
Detection of Human Papillomavirus DNA in Paired Peripheral Blood and Cervix Samples in Patients with Cervical Lesions and Healthy Individuals

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. HPV DNA Cervix and Blood Samples
2.3. Viral Load and Physical Status
2.4. Statistical Analysis
3. Results
3.1. Population
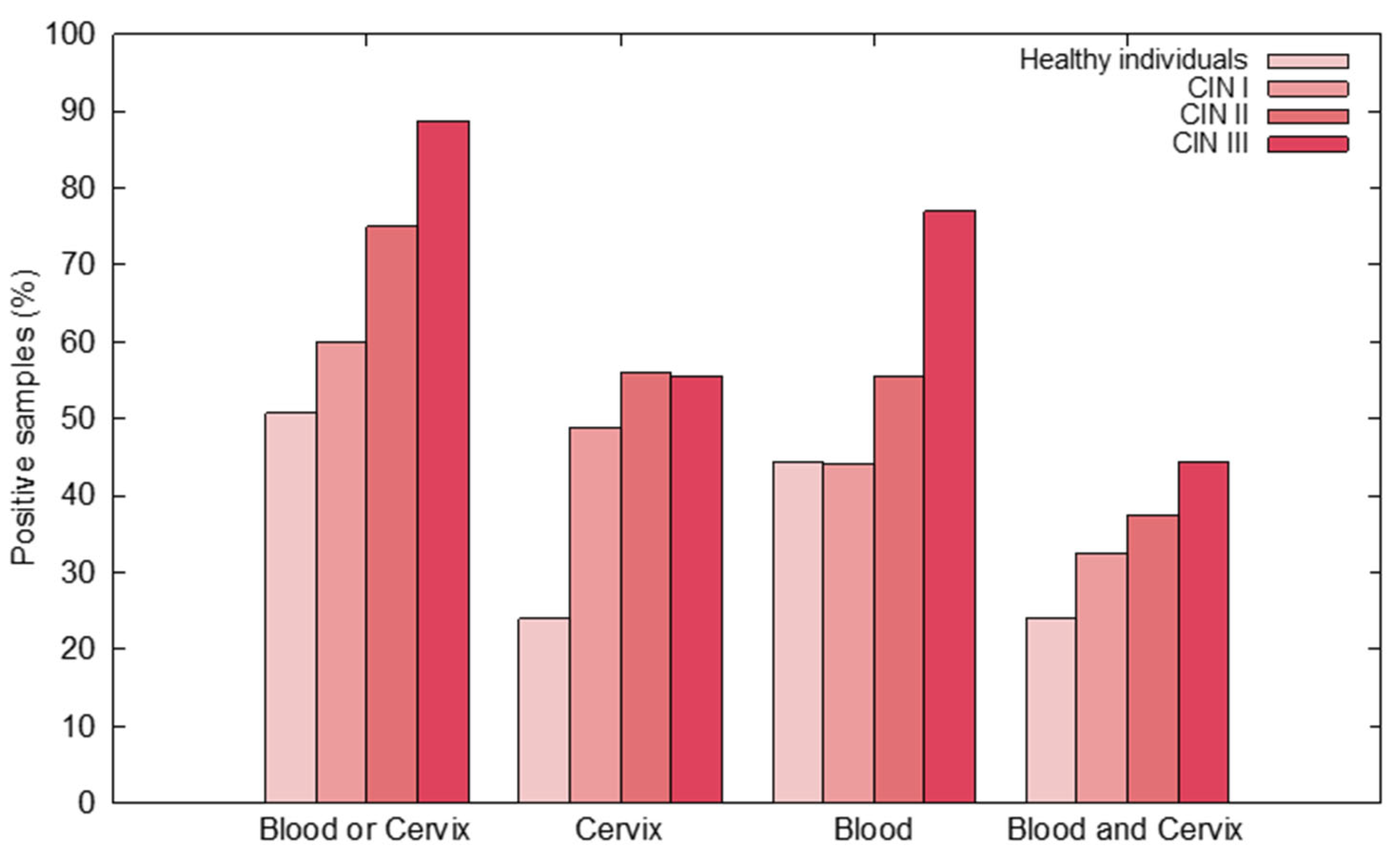
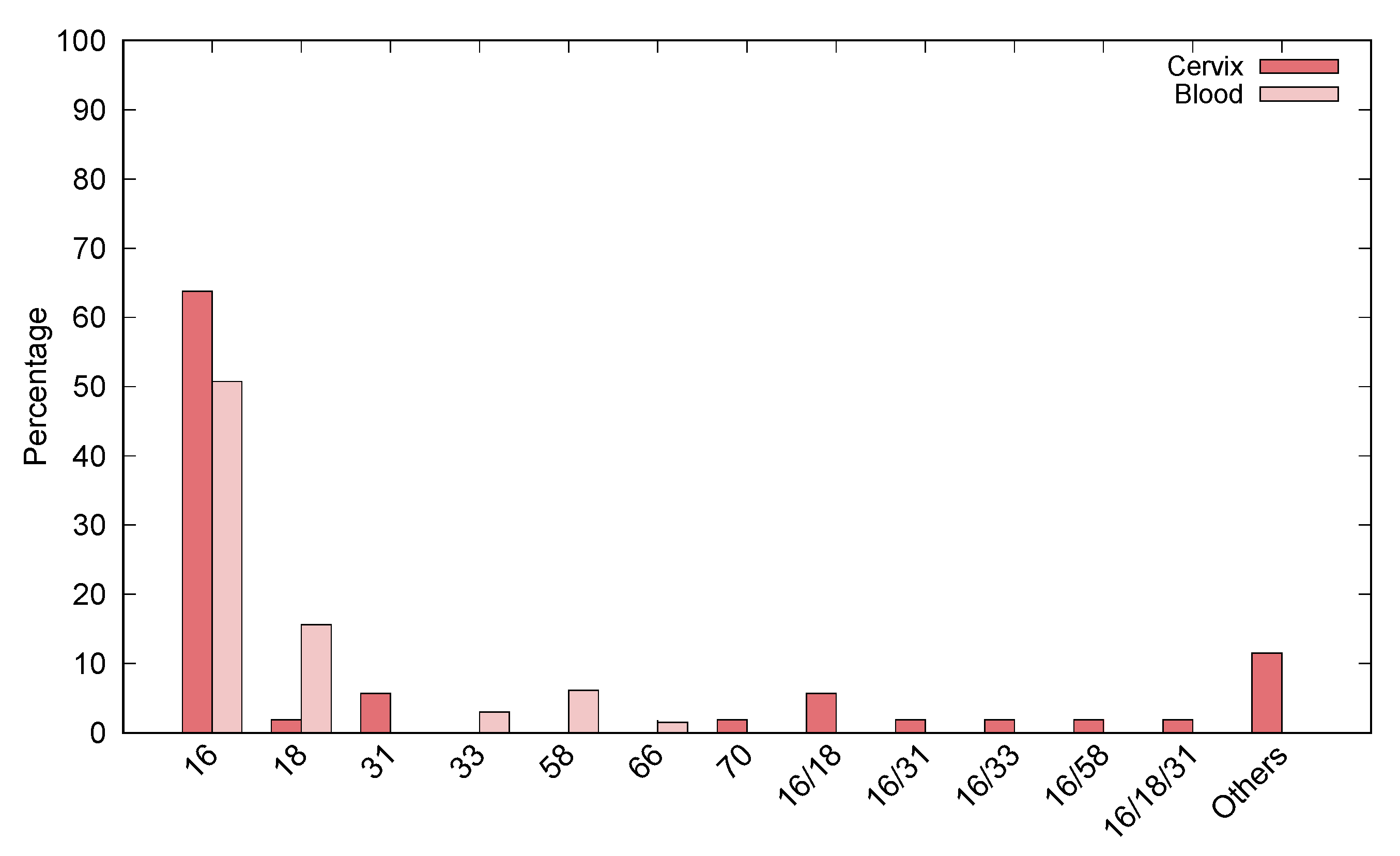
3.2. HPV DNA Detection in Cervix and Blood Samples
3.3. Evaluation of Viral Load in Paired Cervix/Blood Tissues
4. Discussion
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- De Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide Burden of Cancer Attributable to HPV by Site, Country and HPV Type. Int. J. Cancer 2018, 664–670. [Google Scholar] [CrossRef] [PubMed]
- zur Hausen, H. Papillomavirus Infections--a Major Cause of Human Cancers. Biochim. Biophys. Acta 1996, 1288, F55–F78. [Google Scholar] [CrossRef]
- Zur Hausen, H. Papillomaviruses in Human Cancers. Proc. Assoc. Am. Physicians 1999, 111, 581–587. [Google Scholar] [CrossRef] [PubMed]
- zur Hausen, H. Papillomaviruses Causing Cancer: Evasion from Host-Cell Control in Early Events in Carcinogenesis. J. Natl. Cancer Inst. 2000, 92, 690–698. [Google Scholar] [CrossRef]
- zur Hausen, H. Papillomaviruses and Cancer: From Basic Studies to Clinical Application. Nat. Rev. Cancer 2002, 2, 342–350. [Google Scholar] [CrossRef]
- Syrjänen, S. Human Papillomavirus (HPV) in Head and Neck Cancer. J. Clin. Virol. 2005, 32, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Paz, I.B.; Cook, N.; Odom-Maryon, T.; Xie, Y.; Wilczynski, S.P. Human Papillomavirus (HPV) in Head and Neck Cancer. Cancer 1997, 79, 595–604. [Google Scholar] [CrossRef]
- Marur, S.; D’Souza, G.; Westra, W.H.; Forastiere, A.A. HPV-Associated Head and Neck Cancer: A Virus-Related Cancer Epidemic. Lancet Oncol. 2010, 11, 781–789. [Google Scholar] [CrossRef]
