
Acute Kidney Injury Following Admission with Acute Coronary Syndrome: The Role of Diabetes Mellitus


 , and
, and
Abstract
1. Introduction
2. Methods
2.1. Study Design and Population
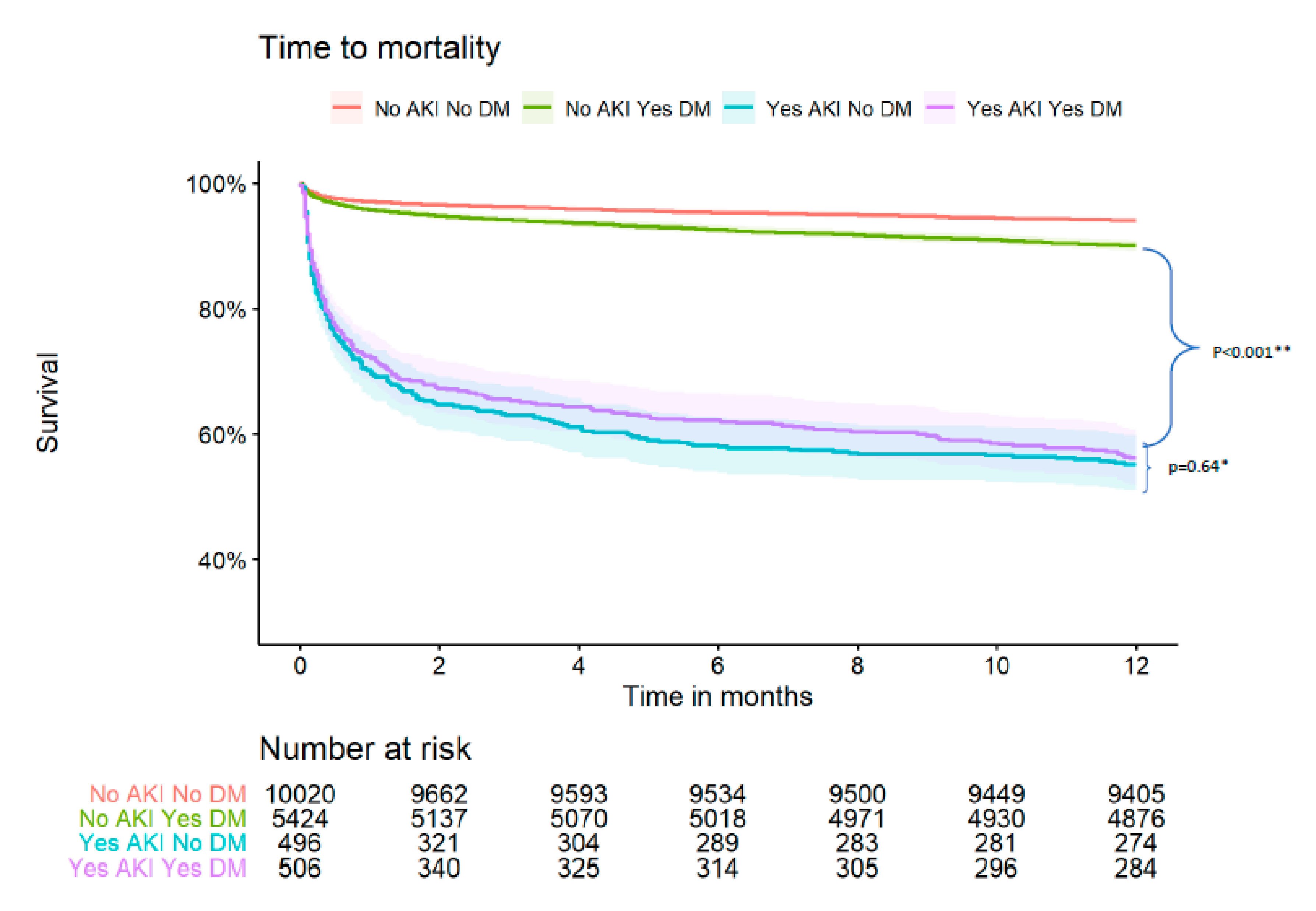
- no-AKI_no-DM: patients without DM that did not develop AKI.
- no-AKI_DM: patients with DM that did not develop AKI.
- AKI_no-DM: patients without DM that developed AKI.
- AKI_DM: patients with DM that developed AKI.
