Girardi, F.P.; Lebl, D.R.; Cammisa, F.P. A comparative study of lateral lumbar interbody fusion and posterior lumbar interbody fusion in degenerative lumbar spondylolisthesis. Asian Spine J. 2015, 9, 668–674. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, M.; Fujiwara, Y.; Uotani, K.; Yamauchi, T. C-ArmeFree Circumferential Minimally Invasive Surgery for Adult Spinal Deformity: Technical Note. World Neurosurg. 2020, 143, 235–246. [Google Scholar] [CrossRef] [PubMed]
- Ozgur, B.M.; Aryan, H.E.; Pimenta, L.; Taylor, W.R. Extreme Lateral Interbody Fusion (XLIF): A novel surgical technique for anterior lumbar interbody fusion. Spine 2006, 6, 435–443. [Google Scholar] [CrossRef]
- Epstein, N.E. Review of Risks and Complications of Extreme Lateral Interbody Fusion (XLIF). Surg. Neurol. Int. 2019, 10, 237. [Google Scholar] [CrossRef] [PubMed]
- Li, H.M.; Zhang, R.J.; Shen, C.L. Radiographic and Clinical Outcomes of Oblique Lateral Interbody Fusion versus Minimally Invasive Transforaminal Lumbar Interbody Fusion for Degenerative Lumbar Disease. World Neurosurg. 2019, 122, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Ouchida, J.; Kanemura, T.; Satake, K.; Nakashima, H.; Ishikawa, Y.; Imagama, S. Simultaneous single-position lateral interbody fusion and percutaneous pedicle screw fixation using O-arm-based navigation reduces the occupancy time of the operating room. Eur. Spine J. 2020, 29, 1277–1286. [Google Scholar] [CrossRef]
- Li, H.M.; Zhang, R.J.; Shen, C.L. Differences in radiographic and clinical outcomes of oblique lateral interbody fusion and lateral lumbar interbody fusion for degenerative lumbar disease: A meta-analysis. BMC Musculoskelet. Disord. 2019, 20, 582. [Google Scholar] [CrossRef]
- Rodgers, W.B.; Gerber, E.J.; Patterson, J. Intraoperative and Early Postoperative Complications in Extreme Lateral Interbody Fusion an Analysis of 600 Cases. Spine 2011, 36, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Khajavi, K.; Shen, A.; Lagina, M.; Hutchison, A. Comparison of clinical outcomes following minimally invasive lateral interbody fusion stratified by preoperative diagnosis. Eur. Spine J. 2015, 24, 322–330. [Google Scholar] [CrossRef]
- Wang, T.Y.; Nayar, G.; Brown, C.R.; Pimenta, L.; Karikari, I.O.; Isaacs, R.E. Bony Lateral Recess Stenosis and Other Radiographic Predictors of Failed Indirect Decompression via Extreme Lateral Interbody Fusion: Multi-Institutional Analysis of 101 Consecutive Spinal Levels. World Neurosurg. 2017, 106, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Prod’Homme, M.; Sans-Merce, M.; Pitteloud, N.; Damet, J.; Lascombes, P. Intraoperative 2D C-arm and 3D O-arm in children: A comparative phantom study. J. Child. Orthop. 2018, 12, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.P.G.; Robertson, P.A.; Lunt, B.; Phys, M.; Jackson, S.A. Radiation Exposure during Fluoroscopically Assisted Pedicle Screw Insertion in the Lumbar Spine. Spine 2000, 25, 1538–1541. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group SO | Group P/T | p-Value | |
|---|---|---|---|
| Number of patients | 63 | 35 | |
| Age (years) | 68.6 ± 10.4 | 71.0 ± 13.5 | 0.802 |
| Gender | |||
| Male | 20 | 15 | |
| Female | 43 | 20 | |
| BMI (kg/m2) | 23.6 ± 4.7 | 22.9 ± 2.9 | 0.552 |
