
Machine Learning Algorithms Provide Greater Prediction of Response to SCS Than Lead Screening Trial: A Predictive AI-Based Multicenter Study

 ,
,  ,
,  ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
- -
- First, one can observe a lack of homogeneity among practices, making comparisons and recommendations regarding lead trialing very difficult: a patient can be trialed with a surgical lead (requiring an invasive approach) vs. a percutaneous trial, where one, two or three percutaneous lead(s) are placed in the spinal canal, under local sedation or general anesthesia [14,18]; the patient can be trialed from 3 to 28 days, depending on the healthcare system [22], which is responsible for significant differences in terms of lead trial complication rates [14]; during the trial, patients can test one, a few or hundreds of programs [18], which might affect the lead trial outcome, depending on the clinical expertise of the implanting team and trial duration. Ultimately, lead trialing could create a bias, since the trial cannot be blinded except in paresthesia-free techniques at the price of strict protocols, which cannot be standardized among practices, centers and countries, except for research purposes.
- -
- Lead trial outcomes have been reported using the Visual Analogue Scale (VAS) or Numeric Pain Rating Scale (NPRS). Based on these assessments, guidelines recommend that a refractory PSPS patient can be eligible to permanent implant, if a 30–50% pain decrease is observed during the trial [14,16,17,19]. It appears that this unidimensional modality of pain assessment can no longer be considered as the only gold standard to delineate the implanting physician’s guidelines and international recommendations, since this would reflect only one dimension of the patient’s quality of life, needs and expectations [23]. While composite multidimensional pain indexes, following the application of pain therapy on chronic refractory patients [23], would help to capture the essence of pain substrate and pain potential relief, they are not currently part of the recommended pain assessment toolbox.
- -
- Third, it appears that patient selection, final implantation ratio and patient outcomes, with or without lead trial, are similar [24]. Indeed, several studies have evaluated the ability of the screening trial to predict the long-term efficacy of SCS [24,25,26]. In a multicentric randomized controlled trial, Eldabe et al. [24] compared pain relief at 6-month follow-up between 54 patients who