
Out-of-Hospital Treatment of Hepatitis C Increases Retention in Care among People Who Inject Drugs and Homeless Persons: An Observational Study


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
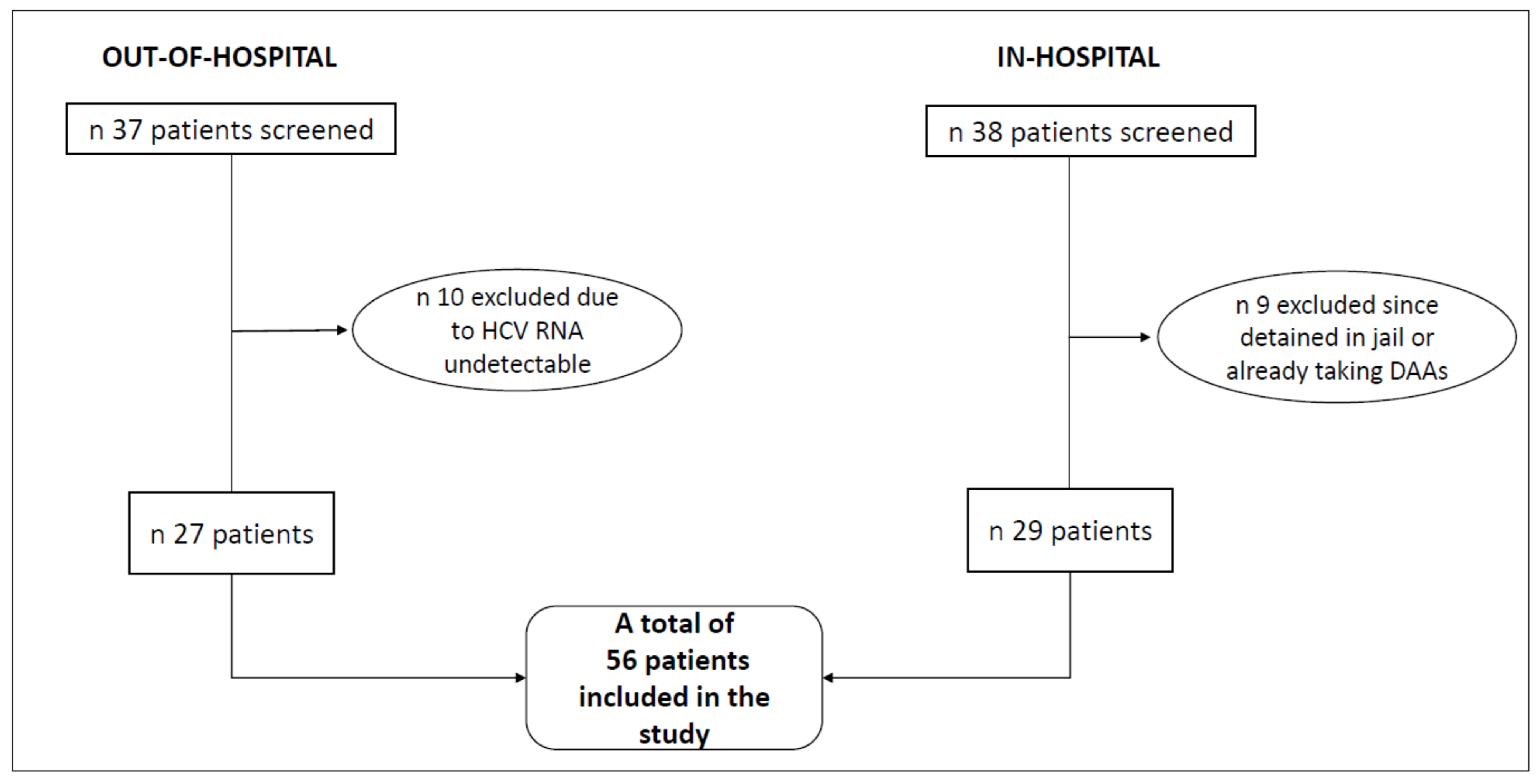
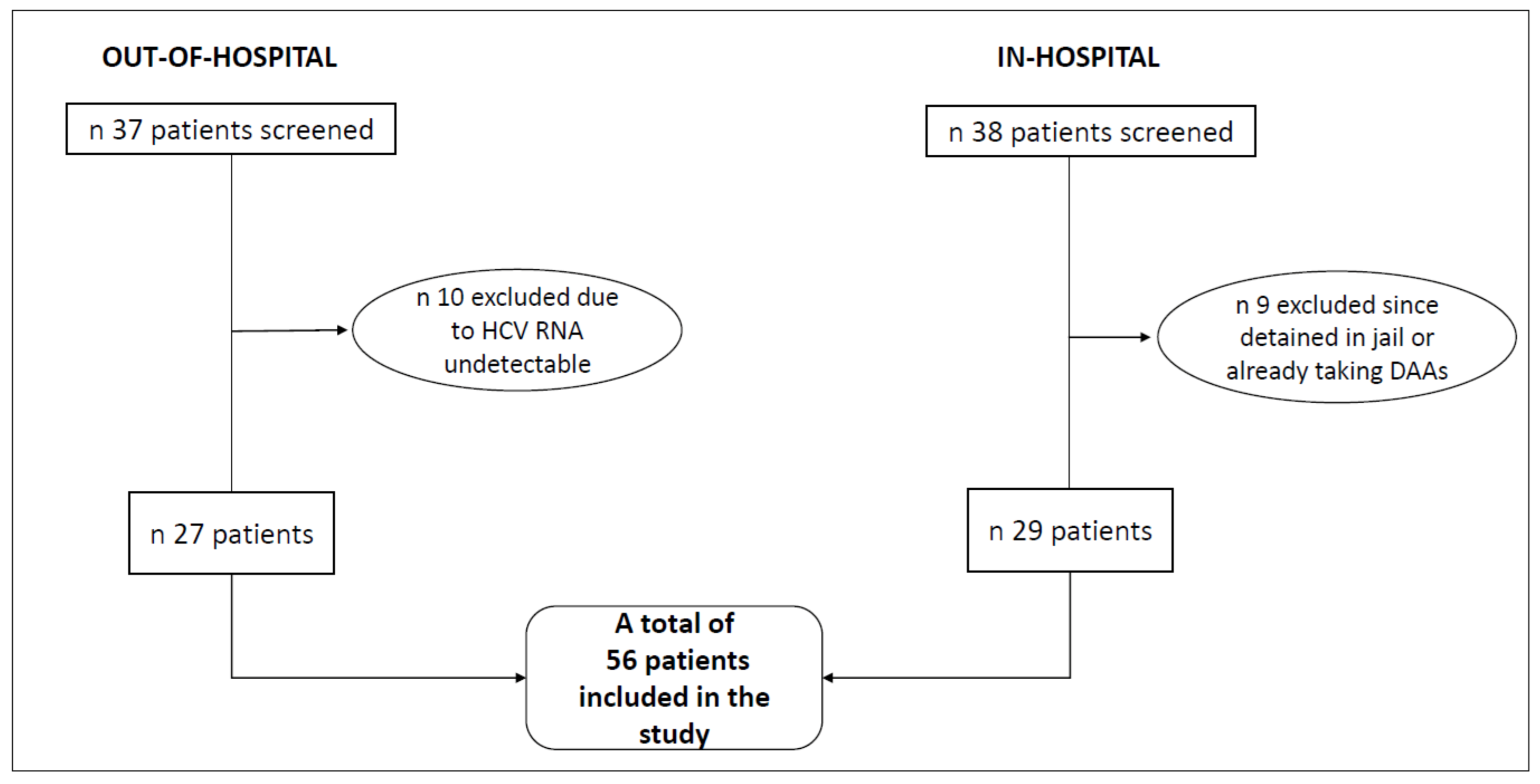
3. Results
3.1. Patient Characteristics at Baseline
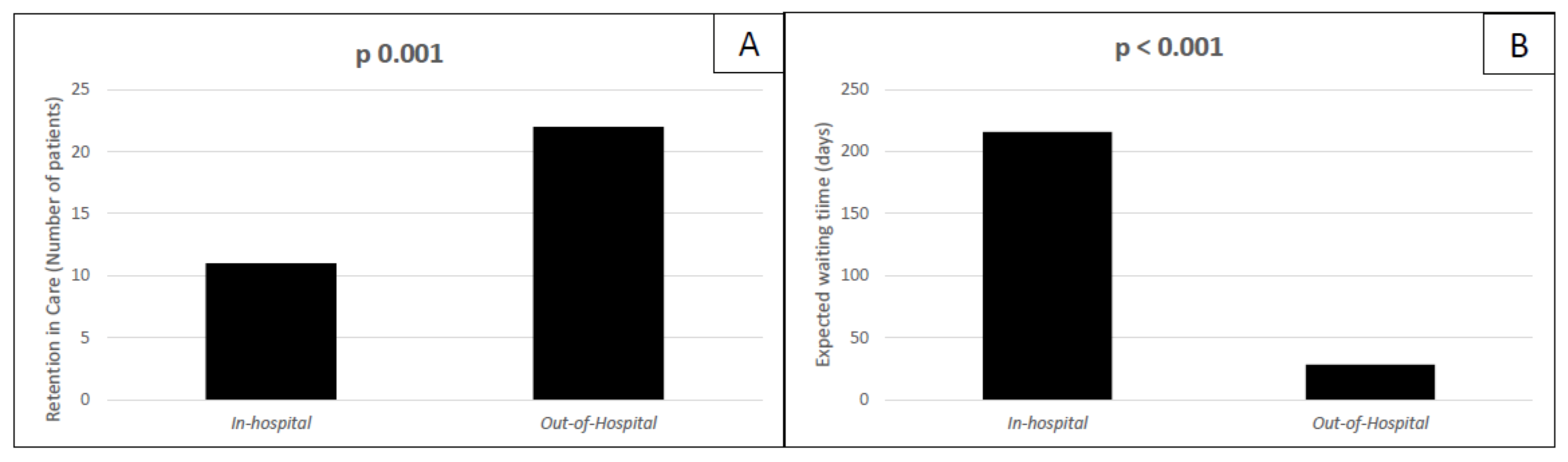
3.2. Primary and Secondary Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global Hepatitis Report 2017: Web Annex B: WHO Estimates of the Prevalence and Incidence of Hepatitis C Virus Infection by WHO Region, 2015. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/277005/WHO-CDS-HIV-18.46-eng.pdf (accessed on 9 October 2021).
- WHO. Global Report on Access to Hepatitis C Treatment—Focus on Overcoming Barriers. Available online: http://www.who.int/Hepatitis/publications/hep-c-access-report/en/ (accessed on 10 October 2021).
