
The Association between Sarcoidosis and Ischemic Heart Disease—A Healthcare Analysis of a Large Israeli Population

 ,
,
Abstract
:1. Introduction
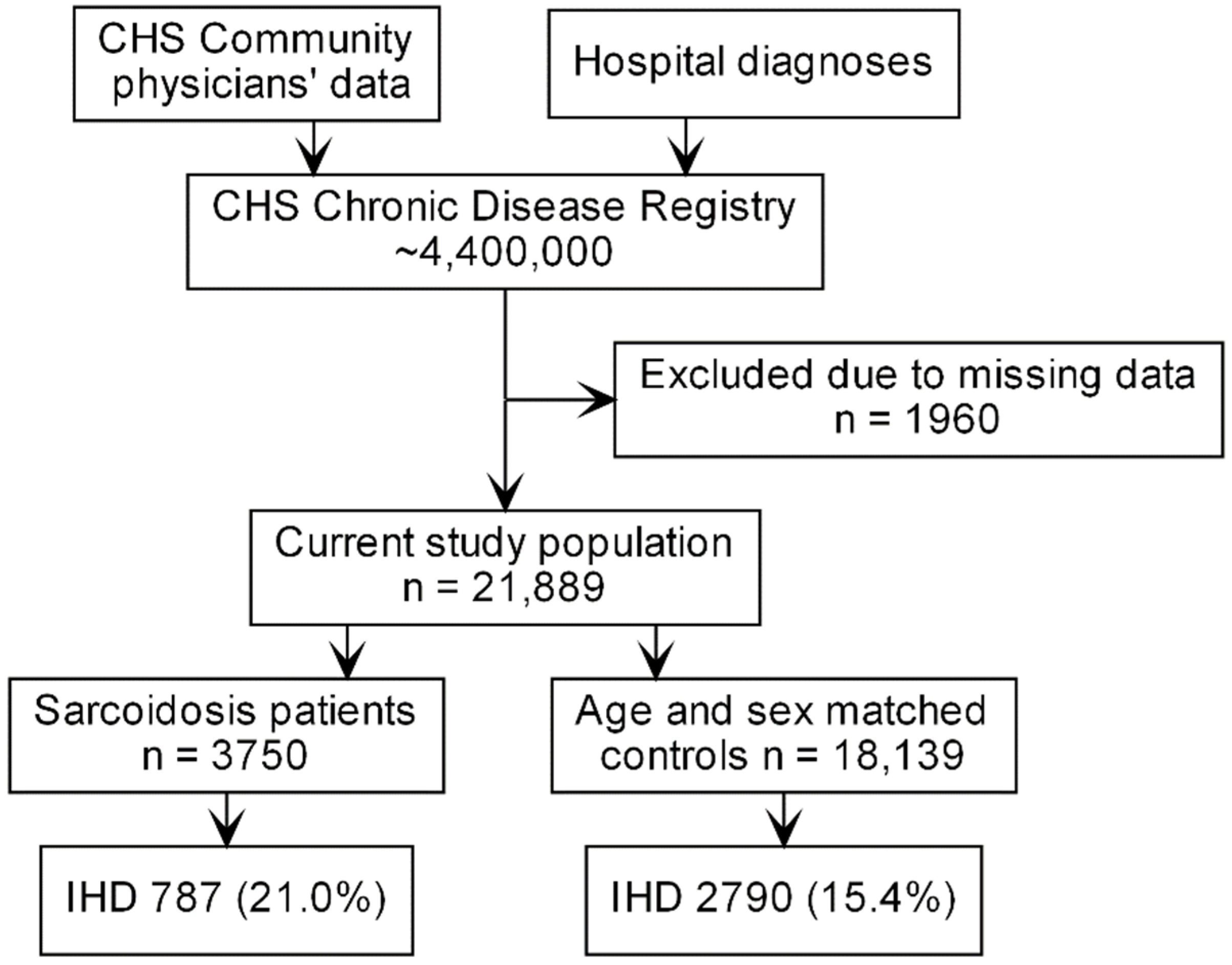
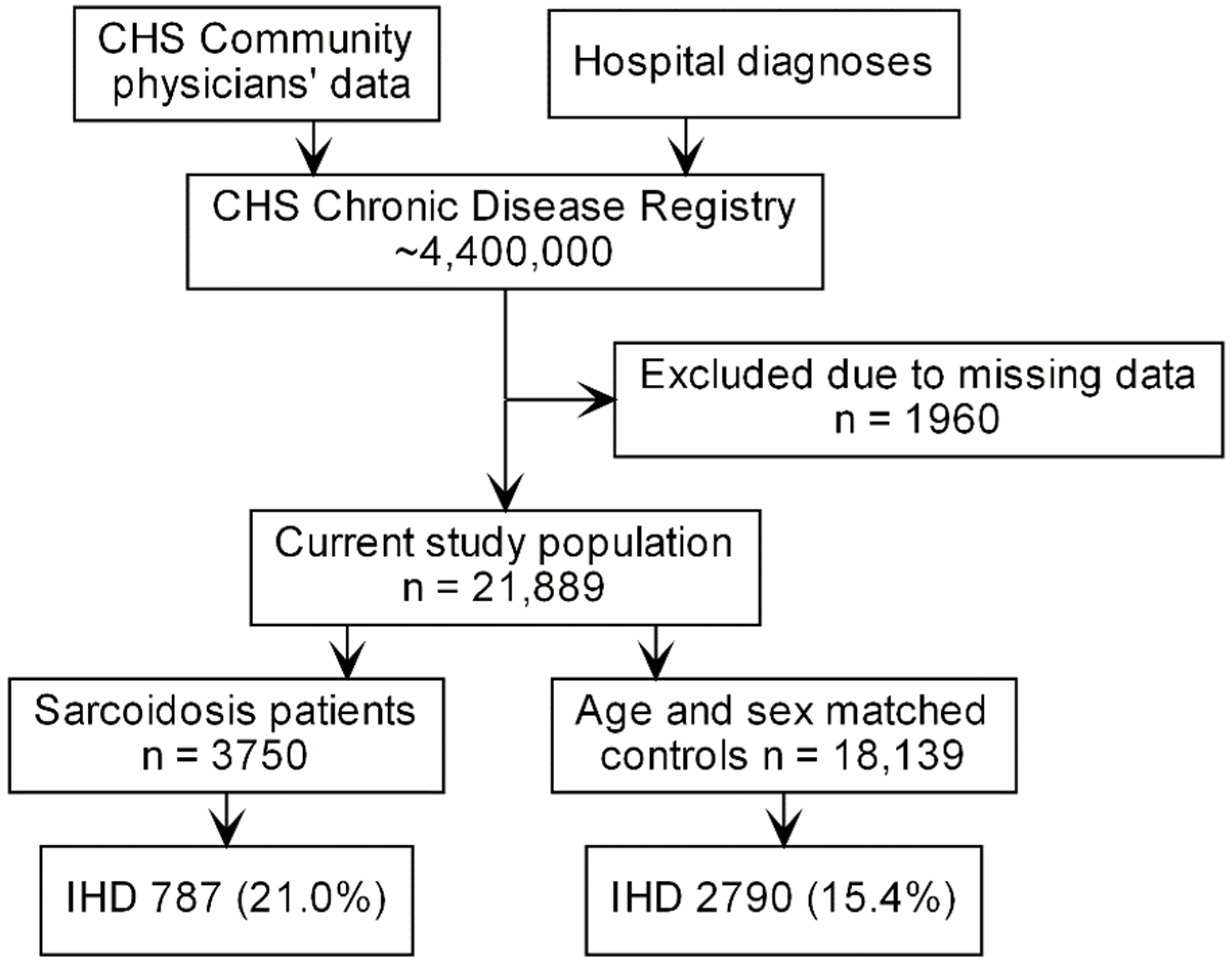
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. Available online: http://www.thelancet.com/gbd (accessed on 4 September 2021). [CrossRef] [Green Version]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; De Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics’ 2017 Update: A Report from the American Heart Association. Circulation 2017, 135, e146–e603. Available online: http://ahajournals.org (accessed on 4 September 2021). [CrossRef] [PubMed]
- Kaski, J.C.; Crea, F.; Gersh, B.J.; Camici, P.G. Reappraisal of ischemic heart disease: Fundamental role of coronary microvascular dysfunction in the pathogenesis of angina pectoris. Circulation 2018, 138, 1463–1480. Available online: https://pubmed.ncbi.nlm.nih.gov/30354347/ (accessed on 4 September 2021). [CrossRef] [PubMed]
- Willerson, J.T.; Ridker, P.M. Inflammation as a cardiovascular risk factor. Circulation 2004, 109, II-2. Available online: https://www.ahajournals.org/doi/full/10.1161/01.CIR.0000129535.04194.38 (accessed on 4 September 2021). [CrossRef] [Green Version]
- Bartova, J.; Sommerova, P.; Lyuya-Mi, Y.; Mysak, J.; Prochazkova, J.; Duskova, J.; Janatova, T.; Podzimek, S. Periodontitis as a risk factor of atherosclerosis. J. Immunol. Res. 2014, 2014, 636893. [Google Scholar] [CrossRef] [Green Version]
- Shoenfeld, Y.; Gerli, R.; Doria, A.; Matsuura, E.; Cerinic, M.M.; Ronda, N.; Jara, L.J.; Abu-Shakra, M.; Meroni, P.L.; Sherer, Y. Accelerated atherosclerosis in autoimmune rheumatic diseases. Circulation 2005, 112, 3337–3347. Available online: https://www.ahajournals.org/doi/full/10.1161/CIRCULATIONAHA.104.507996 (accessed on 4 September 2021). [CrossRef]
- Libby, P. Role of Inflammation in Atherosclerosis Associated with Rheumatoid Arthritis. Am. J. Med. 2008, 121, S21–S31. Available online: http://www.amjmed.com/article/S0002934308005925/fulltext (accessed on 4 September 2021). [CrossRef]
- Heinle, R.; Chang, C. Diagnostic criteria for sarcoidosis. Autoimmun. Rev. 2014, 13, 383–387. [Google Scholar] [CrossRef]