underwent a screening trial and 51 patients who did not. They found no significant difference regarding pain relief between groups. Furthermore, they reported that the diagnostic accuracy of the screening trial presented sensitivity of 100% (percentage of patients with a positive screening trial among responders) and specificity of 17% (percentage of patients with a negative screening trial among non-responders). All in all, the authors concluded that outcomes do not differ with or without the screening trial, and that the screening trial was not able to identify long-term non-responders.
- -
- Fourth, it has been shown that infection rates during SCS trials increase logarithmically within time, after 14 days of trialing, and can compromise the therapy [14].
2. Materials and Methods
2.1. Patient Data
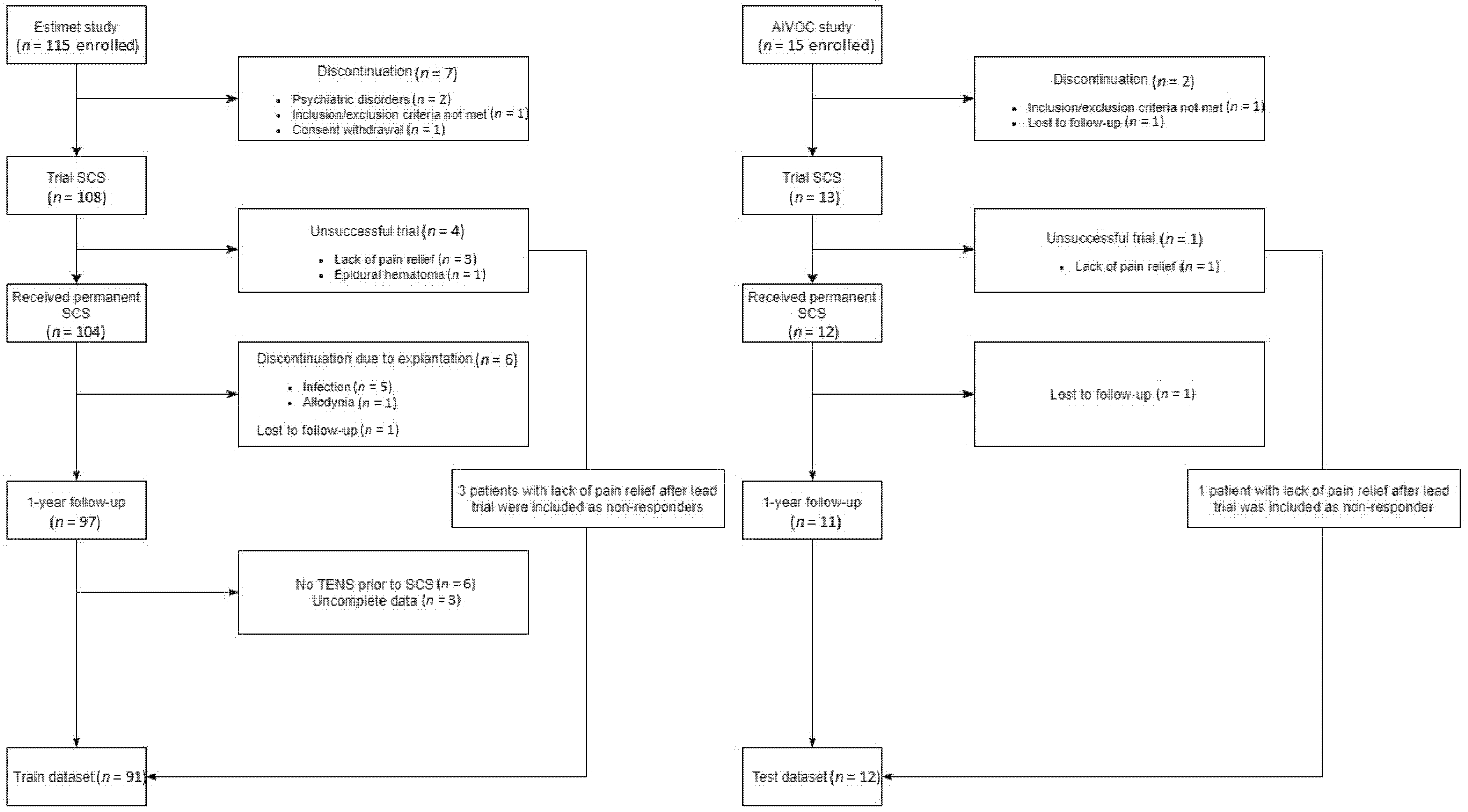
2.1.1. First Dataset
2.1.2. Second Dataset
2.2. Studied Variables
2.2.1. Primary Outcome
2.2.2. Predictors
2.3. Statistical Methods
2.3.1. Descriptive Analysis
2.3.2. Multivariate Analysis
2.4. Testing Data and Model Assessment
2.5. External Validation
3. Results
3.1. Descriptive Analysis
3.2. Training Data Results (Internal Validation)
3.3. External Validation
3.4. Model Interpretability
4. Discussion
4.1. Potential Added Value of a Predictive Model vs. Lead Trialing
4.2. Machine Learning Model Accuracy to Predict SCS Efficacy
4.3. SCS Predictors of Lead Trial Success and SCS Long-Term Outcomes
4.4. Study Strengths and Limitations
- -
- A double dataset, extracted from prospective comparative studies, comprising a large sample size, to reduce biases typically associated with this type of research and to ensure the maximal potential of generalization of our predictive models.
- -
- The multicenter nature of our sample also helps to ensure generalizability and applicability to clinical practice.
- -
- The development of a composite outcome, based on objective methods, which might lead to optimize patient satisfaction evaluation and, therefore, more precisely capture patient needs and expectations so as to define what should be considered as a positive outcome. However, two patients presented positive predictions related to significant “negative” results. While these patients had good outcomes for leg pain, back pain still remained unrelieved, altering the results of the global pain assessment. This highlights the relevance of assessing both global pain and individual pain areas in order to avoid misinterpretation of the overall assessment [60].