2.2. Outcomes
2.3. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ezzati, M.; Obermeyer, Z.; Tzoulaki, I.; Mayosi, B.M.; Elliott, P.; Leon, D.A. Contributions of risk factors and medical care to cardiovascular mortality trends. Nat. Rev. Cardiol. 2015, 12, 508–530. [Google Scholar] [CrossRef]
- Stevens, G.A.; Singh, G.M.; Lu, Y.; Danaei, G.; Lin, J.K.; Finucane, M.M.; Bahalim, A.N.; McIntire, R.K.; Gutierrez, H.R.; Cowan, M.; et al. National, regional, and global trends in adult overweight and obesity prevalences. Popul. Health Metr. 2012, 10, 22. [Google Scholar] [CrossRef]
- Malmberg, K.; Yusuf, S.; Gerstein, H.C.; Brown, J.; Zhao, F.; Hunt, D.; Piegas, L.; Calvin, J.; Keltai, M.; Budaj, A. Impact of diabetes on long-term prognosis in patients with unstable angina and non-Q-wave myocardial infarction: Results of the OASIS (Organization to Assess Strategies for Ischemic Syndromes) Registry. Circulation 2000, 102, 1014–1019. [Google Scholar] [CrossRef]
- Franklin, K.; Goldberg, R.J.; Spencer, F.; Klein, W.; Budaj, A.; Brieger, D.; Marre, M.; Steg, P.G.; Gowda, N.; Gore, J.M. Implications of diabetes in patients with acute coronary syndromes. The Global Registry of Acute Coronary Events. Arch. Intern. Med. 2004, 164, 1457–1463. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.B.; Cheng, H.; Yue, T.; Ye, N.; Zhang, H.J.; Chen, Y.P. Derivation and validation of a prediction score for acute kidney injury secondary to acute myocardial infarction in Chinese patients. BMC Nephrol. 2019, 20, 195. [Google Scholar] [CrossRef]
- Fox, C.S.; Muntner, P.; Chen, A.Y.; Alexander, K.P.; Roe, M.T.; Wiviott, S.D. Short-term outcomes of acute myocardial infarction in patients with acute kidney injury: A report from the national cardiovascular data registry. Circulation 2012, 125, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Bruetto, R.G.; Rodrigues, F.B.; Torres, U.S.; Otaviano, A.P.; Zanetta, D.M.; Burdmann, E.A. Renal function at hospital admission and mortality due to acute kidney injury after myocardial infarction. PLoS ONE 2012, 7, e35496. [Google Scholar] [CrossRef]
- Kim, M.J.; Choi, H.S.; Oh, S.H.; Lee, H.C.; Kim, C.S.; Choi, J.S.; Park, J.W.; Bae, E.H.; Ma, S.K.; Kim, N.H.; et al. Impact of acute kidney injury on clinical outcomes after ST elevation acute myocardial infarction. Yonsei Med. J. 2011, 52, 603–609. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Skalsky, K.; Shiyovich, A.; Bental, T.; Vaknin-Assa, H.; Assali, A.; Gal, T.B.; Avraham, B.B.; Eisen, A.; Steinmetz, T.; Kornowski, R.; et al. Temporal trends of acute kidney injury in patients undergoing percutaneous coronary intervention over a span of 12 years. Int. J. Cardiol. 2021, 326, 44–48. [Google Scholar] [CrossRef]