- Castellsagué, X.; Alemany, L.; Quer, M.; Halec, G.; Quirós, B.; Tous, S.; Clavero, O.; Alòs, L.; Biegner, T.; Szafarowski, T.; et al. HPV Involvement in Head and Neck Cancers: Comprehensive Assessment of Biomarkers in 3680 Patients. JNCI J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef]
- Gu, Y.; Wan, C.; Qiu, J.; Cui, Y.; Jiang, T.; Zhuang, Z. Circulating HPV CDNA in the Blood as a Reliable Biomarker for Cervical Cancer: A Meta-Analysis. PLoS ONE 2020, 15, e0224001. [Google Scholar] [CrossRef]
- Kang, Z.; Stevanović, S.; Hinrichs, C.S.; Cao, L. Circulating Cell-Free DNA for Metastatic Cervical Cancer Detection, Genotyping, and Monitoring. Clin. Cancer Res. 2017, 23, 6856–6862. [Google Scholar] [CrossRef] [PubMed]
- Campitelli, M.; Jeannot, E.; Peter, M.; Lappartient, E.; Saada, S.; de la Rochefordière, A.; Fourchotte, V.; Alran, S.; Petrow, P.; Cottu, P.; et al. Human Papillomavirus Mutational Insertion: Specific Marker of Circulating Tumor DNA in Cervical Cancer Patients. PLoS ONE 2012, 7, e43393. [Google Scholar] [CrossRef]
- Leung, E.; Han, K.; Zou, J.; Zhao, Z.; Zheng, Y.; Wang, T.T.; Siu, L.L.; Pugh, T.J.; Bratman, S.V. Abstract A45: HPV Sequencing Facilitates Ultrasensitive Detection of HPV Circulating Tumor DNA. Clin. Cancer Res. 2020, 26, A45. [Google Scholar] [CrossRef]
- Bernard-Tessier, A.; Jeannot, E.; Guenat, D.; Debernardi, A.; Michel, M.; Proudhon, C.; Vincent-Salomon, A.; Bièche, I.; Pierga, J.-Y.; Buecher, B.; et al. Clinical Validity of HPV Circulating Tumor DNA in Advanced Anal Carcinoma: An Ancillary Study to the Epitopes-HPV02 Trial. Clin. Cancer Res. 2019, 25, 2109–2115. [Google Scholar] [CrossRef]
- Cabel, L.; Bidard, F.-C.; Servois, V.; Cacheux, W.; Mariani, P.; Romano, E.; Minsat, M.; Bieche, I.; Farkhondeh, F.; Jeannot, E.; et al. HPV Circulating Tumor DNA to Monitor the Efficacy of Anti-PD-1 Therapy in Metastatic Squamous Cell Carcinoma of the Anal Canal: A Case Report. Int. J. Cancer 2017, 141, 1667–1670. [Google Scholar] [CrossRef] [PubMed]