- WHO Website. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c (accessed on 10 October 2021).
- Centers for Disease Control and Prevention (CDC). Division of Viral Hepatitis 2025 Strategic Plan, CDC. Available online: https://www.hhs.gov/hepatitis/viral-hepatitis-national-strategic-plan/index.html (accessed on 25 October 2021).
- Schillie, S.; Wester, C. CDC Recommendations for Hepatitis C Screening Among Adults—United States, 2020. MMWR Recomm. Rep. 2020, 69, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Degenhardt, L.; Peacock, A. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: A multistage systematic review. Lancet Glob. Health 2017, 5, e1192–e1207. [Google Scholar] [CrossRef] [Green Version]
- Beijer, U.; Wolf, A. Prevalence of tuberculosis, Hepatitis C virus, and HIV in homeless people: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 859–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arum, C.; Fraser, H. Homelessness, HIV, and HCV Review Collaborative Group. Homelessness, unstable housing, and risk of HIV and Hepatitis C virus acquisition among people who inject drugs: A systematic review and meta-analysis. Lancet Public Health 2021, 6, e309–e323. [Google Scholar] [CrossRef] [PubMed]
- Persico, M.; Aglitti, A. Real-life glecaprevir/pibrentasvir in a large cohort of patients with Hepatitis C virus infection: The MISTRAL study. Liver Int. 2019, 39, 1852–1859. [Google Scholar] [CrossRef]
- Foster, G.R.; Dore, G. Glecaprevir/pibrentasvir in patients with chronic HCV and recent drug use: An integrated analysis of 7 phase III studies. Drug Alcohol Depend. 2019, 194, 487–494. [Google Scholar] [CrossRef]
- AASLD-IDS. HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C. 2018. Available online: https://www.hcvguidelines.org/ (accessed on 30 September 2018).