- Yao, Z.F.; Shen, H.; Tang, M.N.; Yan, Y.; Ge, J.B. A novel risk assessment model of contrast-induced nephropathy after percutaneous coronary intervention in patients with diabetes. Basic Clin. Pharmacol. Toxicol. 2021, 128, 305–314. [Google Scholar] [CrossRef]
- Tsai, T.T.; Patel, U.D.; Chang, T.I.; Kennedy, K.F.; Masoudi, F.A.; Matheny, M.E.; Kosiborod, M.; Amin, A.P.; Messenger, J.C.; Rumsfeld, J.S.; et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: Insights from the NCDR Cath-PCI registry. JACC Cardiovasc. Interv. 2014, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zeng, J.F.; Chen, S.Q.; Ye, J.F.; Chen, Y.; Lei, L.; Liu, X.Q.; Liu, Y.; Wang, Y.; Lin, J.J.; Chen, J.Y. A simple risk score model for predicting contrast-induced nephropathy after coronary angiography in patients with diabetes. Clin. Exp. Nephrol. 2019, 23, 969–981. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Aymong, E.D.; Nikolsky, E.; Lasic, Z.; Iakovou, I.; Fahy, M.; Mintz, G.S.; Lansky, A.J.; Moses, J.W.; Stone, G.W.; et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: Development and initial validation. J. Am. Coll. Cardiol. 2004, 44, 1393–1399. [Google Scholar]
- Hammer, Y.; Eisen, A.; Hasdai, D.; Goldenberg, I.; Shlomo, N.; Cohen, T.; Beigel, R.; Kornowski, R.; Iakobishvili, Z. Comparison of Outcomes in Patients With Acute Coronary Syndrome Presenting With Typical Versus Atypical Symptoms. Am. J. Cardiol. 2019, 124, 1851–1856. [Google Scholar] [CrossRef]
- Shiyovich, A.; Shlomo, N.; Cohen, T.; Iakobishvili, Z.; Kornowski, R.; Eisen, A. Temporal trends of patients with acute coronary syndrome and multi-vessel coronary artery disease—From the ACSIS registry. Int. J. Cardiol. 2020, 304, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Skalsky, K.; Levi, A.; Bental, T.; Vaknin-Assa, H.; Assali, A.; Steinmetz, T.; Kornowski, R.; Perl, L. The Definition of "Acute Kidney Injury" Following Percutaneous Coronary Intervention and Cardiovascular Outcomes. Am. J. Cardiol. 2021, 156, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Keaney, J.J.; Hannon, C.M.; Murray, P.T. Contrast-induced acute kidney injury: How much contrast is safe? Nephrol. Dial. Transplant. 2013, 28, 1376–1383. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Rousan, T.A.; Pappy, R.M.; Chen, A.Y.; Roe, M.T.; Saucedo, J.F. Impact of diabetes mellitus on clinical characteristics, management, and in-hospital outcomes in patients with acute myocardial infarction (from the NCDR). Am. J. Cardiol. 2014, 114, 1136–1144. [Google Scholar] [CrossRef]