4.4.1. Paresthesia Intolerance
4.4.2. Country-Dependent Variety of SCS Practices
4.4.3. Large-Scale Validation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- North, R.B.; Campbell, J.N.; James, C.S.; Conover-Walker, M.K.; Wang, H.; Piantadosi, S.; Rybock, J.D.; Long, D.M. Failed Back Surgery Syndrome: 5-Year Follow-up in 102 Patients Undergoing Repeated Operation. Neurosurgery 1991, 28, 685–690; discussion 690–691. [Google Scholar] [CrossRef] [PubMed]
- Schug, S.A.; Lavand’homme, P.; Barke, A.; Korwisi, B.; Rief, W.; Treede, R.-D. IASP Taskforce for the Classification of Chronic Pain The IASP Classification of Chronic Pain for ICD-11: Chronic Postsurgical or Posttraumatic Pain. Pain 2019, 160, 45–52. [Google Scholar] [CrossRef]
- Christelis, N.; Simpson, B.; Russo, M.; Stanton-Hicks, M.; Barolat, G.; Thomson, S.; Schug, S.; Baron, R.; Buchser, E.; Carr, D.B.; et al. Persistent Spinal Pain Syndrome: A Proposal for Failed Back Surgery Syndrome and ICD-11. Pain Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Ganty, P.; Sharma, M. Failed Back Surgery Syndrome: A Suggested Algorithm of Care. Br. J. Pain 2012, 6, 153–161. [Google Scholar] [CrossRef] [Green Version]
- Law, J.D.; Lehman, R.A.; Kirsch, W.M. Reoperation after Lumbar Intervertebral Disc Surgery. J. Neurosurg. 1978, 48, 259–263. [Google Scholar] [CrossRef]
- Lehmann, T.R.; LaRocca, H.S. Repeat Lumbar Surgery. A Review of Patients with Failure from Previous Lumbar Surgery Treated by Spinal Canal Exploration and Lumbar Spinal Fusion. Spine 1981, 6, 615–619. [Google Scholar] [CrossRef]
- Naiditch, N.; Billot, M.; Moens, M.; Goudman, L.; Cornet, P.; Le Breton, D.; Roulaud, M.; Ounajim, A.; Page, P.; Lorgeoux, B.; et al. Persistent Spinal Pain Syndrome Type 2 (PSPS-T2), a Social Pain? Advocacy for a Social Gradient of Health Approach to Chronic Pain. J. Clin. Med. 2021, 10, 2817. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Kamiya, M.; Nishihara, M.; Arai, Y.-C.P.; Ikemoto, T.; Ushida, T. Prevalence, Characteristics, and Burden of Failed Back Surgery Syndrome: The Influence of Various Residual Symptoms on Patient Satisfaction and Quality of Life as Assessed by a Nationwide Internet Survey in Japan. J. Pain Res. 2017, 10, 811–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farber, S.H.; Han, J.L.; Elsamadicy, A.A.; Hussaini, Q.; Yang, S.; Pagadala, P.; Parente, B.; Xie, J.; Lad, S.P. Long-Term Cost Utility of Spinal Cord Stimulation in Patients with Failed Back Surgery Syndrome. Pain Physician 2017, 20, E797–E805. [Google Scholar] [PubMed]
- Kumar, K.; Taylor, R.S.; Jacques, L.; Eldabe, S.; Meglio, M.; Molet, J.; Thomson, S.; O’Callaghan, J.; Eisenberg, E.; Milbouw, G.; et al. The Effects of Spinal Cord Stimulation in Neuropathic Pain Are Sustained: A 24-Month Follow-up of the Prospective Randomized Controlled Multicenter Trial of the Effectiveness of Spinal Cord Stimulation. Neurosurgery 2008, 63, 762–770; discussion 770. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Ryan, J.; O’Donnell, R.; Eldabe, S.; Kumar, K.; North, R.B. The Cost-Effectiveness of Spinal Cord Stimulation in the Treatment of Failed Back Surgery Syndrome. Clin. J. Pain 2010, 26, 463–469. [Google Scholar] [CrossRef]
- Eldabe, S.S.; Taylor, R.S.; Goossens, S.; Bouche, B.; Gültuna, I.; Green, C.; Tinsley, J.; Luyet, P.; Buchser, E. A Randomized Controlled Trial of Subcutaneous Nerve Stimulation for Back Pain Due to Failed Back Surgery Syndrome: The SubQStim Study. Neuromodulation 2019, 22, 519–528. [Google Scholar] [CrossRef] [Green Version]
- North, R.B.; Kidd, D.H.; Farrokhi, F.; Piantadosi, S.A. Spinal Cord Stimulation versus Repeated Lumbosacral Spine Surgery for Chronic Pain: A Randomized, Controlled Trial. Neurosurgery 2005, 56, 98–107. [Google Scholar] [CrossRef] [Green Version]
- Rigoard, P.; Basu, S.; Desai, M.; Taylor, R.; Annemans, L.; Tan, Y.; Johnson, M.J.; Van den Abeele, C.; North, R. PROMISE Study Group Multicolumn Spinal Cord Stimulation for Predominant Back Pain in Failed Back Surgery Syndrome Patients: A Multicenter Randomized Controlled Trial. Pain 2019, 160, 1410–1420. [Google Scholar] [CrossRef]
- Ounajim, A.; Billot, M.; Louis, P.-Y.; Slaoui, Y.; Frasca, D.; Goudman, L.; Roulaud, M.; Naiditch, N.; Lorgeoux, B.; Baron, S.; et al. Finite Mixture Models Based on Pain Intensity, Functional Disability and Psychological Distress Composite Assessment Allow Identification of Two Distinct Classes of Persistent Spinal Pain Syndrome after Surgery Patients Related to Their Quality of Life. J. Clin. Med. 2021, 10, 4676. [Google Scholar] [CrossRef]
- National Institute for Health and Clinical Excellence Spinal Cord Stimulation for Chronic Pain of Neuropathic or Ischaemic Origin. Available online: https://www.nice.org.uk/guidance/ta159 (accessed on 21 July 2021).