- Carow, K.; Gölitz, M.; Wolf, M.; Häfner, N.; Jansen, L.; Hoyer, H.; Schwarz, E.; Runnebaum, I.B.; Dürst, M. Viral-Cellular DNA Junctions as Molecular Markers for Assessing Intra-Tumor Heterogeneity in Cervical Cancer and for the Detection of Circulating Tumor DNA. Int. J. Mol. Sci. 2017, 18, 2032. [Google Scholar] [CrossRef]
- Kay, P.; Allan, B.; Denny, L.; Hoffman, M.; Williamson, A.-L. Detection of HPV 16 and HPV 18 DNA in the Blood of Patients with Cervical Cancer. J. Med. Virol. 2005, 75, 435–439. [Google Scholar] [CrossRef]
- Tseng, C.J.; Pao, C.C.; Lin, J.D.; Soong, Y.K.; Hong, J.H.; Hsueh, S. Detection of Human Papillomavirus Types 16 and 18 MRNA in Peripheral Blood of Advanced Cervical Cancer Patients and Its Association with Prognosis. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1999, 17, 1391–1396. [Google Scholar] [CrossRef]
- Weismann, P.; Weismanova, E.; Masak, L.; Mlada, K.; Keder, D.; Ferancikova, Z.; Vizvaryova, M.; Konecny, M.; Zavodna, K.; Kausitz, J.; et al. The Detection of Circulating Tumor Cells Expressing E6/E7 HR-HPV Oncogenes in Peripheral Blood in Cervical Cancer Patients after Radical Hysterectomy. Neoplasma 2009, 56, 230–238. [Google Scholar] [CrossRef][Green Version]
- Chiou, H.-L.; Wu, M.-F.; Liaw, Y.-C.; Cheng, Y.-W.; Wong, R.-H.; Chen, C.-Y.; Lee, H. The Presence of Human Papillomavirus Type 16/18 DNA in Blood Circulation May Act as a Risk Marker of Lung Cancer in Taiwan. Cancer 2003, 97, 1558–1563. [Google Scholar] [CrossRef]
- Moustafa, A.; Xie, C.; Kirkness, E.; Biggs, W.; Wong, E.; Turpaz, Y.; Bloom, K.; Delwart, E.; Nelson, K.E.; Venter, J.C.; et al. The Blood DNA Virome in 8000 Humans. PLoS Pathog. 2017, 13, e1006292. [Google Scholar] [CrossRef]
- Bodaghi, S.; Wood, L.V.; Roby, G.; Ryder, C.; Steinberg, S.M.; Zheng, Z.-M. Could Human Papillomaviruses Be Spread through Blood? J. Clin. Microbiol. 2005, 43, 5428–5434. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.C.-H.; Keleher, A.; Kedda, M.-A.; Spurdle, A.B.; McMillan, N.A.J.; Antonsson, A. Human Papillomavirus DNA Detected in Peripheral Blood Samples from Healthy Australian Male Blood Donors. J. Med. Virol. 2009, 81, 1792–1796. [Google Scholar] [CrossRef]