- Ranucci, M.; Castelvecchio, S.; Menicanti, L.; Frigiola, A.; Pelissero, G. Risk of assessing mortality risk in elective cardiac operations: Age, creatinine, ejection fraction, and the law of parsimony. Circulation 2009, 119, 3053–3061. [Google Scholar] [CrossRef]
- Maioli, M.; Toso, A.; Gallopin, M.; Leoncini, M.; Tedeschi, D.; Micheletti, C.; Bellandi, F. Preprocedural score for risk of contrast-induced nephropathy in elective coronary angiography and intervention. J. Cardiovasc. Med. 2010, 11, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.R.; DeVries, J.T.; Piper, W.D.; Robb, J.F.; Hearne, M.J.; Ver Lee, P.M.; Kellet, M.A.; Watkins, M.W.; Ryan, T.J.; Silver, M.T.; et al. Serious renal dysfunction after percutaneous coronary interventions can be predicted. Am. Heart J. 2008, 155, 260–266. [Google Scholar] [CrossRef]
- Li, Y.; Ren, K. The Mechanism of Contrast-Induced Acute Kidney Injury and Its Association with Diabetes Mellitus. Contrast Media Mol. Imaging 2020, 2020, 3295176. [Google Scholar] [CrossRef]
- Wang, C.; Pei, Y.Y.; Ma, Y.H.; Ma, X.L.; Liu, Z.W.; Zhu, J.H.; Li, C.S. Risk factors for acute kidney injury in patients with acute myocardial infarction. Chin. Med. J. 2019, 132, 1660–1665. [Google Scholar] [CrossRef]
- Sun, Y.B.; Liu, B.C.; Zou, Y.; Pan, J.R.; Tao, Y.; Yang, M. Risk factors of acute kidney injury after acute myocardial infarction. Ren. Fail. 2016, 38, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.B.; Tao, Y.; Yang, M. Assessing the influence of acute kidney injury on the mortality in patients with acute myocardial infarction: A clinical trail. Ren. Fail. 2018, 40, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Giacoppo, D.; Madhavan, M.V.; Baber, U.; Warren, J.; Bansilal, S.; Witzenbichler, B.; Dangas, G.D.; Kirtane, A.J.; Xu, K.; Kornowski, R.; et al. Impact of Contrast-Induced Acute Kidney Injury After Percutaneous Coronary Intervention on Short- and Long-Term Outcomes: Pooled Analysis From the HORIZONS-AMI and ACUITY Trials. Circ. Cardiovasc. Interv. 2015, 8, e002475. [Google Scholar] [CrossRef]
- Abusaada, K.; Yuan, C.; Sabzwari, R.; Butt, K.; Maqsood, A. Development of a novel score to predict the risk of acute kidney injury in patient with acute myocardial infarction. J. Nephrol. 2017, 30, 419–425. [Google Scholar] [CrossRef]
- Shacham, Y.; Leshem-Rubinow, E.; Gal-Oz, A.; Arbel, Y.; Keren, G.; Roth, A.; Steinvil, A. Acute Cardio-Renal Syndrome as a Cause for Renal Deterioration Among Myocardial Infarction Patients Treated With Primary Percutaneous Intervention. Can. J. Cardiol. 2015, 31, 1240–1244. [Google Scholar] [CrossRef] [PubMed]