- Centers for Medicare & Medicaid Services National Coverage Determination (NCD) for Electrical Nerve Stimulators. 160:7. Available online: https://www.cms.gov/medicare-coverage-database/view/ncd.aspx?NCDId=240 (accessed on 21 July 2021).
- Rigoard, P.; Billot, M.; Ingrand, P.; Durand-Zaleski, I.; Roulaud, M.; Peruzzi, P.; Dam Hieu, P.; Voirin, J.; Raoul, S.; Page, P.; et al. How Should We Use Multicolumn Spinal Cord Stimulation to Optimize Back Pain Spatial Neural Targeting? A Prospective, Multicenter, Randomized, Double-Blind, Controlled Trial (ESTIMET Study). Neuromodulation 2020. [Google Scholar] [CrossRef] [PubMed]
- HAUTE AUTORITE DE SANTE Evaluation Des Systèmes Implantables de Neurostimulation Médullaire. Available online: https://www.hassante.fr/upload/docs/application/pdf/2014-04/fiche_de_bon_usage_neurostimulation_2014-04-03_10-38-24_855.pdf (accessed on 21 July 2021).
- Deer, T.R.; Lamer, T.J.; Pope, J.E.; Falowski, S.M.; Provenzano, D.A.; Slavin, K.; Golovac, S.; Arle, J.; Rosenow, J.M.; Williams, K.; et al. The Neurostimulation Appropriateness Consensus Committee (NACC) Safety Guidelines for the Reduction of Severe Neurological Injury. Neuromodulation Technol. Neural Interface 2017, 20, 15–30. [Google Scholar] [CrossRef]
- Thomson, S.; Huygen, F.; Prangnell, S.; De Andrés, J.; Baranidharan, G.; Belaïd, H.; Berry, N.; Billet, B.; Cooil, J.; De Carolis, G.; et al. Appropriate Referral and Selection of Patients with Chronic Pain for Spinal Cord Stimulation: European Consensus Recommendations and E-health Tool. Eur. J. Pain 2020, 24, 1169–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Buyten, J.P.; Van Zundert, J.; Vueghs, P.; Vanduffel, L. Efficacy of Spinal Cord Stimulation: 10 Years of Experience in a Pain Centre in Belgium. Eur. J. Pain 2001, 5, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Rigoard, P.; Ounajim, A.; Goudman, L.; Louis, P.-Y.; Slaoui, Y.; Roulaud, M.; Naiditch, N.; Bouche, B.; Page, P.; Lorgeoux, B.; et al. A Novel Multi-Dimensional Clinical Response Index Dedicated to Improving Global Assessment of Pain in Patients with Persistent Spinal Pain Syndrome After Spinal Surgery, Based on a Real-Life Prospective Multicentric Study (PREDIBACK) and Machine Learning. Preprints 2021. [Google Scholar] [CrossRef]
- Eldabe, S.; Duarte, R.V.; Gulve, A.; Thomson, S.; Baranidharan, G.; Houten, R.; Jowett, S.; Sandhu, H.; Chadwick, R.; Brookes, M.; et al. Does a Screening Trial for Spinal Cord Stimulation in Patients with Chronic Pain of Neuropathic Origin Have Clinical Utility and Cost-Effectiveness (TRIAL-STIM)? A Randomised Controlled Trial. Pain 2020, 161, 2820–2829. [Google Scholar] [CrossRef]
- Weinand, M.E.; Madhusudan, H.; Davis, B.; Melgar, M. Acute vs. Prolonged Screening for Spinal Cord Stimulation in Chronic Pain. Neuromodulation 2003, 6, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, T.; Sharma, S.; Aner, M.; Gill, J.S. A Temporary vs. Permanent Anchored Percutaneous Lead Trial of Spinal Cord Stimulation: A Comparison of Patient Outcomes and Adverse Events. Neuromodulation 2018, 21, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Bendersky, D.; Yampolsky, C. Is Spinal Cord Stimulation Safe? A Review of Its Complications. World Neurosurg. 2014, 82, 1359–1368. [Google Scholar] [CrossRef] [PubMed]