- European Association for the Study of the Liver. EASL recommendations on treatment of Hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef]
- Stone, J.; Fraser, H. Incarceration history and risk of HIV and Hepatitis C virus acquisition among people who inject drugs: A systematic review and meta-analysis. Lancet Infect. Dis. 2018, 18, 1397–1409. [Google Scholar] [CrossRef] [Green Version]
- Bruneau, J. Sustained Drug Use Changes After Hepatitis C Screening and Counseling Among Recently Infected Persons Who Inject Drugs: A Longitudinal Study. Clin. Infect. Dis. 2014, 58, 755–761. [Google Scholar] [CrossRef] [Green Version]
- Platt, L. Needle and syringe programmes and opioid substitution therapy for preventing HCV transmission among people who inject drugs: Findings from a Cochrane Review and meta-analysis. Addiction 2018, 113, 545–563. [Google Scholar] [CrossRef]
- Martin, N.K.; Hickman, M. Combination Interventions to Prevent HCV Transmission Among People Who Inject Drugs: Modeling the Impact of Antiviral Treatment, Needle and Syringe Programs, and Opiate Substitution Therapy. Clin. Infect. Dis. 2013, 57, S39–S45. [Google Scholar] [CrossRef]
- Windelinckx, T. C-Buddies: Challenges in the comprehensive approach of Hepatitis C management among people who use drugs in harm reduction setting in Antwerp Belgium. In Proceedings of the 6th International Symposium on Hepatitis Care in Substance Users, Organized by International Network on Hepatitis in Substance Users (INHSU), Jersey City, NY, USA, 6–8 September 2017. [Google Scholar]
- Dore, G.J. Elbasvir-Grazoprevir to Treat Hepatitis C Virus Infection in Persons Receiving Opioid Agonist Therapy: A Randomized Trial. Ann. Intern. Med. 2016, 165, 625–634. [Google Scholar] [CrossRef] [Green Version]
- Grebely, J.; Robaeys, G.; Bruggmann, P.; Aghemo, A.; Backmund, M.; Bruneau, J.; Byrne, J.; Dalgard, O.; Feld, J.J.; Hellard, M.; et al. Recommendations for the management of Hepatitis c virus infection among people who inject drugs. Int. J. Drug Policy 2015, 26, 1028–1038. [Google Scholar] [CrossRef] [Green Version]
- Remy, A.-J.; Bouchkira, H. Successful Cascade of Care and Cure HCV in 5382 Drugs Users: How Increase HCV Treatment by Outreach Care, Since Screening to Treatment. J. Dig. Disord. Diagn. 2019, 1, 27–35. [Google Scholar] [CrossRef]
- Verma, S. The Final Frontier: Testing through community needle exchange pharmacies in London. In Proceedings of the International Symposium on Hepatitis Care in Substance Users, Cascais, Portugal, 19–21 September 2018. [Google Scholar]
- Saludes, V. Community-based screening of Hepatitis C with a one-step RNA detection algorithm from dried-blood spots: Analysis of key populations in Barcelona, Spain. J. Viral Hepat. 2018, 25, 236–244. [Google Scholar] [CrossRef]
- Peters, L. Decentralised HCV care: The SACC project. In Proceedings of the 5th International Symposium on Hepatitis Care in Substance Users, Organized by International Network on Hepatitis in Substance Users (INHSU), Oslo, Norway, 7 September 2016. [Google Scholar]
- Messina, V.; Russo, A. Innovative procedures for micro-elimination of HCV infection in persons who use drugs. J. Viral Hepat. 2020, 27, 1437–1443. [Google Scholar] [CrossRef]