- Shacham, Y.; Steinvil, A.; Arbel, Y. Acute kidney injury among ST elevation myocardial infarction patients treated by primary percutaneous coronary intervention: A multifactorial entity. J. Nephrol. 2016, 29, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Plakht, Y.; Gad Saad, S.N.; Gilutz, H.; Shiyovich, A. Potassium levels as a marker of imminent acute kidney injury among patients admitted with acute myocardial infarction. Soroka Acute Myocardial Infarction II (SAMI-II) Project. Int. J. Cardiol. 2021, 322, 214–219. [Google Scholar] [CrossRef]
- Heyman, S.N.; Rosenberger, C.; Rosen, S.; Khamaisi, M. Why is diabetes mellitus a risk factor for contrast-induced nephropathy? BioMed Res. Int. 2013, 2013, 123589. [Google Scholar] [CrossRef] [PubMed]
- Vallon, V. The proximal tubule in the pathophysiology of the diabetic kidney. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2011, 300, R1009–R1022. [Google Scholar] [CrossRef]
- Clark, B.A.; Kim, D.; Epstein, F.H. Endothelin and atrial natriuretic peptide levels following radiocontrast exposure in humans. Am. J. Kidney Dis. 1997, 30, 82–86. [Google Scholar] [CrossRef]
- Khamaisi, M.; Raz, I.; Shilo, V.; Shina, A.; Rosenberger, C.; Dahan, R.; Abassi, Z.; Meidan, R.; Lecht, S.; Heyman, S.N. Diabetes and radiocontrast media increase endothelin converting enzyme-1 in the kidney. Kidney Int. 2008, 74, 91–100. [Google Scholar] [CrossRef]
- Nechemia-Arbely, Y.; Khamaisi, M.; Rosenberger, C.; Koesters, R.; Shina, A.; Geva, C.; Shriki, A.; Klaus, S.; Rosen, S.; Rose-John, S.; et al. In vivo evidence suggesting reciprocal renal hypoxia-inducible factor-1 upregulation and signal transducer and activator of transcription 3 activation in response to hypoxic and non-hypoxic stimuli. Clin. Exp. Pharmacol. Physiol. 2013, 40, 262–272. [Google Scholar] [CrossRef]
- Carande, E.J.; Brown, K.; Jackson, D.; Maskell, N.; Kouzaris, L.; Greene, G.; Mikhail, A.; Obaid, D.R. Acute Kidney Injury Following Percutaneous Coronary Intervention for Acute Coronary Syndrome: Incidence, Aetiology, Risk Factors and Outcomes. Angiology 2021, 28, 00033197211040375. [Google Scholar] [CrossRef]
- Gupta, R.; Gurm, H.S.; Bhatt, D.L.; Chew, D.P.; Ellis, S.G. Renal failure after percutaneous coronary intervention is associated with high mortality. Catheter. Cardiovasc. Interv. 2005, 64, 442–448. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall | no-AKI_no_DM | no-AKI_DM | AKI_ no-DM | AKI_DM | p * | p ** | |
|---|---|---|---|---|---|---|---|
| n | 16,879 | 10,276 | 5587 | 503 | 513 | ||
| Baseline characteristics and demographics | |||||||
| Age, years (median [IQR) | 64 (54, 74) | 61 (52, 72) | 66 (57, 74) | 78 (69, 83) | 73 (65, 80) | <0.001 | <0.001 |
