
Resilience and Mental Health in the Polish Population during the COVID-19 Lockdown: A Mediation Analysis

 , ,
, ,  , and
, and
Abstract
:1. Introduction
Purpose of the of Study
2. Method
2.1. Participants and Procedure
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Implications
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, C.; Zhao, H. The Impact of COVID-19 on Anxiety in Chinese University Students. Front. Psychol. 2020, 11, 1168. [Google Scholar] [CrossRef] [PubMed]
- Bendau, A. Associations between COVID-19 related media consumption and symptoms of anxiety, depression and COVID-19 related fear in the general population in Germany. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Dymecka, J.; Gerymski, R.; Machnik-Czerwik, A. How does stress affect life satisfaction during the COVID-19 pandemic? Moderated mediation analysis of sense of coherence and fear of coronavirus. Psychol. Health Med. 2021, 31, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Dobrakowski, P.P.; Skalski, S.; Surzykiewicz, J.; Muszyńska, J.; Konaszewski, K. Religious Coping and Life Satisfaction during the COVID-19 Pandemic among Polish Catholics. The Mediating Effect of Coronavirus Anxiety. J. Clin. Med. 2021, 10, 4865. [Google Scholar] [CrossRef]
- Winzer, R.; Lindblad, F.; Sorjonen, K.; Lindberg, L. Positive versus negative mental health in emerging adulthood: A national cross-sectional survey. BMC Public Health 2014, 14, 1238. [Google Scholar] [CrossRef] [Green Version]
- Westerhof, G.J.; Keyes, C.L.M. Mental Illness and Mental Health: The Two Continua Model across the Lifespan. J. Adult Dev. 2009, 17, 110–119. [Google Scholar] [CrossRef] [Green Version]
- Langford, R.; Bonnell, C.P.; Jones, H.E.; Pouliou, T.; Murphy, S.M.; Waters, E.; Komro, K.A.; Gibbs, L.F.; Magnus, D.; Campbell, R. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst. Rev. 2014, 4, CD008958. [Google Scholar] [CrossRef] [PubMed]
- Headey, B.; Kelley, J.; Wearing, A. Dimensions of mental health: Life satisfaction, positive affect, anxiety and depression. Soc. Indic. Res. 1993, 29, 63–82. [Google Scholar] [CrossRef]
- Richardson, G.E. The metatheory of resilience and resiliency. J. Clin. Psychol. 2002, 58, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A.; Mancini, A.D. The Human Capacity to Thrive in the Face of Potential Trauma. Pediatrics 2008, 121, 369–375. [Google Scholar] [CrossRef]
- Fletcher, D.; Sarkar, M. Psychological resilience: A review and critique of definitions, concepts, and theory. Eur. Psychol. 2013, 18, 12–23. [Google Scholar] [CrossRef] [Green Version]
- Ong, A.D.; Bergeman, C.S.; Bisconti, T.L.; Wallace, K.A. Psychological resilience, positive emotions, and successful adaptation to stress in later life. J. Pers. Soc. Psychol. 2006, 91, 730–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, P.Y. Grand challenges in global mental health. Nature 2011, 475, 27–30. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Khazaie, H.; Hosseinian-Far, A.; Khaledi-Paveh, B.; Kazeminia, M.; Mohammadi, M.; Shohaimi, S.; Daneshkhah, A.; Eskandari, S. The prevalence of stress, anxiety and depression within front-line healthcare workers caring for COVID-19 patients: A systematic review and meta-regression. Hum. Resour. Health 2020, 18, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public–A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Moghanibashi-Mansourieh, A. Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian J. Psychiatry 2020, 51, 102076. [Google Scholar] [CrossRef]