- Molinaro, S.; Resce, G. Barriers to effective management of Hepatitis C virus in people who inject drugs: Evidence from outpatient clinics. Drug Alcohol Rev. 2019, 38, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Foschi, F.G.; Borghi, A. Model of Care for Microelimination of Hepatitis C Virus Infection among People Who Inject Drugs. J. Clin. Med. 2021, 10, 4001. [Google Scholar] [CrossRef] [PubMed]
- Schmidbauer, C.; Schwarz, M. Directly observed therapy at opioid substitution facilities using sofosbuvir/velpatasvir results in excellent SVR12 rates in PWID at high risk for non-adherence to DAA therapy. PLoS ONE 2021, 16, e0252274. [Google Scholar] [CrossRef] [PubMed]
- Loo, N. Real-world observational experience with direct-acting antivirals for Hepatitis C: Baseline resistance, efficacy, and need for long-term surveillance. Medicine 2019, 98, e16254. [Google Scholar] [CrossRef]
- Simmons, B.; Saleem, J. Risk of Late Relapse or Reinfection with Hepatitis C Virus after Achieving a Sustained Virological Response: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2016, 62, 683–694. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Characteristics | Total Population (n = 56) | In-Hospital Group (n = 29) | Out-of-Hospital Group (n = 27) | p Value |
|---|---|---|---|---|
| Age (year), median (IQR) | 44.5 (35.5–51) | 45 (36.5–50.5) | 41 (35.0–51) | 0.941 |
| Male, n (%) | 52.0 (92.9%) | 27 (93.1%) | 25 (92.6%) | 1.000 |
| BMI, median (IQR) | 22.8 (20.8–24.8) | 23.2 (21.0–27.2) | 22.6 (20.1–24.5) | 0.154 |
| Active PWID | 41 (73.2%) | 29 (100%) | 12 (44.4%) | <0.001 |
| Previous PWID | 15 (26.8%) | 0 (0%) | 15 (55.6%) | 0.001 |
| Homeless | 12 (21.4%) | 1 (3.4%) | 11 (40.7%) | 0.001 |
| OST, n (%) | 40.0 (71.4%) | 26.0 (89.7%) | 14.0 (51.9%) | 0.003 |
| Psychiatric comorbidity, n (%) | 15.0 (26.8%) | 6.0 (20.7%) | 9.0 (33.3%) | 0.370 |
| HBsAg positive, n (%) | 1.0 (1.9%) | 1 (3.4%) | 0.0 (0.0%) | 1.000 |
| HIV coinfection, n (%) | 13.0 (24.5%) | 10.0 (34.5%) | 3.0 (12.5%) | 0.108 |
| Liver Stiffness 1, kPa, median (IQR) | 6.5 (5.1–8.2) | 6.8 (5.1–8.6) | 6.35 (5.0–8.1) | 0.434 |
| Child-Pugh class 2, n (%) | 1 | |||
| A | 6 | 3 | 3 | |
| B | 2 | 1 | 1 | |
| HCV genotype, n (%) | 0.754 | |||
| 1 | 30.0 (58.8%) | 14.0 (53.8%) | 16.0 (64%) | |
| 3 | 16.0 (31.4%) | 9.0 (34.6%) | 7.0 (28%) | |
| 4 | 5.0 (9.8%) | 3.0 (11.5%) | 2.0 (8%) | |
| Prior Peg-IFN/RBV failure, n (%) | 8.9 (14.8%) | 2.0 (7.4%) | 6.0 (22.2%) | 0.250 |
| HCV RNA, log10 IU/mL, median (IQR) | 6.1 (5.2–6.3) | 6.1 (5.4–6.4) | 6.0 (5.0–6.3) | 0.741 |
| ALT, IU/L, median (IQR) | 45.0 (29.0–110) | 44.0 (28.3–110) | 55.0 (30.0–110) | 0.899 |
| Total bilirubin, mg/dL, median (IQR) | 0.6 (0.4–0.8) | 0.6 (0.4–0.9) | 0.6 (0.4–0.8) | 0.381 |
| Creatinine, mg/dL, median (IQR) | 0.8 (0.7–0.9) | 0.9 (0.8–1) | 0.7 (0.6–0.8) | 0.003 |
| Platelets, ×109/L, median (IQR) | 218 (177–266) | 202 (152–253) | 234 (185–273) | 0.108 |
| Parameters | Total Population (n = 13) | In-Hospital Group (n = 10) | Out-of-Hospital Group (n = 3) | p Value |
|---|---|---|---|---|
| Undetectable HIV RNA, n (%) | 9 (75%) | 8 (88.9%) | 1 (33.3%) | 0.127 |