| Gender (male) | 13038 (77.2) | 8263 (80.4) | 4065 (72.8) | 363 (72.2) | 347 (67.6) | 0.13 | 0.015 |
| Higher education/ academic | 1455 (29.5) | 955 (32.9) | 438 (24.3) | 34 (35.4) | 28 (20.3) | 0.015 | 0.34 |
| Marital status: married | 6951 (78.4) | 4157 (79.2) | 2471 (79.1) | 135 (61.6) | 188 (68.6) | 0.13 | <0.001 |
| Dyslipidemia | 10968 (65.2) | 6053 (59.1) | 4304 (77.3) | 246 (49.1) | 365 (71.4) | <0.001 | 0.003 |
| Hypertension | 10035 (59.6) | 5087 (49.6) | 4190 (75.2) | 341 (67.8) | 417 (81.4) | <0.001 | 0.002 |
| Current smokers | 6303 (37.5) | 4384 (42.8) | 1704 (30.7) | 117 (23.4) | 98 (19.5) | 0.15 | <0.001 |
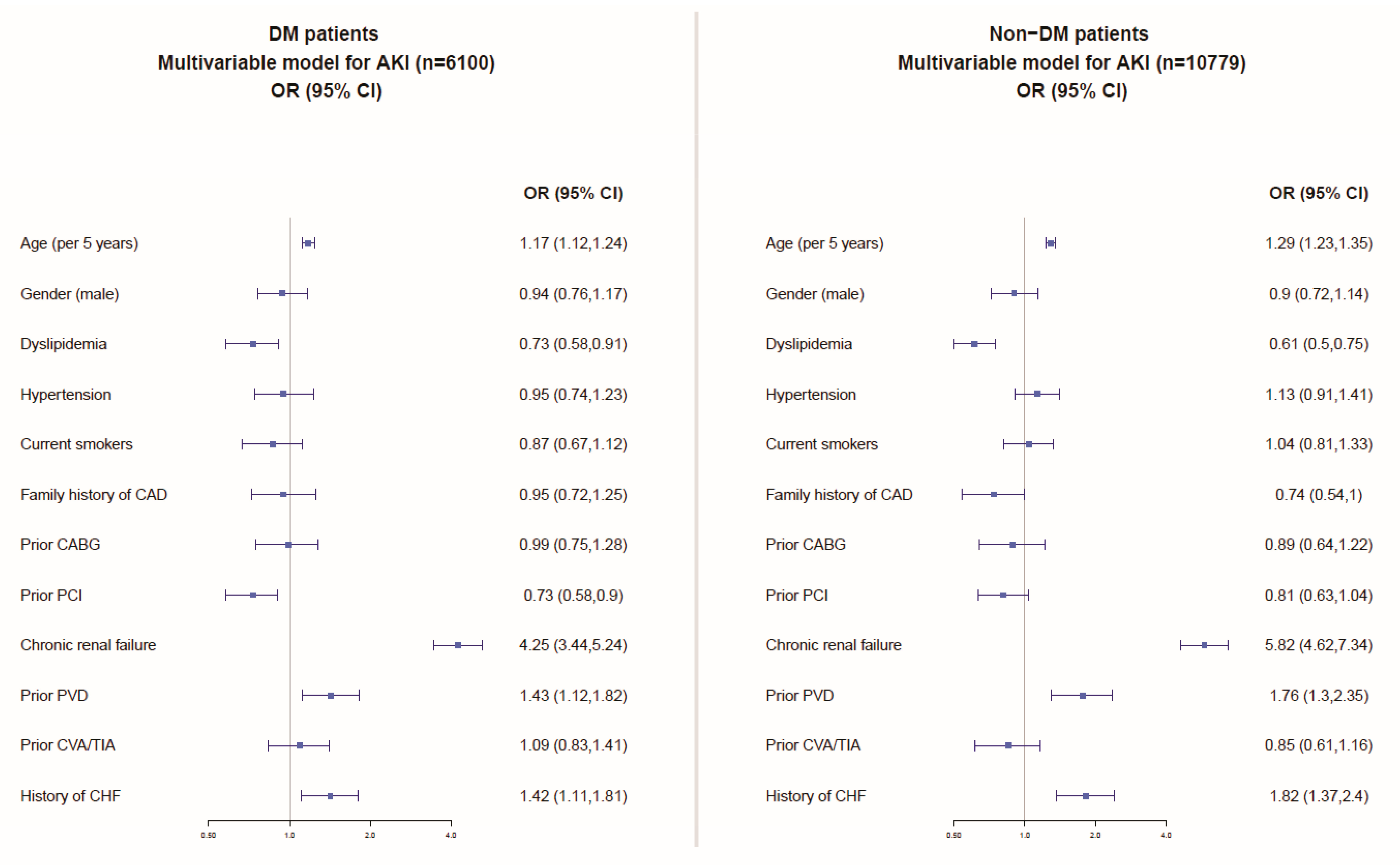
| Diabetes mellitus | 6100 (36.1) | 0 (0.0) | 5587 (100.0) | 0 (0.0) | 513 (100.0) | NA | NA |
| Family history of CAD | 4072 (26.0) | 2753 (28.3) | 1193 (23.7) | 54 (11.6) | 72 (16.1) | 0.062 | <0.001 |
| BMI (kg/m2), (median [IQR]) | 27 (25, 30) | 27 (24, 29) | 28 (25, 31) | 26 (24, 29) | 27 (25, 31) | <0.001 | 0.049 |
| Prior MI | 5275 (31.3) | 2646 (25.8) | 2224 (39.9) | 179 (35.7) | 226 (44.2) | 0.007 | 0.064 |
| Prior CABG | 1655 (9.8) | 724 (7.0) | 774 (13.9) | 61 (12.1) | 96 (18.8) | 0.005 | 0.003 |
| Prior PCI | 4765 (28.3) | 2363 (23.0) | 2115 (38.0) | 116 (23.1) | 171 (33.6) | <0.001 | 0.057 |
| Chronic renal failure | 1832 (10.9) | 559 (5.4) | 815 (14.6) | 207 (41.2) | 251 (49.0) | 0.014 | <0.001 |
| PVD | 1393 (8.3) | 513 (5.0) | 675 (12.1) | 83 (16.5) | 122 (23.9) | 0.004 | <0.001 |
| s/p CVA/TIA | 1373 (8.1) | 596 (5.8) | 631 (11.3) | 60 (11.9) | 86 (16.8) | 0.034 | <0.001 |
| History of CHF | 1363 (8.1) | 479 (4.7) | 651 (11.7) | 104 (20.7) | 129 (25.4) | 0.088 | <0.001 |
| Grace score > 140 | 1451 (15.0) | 576 (9.9) | 631 (19.0) | 116 (50.2) | 128 (44.3) | 0.2 | <0.001 |
| Earliest creatinine (mg/dL) (median [IQR]) | 1.00 (0.9, 1.2) | 1 (0.85, 1.1) | 1 (0.83, 1.3) | 1.7 (1.40, 2.3) | 1.8 (1.4, 2.6) | 0.12 | <0.001 |
| Medical therapy prior to admission | |||||||
| Aspirin | 7021 (47.8) | 3427 (38.4) | 3117 (63.5) | 196 (47.5) | 281 (64.6) | <0.001 | 0.7 |
| Clopidogrel | 1356 (9.4) | 591 (6.7) | 683 (14.2) | 31 (7.5) | 51 (11.8) | 0.05 | 0.19 |
| ACE-I | 3163 (31.3) | 1387 (23.0) | 1567 (44.2) | 81 (31.8) | 128 (43.5) | 0.006 | 0.87 |
| ARB | 1216 (12.5) | 501 (8.6) | 617 (18.1) | 23 (9.2) | 75 (26.0) | <0.001 | 0.001 |
| Beta blockers | 5335 (37.2) | 2625 (30.3) | 2322 (48.3) | 171 (42.3) | 217 (50.0) | 0.03 | 0.52 |
| Statins | 6601 (47.4) | 3245 (38.7) | 2956 (62.5) | 149 (38.1) | 251 (59.1) | <0.001 | 0.17 |
| Calcium channel blockers | 2989 (21.5) | 1380 (16.4) | 1338 (28.8) | 104 (26.1) | 167 (39.4) | <0.001 | <0.001 |
| Nitrates | 1531 (11.2) | 670 (8.0) | 685 (15.0) | 78 (19.6) | 98 (23.4) | 0.2 | <0.001 |