- North, R.; Desai, M.J.; Vangeneugden, J.; Raftopoulos, C.; Van Havenbergh, T.; Deruytter, M.; Remacle, J.; Shipley, J.; Tan, Y.; Johnson, M.J.; et al. Postoperative Infections Associated with Prolonged Spinal Cord Stimulation Trial Duration (PROMISE RCT). Neuromodulation 2020, 23, 620–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strauss, I.; Taha, K.; Krishna, V.; Hodaie, M. Younger Age Predicts Greater Effectiveness of Spinal Cord Stimulation for Chronic Pain. Acta Neurochir. 2016, 158, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Celestin, J.; Edwards, R.R.; Jamison, R.N. Pretreatment Psychosocial Variables as Predictors of Outcomes Following Lumbar Surgery and Spinal Cord Stimulation: A Systematic Review and Literature Synthesis. Pain Med. 2009, 10, 639–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caylor, J.; Reddy, R.; Yin, S.; Cui, C.; Huang, M.; Huang, C.; Rao, R.; Baker, D.G.; Simmons, A.; Souza, D.; et al. Spinal Cord Stimulation in Chronic Pain: Evidence and Theory for Mechanisms of Action. Bioelectron. Med. 2019, 5, 12. [Google Scholar] [CrossRef]
- Mekhail, N.; Mehanny, D.S.; Armanyous, S.; Costandi, S.; Saweris, Y.; Azer, G.; Bolash, R. Choice of Spinal Cord Stimulation versus Targeted Drug Delivery in the Management of Chronic Pain: A Predictive Formula for Outcomes. Reg. Anesth. Pain Med. 2020, 45, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Campbell, C.M.; Jamison, R.N.; Edwards, R.R. Psychological Screening/Phenotyping as Predictors for Spinal Cord Stimulation. Curr. Pain Headache Rep. 2013, 17, 307. [Google Scholar] [CrossRef]
- Bendinger, T.; Plunkett, N.; Poole, D.; Turnbull, D. Psychological Factors as Outcome Predictors for Spinal Cord Stimulation. Neuromodulation 2015, 18, 465–471; discussion 471. [Google Scholar] [CrossRef]
- Sparkes, E.; Duarte, R.V.; Mann, S.; Lawrence, T.R.; Raphael, J.H. Analysis of Psychological Characteristics Impacting Spinal Cord Stimulation Treatment Outcomes: A Prospective Assessment. Pain Physician 2015, 18, E369–E377. [Google Scholar] [PubMed]
- Taylor, R.S.; Desai, M.J.; Rigoard, P.; Taylor, R.J. Predictors of Pain Relief Following Spinal Cord Stimulation in Chronic Back and Leg Pain and Failed Back Surgery Syndrome: A Systematic Review and Meta-Regression Analysis. Pain Pract. 2014, 14, 489–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, K.; Rizvi, S.; Nguyen, R.; Abbas, M.; Bishop, S.; Murthy, V. Impact of Wait Times on Spinal Cord Stimulation Therapy Outcomes. Pain Pract. 2014, 14, 709–720. [Google Scholar] [CrossRef]
- Goudman, L.; Van Buyten, J.-P.; De Smedt, A.; Smet, I.; Devos, M.; Jerjir, A.; Moens, M. Predicting the Response of High Frequency Spinal Cord Stimulation in Patients with Failed Back Surgery Syndrome: A Retrospective Study with Machine Learning Techniques. J. Clin. Med. 2020, 9, 4131. [Google Scholar] [CrossRef] [PubMed]
- Brooks, R. EuroQol: The Current State of Play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef]
- Fairbank, J.C.; Couper, J.; Davies, J.B.; O’Brien, J.P. The Oswestry Low Back Pain Disability Questionnaire. Physiotherapy 1980, 66, 271–273. [Google Scholar] [PubMed]
- Montgomery, S.A.; Asberg, M. A New Depression Scale Designed to Be Sensitive to Change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef]
- Marola, O.; Cherala, R.; Prusik, J.; Kumar, V.; Fama, C.; Wilock, M.; Crimmins, J.; Pilitsis, J.G. BMI as a Predictor of Spinal Cord Stimulation Success in Chronic Pain Patients. Neuromodulation 2017, 20, 269–273. [Google Scholar] [CrossRef]
