
Frequency of Early Intervention Sessions and Vocabulary Skills in Children with Hearing Loss

 , ,
, ,
Abstract
1. Introduction
1.1. Amount of Intervention and Developmental Outcomes
1.2. The Current Study
2. Materials and Methods
2.1. Participants
2.1.1. Characteristics of Participants’ Hearing Loss
2.1.2. Frequency of Participants’ Intervention
2.2. Procedures
2.2.1. Data Collection Instruments
2.2.2. Administration of Expressive Vocabulary Assessment
2.2.3. Scoring of Expressive Vocabulary Assessment
2.3. Data Analysis: Structural Equation Model
2.4. Research Questions
3. Results
3.1. Preliminary Analyses: Skew and Kurtosis
3.2. Descriptive Statistics
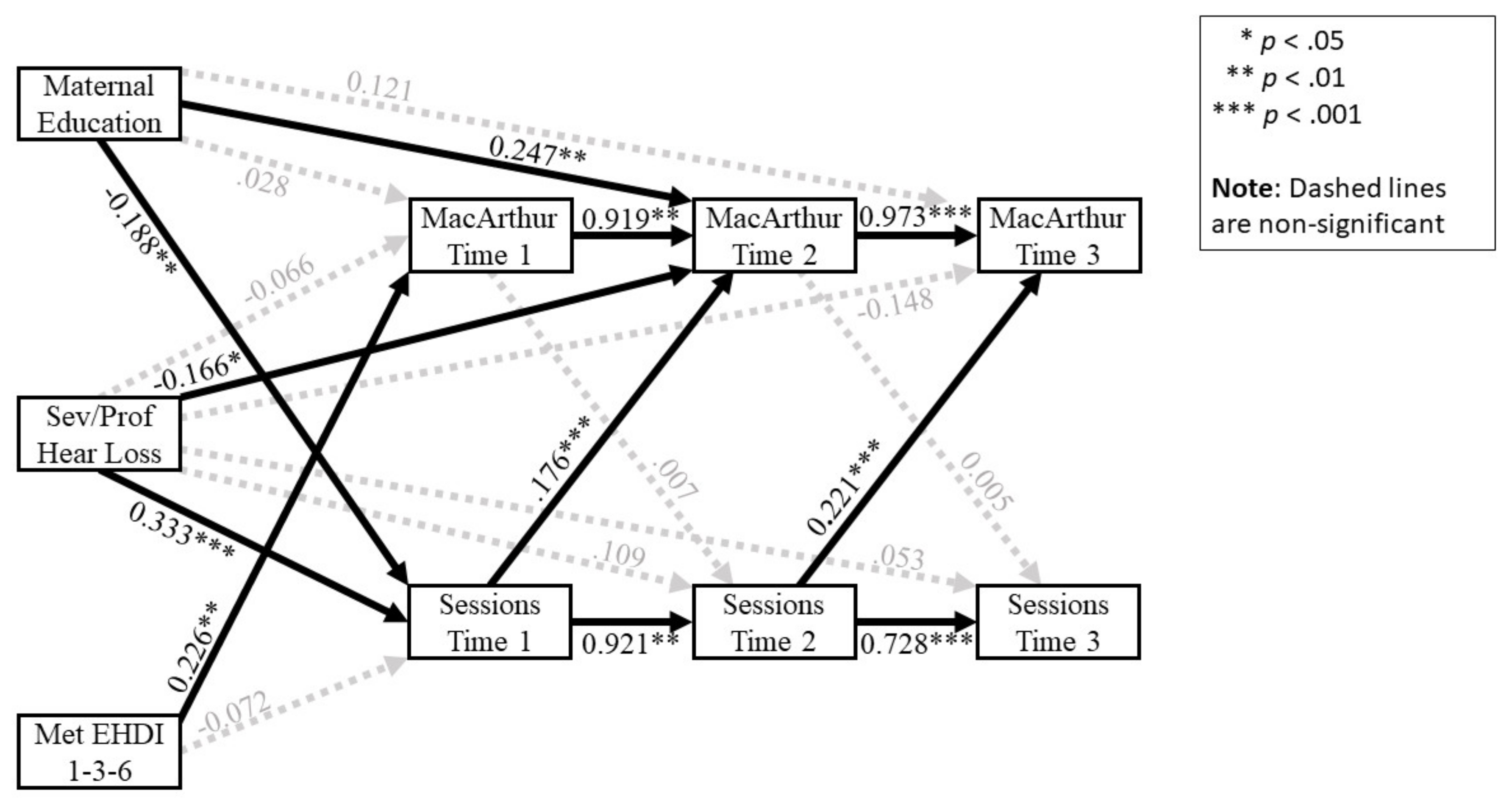
3.3. Structural Equation Model Results
3.3.1. Relationship of Control Variables to Expressive Vocabulary Scores
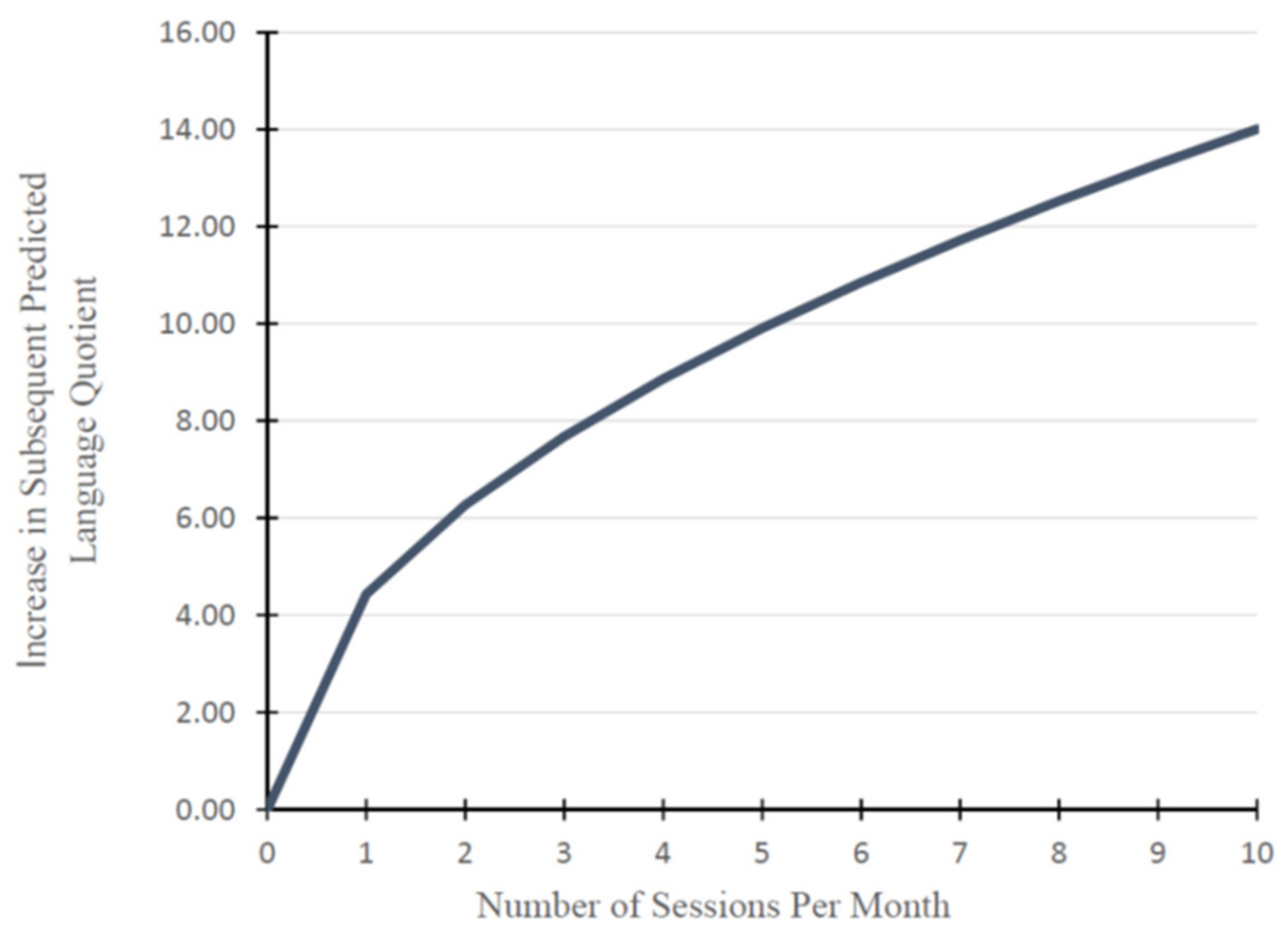
3.3.2. Relationship of Intervention Frequency and Expressive Vocabulary Scores
4. Discussion
4.1. Clinical Implications
4.2. Relationship of Control Variables to Vocabulary Outcomes
4.3. Influence of Vocabulary Ability on Intervention Frequency
4.4. Relationship of Control Variables to Intervention Frequency
4.5. Study Limitations and Directions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yoshinaga-Itano, C.; Sedey, A.L.; Wiggin, M.; Chung, W. Early hearing detection and vocabulary of children with hearing loss. Pediatrics 2017, 140, e20162964. [Google Scholar] [CrossRef]
- American Speech-Language-Hearing Association (ASHA). Effects of Hearing Loss on Development. Available online: www.asha.org/public/hearing/effects-of-hearing-loss-on-development (accessed on 12 February 2017).