- Arora, A.; Jha, A.K.; Alat, P.; Das, S.S. Understanding coronaphobia. Asian J. Psychiatry 2020, 54, 102384. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S. COVID stress syndrome: Concept, structure, and correlates. Depress. Anxiety 2020, 37, 706–714. [Google Scholar] [CrossRef]
- Mak, I.W.C.; Chu, C.M.; Pan, P.C.; Yiu, M.G.C.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 2009, 31, 318–326. [Google Scholar] [CrossRef]
- Lee, S.A.; Jobe, M.C.; Mathis, A.A.; Gibbons, J.A. Incremental validity of coronaphobia: Coronavirus anxiety explains depression, generalized anxiety, and death anxiety. J. Anxiety Disord. 2020, 74, 102268. [Google Scholar] [CrossRef] [PubMed]
- Morganstein, J.C.; Ursano, R.J. Ecological Disasters and Mental Health: Causes, Consequences, and Interventions. Front. Psychiatry 2020, 11, 1. [Google Scholar] [CrossRef]
- Cheung, Y.T.; Chau, P.H.; Yip, P.S.F. A revisit on older adults suicides and Severe Acute Respiratory Syndrome (SARS) epidemic in Hong Kong. Int. J. Geriatr. Psychiatry 2008, 23, 1231–1238. [Google Scholar] [CrossRef]
- Zou, P.; Sun, L.; Yang, W.; Zeng, Y.; Chen, Q.; Yang, H.; Zhou, N.; Zhang, G.; Liu, J.; Li, Y.; et al. Associations between negative life events and anxiety, depressive, and stress symptoms: A cross-sectional study among Chinese male senior college students. Psychiatry Res. 2018, 270, 26–33. [Google Scholar] [CrossRef]
- Antonovsky, A. The salutogenic model as a theory to guide health promotion. Health Promot. Int. 1996, 11, 11–18. [Google Scholar] [CrossRef]
- Zimmerman, M.A. Resiliency Theory: A Strengths-Based Approach to Research and Practice for Adolescent Health; Sage Publications: Los Angeles, CA, USA, 2013. [Google Scholar]
- Länsimies, H.; Pietilä, A.-M.; Hietasola-Husu, S.; Kangasniemi, M. A systematic review of adolescents’ sense of coherence and health. Scand. J. Caring Sci. 2017, 31, 651–661. [Google Scholar] [CrossRef] [PubMed]
- Edward, K.-L. Resilience: A Protector from Depression. J. Am. Psychiatr. Nurses Assoc. 2005, 11, 241–243. [Google Scholar] [CrossRef]
- Luthar, S.S.; Cicchetti, D.; Becker, B. Research on Resilience: Response to Commentaries. Child. Dev. 2000, 71, 573–575. [Google Scholar] [CrossRef]
- Sominsky, L.; Walker, D.W.; Spencer, S.J. One size does not fit all–Patterns of vulnerability and resilience in the COVID-19 pandemic and why heterogeneity of disease matters. Brain. Behav. Immun. 2020, 87, 1. [Google Scholar] [CrossRef]
- Blanc, J.; Rahill, G.J.; Laconi, S.; Mouchenik, Y. Religious Beliefs, PTSD, Depression and Resilience in Survivors of the 2010 Haiti Earthquake. J. Affect. Disord. 2016, 190, 697–703. [Google Scholar] [CrossRef]
- Hansel, T.C.; Osofsky, J.D.; Osofsky, H.J.; Friedrich, P. The Effect of Long-Term Relocation on Child and Adolescent Survivors of Hurricane Katrina. J. Trauma. Stress 2013, 26, 613–620. [Google Scholar] [CrossRef]