- Van Eijs, F.; Smits, H.; Geurts, J.W.; Kessels, A.G.H.; Kemler, M.A.; van Kleef, M.; Joosten, E.A.J.; Faber, C.G. Brush-Evoked Allodynia Predicts Outcome of Spinal Cord Stimulation in Complex Regional Pain Syndrome Type 1. Eur. J. Pain 2010, 14, 164–169. [Google Scholar] [CrossRef]
- Mathew, L.; Winfree, C.; Miller-Saultz, D.; Sonty, N. Transcutaneous Electrical Nerve Stimulator Trial May Be Used as a Screening Tool Prior to Spinal Cord Stimulator Implantation. Pain 2010, 150, 327–331. [Google Scholar] [CrossRef]
- Goudman, L.; De Smedt, A.; Eldabe, S.; Rigoard, P.; Linderoth, B.; De Jaeger, M.; Moens, M.; Consortium, D. High-Dose Spinal Cord Stimulation for Patients with Failed Back Surgery Syndrome: A Multicenter Effectiveness and Prediction Study. Pain 2020, in press. [Google Scholar] [CrossRef]
- Friedman, J.H.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Hearst, M.A.; Dumais, S.T.; Osuna, E.; Platt, J.; Scholkopf, B. Support Vector Machines. IEEE Intell. Syst. Appl. 1998, 13, 18–28. [Google Scholar] [CrossRef] [Green Version]
- Meyer, D.; Dimitriadou, E.; Hornik, K.; Weingessel, A.; Leisch, F.; Chang, C.C.; Lin, C.C. libsvm E1071: Misc Functions of the Department of Statistics, Probability Theory Group (Formerly: E1071); TU Wien: Vienna, Austria, 2020. [Google Scholar]
- Friedman, N.; Geiger, D.; Goldszmidt, M. Bayesian Network Classifiers. Mach. Learn. 1997, 29, 131–163. [Google Scholar] [CrossRef] [Green Version]
- Haykin, S. Neural Networks: A Comprehensive Foundation, 2nd ed.; Prentice Hall PTR: Hoboken, NJ, USA, 1998; ISBN 978-0-13-273350-2. [Google Scholar]
- Arnold, T.B. KerasR: R Interface to the Keras Deep Learning Library. J. Open Source Softw. 2017. [Google Scholar] [CrossRef] [Green Version]
- Therneau, T.; Atkinson, B.; Ripley, B. Rpart: Recursive Partitioning and Regression Trees. 2019. Available online: http://CRAN.R-project.org/package=rpart (accessed on 2 September 2019).
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Wright, M.N.; Wager, S.; Probst, P. Ranger: A Fast Implementation of Random Forests. 2020. Available online: https://CRAN.R-project.org/package=ranger (accessed on 6 March 2020).
- Friedman, J.H. Stochastic Gradient Boosting. Comput. Stat. Data Anal. 2002, 38, 367–378. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar] [CrossRef] [Green Version]
- Rudiger, J.; Thomson, S. Infection Rate of Spinal Cord Stimulators After a Screening Trial Period. A 53-Month Third Party Follow-Up. Neuromodul. Technol. Neural Interface 2011, 14, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Naiditch, N.; Billot, M.; Goudman, L.; Cornet, P.; Roulaud, M.; Ounajim, A.; Page, P.; Lorgeoux, B.; Baron, S.; Nivole, K.; et al. Professional Status of Persistant Spinal Pain Syndrome Patients after Spinal Surgery (PSPS-T2): What Does Really Matter? A pro-Spective Study Introducing the Concept of “Adapted Profession-al Activity” Infering from Clinical, Psychological and Social influence. J. Clin. Med. 2021, Submitted. [Google Scholar]
- Bouhassira, D.; Attal, N.; Fermanian, J.; Alchaar, H.; Gautron, M.; Masquelier, E.; Rostaing, S.; Lanteri-Minet, M.; Collin, E.; Grisart, J.; et al. Development and Validation of the Neuropathic Pain Symptom Inventory. Pain 2004, 108, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Rigoard, P.; Nivole, K.; Blouin, P.; Monlezun, O.; Roulaud, M.; Lorgeoux, B.; Bataille, B.; Guetarni, F. A Novel, Objective, Quantitative Method of Evaluation of the Back Pain Component Using Comparative Computerized Multi-Parametric Tactile Mapping before/after Spinal Cord Stimulation and Database Analysis: The “Neuro-Pain’t” Software. Neurochirurgie 2015, 61 (Suppl. 1), S99–S108. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographics | Train Set Descriptive Statistics | Test Set Descriptive Statistics |