- Valeyre, D.; Prasse, A.; Nunes, H.; Uzunhan, Y.; Brillet, P.Y.; Müller-Quernheim, J. Sarcoidosis. Lancet 2014, 383, 1155–1167. Available online: https://pubmed.ncbi.nlm.nih.gov/24090799/ (accessed on 4 September 2021). [CrossRef]
- Swigris, J.J.; Olson, A.L.; Huie, T.J.; Fernandez-Perez, E.R.; Solomon, J.; Sprunger, D.; Brown, K.K. Sarcoidosis-related mortality in the United States from 1988 to 2007. Am. J. Respir. Crit. Care Med. 2011, 183, 1524–1530. Available online: https://pubmed.ncbi.nlm.nih.gov/21330454/ (accessed on 4 September 2021). [CrossRef]
- Etinger, R.; Comaneshter, D.; Amital, H.; Cohen, A.D.; Tiosano, S. The long-term prognostic significance of heart failure in sarcoidosis patients—A cohort study. Postgrad. Med. 2019, 133, 202–208. [Google Scholar] [CrossRef]
- Zöller, B.; Li, X.; Sundquist, J.; Sundquist, K. Risk of subsequent coronary heart disease in patients hospitalized for immune-mediated diseases: A nationwide follow-up study from Sweden. PLoS ONE 2012, 7, e33442. Available online: https://pubmed.ncbi.nlm.nih.gov/22438933/ (accessed on 4 September 2021). [CrossRef] [PubMed] [Green Version]
- Ungprasert, P.; Crowson, C.S.; Matteson, E.L. Risk of cardiovascular disease among patients with sarcoidosis: A population-based retrospective cohort study, 1976–2013. Eur. Respir. J. 2017, 49, 1601290. [Google Scholar] [CrossRef] [Green Version]
- Levi, E.H.; Watad, A.; Whitby, A.; Tiosano, S.; Comaneshter, D.; Cohen, A.D.; Amital, H. Coexistence of ischemic heart disease and rheumatoid arthritis patients—A case control study. Autoimmun. Rev. 2016, 15, 393–396. Available online: https://pubmed.ncbi.nlm.nih.gov/26808075/ (accessed on 4 September 2021). [CrossRef] [PubMed]
- Faurschou, M.; Mellemkjaer, L.; Starklint, H.; Kamper, A.L.; Tarp, U.; Voss, A.; Jacobsen, S. High Risk of Ischemic Heart Disease in Patients with Lupus Nephritis. J. Rheumatol. 2011, 38, 2400–2405. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Singh, H.; Loftus, E.V.; Pardi, D.S. Risk of Cerebrovascular Accidents and Ischemic Heart Disease in Patients With Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2014, 12, 382–393. [Google Scholar] [CrossRef]
- Yavne, Y.; Tiosano, S.; Watad, A.; Comaneshter, D.; Cohen, A.D.; Amital, H. Investigating the link between ischemic heart disease and Behcet’s disease: A cross-sectional analysis. Int. J. Cardiol. 2017, 241, 41–45. Available online: https://pubmed.ncbi.nlm.nih.gov/28285799/ (accessed on 4 September 2021). [CrossRef]