- Li, F.; Luo, S.; Mu, W.; Li, Y.; Ye, L.; Zheng, X.; Xu, B.; Ding, Y.; Ling, P.; Zhou, M.; et al. Effects of sources of social support and resilience on the mental health of different age groups during the COVID-19 pandemic. BMC Psychiatry 2021, 21, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hou, W.K.; Tong, H.; Liang, L.; Li, T.W.; Liu, H.; Ben-Ezra, M.; Goodwin, R.; Lee, T.M.-C. Probable anxiety and components of psychological resilience amid COVID-19: A population-based study. J. Affect. Disord. 2021, 282, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Skalski, S.; Konaszewski, K.; Dobrakowski, P.; Surzykiewicz, J.; Lee, S.A. Pandemic grief in Poland: Adaptation of a measure and its relationship with social support and resilience. Curr. Psychol. 2021, 1–9. [Google Scholar]
- PeConga, E.K.; Gauthier, G.M.; Holloway, A.; Walker, R.S.W.; Rosencrans, P.L.; Zoellner, L.A.; Bedard-Gilligan, M. Resilience is spreading: Mental health within the COVID-19 pandemic. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S47–S48. [Google Scholar] [CrossRef]
- PeConga, E.K.; Thøgersen, M.H. Post-traumatic stress disorder, depression, and anxiety in adult Syrian refugees: What do we know? Scand. J. Public Health 2020, 48, 677–687. [Google Scholar] [CrossRef]
- Chong, M.-Y.; Wang, W.-C.; Hsieh, W.-C.; Lee, C.-Y.; Chiu, N.-M.; Yeh, W.-C.; Huang, O.-L.; Wen, J.-K.; Chen, C.-L. Psychological impact of severe acute respiratory syndrome on health workers in a tertiary hospital. Br. J. Psychiatry 2004, 185, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheaton, M.; Abramowitz, J.S.; Berman, N.C.; Fabricant, L.E.; Olatunji, B.O. Psychological Predictors of Anxiety in Response to the H1N1 (Swine Flu) Pandemic. Cogn. Ther. Res. 2011, 36, 210–218. [Google Scholar] [CrossRef]
- Yip, P.S.; Cheung, Y.T.D.; Chau, P.H.; Law, Y. The Impact of Epidemic Outbreak. Crisis 2010, 31, 86–92. [Google Scholar] [CrossRef]
- Skalski, S.; Uram, P.; Dobrakowski, P.; Kwiatkowska, A. The link between ego-resiliency, social support, SARS-CoV-2 anxiety and trauma effects. Polish adaptation of the Coronavirus Anxiety Scale. Pers. Individ. Differ. 2021, 171, 110540. [Google Scholar] [CrossRef] [PubMed]
- Skalski, S.; Uram, P.; Dobrakowski, P.; Kwiatkowska, A. Thinking too much about the novel coronavirus. The link between persistent thinking about COVID-19, SARS-CoV-2 anxiety and trauma effects. Curr. Issues Pers. Psychol. 2020, 8, 169–174. [Google Scholar]
- Langlois, F.; Freeston, M.H.; Ladouceur, R. Differences and similarities between obsessive intrusive thoughts and worry in a non-clinical population: Study 1. Behav. Res. Ther. 2000, 38, 157–173. [Google Scholar] [CrossRef]
- Beck, A.T. Cognitive approaches to panic disorder: Theory and therapy. In Panic: Psychological Perspectives; Rachman, S., Maser, J.D., Eds.; Lawrence Erlbaum Associates, Inc.: Mahwah, NJ, USA, 1988; pp. 91–109. [Google Scholar]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, H.; Skoog, T. The mediational role of perceived stress in the relation between optimism and burnout in competitive athletes. Anxiety Stress Coping 2012, 25, 183–199. [Google Scholar] [CrossRef]
- Wang, Q.; Xu, W.; Ren, L.; Wang, W.; Wang, Y. The relationship between hope and post-traumatic stress disorder in Chinese shidu parents: The mediating role of perceived stress. J. Affect. Disord. 2019, 251, 23–30. [Google Scholar] [CrossRef]