| Hypoglycemic agents | 3488 (23.1) | 34 (0.4) | 3192 (62.9) | 2 (0.5) | 260 (58.2) | <0.001 | 0.054 |
| Diuretics | 2066 (17.5) | 818 (11.5) | 987 (24.5) | 101 (28.9) | 160 (43.0) | <0.001 | <0.001 |
| Overall | no-AKI_no_DM | no-AKI_DM | AKI_ no-DM | AKI_DM | p * | p ** | |
|---|---|---|---|---|---|---|---|
| In-hospital complications | |||||||
| CHF mild-moderate (Killip-2) | 1544 (9.2) | 720 (7.0) | 570 (10.2) | 106 (21.5) | 148 (29.1) | 0.007 | <0.001 |
| Pulmonary oedema (Killip-3) | 1099 (6.5) | 360 (3.5) | 419 (7.5) | 155 (30.9) | 165 (32.2) | 0.7 | <0.001 |
| Cardiogenic shock (Killip-4) | 569 (3.4) | 200 (1.9) | 124 (2.2) | 137 (27.3) | 108 (21.1) | 0.03 | <0.001 |
| Hemodynamically significant RVI | 88 (0.8) | 39 (0.6) | 22 (0.6) | 10 (4.0) | 17 (5.6) | 0.5 | <0.001 |
| Reinfarction | 223 (1.3) | 106 (1.0) | 70 (1.3) | 24 (4.8) | 23 (4.5) | 0.95 | <0.001 |
| Post MI angina | 793 (4.7) | 463 (4.5) | 246 (4.4) | 33 (6.6) | 51 (10.0) | 0.07 | <0.001 |
| Stent thrombosis (definite/probable/possible) | 79 (0.7) | 46 (0.7) | 28 (0.7) | 2 (0.8) | 3 (1.0) | 1 | 0.87 |
| Free wall rupture | 59 (0.3) | 36 (0.4) | 15 (0.3) | 6 (1.2) | 2 (0.4) | 0.27 | 0.95 |
| Tamponade | 43 (0.3) | 25 (0.2) | 12 (0.2) | 4 (0.8) | 2 (0.4) | 0.66 | 0.76 |
| VSD | 20 (0.1) | 8 (0.1) | 5 (0.1) | 2 (0.4) | 5 (1.0) | 0.47 | <0.001 |
| MR moderate—severe | 323 (1.9) | 125 (1.2) | 96 (1.7) | 48 (9.6) | 54 (10.6) | 0.69 | <0.001 |
| Pericarditis | 107 (0.6) | 72 (0.7) | 23 (0.4) | 4 (0.8) | 8 (1.6) | 0.4 | 0.002 |
| Sustained VT (>125 bpm) | 247 (1.5) | 132 (1.3) | 54 (1.0) | 30 (6.0) | 31 (6.0) | 1 | <0.001 |
| Primary VF | 311 (1.8) | 225 (2.2) | 55 (1.0) | 18 (3.6) | 13 (2.5) | 0.43 | 0.003 |
| Secondary VF | 126 (0.7) | 62 (0.6) | 28 (0.5) | 20 (4.0) | 16 (3.1) | 0.56 | <0.001 |
| New A. Fib. | 895 (5.3) | 400 (3.9) | 265 (4.7) | 123 (24.5) | 107 (20.9) | 0.2 | <0.001 |
| High degree (2–3 degree) AV block | 382 (2.3) | 197 (1.9) | 106 (1.9) | 37 (7.4) | 42 (8.2) | 0.7 | <0.001 |
| Asystole | 359 (2.1) | 138 (1.3) | 81 (1.4) | 67 (13.3) | 73 (14.3) | 0.74 | <0.001 |
| Stroke | 103 (0.6) | 42 (0.4) | 36 (0.6) | 11 (2.2) | 14 (2.7) | 0.73 | <0.001 |
| Bleeding | 238 (1.4) | 99 (1.0) | 72 (1.3) | 33 (6.6) | 34 (6.6) | 1 | <0.001 |
| Blood transfusions | 170 (3.1) | 57 (1.8) | 54 (2.6) | 23 (18.9) | 36 (22.4) | 0.57 | <0.001 |
| Coronary angiography and PCI | |||||||
| PCI | 10,308 (61.1) | 6631 (64.5) | 3196 (57.2) | 237 (47.1) | 244 (47.6) | 0.94 | <0.001 |
| STEMI | 7659 (45.4) | 5087 (49.5) | 2114 (37.9) | 243 (48.3) | 215 (41.9) | 0.1 | <0.001 |
| Coronary angiography | 11,428 (87.2) | 7068 (89.7) | 3874 (85.7) | 230 (70.6) | 256 (68.4) | 0.6 | <0.001 |