- Park, J.E.; Kim, Y.S.; Kang, M.J.; Kim, C.J.; Han, C.H.; Lee, S.M.; Park, S.C. Prevalence, incidence, and mortality of sarcoidosis in Korea, 2003–2015: A nationwide population-based study. Respir. Med. 2018, 144, S28–S34. [Google Scholar] [CrossRef]
- Rossides, M.; Kullberg, S.; Askling, J.; Eklund, A.; Grunewald, J.; Arkema, E.V. Sarcoidosis mortality in Sweden: A population-based cohort study. Eur. Respir. J. 2018, 51, 1701815. [Google Scholar] [CrossRef] [Green Version]
- Mirsaeidi, M.; Omar, H.R.; Ebrahimi, G.; Campos, M. The Association between ESR and CRP and Systemic Hypertension in Sarcoidosis. Int. J. Hypertens. 2016, 2016, 2402515. Available online: https://pubmed.ncbi.nlm.nih.gov/27433355/ (accessed on 4 September 2021). [CrossRef]
- Kim, J.S.; Judson, M.A.; Donnino, R.; Gold, M.; Cooper, L.T., Jr.; Prystowsky, E.N.; Prystowsky, S. Cardiac sarcoidosis. Am. Heart J. 2009, 157, 9–21. Available online: https://pubmed.ncbi.nlm.nih.gov/19081391/ (accessed on 4 September 2021). [CrossRef] [PubMed]
- Ward, E.V.; Nazari, J.; Edelman, R.R. Coronary artery vasculitis as a presentation of cardiac sarcoidosis. Circulation 2012, 125, 344–346. Available online: http://circ.ahajournals.org/lookup/suppl/doi:10.1161/CIRCULATIONAHA (accessed on 4 September 2021). [CrossRef] [Green Version]
- Butany, J.; Bahl, N.E.; Morales, K.; Thangaroopan, M.; Ross, H.; Rao, V.; Leong, S.W. The intricacies of cardiac sarcoidosis: A case report involving the coronary arteries and a review of the literature. Cardiovasc. Pathol. 2006, 15, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, A.R.; Dahy, A.; Dibas, M.; Abbas, A.S.; Ghozy, S.; El-Qushayri, A.E. Association between sarcoidosis and cardiovascular comorbidity: A systematic review and meta-analysis. Heart Lung 2020, 49, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Ungprasert, P.; Matteson, E.L.; Crowson, C.S. Reliability of Cardiovascular Risk Calculators to Estimate Accurately the Risk of Cardiovascular Disease in Patients With Sarcoidosis. Am. J. Cardiol. 2017, 120, 868–873. [Google Scholar] [CrossRef]
- Kul, S.; Kutlu, G.A.; Guvenc, T.S.; Kavas, M.; Demircioglu, K.; Yilmaz, Y.; Yakar, H.I.; Kanbay, A.; Boga, S.; Caliskan, M. Coronary flow reserve is reduced in sarcoidosis. Atherosclerosis 2017, 264, 115–121. [Google Scholar] [CrossRef]