- Vinkers, C.H.; van Amelsvoort, T.; Bisson, J.I.; Branchi, I.; Cryan, J.F.; Domschke, K.; Howes, O.D.; Manchia, M.; Pinto, L.; de Quervain, D.; et al. Stress resilience during the coronavirus pandemic. Eur. Neuropsychopharmacol. 2020, 35, 12–16. [Google Scholar] [CrossRef]
- Chen, S.; Bonanno, G.A. Psychological adjustment during the global outbreak of COVID-19: A resilience perspective. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S51–S54. [Google Scholar] [CrossRef]
- Burke, J.; Arslan, G. Positive Education and School Psychology during COVID-19 Pandemic. J. Posit. Sch. Psychol. 2020, 4, 137–139. [Google Scholar] [CrossRef]
- Mahamid, F.A.; Bdier, D. The Association between Positive Religious Coping, Perceived Stress, and Depressive Symptoms During the Spread of Coronavirus (COVID-19) Among a Sample of Adults in Palestine: Across Sectional Study. J. Relig. Health 2021, 60, 34–49. [Google Scholar] [CrossRef]
- Fuhrman, S.; Kalyanpur, A.; Friedman, S.; Tran, N.T. Gendered implications of the COVID-19 pandemic for policies and programmes in humanitarian settings. BMJ Glob. Health 2020, 5, e002624. [Google Scholar] [CrossRef] [PubMed]
- Conversano, C.; Miniati, M. Psychological distress among healthcare professionals involved in the COVID-19 emergency: Vulnerability and resilience factors. Neuropsychiatry 2020, 17, 94–96. [Google Scholar]
- Jahanshahi, A.A.; Dinani, M.M.; Madavani, A.N.; Li, J.; Zhang, S.X. The distress of Iranian adults during the COVID-19 pandemic—More distressed than the Chinese and with different predictors. Brain Behav. Immun. 2020, 87, 124–125. [Google Scholar] [CrossRef]
- Asmundson, G.J.G.; Taylor, S. How health anxiety influences responses to viral outbreaks like COVID-19: What all decision-makers, health authorities, and health care professionals need to know. J. Anxiety Disord. 2020, 71, 102211. [Google Scholar] [CrossRef]
- Seligman, M.E. Positive psychology, positive prevention, and positive therapy. Handb. Posit. Psychol. 2002, 2, 3–12. [Google Scholar]
- Peterson, C.; Seligman, M.E. Character Strengths and Virtues: A Handbook and Classification; Oxford University Press: Oxford, UK, 2004. [Google Scholar]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Cichoń, E.; Kiejna, A.; Kokoszka, A.; Gondek, T.; Rajba, B.; Lloyd, C.E.; Sartorius, N. Validation of the Polish version of WHO-5 as a screening instrument for depression in adults with diabetes. Diabetes Res. Clin. Pract. 2020, 159, 107970. [Google Scholar] [CrossRef] [PubMed]
- Büssing, A.; Recchia, D.R.; Hein, R.; Dienberg, T. Perceived changes of specific attitudes, perceptions and behaviors during the Corona pandemic and their relation to wellbeing. Health Qual. Life Outcomes 2020, 18, 1–17. [Google Scholar] [CrossRef]
- Lee, S.A.; Mathis, A.A.; Jobe, M.C.; Pappalardo, E.A. Clinically significant fear and anxiety of COVID-19: A psychometric examination of the Coronavirus Anxiety Scale. Psychiatry Res. 2020, 290, 113112. [Google Scholar] [CrossRef]
- Lee, S.A. How much “Thinking” about COVID-19 is clinically dysfunctional? Brain. Behav. Immun. 2020, 87, 97. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Konaszewski, K.; Niesiobędzka, M.; Surzykiewicz, J. Validation of the Polish version of the Brief Resilience Scale (BRS). PLoS ONE 2020, 15, e0237038. [Google Scholar] [CrossRef]