| CD4+ cell count/mm3, median (IQR) | 632 (419–849) | 575 (377–891) | 688 (545–746) | 1.000 |
| ART regimen, n (%) | 0.931 | |||
| 2NRTI + NNRTI | 4 (33.3%) | 3 (33.3%) | 1 (33.3%) | |
| 2NRTI + INSTI | 3 (25%) | 2 (22.2%) | 1 (33. 3%) | |
| 2NRTI + PI | 1 (8.3%) | 1 (11.1%) | none | |
| Others | 4 (33.3%) | 3 (33.3%) | 1 (33.3%) |
| Outcomes | Total Population (n = 56) | In-Hospital Group (n = 29) | Out-of-Hospital Group (n = 27) | p Value |
|---|---|---|---|---|
| Retention in care 1, n (%) | 33 (58.9%) | 11 (37.9%) | 22 (81.5%) | 0.001 |
| Expected waiting time 2, days, median (IQR) | 42 (28.0–215.3) | 216 (168.5–314.8) | 28.0 (21.0–28.0) | <0.001 |
| Treated population (n = 33) | In-hospital group (n = 11) | Out-of-hospital group (n = 22) | ||
| SVR12, n (%) | 31 (93.9%) | 10 (90.9%) | 21 (94.5%) | 0.6 |
| Variables | Univariate Analysis | ||
|---|---|---|---|
| Exp (B) | 95% CI | p-Value | |
| Age | 1.042 | 0.989; 1.099 | 0.123 |
| Male sex | 0.68 | 0.088; 5.19 | 0.71 |
| Metavir F4 | 0.281 | 0.031; 2.552 | 0.26 |
| BMI | 0.91 | 0.79; 1.047 | 0.18 |
| Homelessness | 1.032 | 0.28; 3.77 | 0.96 |
| OST | 2.71 | 0.747; 9.87 | 0.129 |
| Psychiatric comorbidity | 0.64 | 0.19; 2.2 | 0.48 |
| HIV coinfection | 1.43 | 0.40; 5.1 | 0.58 |
| Prior Peg-IFN/RBV failure | 3.13 | 0.66; 14.8 | 0.15 |
| ALT | 1.002 | 0.99; 1.01 | 0.71 |
| Bilirubin | 1.25 | 0.453; 3.46 | 0.67 |
| Creatinine | 0.128 | 0.006; 2.77 | 0.19 |
| Platelets | 0.997 | 0.99; 1.004 | 0.434 |
| Expected waiting time 1, days | 0.992 | 0.987; 0.997 | 0.003 |
| Out-of-hospital management | 0.139 | 0.041; 0.474 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Granozzi, B.; Guardigni, V.; Badia, L.; Rosselli Del Turco, E.; Zuppiroli, A.; Tazza, B.; Malosso, P.; Pieralli, S.; Viale, P.; Verucchi, G. Out-of-Hospital Treatment of Hepatitis C Increases Retention in Care among People Who Inject Drugs and Homeless Persons: An Observational Study. J. Clin. Med. 2021, 10, 4955. https://doi.org/10.3390/jcm10214955
Granozzi B, Guardigni V, Badia L, Rosselli Del Turco E, Zuppiroli A, Tazza B, Malosso P, Pieralli S, Viale P, Verucchi G. Out-of-Hospital Treatment of Hepatitis C Increases Retention in Care among People Who Inject Drugs and Homeless Persons: An Observational Study. Journal of Clinical Medicine. 2021; 10(21):4955. https://doi.org/10.3390/jcm10214955
Chicago/Turabian StyleGranozzi, Bianca, Viola Guardigni, Lorenzo Badia, Elena Rosselli Del Turco, Alberto Zuppiroli, Beatrice Tazza, Pietro Malosso, Stefano Pieralli, Pierluigi Viale, and Gabriella Verucchi. 2021. "Out-of-Hospital Treatment of Hepatitis C Increases Retention in Care among People Who Inject Drugs and Homeless Persons: An Observational Study" Journal of Clinical Medicine 10, no. 21: 4955. https://doi.org/10.3390/jcm10214955
APA StyleGranozzi, B., Guardigni, V., Badia, L., Rosselli Del Turco, E., Zuppiroli, A., Tazza, B., Malosso, P., Pieralli, S., Viale, P., & Verucchi, G. (2021). Out-of-Hospital Treatment of Hepatitis C Increases Retention in Care among People Who Inject Drugs and Homeless Persons: An Observational Study. Journal of Clinical Medicine, 10(21), 4955. https://doi.org/10.3390/jcm10214955