- Foresta, C.; Bertoldo, A.; Garolla, A.; Pizzol, D.; Mason, S.; Lenzi, A.; De Toni, L. Human Papillomavirus Proteins Are Found in Peripheral Blood and Semen Cd20+ and Cd56+ Cells during Hpv-16 Semen Infection. BMC Infect. Dis. 2013, 13, 593. [Google Scholar] [CrossRef]
- Pao, C.C.; Lin, S.S.; Lin, C.Y.; Maa, J.S.; Lai, C.H.; Hsieh, T.T. Identification of Human Papillomavirus DNA Sequences in Peripheral Blood Mononuclear Cells. Am. J. Clin. Pathol. 1991, 95, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Widschwendter, A.; Blassnig, A.; Wiedemair, A.; Müller-Holzner, E.; Müller, H.M.; Marth, C. Human Papillomavirus DNA in Sera of Cervical Cancer Patients as Tumor Marker. Cancer Lett. 2003, 202, 231–239. [Google Scholar] [CrossRef]
- Jeannot, E.; Becette, V.; Campitelli, M.; Calméjane, M.-A.; Lappartient, E.; Ruff, E.; Saada, S.; Holmes, A.; Bellet, D.; Sastre-Garau, X. Circulating Human Papillomavirus DNA Detected Using Droplet Digital PCR in the Serum of Patients Diagnosed with Early Stage Human Papillomavirus-Associated Invasive Carcinoma. J. Pathol. Clin. Res. 2016, 2, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Gnanamony, M.; Peedicayil, A.; Subhashini, J.; Ram, T.S.; Rajasekar, A.; Gravitt, P.; Abraham, P. Detection and Quantitation of HPV 16 and 18 in Plasma of Indian Women with Cervical Cancer. Gynecol. Oncol. 2010, 116, 447–451. [Google Scholar] [CrossRef]
- Sathish, N.; Abraham, P.; Peedicayil, A.; Sridharan, G.; John, S.; Shaji, R.V.; Chandy, G. HPV DNA in Plasma of Patients with Cervical Carcinoma. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2004, 31, 204–209. [Google Scholar] [CrossRef]
- Cocuzza, C.E.; Martinelli, M.; Sina, F.; Piana, A.; Sotgiu, G.; Dell’Anna, T.; Musumeci, R. Human Papillomavirus DNA Detection in Plasma and Cervical Samples of Women with a Recent History of Low Grade or Precancerous Cervical Dysplasia. PLoS ONE 2017, 12, e0188592. [Google Scholar] [CrossRef]