- Taqueti, V.R.; di Carli, M.F. Clinical significance of noninvasive coronary flow reserve assessment in patients with ischemic heart disease. Curr. Opin. Cardiol. 2016, 31, 662–669. [Google Scholar] [CrossRef]
- Yong, W.C.; Sanguankeo, A.; Upala, S. Association between sarcoidosis, pulse wave velocity, and other measures of subclinical atherosclerosis: A systematic review and meta-analysis. Clin. Rheumatol. 2018, 37, 2825–2832. [Google Scholar] [CrossRef]
- Aciksari, G.; Kavas, M.; Atici, A.; Kul, S.; Erman, H.; Yilmaz, Y.; Demircioglu, K.; Yalcinkaya, E.; Kanbay, A.; Caliskan, M. Endocan Levels and Endothelial Dysfunction in Patients With Sarcoidosis. Angiology 2018, 69, 878–883. Available online: https://journals.sagepub.com/doi/full/10.1177/0003319718775283 (accessed on 4 September 2021). [CrossRef]
- Sitia, S.; Tomasoni, L.; Atzeni, F.; Ambrosio, G.; Cordiano, C.; Catapano, A.; Tramontana, S.; Perticone, F.; Naccarato, P.; Camici, P.; et al. From endothelial dysfunction to atherosclerosis. Autoimmun. Rev. 2010, 9, 830–834. Available online: https://pubmed.ncbi.nlm.nih.gov/20678595/ (accessed on 4 September 2021). [CrossRef]
- Santos-Gallego, C.G.; Weiss, A.J.; Sanz, J. Non-cardiac sarcoid actually affects the heart by reducing coronary flow reserve. Atherosclerosis 2017, 264, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Bargagli, E.; Rosi, E.; Pistolesi, M.; Lavorini, F.; Voltolini, L.; Rottoli, P. Increased Risk of Atherosclerosis in Patients with Sarcoidosis. Pathobiology 2017, 84, 258–263. Available online: www.karger.com/pat (accessed on 4 September 2021). [CrossRef] [PubMed] [Green Version]
- Seguro, L.P.C.; Rosario, C.; Shoenfeld, Y. Long-term complications of past glucocorticoid use. Autoimmun. Rev. 2013, 12, 629–632. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristic | Sarcoidosis (n = 3750) | Controls (n = 18,139) | p-Value |
|---|---|---|---|
| Age, years (mean ± SD) | 55.9 ± 14.8 | 56.3 ± 14.8 | 0.136 |
| Female gender | 2384 (63.6%) | 11,630 (64.1%) | 0.528 |
| BMI, kg/m2 (mean ± SD) | 28.7 (6.32) | 27.9 (5.78) | <0.001 |
| Socioeconomic status | |||
| Low | 1545 (41.7%) | 6789 (37.8%) | |
| Medium | 1491 (40.2%) | 7336 (40.9%) | 0.005 |