| Medical therapy upon discharge | |||||||
| Aspirin | 15,557 (94.4) | 9665 (95.5) | 5163 (94.4) | 357 (80.2) | 372 (83.2) | 0.28 | <0.001 |
| P2Y12 | 11,926 (72.9) | 7504 (74.6) | 3923 (72.3) | 227 (51.6) | 272 (60.7) | 0.008 | <0.001 |
| Statins | 13,946 (85.2) | 8612 (85.6) | 4777 (88.0) | 256 (58.3) | 301 (67.3) | 0.007 | <0.001 |
| ACE-I/ARB | 12,029 (74.2) | 7139 (71.9) | 4412 (82.2) | 237 (51.9) | 241 (52.9) | 0.8 | <0.001 |
| Beta blockers | 12,873 (79.9) | 7910 (80.1) | 4416 (82.6) | 255 (57.4) | 292 (65.0) | 0.002 | <0.001 |
| Overall | no-AKI_no-DM | no-AKI_DM | AKI_ no-DM | AKI_DM | p * | p ** | |
| 30-day outcomes | |||||||
| Major adverse cardiac events | 2376 (14.1) | 1221 (11.9) | 744 (13.4) | 202 (40.3) | 209 (40.8) | 0.92 | <0.001 |
| mortality | 805 (4.8) | 290 (2.8) | 227 (4.1) | 148 (29.7) | 140 (27.4) | 0.45 | <0.001 |
| re-hospitalization | 2868 (18.9) | 1697 (18.1) | 1001 (19.9) | 83 (23.4) | 87 (23.8) | 0.99 | 0.09 |
| reinfarction | 286 (1.9) | 150 (1.7) | 92 (1.8) | 21 (5.0) | 23 (5.2) | 1 | <0.001 |
| Angina | 322 (4.0) | 189 (3.9) | 123 (4.3) | 5 (3.6) | 5 (2.8) | 0.91 | 0.4 |
| CABG | 1397 (8.4) | 785 (7.8) | 556 (10.1) | 30 (6.0) | 26 (5.2) | 0.69 | <0.001 |
| 1-year outcomes | |||||||
| mortality | 1580 (9.6) | 597 (6.0) | 540 (10.0) | 222 (44.8) | 221 (43.7) | 0.78 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiyovich, A.; Skalsky, K.; Steinmetz, T.; Ovdat, T.; Eisen, A.; Samara, A.; Beigel, R.; Gleitman, S.; Kornowski, R.; Orvin, K. Acute Kidney Injury Following Admission with Acute Coronary Syndrome: The Role of Diabetes Mellitus. J. Clin. Med. 2021, 10, 4931. https://doi.org/10.3390/jcm10214931
Shiyovich A, Skalsky K, Steinmetz T, Ovdat T, Eisen A, Samara A, Beigel R, Gleitman S, Kornowski R, Orvin K. Acute Kidney Injury Following Admission with Acute Coronary Syndrome: The Role of Diabetes Mellitus. Journal of Clinical Medicine. 2021; 10(21):4931. https://doi.org/10.3390/jcm10214931
Chicago/Turabian StyleShiyovich, Arthur, Keren Skalsky, Tali Steinmetz, Tal Ovdat, Alon Eisen, Abed Samara, Roy Beigel, Sagi Gleitman, Ran Kornowski, and Katia Orvin. 2021. "Acute Kidney Injury Following Admission with Acute Coronary Syndrome: The Role of Diabetes Mellitus" Journal of Clinical Medicine 10, no. 21: 4931. https://doi.org/10.3390/jcm10214931
APA StyleShiyovich, A., Skalsky, K., Steinmetz, T., Ovdat, T., Eisen, A., Samara, A., Beigel, R., Gleitman, S., Kornowski, R., & Orvin, K. (2021). Acute Kidney Injury Following Admission with Acute Coronary Syndrome: The Role of Diabetes Mellitus. Journal of Clinical Medicine, 10(21), 4931. https://doi.org/10.3390/jcm10214931