- Pao, C.; Hor, J.J.; Yang, F.; Lin, C.; Tseng, C. Detection of Human Papillomavirus MRNA and Cervical Cancer Cells in Peripheral Blood of Cervical Cancer Patients with Metastasis. J. Clin. Oncol. 1997, 1012. [Google Scholar] [CrossRef]
- Vergara, N.; Balanda, M.; Vidal, D.; Roldán, F.; Martín, H.S.; Ramírez, E. Detection and Quantitation of Human Papillomavirus DNA in Peripheral Blood Mononuclear Cells from Blood Donors. J. Med. Virol. 2019, 91, 2009–2015. [Google Scholar] [CrossRef]
- Peitsaro, P.; Johansson, B.; Syrjänen, S. Integrated Human Papillomavirus Type 16 Is Frequently Found in Cervical Cancer Precursors as Demonstrated by a Novel Quantitative Real-Time PCR Technique. J. Clin. Microbiol. 2002, 40, 886–891. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.M.; Pai, S.I.; Rha, S.-H.; Hildesheim, A.; Kurman, R.J.; Schwartz, P.E.; Mortel, R.; McGowan, L.; Greenberg, M.D.; Barnes, W.A.; et al. Detection and Quantitation of Human Papillomavirus DNA in the Plasma of Patients with Cervical Carcinoma. Cancer Epidemiol. Biomarkers Prev. 2002, 11, 3–6. [Google Scholar]
- Pornthanakasem, W.; Shotelersuk, K.; Termrungruanglert, W.; Voravud, N.; Niruthisard, S.; Mutirangura, A. Human Papillomavirus DNA in Plasma of Patients with Cervical Cancer. BMC Cancer 2001, 1, 2. [Google Scholar] [CrossRef]
- Ho, C.-M.; Yang, S.-S.; Chien, T.-Y.; Huang, S.-H.; Jeng, C.-J.; Chang, S.-F. Detection and Quantitation of Human Papillomavirus Type 16, 18 and 52 DNA in the Peripheral Blood of Cervical Cancer Patients. Gynecol. Oncol. 2005, 99, 615–621. [Google Scholar] [CrossRef]
- Cao, H.; Banh, A.; Kwok, S.; Shi, X.; Wu, S.; Krakow, T.; Khong, B.; Bavan, B.; Bala, R.; Pinsky, B.A.; et al. Quantitation of Human Papillomavirus DNA in Plasma of Oropharyngeal Carcinoma Patients. Int. J. Radiat. Oncol. 2012, 82, e351–e358. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Câncer (INCA). Estimativa 2020: Incidência de Câncer No Brasil. Available online: https://www.inca.gov.br/publicacoes/livros/estimativa-2020-incidencia-de-cancer-no-brasil (accessed on 3 November 2021).