|---|---|---|
| Profession | ||
| Blue-collar job | 9 (9.9%) | 1 (8.3%) |
| White-collar job | 39 (42.8%) | 4 (33.3%) |
| Craftsman, shopkeeper, business | 5 (5.5%) | 2 (16.7%) |
| owner | ||
| Executive | 2 (2.2%) | 0 |
| Disability | 6 (6.6%) | 0 |
| Intermediate profession | 4 (4.4%) | 0 |
| Retired | 6 (6.6%) | 4 (33.3%) |
| Without professional activity | 14 (15.4%) | 1 (8.3%) |
| Other | ||
| 11 | 6 (6.6%) | 0 (0%) |
| Work stopage | ||
| Yes | 60 (65.9%) | Not available |
| No | 16 (17.6%) | Not available |
| Unemployed | 8 (8.8%) | Not available |
| Retired and other | 7 (7.7%) | Not available |
| Pain history and management | ||
| Number of spinal surgeries | ||
| 1 | 44 (48.4%) | 8 (66.7%) |
| 2 | 24 (26.4%) | 2 (16.7%) |
| 3 | 13 (14.3%) | 2 (16.7%) |
| 4 | 6 (6.6%) | 0 (0%) |
| 5 | 3 (3.3%) | 0 (0%) |
| Unknown | 1 (1.1%) | 0 (0%) |
| Type of spinal surgeries | ||
| Decompression | 69 (75.8%) | 8 (66.7%) |
| Fusion | 8 (8.8%) | 2 (16.7%) |
| Decompression AND fusion | 14 (15.4%) | 0 (0%) |
| Unknown | 0 (0%) | 2 (16.7%) |
| Pain management with kinesiotherapy | ||
| Yes | 57 (62.6%) | Not available |
| No | 34 (37.4%) | Not available |
| Pain management with osteopathy | ||
| Yes | 15 (16.5%) | Not available |
| No | 76 (83.5%) | Not available |
| Pain management at a center of functional | rehabilitation | |
| Yes | 11 (12.1%) | Not available |
| No | 80 (87.9%) | Not available |
| Pain management using infiltrations | ||
| Yes | 35 (38.5%) | Not available |
| No | 56 (61.5%) | Not available |
| Response variable | ||
| Good composite outcome | 45 (49.5%) | 6 (50.0%) |
| Bad composite outcome | 46 (50.5%) | 6 (50.0%) |
| Predictors at baseline | ||
| Age | 47.7 (9.5) | 49.5 (14.7) |
| Sex | ||
| Male | 45 (49.5%) | 5 (41.7%) |
| Female | 46 (50.5%) | 7 (58.3%) |
| BMI | 27.4 (5.04) | 24.6 (3.9) |
| Pain duration | 12.2 (10.7) | 15.8 (15.1) |
| ODI | 50.5 (9.1) | 44.7 (12.8) |
| MADRS | 16.9 (10.4) | 11.3 (8.3) |
| EQ-5D | 0.38 (0.20) | 0.54 (0.19) |
| EQ-5D VAS | 45.8 (17.3) | 51.1 (20.0) |
| Leg VAS | 75.0 (11.3) | 72.9 (16.0) |
| Back VAS | 71.2 (15.1) | 67.6 (21.8) |
| TENS efficacy | ||
| Effective | 48 (52.7%) | 10 (83.3%) |
| Not effective | 43 (47.3%) | 2 (16.7%) |
| Hypoesthesia | ||
| Yes | 28 (30.8%) | 2 (16.7%) |
| No | 63 (69.2%) | 10 (83.3%) |
| Allodynia | ||
| Yes | 22 (24.2%) | 5 (41.7%) |
| No | 69 (75.8%) | 7 (58.3%) |
| Positional pain changes | ||
| Yes | 74 (81.3%) | 9 (75.0%) |
| No | 17 (18.7%) | 3 (25%) |
| MQS | 24.5 (14.7) | 5.6 (7.8) |
| Variables Changes (%) between Baseline and 12 Months | 1st Principal Component Loadings (50.1% of the Total Variance) |
|---|---|
| ODI | 0.86 |
| VAS | 0.81 |
| MADRS | 0.59 |
| EQ-5D score | 0.51 |
| Outcomes | Good Composite Outcome (GHIS ≥ 0) | Bad Composite Outcome GHIS < 0 |
|---|---|---|
| 50% global VAS decrease | ||
| Yes | 43 (93.5%) | 8 |
| No | 3 | 37 (82.2%) |
| 30% ODI decrease | ||
| Yes | 34 (73.9%) | 8 |
| No | 12 | 37 (82.2%) |
| 0.19 points change in EQ-5D | ||
| Yes | 30 (65.2%) | 17 |
| No | 16 | 28 (62.2%) |
| Model | True Good Outcome | True Bad Outcome |
|---|---|---|
| Screening trial (AUC = 0.69) | ||