- De Diego-Lazaro, B.; Restrepo, M.A.; Sedey, A.L.; Yoshinaga-Itano, C. Predictors of vocabulary outcomes in children who are deaf or hard of hearing from Spanish-speaking families. Lang. Speech Hear. Serv. Sch. 2019, 50, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Nott, P.; Cowan, R.; Brown, P.M.; Wigglesworth, G. Early language development in children with profound hearing loss fitted with a device at a young age: Part I–the time period taken to acquire first words and first word combinations. Ear Hear. 2009, 30, 526–540. [Google Scholar] [CrossRef]
- Tomblin, J.B.; Harrison, M.; Ambrose, S.E.; Walker, E.A.; Oleson, J.J.; Moeller, M.P. Language outcomes in young children with mild to severe hearing loss. Ear Hear. 2015, 36 (Suppl. 1), 76S–91S. [Google Scholar] [CrossRef]
- Joint Committee on Infant Hearing. Year 2019 position statement: Principles and guidelines for early hearing detection and intervention programs. J. Early Hear. Detect. Interv. 2019, 4, 1–44. [Google Scholar] [CrossRef]
- Walton, R.; Dovey, S.; Harvey, E.; Freemantle, N. Computer support for determining drug dose: Systematic review and meta-analysis. BMJ 1999, 318, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Baker, E. Optimal intervention intensity in speech-language pathology: Discoveries, challenges, and unchartered territories. Int. J. Speech Lang. Pathol. Audiol. 2012, 14, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Warren, S.F.; Fey, M.E.; Yoder, P.J. Differential treatment intensity research: A missing link to creating optimally effective communication interventions. Ment. Retard. Dev. Disabil. Res. Rev. 2007, 13, 70–77. [Google Scholar] [CrossRef]
- Enderby, P. How much therapy is enough? The impossible question! Int. J. Speech Lang. Pathol. 2012, 14, 432–437. [Google Scholar] [CrossRef]
- McManus, B.M.; Richardson, Z.; Schenkman, M.; Murphy, N.; Morrato, E.H. Timing and intensity of early intervention service use and outcomes among a safety-net population of children. JAMA Netw. Open. 2019, 2, e187529. [Google Scholar] [CrossRef]
- Yoder, P.; Woynaroski, T.; Fey, M.; Warren, S. Effects of dose frequency of early communication intervention in young children with and without Down syndrome. Am. J. Intellect. Dev. Disabil. 2014, 119, 17–32. [Google Scholar] [CrossRef]