- Capone, R.B.; Pai, S.I.; Koch, W.M.; Gillison, M.L.; Danish, H.N.; Westra, W.H.; Daniel, R.; Shah, K.V.; Sidransky, D. Detection and Quantitation of Human Papillomavirus (HPV) DNA in the Sera of Patients with HPV-Associated Head and Neck Squamous Cell Carcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2000, 6, 4171–4175. [Google Scholar]
- Anayannis, N.V.; Schlecht, N.F.; Ben-Dayan, M.; Smith, R.V.; Belbin, T.J.; Ow, T.J.; Blakaj, D.M.; Burk, R.D.; Leonard, S.M.; Woodman, C.B.; et al. Association of an Intact E2 Gene with Higher HPV Viral Load, Higher Viral Oncogene Expression, and Improved Clinical Outcome in HPV16 Positive Head and Neck Squamous Cell Carcinoma. PLoS ONE 2018, 13, e0191581. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Zeng, X.; Li, W.; Zhu, H.; Wang, G.; Liu, X.; Lv, Y.; Wu, J.; Zhuang, X.; Zhang, J.; et al. Detection and Analysis of Human Papillomavirus (HPV) DNA in Breast Cancer Patients by an Effective Method of HPV Capture. PLoS ONE 2014, 9, e90343. [Google Scholar] [CrossRef]
- Syrjänen, S. Current Concepts on Human Papillomavirus Infections in Children. APMIS 2010, 118, 494–509. [Google Scholar] [CrossRef]
- Münger, K.; Baldwin, A.; Edwards, K.M.; Hayakawa, H.; Nguyen, C.L.; Owens, M.; Grace, M.; Huh, K. Mechanisms of Human Papillomavirus-Induced Oncogenesis. J. Virol. 2004, 78, 11451–11460. [Google Scholar] [CrossRef] [PubMed]
- Keller, L.; Belloum, Y.; Wikman, H.; Pantel, K. Clinical Relevance of Blood-Based CtDNA Analysis: Mutation Detection and Beyond. Br. J. Cancer 2020, 1–14. [Google Scholar] [CrossRef]
- De Freitas, A.C.; de Carvalho, C.; Brunner, O.; Harry Birgel, E., Jr.; Melville Paiva Dellalibera, A.M.; Benesi, F.J.; Gregory, L.; Beçak, W.; de Cassia Stocco dos Santos, R. Viral DNA Sequences in Peripheral Blood and Vertical Transmission of the Virus: A Discussion about BPV-1. Braz. J. Microbiol. 2003, 34, 76–78. [Google Scholar] [CrossRef]
- De Carvalho, C.; de Freitas, A.C.; Brunner, O.; Góes, L.G.B.; Cavalcante, A.Y.; Beçak, W.; de Cassia Stocco dos Santos, R. Bovine Papillomavirus Type 2 in Reproductive Tract and Gametes of Slaughtered Bovine Females. Braz. J. Microbiol. 2003, 34, 82–84. [Google Scholar] [CrossRef]
- Yaguiu, A.; Dagli, M.L.Z.; Birgel, E.H., Jr.; Alves Reis, B.C.A.; Ferraz, O.P.; Pituco, E.M.; Freitas, A.C.; Beçak, W.; Stocco, R.C. Simultaneous Presence of Bovine Papillomavirus and Bovine Leukemia Virus in Different Bovine Tissues: In Situ Hybridization and Cytogenetic Analysis. Genet. Mol. Res. GMR 2008, 7, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.a.R.; De Albuquerque, B.M.F.; Pontes, N.E.; Coutinho, L.C.A.; Leitão, M.C.G.; Reis, M.C.; Castro, R.S.; Freitas, A.C. Detection and Expression of Bovine Papillomavirus in Blood of Healthy and Papillomatosis-Affected Cattle. Genet. Mol. Res. GMR 2013, 12, 3150–3156. [Google Scholar] [CrossRef]