- Hayes, A.F. Methodology in the Social Sciences: Introduction to Mediation, Moderation, and Conditional Process. Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Cosco, T.D.; Howse, K.; Brayne, C. Healthy ageing, resilience and wellbeing. Epidemiol. Psychiatr. Sci. 2017, 26, 579–583. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.; Hollinger-Smith, L. Savoring, resilience, and psychological well-being in older adults. Aging Ment. Health 2014, 19, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Burack, J.; Blidner, A.; Flores, H.; Fitch, T. Constructions and Deconstructions of Risk, Resilience and Wellbeing: A Model for Understanding the Development of Aboriginal Adolescents. Australas. Psychiatry 2007, 15, S18–S23. [Google Scholar] [CrossRef]
- Benson, P.L.; Scales, P.C.; Hamilton, S.F.; Sesma, A., Jr. Positive Youth Development: Theory, Research, and Applications. In Handbook of Child Psychology, 6th ed.; Damon, W., RM, L., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2007. [Google Scholar]
- Turner, K.; McCarthy, V.L. Stress and anxiety among nursing students: A review of intervention strategies in literature between 2009 and 2015. Nurse Educ. Pract. 2017, 22, 21–29. [Google Scholar] [CrossRef]
- Haggerty, R.J.; Sherrod, L.R.; Garmezy, N.; Rutter, M. Stress, Risk, and Resilience in Children and Adolescents: Processes, Mechanisms, and Interventions; Cambridge University Press: Cambridge, UK, 1996. [Google Scholar]
- Melnyk, B.M.; Small, L.; Morrison-Beedy, D.; Strasser, A.; Spath, L.; Kreipe, R.; Crean, H.; Jacobson, D.; Kelly, S.; O’Haver, J. The COPE Healthy Lifestyles TEEN Program: Feasibility, Preliminary Efficacy, & Lessons Learned from an After School Group Intervention with Overweight Adolescents. J. Pediatr. Health Care 2007, 21, 315–322. [Google Scholar]
- Satici, S.A. Psychological vulnerability, resilience, and subjective well-being: The mediating role of hope. Pers. Individ. Differ. 2016, 102, 68–73. [Google Scholar] [CrossRef]
- Karreman, A.; Vingerhoets, A.J. Attachment and well-being: The mediating role of emotion regulation and resilience. Pers. Individ. Differ. 2012, 53, 821–826. [Google Scholar] [CrossRef]
- Windgassen, S.; Goldsmith, K.; Moss-Morris, R.; Chalder, T. Establishing how psychological therapies work: The importance of mediation analysis. J. Ment. Health 2016, 25, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Chmielewski, J.P.; Raczek, M.; Puścion, M.; Chmielowiec, B.; Pawlas, N.; Luszczki, J.J. COVID-19, wywołany przez wirus SARS-CoV-2, jako choroba zawodowa osób wykonujących zawody medyczne. Med. Ogólna Nauk. O Zdrowiu 2021, 27, 235–243. [Google Scholar] [CrossRef]
- Sagone, E.; De Caroli, M.E. Relationships between Psychological Well-being and Resilience in Middle and Late Adolescents. Procedia-Soc. Behav. Sci. 2014, 141, 881–887. [Google Scholar] [CrossRef] [Green Version]
- Bajaj, B.; Pande, N. Mediating role of resilience in the impact of mindfulness on life satisfaction and affect as indices of subjective well-being. Pers. Individ. Differ. 2016, 93, 63–67. [Google Scholar] [CrossRef]