- Meinzen-Derr, J.; Tabangin, M.; Altaye, M.; Minter-Mohr, M.; Van Horn, A.; DeDino, N.; Wiley, S. Early Intervention Intensity for Children who are Deaf/Hard-of-Hearing: Beyond EHDI Benchmarks. In Proceedings of the Conference for Early Hearing Detection and Intervention, Kansas City, MO, USA, 9 March 2020. [Google Scholar]
- Fenson, L.; Marchman, V.A.; Thal, D.J.; Dale, P.S.; Reznick, J.S. MacArthur-Bates Communicative Development Inventories: User’s Guide and Technical Manual; Brookes: Baltimore, MD, USA, 2007. [Google Scholar]
- Bennetts, S.K.; Mensah, F.K.; Westrupp, E.M.; Hackworth, N.J.; Reilly, S. The agreement between parent-reported and directly measured child language and parenting behaviors. Front. Psychol. 2016, 7, 1710. [Google Scholar] [CrossRef]
- Bornstein, M.H.; Haynes, O.M. Vocabulary competence in early childhood: Measurement, latent construct, and predictive validity. Child Dev. 1998, 69, 654–671. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, I.; Pisoni, D.B.; Kronenberger, W.G.; Beer, J. Early expressive language skills predict long-term neurocognitive outcomes in cochlear implant users: Evidence from the MacArthur–Bates Communicative Development Inventories. Am. J. Speech Lang. Pathol. 2016, 25, 381–392. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Thal, D.; Desjardin, J.L.; Eisenberg, L.S. Validity of the MacArthur-Bates Communicative Development Inventories for measuring language abilities in children with cochlear implants. Am. J. Speech Lang. Pathol. 2007, 16, 54–64. [Google Scholar] [CrossRef]
- Can, D.D.; Ginsburg-Block, M.; Golinkoff, R.M.; Hirsh-Pasek, K. A long-term predictive validity study: Can the CDI Short Form be used to predict language and early literacy skills four years later? J. Child Lang. 2013, 40, 821–835. [Google Scholar] [CrossRef] [PubMed]