- Brandt, S.; Schoster, A.; Tober, R.; Kainzbauer, C.; Burgstaller, J.P.; Haralambus, R.; Steinborn, R.; Hinterhofer, C.; Stanek, C. Consistent Detection of Bovine Papillomavirus in Lesions, Intact Skin and Peripheral Blood Mononuclear Cells of Horses Affected by Hoof Canker. Equine Vet. J. 2011, 43, 202–209. [Google Scholar] [CrossRef]
- Roperto, S.; Comazzi, S.; Ciusani, E.; Paolini, F.; Borzacchiello, G.; Esposito, I.; Lucà, R.; Russo, V.; Urraro, C.; Venuti, A.; et al. PBMCs Are Additional Sites of Productive Infection of Bovine Papillomavirus Type 2. J. Gen. Virol. 2011, 92, 1787–1794. [Google Scholar] [CrossRef] [PubMed]
- Roperto, S.; Brun, R.; Paolini, F.; Urraro, C.; Russo, V.; Borzacchiello, G.; Pagnini, U.; Raso, C.; Rizzo, C.; Roperto, F.; et al. Detection of Bovine Papillomavirus Type 2 in the Peripheral Blood of Cattle with Urinary Bladder Tumours: Possible Biological Role. J. Gen. Virol. 2008, 89, 3027–3033. [Google Scholar] [CrossRef]
- Roperto, S.; Russo, V.; Leonardi, L.; Martano, M.; Corrado, F.; Riccardi, M.G.; Roperto, F. Bovine Papillomavirus Type 13 Expression in the Urothelial Bladder Tumours of Cattle. Transbound. Emerg. Dis. 2016, 63, 628–634. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sequence (5′3′) | Size (bp) | |
|---|---|---|
| β-globina | 110 bp | |
| PC04 GH20 | ACACAACTGTGTTCACTAGC CAACTTCATCCACGTTCACC | |
| MY09 MY11 | CGTCCMARRGGAWACTGATC GCMCAGGGWCATAAYAATGG | 450 bp |
| GP5 GP6 | TTTGTTACTGTGGTAGATAC GAAAAATAAACTGTAAATCA | 110 bp |
| E6 HPV16 | ||
| Forward | GAGAAACTGCAATGTTTCAGGACC | 81 bp |
| Reverse | TGTATAGTTGTTTGCAGCTCTGTGC | |
| E2 HPV16 | ||
| Forward | AACGAAGTATCCTCTCCTGAAATTATTAG | 76 bp |
| Reverse | CCAAGGCGACGGCTTTG |
| HPV Negative (Cervix) N° (%) | HPV Positive (Cervix) N° (%) | p-Value | OR (IC) | ||
|---|---|---|---|---|---|
| Age | <45 | 53 (38.1%) | 31 (22.3%) | 0.937 | |
| 46–60 | 32 (23.0%) | 20 (14.4%) | |||
| >60 | 2 (1.4%) | 1 (0.7%) | |||
| Total | 87 (62.6%) | 52 (37.4%) | |||
| Residence | Rural | 13 (9.6%) | 5 (3.7%) | 0.382 | |
| Urban | 72 (53.3%) | 45 (33.3%) | |||
| Total | 85 (63.0%) | 50 (37.0%) | |||
| Ethnicity | Black | 15 (10.8%) | 8 (5.8%) | 0.791 | |
| Other | 35 (25.2%) | 24 (17.3%) | |||
| White | 37 (26.6%) | 20 (14.4%) | |||
| Total | 87 (62.6%) | 52 (37.4%) | |||
| Age at the first sexual relation | <20 | 67 (48.2%) | 44 (31.7%) | 0.824 | |
| 20–30 | 17 (12.2%) | 7 (5.0%) | |||
| 30–40 | 2 (1.4%) | 1 (0.7%) | |||
| >40 | 1 (0.7%) | 0 (0.0%) | |||
| Total | 87 (62.6%) | 52 (37.4%) | |||
| Number of pregnancies | 1 | 17 (16.2%) | 8 (7.6%) | 0.209 | |
| 2–3 | 42 (40%) | 15 (14.2%) | |||
| >4 | 11 (10.5%) | 12 (11.4%) | |||
| Total | 70 (66.7%) | 35 (33.3%) | |||
| Contraceptive use | No | 70 (50.4%) | 43 (30.9%) | 0.744 | |
| Yes | 17 (12.2%) | 9 (6.5%) | |||