- Souri, H.; Hasanirad, T. Relationship between Resilience, Optimism and Psychological Well-Being in Students of Medicine. Procedia-Soc. Behav. Sci. 2011, 30, 1541–1544. [Google Scholar] [CrossRef] [Green Version]
- Takebayashi, Y.; Tanaka, K.; Sugiura, Y.; Sugiura, T. Well-Being and Generalized Anxiety in Japanese Undergraduates: A Prospective Cohort Study. J. Happiness Stud. 2018, 19, 917–937. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, S.; Wabano, M.J.; Russell, K.; Enosse, L.; Young, N. Promoting resilience and wellbeing through an outdoor intervention designed for Aboriginal adolescents. Rural Remote Health 2014, 14, 2523. [Google Scholar] [PubMed]
- Davydov, D.M.; Stewart, R.; Ritchie, K.; Chaudieu, I. Resilience and mental health. Clin. Psychol. Rev. 2010, 30, 479–495. [Google Scholar] [CrossRef] [Green Version]
- Dunn, L.B.; Iglewicz, A.; Moutier, C. A Conceptual Model of Medical Student Well-Being: Promoting Resilience and Preventing Burnout. Acad. Psychiatry 2008, 32, 44–53. [Google Scholar] [CrossRef]
- Haase, J.E. The Adolescent Resilience Model as a Guide to Interventions. J. Pediatr. Oncol. Nurs. 2004, 21, 289–299. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| M (SD) | Min | Max | 1. | 2. | 3. | 4. | |
|---|---|---|---|---|---|---|---|
| 1. Resilience | 18.64 (5.28) | 6 | 30 | 1 | |||
| 2. Coronavirus anxiety | 1.59 (2.95) | 0 | 20 | −0.18 *** | 1 | ||
| 3. Persistent thinking | 3.03 (3.18) | 0 | 16 | −0.17 *** | 0.54 *** | 1 | |
| 4. Perceived stress | 173.03 (123.69) | 0 | 500 | −0.29 *** | 0.36 *** | 0.44 *** | 1 |
| 5. Well-being | 13.72 (5.72) | 0 | 25 | 0.38 *** | −0.23 *** | −0.31 *** | −0.48 *** |
| a Path | b Path | c Path | c′ Path | Indirect Effect and B (SE) | 95% CI Lower Upper | |
|---|---|---|---|---|---|---|
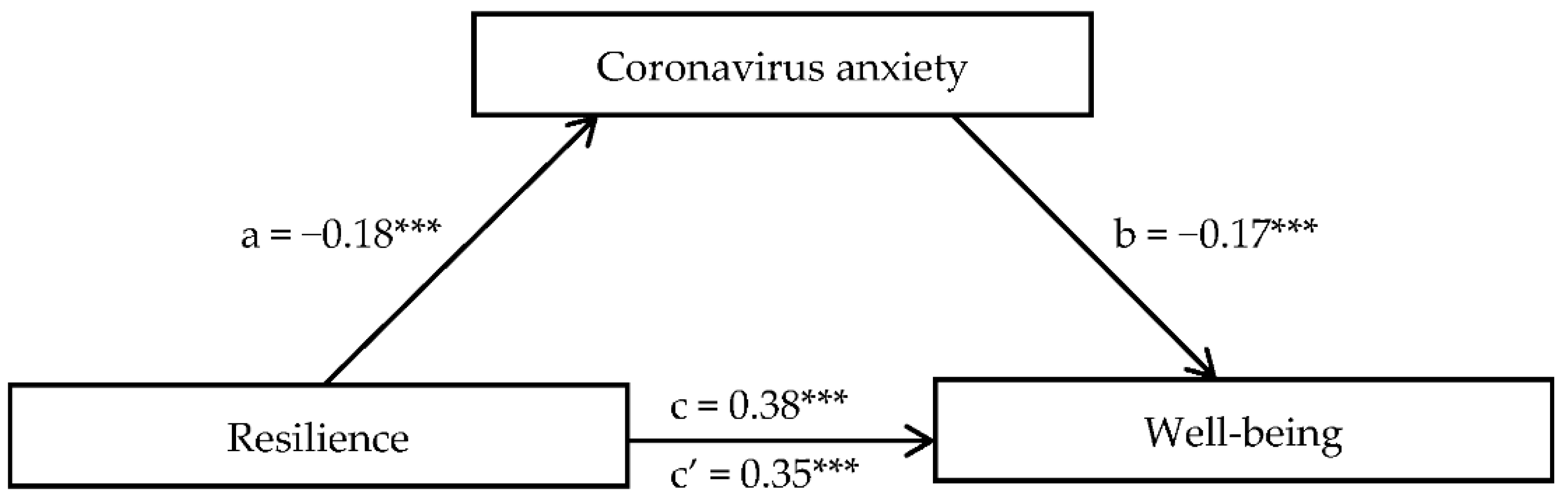
| Resilience → Coronavirus anxiety → Well-being | −0.18 *** | −0.17 *** | 0.38 *** | 0.35 *** | 0.031 (0.006) | 0.020; 0.043 |
| Resilience → Persistent thinking → Well-being | −0.17 *** | −0.25 *** | 0.38 *** | 0.34 *** | 0.044 (0.007) | 0.030; 0.058 |
| Resilience → Perceived stress → Well-being | −0.29 *** | −0.41 *** | 0.38 *** | 0.26 *** | 0.119 (0.010) | 0.099; 0.141 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Surzykiewicz, J.; Konaszewski, K.; Skalski, S.; Dobrakowski, P.P.; Muszyńska, J. Resilience and Mental Health in the Polish Population during the COVID-19 Lockdown: A Mediation Analysis. J. Clin. Med. 2021, 10, 4974. https://doi.org/10.3390/jcm10214974
Surzykiewicz J, Konaszewski K, Skalski S, Dobrakowski PP, Muszyńska J. Resilience and Mental Health in the Polish Population during the COVID-19 Lockdown: A Mediation Analysis. Journal of Clinical Medicine. 2021; 10(21):4974. https://doi.org/10.3390/jcm10214974
Chicago/Turabian StyleSurzykiewicz, Janusz, Karol Konaszewski, Sebastian Skalski, Paweł Piotr Dobrakowski, and Jolanta Muszyńska. 2021. "Resilience and Mental Health in the Polish Population during the COVID-19 Lockdown: A Mediation Analysis" Journal of Clinical Medicine 10, no. 21: 4974. https://doi.org/10.3390/jcm10214974
APA StyleSurzykiewicz, J., Konaszewski, K., Skalski, S., Dobrakowski, P. P., & Muszyńska, J. (2021). Resilience and Mental Health in the Polish Population during the COVID-19 Lockdown: A Mediation Analysis. Journal of Clinical Medicine, 10(21), 4974. https://doi.org/10.3390/jcm10214974