| High | 673 (18.1%) | 3828 (21.3%) | <0.001 |
| Systemic hypertension | 1926 (51.4%) | 8057 (44.4%) | <0.001 |
| Smoking | 1286 (34.3%) | 6542 (36.1%) | 0.039 |
| Characteristic | Odds Ratio | Confidence Interval | p-Value |
|---|---|---|---|
| Sarcoidosis | 1.5 | 1.36–1.66 | <0.001 |
| Age at diagnosis | 1.06 | 1.05–1.06 | <0.001 |
| Female gender | 0.39 | 0.35–0.42 | <0.001 |
| Body mass index * | |||
| 20–25 | 1.34 | 1.008–1.83 | 0.04 |
| 25–30 | 1.74 | 1.31–2.35 | <0.001 |
| >30 | 2.12 | 1.59–2.87 | <0.001 |
| Systemic hypertension | 4.26 | 3.84–4.72 | <0.001 |
| Smoking | 1.6 | 1.47–1.74 | <0.001 |
| Characteristic | Hazard Ratio | Confidence Interval | p-Value |
|---|---|---|---|
| Sarcoidosis | 1.93 | 1.76–2.13 | <0.001 |
| Age at diagnosis * | 1.1 | 1.09–1.10 | <0.001 |
| Female gender | 0.77 | 0.70–0.85 | <0.001 |
| Body mass index ** | |||
| 20–25 | 0.51 | 0.41–0.62 | <0.001 |
| 25–30 | 0.43 | 0.35–0.53 | <0.001 |
| >30 | 0.52 | 0.43–0.64 | <0.001 |
| Systemic hypertension | 1.36 | 1.22–1.52 | <0.001 |
| Smoking | 1.22 | 1.11–1.34 | <0.001 |
| Ischemic heart disease | 1.66 | 1.51–1.82 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonen, T.; Katz-Talmor, D.; Amital, H.; Comaneshter, D.; Cohen, A.D.; Tiosano, S. The Association between Sarcoidosis and Ischemic Heart Disease—A Healthcare Analysis of a Large Israeli Population. J. Clin. Med. 2021, 10, 5067. https://doi.org/10.3390/jcm10215067
Gonen T, Katz-Talmor D, Amital H, Comaneshter D, Cohen AD, Tiosano S. The Association between Sarcoidosis and Ischemic Heart Disease—A Healthcare Analysis of a Large Israeli Population. Journal of Clinical Medicine. 2021; 10(21):5067. https://doi.org/10.3390/jcm10215067
Chicago/Turabian StyleGonen, Tal, Daphna Katz-Talmor, Howard Amital, Doron Comaneshter, Arnon D. Cohen, and Shmuel Tiosano. 2021. "The Association between Sarcoidosis and Ischemic Heart Disease—A Healthcare Analysis of a Large Israeli Population" Journal of Clinical Medicine 10, no. 21: 5067. https://doi.org/10.3390/jcm10215067
APA StyleGonen, T., Katz-Talmor, D., Amital, H., Comaneshter, D., Cohen, A. D., & Tiosano, S. (2021). The Association between Sarcoidosis and Ischemic Heart Disease—A Healthcare Analysis of a Large Israeli Population. Journal of Clinical Medicine, 10(21), 5067. https://doi.org/10.3390/jcm10215067