| Disorder | |||
| Spondylolisthesis | 49 | 28 | |
| Lumbar stenosis | 11 | 5 | |
| Degenerative Disc Disease | 3 | 2 | |
| Fused level of vertebra | |||
| L2/3 | 1 | 2 | |
| L3/4 | 10 | 4 | |
| L4/5 | 51 | 22 | |
| L5/S1 | 1 | 7 |
| Group SO | Group P/T | p-Value | |
|---|---|---|---|
| Mean Follow up (month) | 23.2 ± 6.9 | 27.9 ± 11.7 | |
| Surgical time (min) | 112.0 ± 32.4 | 171.8 ± 40.6 | <0.001 |
| Blood loss (ml) | 139.2 ± 82.0 | 374.2± 247.7 | <0.001 |
| Mobilization time (day) | 2.7 ± 1.0 | 3.9 ± 2.4 | 0.002 |
| Cage height (mm) | 10.1 ± 1.3 | 7.8 ± 1.0 | <0.001 |
| DH pre OR (mm) | 5.0 ± 2.2 | 5.2 ± 2.4 | 0.992 |
| FH pre OR (mm) | 14.4 ± 4.5 | 11.7 ± 5.3 | 0.021 |
| FA pre OR (mm2) | 111.4 ± 42.6 | 96.4 ± 43.2 | 0.098 |
| DH correction (mm) | 5.2 ± 1.9 | 2.5 ± 2.3 | <0.001 |
| DH post OR (mm) | 8.2 ± 2.0 | 7.3 ± 2.0 | 0.042 |
| FH post OR (mm) | 18.1 ± 3.7 | 14.9 ± 3.9 | <0.001 |
| FA post OR (mm2) | 145.4 ± 43.5 | 124.6 ± 41.2 | 0.044 |
| DH change (mm) | 3.2 ± 2.0 | 2.1 ± 1.9 | 0.048 |
| Segmental lordosis pre OR (degree) | 10.3 ± 5.9 | 11.5 ± 8.4 | 0.404 |
| Segmental lordosis post OR (degree) | 10.0 ± 6.0 | 12.8 ± 8.1 | 0.201 |
| Group SO | Group P/T | p-Value | |
|---|---|---|---|
| Number of patients | 63 | 35 | |
| VAS of back pain | 5.6 ± 2.4 | 6.0 ± 2.9 | 0.578 |
| ODI | 45.4 ± 17.7 | 55.4 ± 19.7 | 0.142 |
| Complication | 6.3% | 14.1% | 0.191 |
| Neural injury | 2 | 0 | |
| Dural tear | 0 | 2 | |
| SSI | 1 | 0 | |
| Hematoma | 0 | 2 | |
| Reoperation | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, Y.; Tanaka, M.; Sonawane, S.; Uotani, K.; Oda, Y.; Fujiwara, Y.; Arataki, S.; Yamauchi, T.; Takigawa, T.; Ito, Y. Comparison of Simultaneous Single-Position Oblique Lumbar Interbody Fusion and Percutaneous Pedicle Screw Fixation with Posterior Lumbar Interbody Fusion Using O-arm Navigated Technique for Lumbar Degenerative Diseases. J. Clin. Med. 2021, 10, 4938. https://doi.org/10.3390/jcm10214938
Tan Y, Tanaka M, Sonawane S, Uotani K, Oda Y, Fujiwara Y, Arataki S, Yamauchi T, Takigawa T, Ito Y. Comparison of Simultaneous Single-Position Oblique Lumbar Interbody Fusion and Percutaneous Pedicle Screw Fixation with Posterior Lumbar Interbody Fusion Using O-arm Navigated Technique for Lumbar Degenerative Diseases. Journal of Clinical Medicine. 2021; 10(21):4938. https://doi.org/10.3390/jcm10214938
Chicago/Turabian StyleTan, Ying, Masato Tanaka, Sumeet Sonawane, Koji Uotani, Yoshiaki Oda, Yoshihiro Fujiwara, Shinya Arataki, Taro Yamauchi, Tomoyuki Takigawa, and Yasuo Ito. 2021. "Comparison of Simultaneous Single-Position Oblique Lumbar Interbody Fusion and Percutaneous Pedicle Screw Fixation with Posterior Lumbar Interbody Fusion Using O-arm Navigated Technique for Lumbar Degenerative Diseases" Journal of Clinical Medicine 10, no. 21: 4938. https://doi.org/10.3390/jcm10214938
APA StyleTan, Y., Tanaka, M., Sonawane, S., Uotani, K., Oda, Y., Fujiwara, Y., Arataki, S., Yamauchi, T., Takigawa, T., & Ito, Y. (2021). Comparison of Simultaneous Single-Position Oblique Lumbar Interbody Fusion and Percutaneous Pedicle Screw Fixation with Posterior Lumbar Interbody Fusion Using O-arm Navigated Technique for Lumbar Degenerative Diseases. Journal of Clinical Medicine, 10(21), 4938. https://doi.org/10.3390/jcm10214938