- Rowe, M.L.; Raudenbush, S.W.; Goldin-Meadow, S. The pace of vocabulary growth helps predict later vocabulary skill. Child Dev. 2012, 83, 508–525. [Google Scholar] [CrossRef]
- Niparko, J.K.; Tobey, E.A.; Thal, D.J.; Eisenberg, L.S.; Wang, N.Y.; Quittner, A.L.; Fink, N.E.; CDaCI Investigative Team. Spoken language development in children following cochlear implantation. JAMA J. Am. Med. Assoc. 2010, 303, 1498–1506. [Google Scholar] [CrossRef]
- Yoshinaga-Itano, C.; Baca, R.L.; Sedey, A.L. Describing the trajectory of language development in the presence of severe to profound hearing loss: A closer look at children with cochlear implants versus hearing aids. Otol. Neurotol. 2010, 31, 1268–1274. [Google Scholar] [CrossRef]
- Vohr, B.; Jodoin-Krauzyk, J.; Tucker, R.; Johnson, M.J.; Topol, D.; Ahlgren, M. Early language outcomes of early-identified infants with permanent hearing loss at 12 to 16 months of age. Pediatrics 2008, 122, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Vohr, B.; Jodoin-Krauzyk, J.; Tucker, R.; Topol, D.; Johnson, M.J.; Ahlgren, M.; St Pierre, L. Expressive vocabulary of children with hearing loss in the first 2 years of life: Impact of early intervention. Am. J. Perinatol. 2011, 31, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Wake, M.; Poulakis, Z.; Hughes, E.K.; Carey-Sargeant, C.; Rickards, F.W. Hearing impairment: A population study of age at diagnosis, severity, and language outcomes at 7–8 years. Arch. Dis. Child. 2005, 90, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Offices of the Department of Education. Code of Federal Regulations: Title 34-Education. Part 303-Early Intervention Programs for Infants and Toddlers with Disabilities. Volume 2. Published 1 July 2019. Available online: https://www.govinfo.gov/content/pkg/CFR-2019-title34-vol2/xml/CFR-2019-title34-vol2-part303.xml#seqnum303.344 (accessed on 3 October 2020).