| Total | 87 (62.6%) | 52 (37.4%) | |||
| Smoking | No | 70 (50.4%) | 42 (30.2%) | 1.00 | |
| Yes | 10 (7.2%) | 6 (4.3%) | |||
| Ex-smoking | 7 (5.0%) | 4 (2.9%) | |||
| Total | 87 (62.6%) | 52 (37.4%) | |||
| Number of sexual partners | 1 | 38 (29.2%) | 28 (21.5%) | 0.779 | |
| 2–3 | 33 (25.5%) | 15 (11.5%) | |||
| >4 | 10 (7.7%) | 6 (8.5%) | |||
| Total | 81 (62.3%) | 49 (37.7%) | |||
| Previous STIs | No | 67 (56.8%) | 30 (25.4%) | 0.023 * | 2.978 (1.134–7.821) |
| Yes | 9 (7.6%) | 12 (10.2%) | |||
| Total | 76 (64.4%) | 42 (35.6%) | |||
| HPV in blood | No | 60 (43.2%) | 11 (7.9%) | 0.000 * | 8.283 (3.700–18.540) |
| Yes | 27 (19.4%) | 41 (29.5%) | |||
| Total | 87 (62.6%) | 52 (37.4%) | |||
| CINI/II or III | Without lesion | 54 (38.8%) | 17 (12.2%) | 0.007 * | |
| CIN I | 22 (15.8%) | 21 (15.1%) | |||
| CIN II | 7 (5.0%) | 9 (6.5%) | |||
| CIN III | 4 (2.9%) | 5 (3.6%) | |||
| Total | 87 (62.6%) | 52 (37.4%) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conceição Gomes Nascimento, K.; Gonçalves Lima, É.; Mota Nunes, Z.; Rêgo Barros Júnior, M.; de Aragão Batista, M.V.; Lucena Araujo, A.R.; da Costa Silva Neto, J.; Simas Chagas, B.; Almeida Diniz Gurgel, A.P.; de Freitas, A.C. Detection of Human Papillomavirus DNA in Paired Peripheral Blood and Cervix Samples in Patients with Cervical Lesions and Healthy Individuals. J. Clin. Med. 2021, 10, 5209. https://doi.org/10.3390/jcm10215209
Conceição Gomes Nascimento K, Gonçalves Lima É, Mota Nunes Z, Rêgo Barros Júnior M, de Aragão Batista MV, Lucena Araujo AR, da Costa Silva Neto J, Simas Chagas B, Almeida Diniz Gurgel AP, de Freitas AC. Detection of Human Papillomavirus DNA in Paired Peripheral Blood and Cervix Samples in Patients with Cervical Lesions and Healthy Individuals. Journal of Clinical Medicine. 2021; 10(21):5209. https://doi.org/10.3390/jcm10215209
Chicago/Turabian StyleConceição Gomes Nascimento, Kamylla, Élyda Gonçalves Lima, Zhilbelly Mota Nunes, Marconi Rêgo Barros Júnior, Marcus Vinícius de Aragão Batista, Antonio Roberto Lucena Araujo, Jacinto da Costa Silva Neto, Bárbara Simas Chagas, Ana Pavla Almeida Diniz Gurgel, and Antonio Carlos de Freitas. 2021. "Detection of Human Papillomavirus DNA in Paired Peripheral Blood and Cervix Samples in Patients with Cervical Lesions and Healthy Individuals" Journal of Clinical Medicine 10, no. 21: 5209. https://doi.org/10.3390/jcm10215209
APA StyleConceição Gomes Nascimento, K., Gonçalves Lima, É., Mota Nunes, Z., Rêgo Barros Júnior, M., de Aragão Batista, M. V., Lucena Araujo, A. R., da Costa Silva Neto, J., Simas Chagas, B., Almeida Diniz Gurgel, A. P., & de Freitas, A. C. (2021). Detection of Human Papillomavirus DNA in Paired Peripheral Blood and Cervix Samples in Patients with Cervical Lesions and Healthy Individuals. Journal of Clinical Medicine, 10(21), 5209. https://doi.org/10.3390/jcm10215209