| Good outcome | 6 (sensitivity = 100%) | 4 |
| Bad outcome | 0 | 2 (specificity = 33.3%) |
| LR (AUC = 0.72) | ||
| Predicted good outcome | 5 (sensitivity = 83.3%) | 2 |
| Predicted bad outcome | 1 | 4 (specificity = 66.7%) |
| RLR (AUC = 0.81) | ||
| Predicted good outcome | 5 (sensitivity = 83.3%) | 2 |
| Predicted bad outcome | 1 | 4 (specificity = 66.7%) |
| SVM (AUC = 0.75) | ||
| Predicted good outcome | 6 (sensitivity = 100%) | 2 |
| Predicted bad outcome | 0 | 4 (specificity = 66.7%) |
| NB (AUC = 0.81) | ||
| Predicted good outcome | 5 (sensitivity = 83.3%) | 1 |
| Predicted bad outcome | 1 | 5 (specificity = 83.3%) |
| ANN (AUC = 0.72) | ||
| Predicted good outcome | 5 (sensitivity = 83.3%) | 2 |
| Predicted bad outcome | 1 | 4 (specificity = 66.7%) |
| CART (AUC = 0.72) | ||
| Predicted good outcome | 4 (sensitivity = 66.7%) | 1 |
| Predicted bad outcome | 2 | 5 (specificity = 83.3%) |
| RF (AUC = 0.83) | ||
| Predicted good outcome | 5 (sensitivity = 83.3%) | 1 |
| Predicted bad outcome | 1 | 5 (specificity = 83.3%) |
| GBT (AUC = 0.81) | ||
| Predicted good outcome | 5 (sensitivity = 83.3%) | 1 |
| Predicted bad outcome | 1 | 5 (specificity = 83.3%) |
| Variables | Unstandardized Coefficients (β) | Standardized Coefficients | 95% CI | p-Value |
|---|---|---|---|---|
| Intercept | −3.044 | −0.070 | [−0.586; 0.447] | 0.792 |
| Duration of pain | −0.038 | −0.041 | [−0.939; 0.116] | 0.137 |
| MADRS | −0.097 | −1.012 | [−1.653; −0.371] | 0.002 ** |
| EQ5D VAS | 0.032 | 0.554 | [0.015; 1.093] | 0.044 * |
| Leg VAS | 0.040 | 0.449 | [−0.09; 0.988] | 0.102 |
| Hypoesthesia: yes | 2.361 | 1.096 | [0.455; 1.737] | 0.0008 *** |
| TENS: not effective | −1.312 | −0.659 | [−1.196; −0.122] | 0.016 * |
| MQS | −0.024 | −0.449 | [−1.061; 0.163] | 0.151 |
| Positional pain changes: yes | 1.500 | 0.588 | [0.017; 1.159] | 0.043 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ounajim, A.; Billot, M.; Goudman, L.; Louis, P.-Y.; Slaoui, Y.; Roulaud, M.; Bouche, B.; Page, P.; Lorgeoux, B.; Baron, S.; et al. Machine Learning Algorithms Provide Greater Prediction of Response to SCS Than Lead Screening Trial: A Predictive AI-Based Multicenter Study. J. Clin. Med. 2021, 10, 4764. https://doi.org/10.3390/jcm10204764
Ounajim A, Billot M, Goudman L, Louis P-Y, Slaoui Y, Roulaud M, Bouche B, Page P, Lorgeoux B, Baron S, et al. Machine Learning Algorithms Provide Greater Prediction of Response to SCS Than Lead Screening Trial: A Predictive AI-Based Multicenter Study. Journal of Clinical Medicine. 2021; 10(20):4764. https://doi.org/10.3390/jcm10204764
Chicago/Turabian StyleOunajim, Amine, Maxime Billot, Lisa Goudman, Pierre-Yves Louis, Yousri Slaoui, Manuel Roulaud, Bénédicte Bouche, Philippe Page, Bertille Lorgeoux, Sandrine Baron, and et al. 2021. "Machine Learning Algorithms Provide Greater Prediction of Response to SCS Than Lead Screening Trial: A Predictive AI-Based Multicenter Study" Journal of Clinical Medicine 10, no. 20: 4764. https://doi.org/10.3390/jcm10204764
APA StyleOunajim, A., Billot, M., Goudman, L., Louis, P.-Y., Slaoui, Y., Roulaud, M., Bouche, B., Page, P., Lorgeoux, B., Baron, S., Adjali, N., Nivole, K., Naiditch, N., Wood, C., Rigoard, R., David, R., Moens, M., & Rigoard, P. (2021). Machine Learning Algorithms Provide Greater Prediction of Response to SCS Than Lead Screening Trial: A Predictive AI-Based Multicenter Study. Journal of Clinical Medicine, 10(20), 4764. https://doi.org/10.3390/jcm10204764