- Law, J.; Conti-Ramsden, G. Treating children with speech and language impairments. BMJ 2000, 321, 908–909. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Percentage of Participants |
|---|---|
| Sex | |
| Male | 47% |
| Female | 53% |
| Ethnicity | |
| Non-Hispanic | 80% |
| Hispanic | 20% |
| Race | |
| White | 87% |
| African American/Black | 2% |
| Asian | 2% |
| Native American | 1% |
| Hawaiian/Pacific Islander | 1% |
| Mixed race | 7% |
| Communication mode used with the child | |
| Primarily spoken language | 79% |
| Spoken language only | 28% |
| Spoken with very occasional use of sign | 51% |
| Sign language + spoken language | 19% |
| Sign only | 2% |
| Hearing status of the parent | |
| Both parents hearing | 81% |
| One or both parents deaf/hard of hearing a | 19% |
| Mother’s highest educational degree | |
| Less than high school | 7% |
| High school | 36% |
| Vocational | 5% |
| Associate’s | 15% |
| Bachelor’s | 26% |
| Graduate | 11% |
| Characteristic | Percentage of Participants |
|---|---|
| Degree of hearing loss | |
| Mild to moderate | 60% |
| Mild (26 to 40 dB HL) | 37% |
| Moderate (41 to 55 dB HL) | 23% |
| Moderate–severe to profound | 40% |
| Moderate–severe (56 to 70 dB HL) | 11% |
| Severe (71 to 90 dB HL) | 9% |
| Profound (>90 dB HL) | 20% |
| Onset of Hearing Loss | |
| Congenital | 97% |
| Acquired prior to 8 months of age | 3% |
| Met EHDI 1-3-6 guidelines | |
| Yes, met guidelines | 74% |
| No, did not meet guidelines | 26% |
| Type of amplification used | |
| None | 10% |
| Hearing aids | 76% |
| Cochlear implant | 9% |
| Bone conduction hearing aid | 3% |
| Hearing aid + cochlear implant | 2% |
| Independent Variable | Coding of Variable |
|---|---|
| Adherence to the EHDI 1-3-6 guidelines | 0 = does not meet 1-3-6 guidelines; |
| 1 = meets 1-3-6 guidelines | |
| Maternal level of education | Continuous variable: 1 year increments |
| Degree of hearing loss | 0 = mild/moderate levels; |
| 1 = moderate–severe to profound levels | |
| Sessions | Continuous variable: number per month |
| Mean | SD | N | |
|---|---|---|---|
| Mac:CDI vocabulary | |||
| quotient | |||
| Time 1 | 94.3 | 20.0 | 210 |
| Time 2 | 82.0 | 14.9 | 164 |
| Time 3 | 73.7 | 14.5 | 130 |
| Number of sessions | |||
| Time 1 | 3.4 | 2.1 | 210 |
| Time 2 | 4.0 | 2.7 | 164 |
| Time 3 | 4.0 | 2.8 | 130 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiggin, M.; Sedey, A.L.; Yoshinaga-Itano, C.; Mason, C.A.; Gaffney, M.; Chung, W. Frequency of Early Intervention Sessions and Vocabulary Skills in Children with Hearing Loss. J. Clin. Med. 2021, 10, 5025. https://doi.org/10.3390/jcm10215025
Wiggin M, Sedey AL, Yoshinaga-Itano C, Mason CA, Gaffney M, Chung W. Frequency of Early Intervention Sessions and Vocabulary Skills in Children with Hearing Loss. Journal of Clinical Medicine. 2021; 10(21):5025. https://doi.org/10.3390/jcm10215025
Chicago/Turabian StyleWiggin, Mallene, Allison L. Sedey, Christine Yoshinaga-Itano, Craig A. Mason, Marcus Gaffney, and Winnie Chung. 2021. "Frequency of Early Intervention Sessions and Vocabulary Skills in Children with Hearing Loss" Journal of Clinical Medicine 10, no. 21: 5025. https://doi.org/10.3390/jcm10215025
APA StyleWiggin, M., Sedey, A. L., Yoshinaga-Itano, C., Mason, C. A., Gaffney, M., & Chung, W. (2021). Frequency of Early Intervention Sessions and Vocabulary Skills in Children with Hearing Loss. Journal of Clinical Medicine, 10(21), 5025. https://doi.org/10.3390/jcm10215025